Embed Size (px)
DESCRIPTION
The Maryland hospitals have gone through an unprecedented transformation in how their payments and operations are regulated. This transformation was not taken lightly and can serve as a guide for hospitals outside the State of Maryland as they look to take on additional financial risk in value-based contracts.
Citation preview

Transforming the Provider Market
What Pennsylvania Hospitals and Health Systems Can Learn from the New Maryland Medicare Waiver

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
1
Agenda
Changes in the Maryland Provider Market
Assessing Readiness to Take on Risk
Implementing Population Health Strategies In Value-Based Contracts

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
2
Introduction
With You Today:
James Case
Manager - Healthcare Advisory
■ James Case is a Manager in KPMG’s Healthcare Regulatory and Compliance practice in Baltimore. James has a strong background across a spectrum of financial services including:
– strategic and business planning,
– third party hospital reimbursement, and
– compliance services.
■ James has a MHS in Health Finance and Management from the Johns Hopkins Bloomberg School of Public Health and a BA in Health Administration and Policy from the University of Maryland.

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
3
There is unprecedented change going on in the acute hospital provider market in Maryland
Maryland reaches milestone deal with the feds for new Medicare Waiver
Baltimore Business Journal, January 10, 2014 Sarah Gantz
Maryland may be the model for curbing hospital costs
Instead of drumming up more business with big-name doctors, stand-alone emergency departments
And high tech equipment, Maryland hospitals this yea will do the unthinkable; strive to admit fewer patients
USA Today, January 31, 2014 Christine Vestal, Pew/Stateline Staff Writer
A bold experiment in per capita spending limits
Modern Healthcare, January 18, 2014 Merrill Goozner

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
4
Many hospitals are evaluating risk related to population health, but Maryland hospitals have been put on an accelerated time schedule

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
5
In taking that leap, there are lessons the Pennsylvania hospitals can learn when evaluating their strategies going forward
What does my population demand or need for healthcare services?
How do I make population health initiatives sustainable?
How do I measure my ability to control outcomes?
What does this population health trend mean to my bottom line?

Change in the Maryland Acute Care Provider Market

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
7
Why Does Maryland Matter? Maryland’s Unique All-Payer System
Maryland is the only State in the nation with an all-payer system
The Health Services Cost Review Commission (“HSCRC”) sets rates for hospital services, and all payers--including Medicare and Medicaid--are required to pay those rates to hospitals in the State
Act of Congress: Section 1814(b)(3) of the Social Security Act provides for Maryland’s unique status:
■ Requires all-payer participation with no undue discrimination between payers
■ Requires the State to meet a test to maintain this legislative waiver

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
8
The Maryland market consists of a wide variety of hospitals

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
9
The original Maryland Medicare Waiver was focused on controlling inpatient unit costs
The Original “Waiver Test”
Cumulative rate of growth in Maryland inpatient Medicare payments per case compared to the cumulative rate of growth nationally over the same time period (January 1, 1981 to present)
Key Original Waiver Tenants
Inpatient cost per case focus The original waiver test was based on Maryland inpatient regulated acute and chronic Medicare payments only
■ Did not include outpatient payments
■ Did not adjust for changes in case mix over time
■ Did not include physician or post acute care
Since the inception of the Medicare Waiver 35 years ago, the delivery of healthcare changed significantly
■ HSCRC quality and readmission policies that focused on quality of care incentivized shifting lower cost cases to outpatient settings and left the remaining inpatient cases more acute and costly.
■ The focus of the original waiver on inpatient cost per case no longer aligned with the current focus on population health

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
10
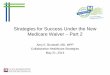
The operating margin of Maryland hospitals deteriorated starting in 2012 which led to discussions of a redesigned Waiver
Maryland hospitals experienced declines in financial performance due to decreased volumes and low update factors designed to save the original waiver
3.3%
2.2%
2.4%
2.2%
2.7%2.9%
2.5%
1.6%
1.9%
0.6%
1.7%
3.2%
0.0%
1.0%
2.0%
3.0%
4.0%
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
0.8%
2.4%
1.5%
Ope
ratin
g M
argi
n
Fiscal Year
Discussions of New Waiver Begin
2.5% HSCRC Operating Margin Target = 2.75%
Trend of Operating Margin Performance of Maryland Hospitals
Source: Maryland Hospital Association Financial Conditions of Maryland Hospitals; April 2013

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
11
Maryland decided to apply for a new Waiver to better align with today’s healthcare environment
Demonstration Project through the Center for Medicare & Medicaid Innovations (“CMMI”)
Effective 1/1/2014, Phase I is 2014-18. Phase II extends until 2022.
Modernized Waiver Tests:
■ Limit growth in Maryland per capita Revenue (inpatient and outpatient) to 3.58% (population growth estimated 0.6% annually)
■ Demonstrate $330 million over 5 years in Medicare savings via a slower growth rate in hospital payments for Maryland Medicare beneficiaries versus the National payment per beneficiary average
■ Reduce the Medicare readmissions rate to the national level in 5 years (CY2014-CY2018)
■ Reduce Potentially Preventable Complications by 30% in five years (CY2014-CY2015)
Renewal after 5 years with favorable performance and expansion to include physician and post acute services; if not renewed, revert to the national system.

