Right access - and some myth busting about general practice
18
www.england.nhs.uk @robertvarnam #PMChallengeFund Delivering right access Dr Robert Varnam Head of general practice development [email protected]@robertvarnam Sheffield PMCF 25 June 2015 bit.ly/ 20150625access
Right access - and some myth busting about general practice
1. www.england.nhs.uk @robertvarnam #PMChallengeFund Delivering
right access Dr Robert Varnam Head of general practice development
[email protected] @robertvarnam Sheffield PMCF 25 June 2015
bit.ly/20150625access
2. www.england.nhs.uk @robertvarnam #PMChallengeFund One of the
things motivating me as I first looked outside the walls of our
practice, to lead some local service redesign for diabetes, was
fear. A fear that general practice, despite being a service
depended on by the country, had a very uncertain future. In fact, I
was afraid that general practice was being run into the ground.
Although NHS spending was rising, with growing amounts of staff and
money, the majority was going elsewhere in the system. Even though
we were talking increasingly about the importance of providing more
care outside hospital, the investment was going inside
hospital.
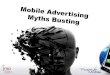
3. www.england.nhs.uk @robertvarnam #PMChallengeFund Hows it
feeling? Figure 1 Proportion of patients reporting positive
experiences of primary care services, England 2011-12 to 2013-14
11% of requests for an appointment are unmet 10% of those divert to
A&E/WIC, 3% see a pharmacist instead, 12% get no care An
estimated 2-5% of A&E attenders have not tried to obtain GP
care
4. www.england.nhs.uk @robertvarnam #PMChallengeFund The
founding principles of UK primary care are admired the world over,
and rightly so. General practice is a jewel in the crown of this
country. Right now, general practice feels in a bad place.
Constrained, hemmed-in and, to some, marginalised. Whatever the
state of things in your part of the country, in general, I think
its fair to say that, at the very least, general practice is
currently constrained from delivering its full potential. We need
to see increases in funding, a growth in the workforce, and
improvements to premises. Without those, existing services may not
be sustainable. Hows it feeling? We DO care but its too hard to
right now to deliver our potential
5. www.england.nhs.uk @robertvarnam #PMChallengeFund In my work
over the past few years, Ive encountered some persistent myths
about general practice and change. They run quite deep and hold
back a lot of potential. They dont just affect policymakers or
politicians, either theyre often things primary care leaders
believe themselves. The Challenge Fund is a great opportunity to
achieve lasting transformational change in your area. But, to make
the most of that, youre going to have to be confident in
challenging five key myths. @robertvarnam #PMChallengeFund
Myth-busting
6. www.england.nhs.uk @robertvarnam #PMChallengeFund Myth
One
7. @robertvarnam #PMChallengeFund Myth 1: general practice is
finished. Or, at least, not far off. There are some who talk as
though general practice is finished, or as near as makes no
difference. Sometimes, these are people within the profession,
sometimes outside. When morale is low, its understandable for
negative emotions to influence our assessment. But just look what
happened when the government invited practices to apply for this
innovation programme nearly two thirds of the country responded!
And, with very exceptions, every proposal was for worthwhile
change. The team here were nearly drowned by the work of processing
it all. Thats not a part of the NHS thats dead, lacking in energy
or in ideas. We just need to give general practice the headroom for
it to fulfil the enormous potential it has. The creativity, plans
and energy are already there. General practice is finished
@robertvarnam #PMChallengeFund PM Challenge Fund 57 schemes 2500
practices 18m patients
8. www.england.nhs.uk @robertvarnam #PMChallengeFund Myth
Two
9. @robertvarnam #PMChallengeFund Myth 2: Access is simple Weve
been here before, launching a national programme to improve access
in general practice. But Im struck by how simplistic much of the
thinking has been on previous occasions. Weve treated access as
though it stands alone as a feature of general practice. As though
its meaningful to improve speed of making an appointment without
asking who its with, or what kind of care theyre able to provide.
