Embed Size (px)
Citation preview

The role of NeuroEndoscopyin NeuroOncology
M. TriffauxV. MarneffeA. TyberghienI. Origer
7th EANO Congress, Vienna 16/09/06

NeuroEndoscopyNeuroEndoscopy
Ventriculoscopy Pituitary Key hole surgery

Ventriculoscopy in OncologyVentriculoscopy in Oncology
• In ventricular and paraventricular tumor management
• In Endoscopic Third Ventriculostomy (ETV)
– In the same time of supratentorial procedure
– in management of hydrocephalus from posterior fossa tumor
• Rigid
• Flexible
VentriculoscopeVentriculoscope

• Image Guided surgery– Choice of the best entry point and the best trajectory
– Endoscope tracking per operative
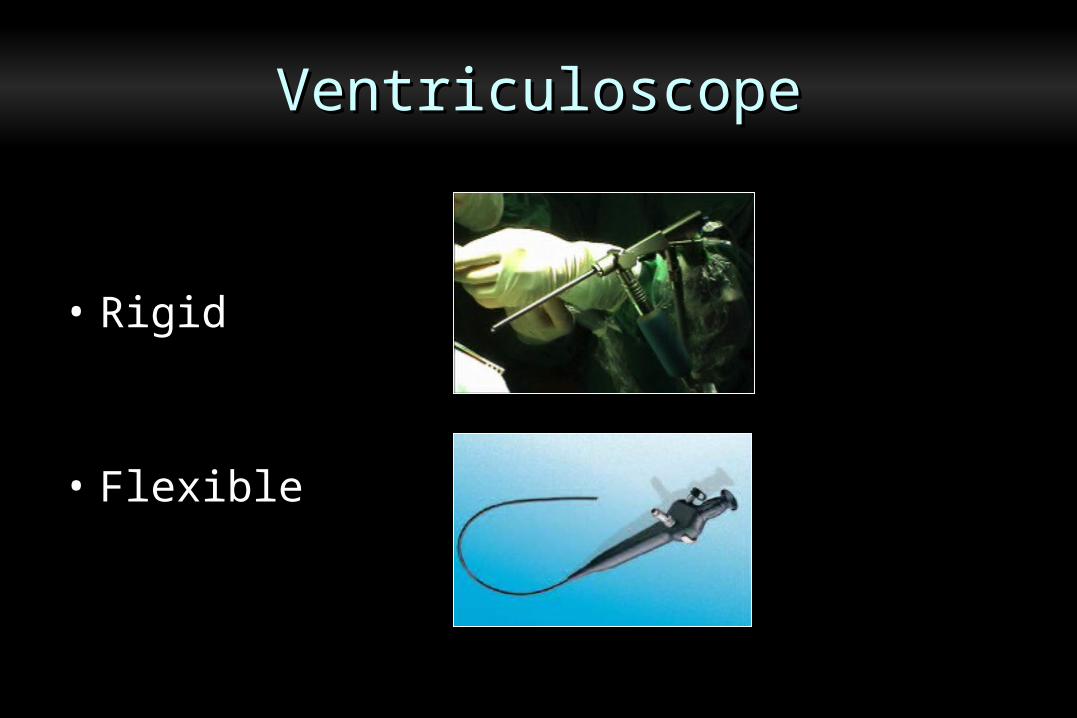
Advantages of the rigid scopeAdvantages of the rigid scope
• Image Guided surgery
• Endoscope stability – Pneumatic arm
– microdriver
Advantages of the rigid scopeAdvantages of the rigid scope