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
12
The HSCRC has two revenue methodologies to control per capital costs
Fee for Service
Revenue is based on volumes – number of inpatient episodes of care and outpatient procedures
More inpatient episode of care and
outpatient visits = more revenue
Encourages caring for the ill and maximizing volumes
Global Budget Revenue
Revenue is fixed—annual revenue is pre-determined and does not change from year to year
More admissions and outpatient
visits = no more revenue
Encourages cost effective delivery of care with a focus on preventative care and patient wellness.
All Hospitals in the State are moving to the Global Budget Revenue Model

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
13
The Global Budget Model:
■ Annual fixed revenue budget for inpatient and outpatient regulated services.
■ Annual adjustments for changes in market share and quality programs.
■ As volumes decline, prices will need to increase to achieve GBR cap. Significant volume declines will cause price inefficiency.
■ This GBR cap could be enhanced or reduced based on hospital efficiency and utilization.
To achieve success under the new Waiver, hospitals have entered into revenue agreements to set fixed revenue targets called Global Budgets

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
14
Not all revenue is included under Global Budgets
The regulated revenue that is being capped is not all inclusive. At this time, it still excludes areas of patient care outside of the HSCRC’s authority:
■ Outpatient Renal
■ Outpatient Programs off the Hospital Campuses
■ Physician Professional Fees
■ Non-Patient Revenue (cafeteria, parking lot, rental income, etc.)
■ Specimen Only Labs (the patient does not physically reside in the Hospital)
Out-of-state revenue may or may not be included in the cap depending on the provider
May represent collaboration opportunities between Maryland and Pennsylvania hospitals

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
15
The incentives under the GBR model promote a population health perspective
■ Providing appropriate care at appropriate level or location (Physician office vs. Emergency Room)
■ Move towards Chronic Disease management
Success under GBR model includes:
Preventing Unnecessary Admissions Improving Patient Satisfaction
Preventing Readmission Increasing Primary Care Services
Preventing Unnecessary ED Visits Decreasing Unnecessary Utilization
Reducing Hospital complications Increasing Physician Alignment
Reducing Unnecessary Admissions from Nursing Homes
Reduce the number of patients admitted with Ambulatory Sensitive and Chronic Conditions
Controlling hospital costs is a key success factor under GBR

Assessing Readiness to take on Risk

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
17
In order to evaluate the readiness for risk, hospitals must start to build the case for change
Activities
Understand Demographics & Population Needs
Confirm population /services in and out of scope Assess unmet demand using public health intelligence to identify health inequalities, morbidity,
disease prevalence and social care needs Develop and agree patient needs assessment criteria
Demand and Capacity forecast modelling
Establish current demand and capacity Model population forecasts to create a picture of demand by specialty. Project future demand Assess future unmet demand
Market Analysis
Identify all providers within market including beds, services, activity, facilities, income, financial position
Identify all providers including services provided, income, bed base, and facilities Assess patient travel times between core services Horizon scan for factors impacting on capacity and demand
Sustainability tests (Clinical / Financial /Operational)
Conduct clinical sustainability test including clinical outcomes, patient experience and medical workforce establishment /turnover against industry guidance
Carry out high level financial analysis including performance and future efficiency requirement, and service line profitability/deficit by specialty
Assess operational performance and future sustainability including access and workforce performance indicators
Baselining & Benchmarking
Select peers and KPIs Conduct benchmarking exercise to signpost areas where differences exist (strengths and
weaknesses) Interpret findings from benchmarking exercise Use outputs of above activities to collate report on implications of ‘do nothing‘ option

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
18
Hospitals began by looking at trends in the demographics of their populations to assess underlying patient needs
Example Calculation of Life Expectancy in Baltimore City

