Embed Size (px)
DESCRIPTION
Value Based Healthcare
Citation preview

Value Based Health Care

Quality care pays out

How does benchmarking create more value in healthcare?
OutcomeCosts
Value = Michael Porter PhD, Professor, Harvard Business School, “What is Value in Health Care“ New England Journal of Medicine, December 23, 2010
“The Strategy that will fix healthcare”, September 2013

About the costs
Porter et al (2013): Calculate the full patient cycle costsMeasure activities per patientMeasure resources per activityRequires a well defined uniform costing methodology

Status of costing in Ireland
Costing requires local hospital knowledge, feedback and actionsNational costing project importantAccess to data needs to be improvedGalway/WNWHG first public group to deploy costing properly, with departments’ input
Bon Secours System first private group to deploy costing on a group-wide basis

Cost benchmarking possibilities
Purchase pricesEuropean market for high costs elements, devices. Are prices too high?
Resource utilisationWe all have doctors, nurses, administrative staff. How much should they produce?
Activities per patientSame patient diagnosesHow many activities are expected? (LOS, theatre, laboratories)
Treatment mix Treatment possibilities are global.Which options do we choose? (PCI, CABG)

OutcomeCosts
Value =
Now about the outcome

The outcome
Indicators set per disease/treatment in collaboration with doctors, for example:Complications (Intensive Care/infections/re-operations)MortalityVolume
New indicator sets define quality of lifeHospital mortality is getting very lowHigh differences in functional results For example after prostate surgery
Indicators supported by professionals

About DICA/DSCA
DSCA means Dutch Surgical Colorectal Audit. The DSCA records the results of cancer surgeries. This gives the professional insight into the quality of their own care and that of colleagues. This so-called benchmark information can demonstrably improve their work.
The DSCA was created by: The Dutch Society of Surgical Oncology, the Dutch Society for Gastrointestinal Surgery and the Dutch Colorectal Cancer Group.
DSCA is part of the Dutch Institute for Clinical Auditing (DICA).
Performation and DICA team up in measuring value of healthcare
A PhD study is focusing on relation of costs and clinical quality

Benchmark - quality
Funnel plot complicated clinical pathway vs. volume (2010-2012)

Making choices
Jointly with you we create high value healthcare for Europe
OutcomeCosts
Value =

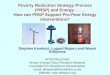
Value chart, colorectal surgery
Less complications (case mix corrected)
Low
er c
osts
/cas
eVolume of interventions : <85 per year : 85-140 per year : >140 per year
€ 18,000
€ 16,000
€ 14,000
€ 12,000
€ 10,000
€ 8,000
€ 6,00020% 30% 40% 50%10%0%
This team saves 7 complications/yearand saves € 3,300 per patient = € 270k/year
(compared to average hospital)

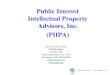
Focus: making choices
Less
cos
ts/c
ase
than
pee
rs
Less complications than peers
Observed/expected outcome compared to costs
Orthopaedics
HeartOncology
Obstetrics
FOCUSGood & efficient
STOPExpensive and
sub-standard
IMPROVECheap & sub-standard
‘LEAN’Expensive but good

Results DICA 2010-2012
201020112012
-23%201020112012
-18%
Mortality Complications
2010 2011 2012Patients 2553 2555 2939Died 102 95 91Mortality 4,0% 3,7% 3,1%
2010 2011 2012Patients 2553 2555 2939X-Patients 625 563 593X-Rate 24,5% 22,0% 20,2%
201020112012
-10%
2010 2011 2012Patients 2553 2555 2939Costs/case € 11.487 € 10.647 € 10.368
Costs
MEASUREFEEDBACKCOMPAREIMPROVE

How to make it happen?

Hospital Patient and activity data
Costing dataHospital
Patient and activity data
Costing dataHospital
Patient and activity data
Costing data
The key: reliable data
Patient and activity data(Hipe/PAS)
Costing data
Central ‘cloud’ data warehouse Benchmarkdatabase Reporting….
> 200 hospitals in NL/UK/IE
Clinical data

Easy to understand and easy to utilise reporting

The Dutch perspective

Experiences in the Netherlands
UHI introduced 1998MFTP introduced 2007-2012Freedom of choice in insurer, hospitalSafety nets along the routeHospitals were already foundation trusts
Autonomous seeking for best information systems
Management information has improved dramaticallyWaiting lists have reduced, quality has improvedAcute hospital costs are now going down
EfficiencyQualityBetter purchasing

Outside – in observationsMFTP/UHI is the way to goIn Ireland, administrative data is widely available, however data is not structuredMost key players are still in the dark on essential information!
Major backlog on ICT investments (expenditures are only 0.3%!)Need for wall-to-wall HISNeed for Business Intelligence, DWH, dashboardsHigh investment per hospital, or innovative, cloud solutions….
Cultural / regulations aspect make it very hard to innovate at local level Hospital managers need to empowered to take a risk
Clinical data needs to be collected, monitored and actioned DICA?Connect the doctors stronger to the hospitals

Summary

Summary
Value = Outcome / Costs (Porter)Benchmarking is an essential driving force
Benchmarking on efficiency requires costing modelsBenchmarking on outcome requires clinician involvement
Value charts allow strategic choicesWith benchmarking, value increasesWNWHG and Bon Secours System are frontrunners in financial transparencyData is a challenge in IrelandCloud Data Warehouse is a viable route, comparing UK/NL/IE

Sweelincklaan 1 Baggot Street Upper 9-113712 JA Bilthoven Dublin 4The Netherlands Ireland+31 30 233 3872 +353 1 662 8280
www.performation.com