• Image Guided surgery
• Endoscop stabilisation
• Higher quality– optical resolution
– trocars: multiple channels
AdvantagesAdvantages of the rigid scope
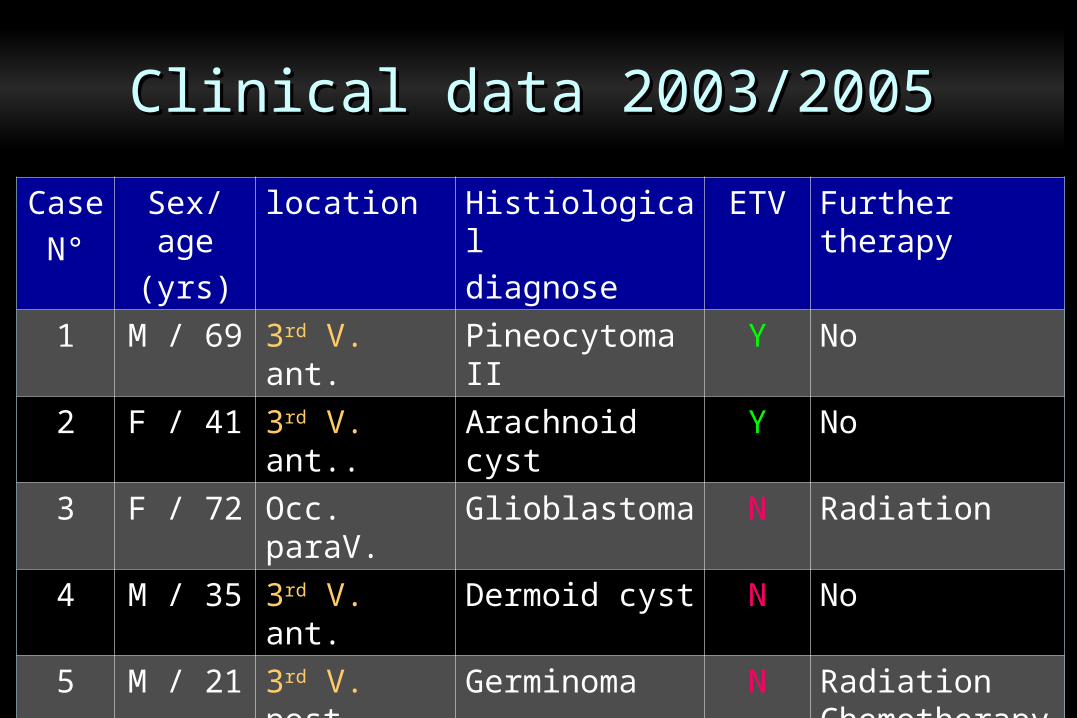
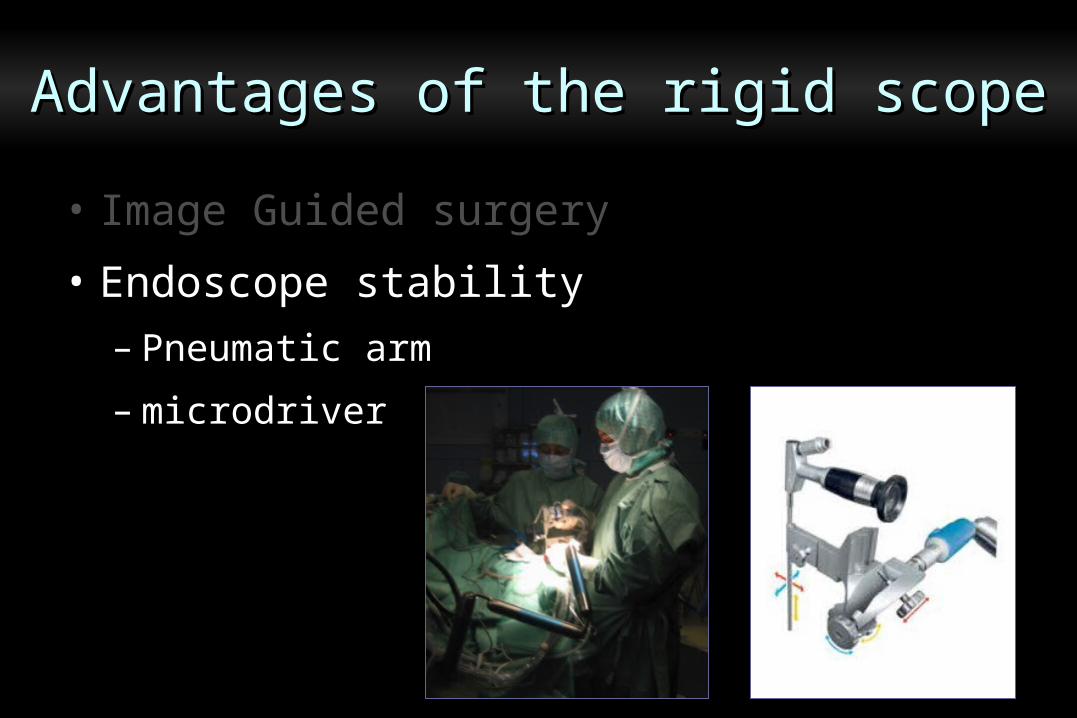
CaseN°
Sex/age(yrs)
location Histiologicaldiagnose
ETV Further therapy
1 M / 69 3rd V. ant. Pineocytoma II Y No
2 F / 41 3rd V. ant.. Arachnoid cyst Y No
3 F / 72 Occ. paraV. Glioblastoma N Radiation
4 M / 35 3rd V. ant. Dermoid cyst N No
5 M / 21 3rd V. post Germinoma N Radiation Chemotherapy
6 F / 16 Thalamic Astrocytoma III Y Open surgery
Clinical data 2003/2005Clinical data 2003/2005
• 21 yrs , recent diplopia
• CT MR imaging: pineal tumor whithout hydrocephalus
• Pet methionine: +
• Blood fetoproteine , HCG: nl < 1 mUI/ml
• CSF fetoproteine: nl, HCG: 3 mUI/ml
Case N° 5Case N° 5