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
19
Historical utilization was analyzed to draw assumptions about future utilization with changes in demographics
All Payors FY 2010 FY 2011 FY 2012 FY 2013 ODS Cases (1) 4,261 3,954 3,121 2,771 2+ Day Stays (1) 19,703 19,334 18,104 17,042
Total Admissions 23,964 23,288 21,225 19,813
Observation (OBV) (2) - 347 1,780 2,089
Total Admissions and OBV 23,635 23,005 21,902
Readmissions (3) - 1,904 1,705 1,526
Change in:ODS (307) (833) (350) (1,490) OBV 347 1,433 309 2,089
Net ODS and OBV 40 600 (41) 599 2+ Day Stays (369) (1,230) (1,062) (2,661)
Total Admissions plus OBV (329) (630) (1,103) (2,062)
Readmissions - 199 179 378
Change in Originating Volume (329) (431) (924) (1,684)
Cumulative FY 2010 - FY 2013

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
20
The Hospitals performed broad and specific market analyses to understand their competitors and potential collaborators
Social Care
Specialist Care
Primary Care Community Care
Mental Health
Acute Care
Community services • Reassess entire community services
provision • Linked with pathway redesign, ‘right
size’ and consolidate services, close services/sites where appropriate
• Integrate with strategic long term conditions management approaches
• ‘Facilitated network hubs’ to act as focal point for elderly and end of life care
Primary Care • With above average investment in primary
care, identify services provided, review for value for money
• Explore ‘hub and spoke’ models to maximise impact primary care can have
• Identify linkages to community/acute spend and ensure anticipated benefits are realised e.g. capacity removed
Mental Health • Address balance between
institutional and community care and ensure investment priorities are right
• Remove acute capacity where feasible
What is the optimum size of community services?
Maternity & reproductive services • Review provision of maternity services against
best practice, consolidate/close services • Review C-Section rates • Assess whether community infrastructure is
appropriate and prevent ante-natal admissions • Implement gynaecology decision aides to
reduce clinical variation
Trauma, injury & musculoskeletal • Review clinical practice, variation and ‘over-
treatment’ • For orthopaedics delineate between
specialist ‘focus factory’ non-elective care, and ‘value adding’ elective orientated services
• Integrate appropriately with community, pre/re-hab and other support services, further use of decision aides to reduce variation

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
21
Demand models were quantified to ultimately understand the net financial impact under various scenarios
Income Statement Impact under FFS Model $ in millions
Income Statement Impact under GBR Model $ in millions
$181$190
$200
$152$156$160
2015 2014 2016
Margin of $29M
Expenses Revenue
$200$200$200
$152$156$160
Margin of $48M
2014 2015 2016
The incremental margin can be used for further population health management investments

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
22
Scenario financial performance was then benchmarked to understand the implications of moving to GBR versus the status quo
3.5%
4.4%
5.0%
3.5%
3.5%3.6%
1.2%1.2%
1.7%
2.0%
2.7%
3.6%3.8%
3.9%4.1%
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
4.0%
4.5%
5.0%
2014 2015 2016
Baa Rating
Aa3 Rating Baseline
Baseline Including Capital Investments
Status Quo
Trend of Operating Margin Performance

Implementing Population Health Strategies In Value-Based Contracts

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
24
After establishing this type of payment arrangement, Maryland hospital are establishing processes to implement change in their organizations
Generate insights into the health dynamics of a population and the clinical focal points and clinical teams that will address care delivery pathways and questions of pricing and revenue.
Collect
Data Identification and Collection – combine longitudinal clinical data and non-traditional fields such as income and education levels
Focus
Focal Point Analysis – calibrated to the high-risk, high-priority patient population to identify additional co-morbidities and develop targeted clinical team
Implement
Implementing Clinical Analytics – creating a road map for operationalizing clinical analytics within your organization
Develop
Clinical Pathways and Economic Pricing – establish framework for contract pricing and risk management of care delivery
Vizualize
Extraction and Analytics – application of modeling algorithms and visualization techniques to identify high-risk, high-priority focal points based upon co-morbidities.
Verify
Data Integrity – reconcile and validate data to ensure consistency and completeness

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
25
$0
$50
$100
$150
$200
$250
$300
$350
$400
$450
$500
DIAGC DIAGIM NEURAD NUCRAD RAD
Med
icare
Allo
wed
Am
ount
s,
Radiology Services, 2010-2013
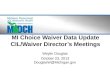
There is financial risk associated with clinical variation that is controllable through process redesign
Under a capitated arrangement, clinical variation creates economic risk as well as financial opportunity
■ Need to identify opportunities to eliminate clinical variation
– Example: an analysis we performed on Medicare-based Radiology expenses illustrates tremendous variation even after adjusting for risk factors or clinical complexity
$1,000
$10,000
$100,000
$1,000,000
$10,000,000
DIAGC DIAGIM NEURAD PEDRAD RAD
Med
icar
e A
llow
ed A
mou
nts,
Lo
gari
thm
ic S
cale
Radiology Services, 2010-2013
65th Percentile
Average
Medicare Based Radiology Charges
Variation in costs that need further explanation and analysis
Radiology Charges By Practice Radiology Charges Per Unit, Non-traumatic joint disorders