Case N° 5Case N° 5

• Biopsy diagnosis: germinoma
• Treatment: chemotherapy & radiotherapy2 cycles carbo/ etoposide / Ifosfamide40 Gy radiotherapy
Case N° 5Case N° 5

Case N° 5Case N° 5
Initial MR Post multimodal therapy

Case N° 6Case N° 6
• 16 yrs , Parinaud’s syndrome
• CT MR imaging: left thalamic mass
hydrocephalus
• Pet FDG: – Pet methionine: +

Case N° 6Case N° 6
CT Pet FDG MR Pet met.

Case N° 6Case N° 6

J10 post biopsy & ETVPre operative
Case N° 6Case N° 6

• Biopsy diagnosis: astrocytoma III
• Treatement: conventional surgery
astrocytoma III confirmed
Case N° 6Case N° 6
• Acute hydrocephalus needs treatement:– External Ventricular drainage– VP shunt– ETV
• In pediatric series: – Majority of the authors advocate ETV prior to
definitive surgery– Some others do not justify routine preoperative ETV
• In adult patients: there is no specific data
Hydrocephalus from P-fossa tumorHydrocephalus from P-fossa tumor

CaseN°
s/age ICP Symp
ETV diagnose Open surgery
1 M/46 Y pre Lung metastase Y , radiation2 F/22 Y pre Medulloblastoma Y , chemo + radiation3 M/45 Y pre Ependymome II Y
4 M/55 Y pre Gliome II Y5 F/34 Y pre Melanocytoma Y6 F/39 Y pre Neurinoma VIII Y7 M/23 N post cavernoma Y8 F/56 Y single Breast mets. (3) palliatif
Clinical data in adult populationClinical data in adult population

• GA, supine position
• ETV with neuroballon
• Insertion of a ventricular reservoir
• Monitoring ICP 24h-48h with butterfly needle
without ventricular drainage
Surgical procedureSurgical procedure

• Complication: 1 infection (case 8: palliative)
resolved with antiobiotherapy
• No shunt
• No CSF leak after posterior fossa surgery
Out comeOut come

• Ventriculoscopy is safe and efficientin selected cases
• It is more easier with navigation endoscope guided • It takes its place in multimodal approach
• The ETV makes easier the management in P-Fossa tumors with acute hydrocephalus in adult patientsas well as in pediatric
ConclusionsConclusions