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
26
Identifying clinical variation will lead to creation of clinical cohorts to target interventions and protocols
■ Identify patients with significant costs of care across multiple conditions
– (i.e. patients with a non-chronic digestive disease diagnosis that are also diabetic)
■ The assumed complexity of cases identified by this analysis helps frame potential teaming and/or care management efforts
FOCUS
1. FOCUS COHORT IDENTIFIED
2. CLINICAL TEAM ASSEMBLED BASED ON CO-MORBITITIES WITHIN
FOCUS COHORT
Outcomes Treatment Pathways
and Protocols
Secondary Diagnosis
Primary Diagnosis
e.g., Hypertension
e.g., Diabetic
e.g., Arthritic
3. CLINICAL TEAM DEFINES THE CLINICAL PATHWAYS AND PROTOCOLS TO ADDRESS CLINICAL VARIATION AND TO IDENTIFY ADDITIONAL SOURCES OF CARE DELIVERY AND FINANCIAL RISK

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
27
Focusing on high risk patient types first have created the most initial value
■ Clinical Team Focuses Redesign of Care Delivery Process on High Economic Risk Populations
■ Outcomes differ for each “pathway”; leverage published materials such as AHRQ, HEDIS or HHS’ quality – and cost-based resources
■ For each pathway, need to identify sources of volatility (e.g., population risk drivers) and care service delivery variability (e.g., operational and supply chain issues)
Case Based Reasoning
Outcomes Treatment Pathways
and Protocols
Secondary Diagnosis
Primary Diagnosis
e.g., Hypertension
e.g., Diabetic
e.g., Arthritic
Primary disease states
Co-Morbidities
Dat
a An
alyt
ics
Focus Sub-Population
Multi-Disciplinary Clinical Team
Case Based Reasoning

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
28
Finance and performance management competencies may need to be augmented to support development of these types of programs
Identifying Care Needs Providing Population Health Management
Care Coordination Evidence-based Practices Provider Services Measurement &
Quality Improvement Program
Management
Case Assessment Transition of Care Management
Gaps in Care Analysis
Remote Monitoring & Management
Readmission Management
Authorization of Care
Comprehensive Utilization
Review Peer Review Standards &
Compliance Appeals & Grievance
Analysis of Utilization
Costing & Savings
Analysis Report
Patient Diagnosis
Secondary Preventive
Care
Planning or Implementing
Treatment
Follow-up Management
Hospital Provider
Efficiency
Cost Reductions
Evidence-based
Standards
Core Performance Measures
Patient Experience Measures
Practice Performance Reporting
Reporting Performance Publicity
Finance Information Technology Human Resources Operations Compliance
Patient Services Improved Patient Convenience Patient Education Patient Involvement Patient Satisfaction
Population Health
Management
Disease Management
Case Management
Utilization Review
Clinical Decision &
Support
Performance Management
Core Infrastructure
Patient Engagement
Tale
nt M
anag
emen
t
Pro
cess
Impr
ovem
ent
Tech
nolo
gy E
nabl
emen
t
Dat
a M
anag
emen
t

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
29
Pennsylvania hospitals will need to think through the types of cases that could use the Maryland model as learning platform
■ Encounters for a relatively low dollar amount (think preventive services or singular office visit) may be candidates for capitation
■ Less frequent and slightly more expensive care, e.g., office procedures and follow-ups etc., may be bundled because of the one-off nature of the services and needs
■ More complex encounters (but which are still manage-able) represent lower frequency and greater clinical variability, requiring a cross functional team and a more complex value-based reimbursement structure as well – Accountable care organizations, with a performance attribution methodology down to the
physician level, may be an example of this type of VBP arrangement ■ Random, catastrophic events are largely uncontrollable or manage-able, and are likely best
suited for fee-for-service arrangements ■ One budgeted value can be derived across these bands and across the population,
considering the distribution of major epidemiology or diagnostic groups

© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.
30
Presenters Contact Details
Questions and Discussion
James Case Manager
KPMG LLP 410.949.8895

The KPMG name, logo and “cutting through complexity” are registered trademarks or trademarks of KPMG International.
© 2014 KPMG LLP, a Delaware limited liability partnership and the U.S. member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity. All rights reserved.