Thats clearly nonsense, and we risk providing very poor value to
individual patients and taxpayers if we dont acknowledge that
access is one facet of a complex system of care. We similarly risk
thinking that every patient needs the same kind of access. Just
saying it like that, its clearly untrue. Yet how many times have we
even you or I been involved in a change which was about moving from
one monolithic, one-size-fits-all appointment system to another? In
the first year of the Challenge Fund I was delighted to see that
many schemes were actually aiming to deliver what Ive dubbed right
access connecting the right patient with the right person, able to
give the right care in the right place at the right time. And
acknowledging that its right for some patients not to see the
doctor, just as it is for some to have much greater confidence that
they will, soon. Access is simple Right Access @robertvarnam
#PMChallengeFund
10. www.england.nhs.uk @robertvarnam #PMChallengeFund Myth
Three
11. @robertvarnam #PMChallengeFund Myth 3: if we just did this
one thing Its probably human nature, but silver bullet thinking
abounds in the NHS. Probably in your own team meetings. How many
times, often with a sigh of frustration, does someone (maybe you)
exclaim If we just did x/y/z, it would solve this? Sometimes, a
single change makes a massive difference. But rarely. Every one of
the innovations youre proposing is very sensible. Most have at
least some evidence already. But none of them has ever been found
to achieve all the improvement we need. Youre going to need
several, combined. At best, silver bullet thinking will lead you
disappointed and tired. At worst, itll discredit the ideas youre
trying out, simply because someone allowed in the thought that just
doing this one thing would achieve all your goals. Its almost never
true. If we just @robertvarnam #PMChallengeFund
12. Its too easy to approach challenges just by thinking we
need more. The NHS has a well established habit of this new
initiatives, new challenges or opportunities are usually met by us
talking about more. More money, more staff or both. And, we know
that, in general practice, we do need both more money and more
staff. BUT and its a big but just doing more of the same is simply
not going to cut it any longer. Not just more of the same
13. @robertvarnam #PMChallengeFund Myth 3: if we just did this
one thing Its probably human nature, but silver bullet thinking
abounds in the NHS. Probably in your own team meetings. How many
times, often with a sigh of frustration, does someone (maybe you)
exclaim If we just did x/y/z, it would solve this? Sometimes, a
single change makes a massive difference. But rarely. Every one of
the innovations youre proposing is very sensible. Most have at
least some evidence already. But none of them has ever been found
to achieve all the improvement we need. Youre going to need
several, combined. At best, silver bullet thinking will lead you
disappointed and tired. At worst, itll discredit the ideas youre
trying out, simply because someone allowed in the thought that just
doing this one thing would achieve all your goals. Its almost never
true. If we just @robertvarnam #PMChallengeFund
14. www.england.nhs.uk @robertvarnam #PMChallengeFund Myth
Four
15. @robertvarnam #PMChallengeFund Myth 4: Our good ideas are
all we need When youve been working on a set of ideas for what
changes to make to your service, its natural to become quite
attached to them. You may have had some feelings of resentment
lately as people have asked you probing questions about them,
through the due diligence process. The trouble is, the consistent
experience of people leading large scale change is that 70% of
efforts fail. Not just in the NHS, or in healthcare, but worldwide
in every industry. And one of the big factors causing that
depressing experience is a belief that good ideas are enough.
Theyre not. Theyre obviously necessary, but Im afraid theyre not
sufficient. Along with the WHAT of your change, you need the HOW.
The strategies, tactics and methodologies by which you turn the
good idea into a movement of people and a plan of action. If you
dont skilfully lead people, if you dont use an effective
improvement methodology, if you dont measure right the evidence
shows you risk failing. Well do all we can this year to support you
with the HOW of change. Id ask you to start by commiting to have
plans which combine the how and the what, and which unleash your
practices commitment by clearly articulating the WHY (well talk
more about that later) Good ideas are enough WHAT HOWWHY
@robertvarnam #PMChallengeFund
16. www.england.nhs.uk @robertvarnam #PMChallengeFund Myth
Five
17. @robertvarnam #PMChallengeFund Myth 5: failure is not an
option In the NHS, one can be led by a culture of regulation or
performance management to fear failure or change. Even to be
tempted to cover them up. Is that appropriate for innovation
leaders? Do you know the significance of the number 5127? Its the
number of prototypes James Dyson had to make before his first
bagless vacuum cleaner worked fully. Is that 5127 failures? Of
course not, its 5127 steps on the way to getting a good idea to
work in the real world. Eddison once said I have not failed, I have
found 10,000 ways NOT to make a lightbulb. If, at the end of this
year, you tell us that every part of your initial plans was a
fantastic success, I will conclude that you are either foolish,
deluded or lying. Because they wont be. Everyone who has ever set
out with an idea about making a service better has found that some
aspects of the idea work first time, and others need to be tweaked.
And some of our ideas just dont seem to work at least not in our
context or with our implementation approach. Discovering that is
not a failure, it is necessary. The failure would be not to
anticipate it or not to spot it. If you encounter something thats
not working as you expected, change it. It would be an appalling
waste of public money and confidence if you didnt. Just do it with
your eyes open and your brain engaged. Please dont make decisions
based solely on instinct or opinion. If you suspect somethings not
working right, measure it. Make a rational, evidence based
assessment. And when you start finding things that need tweaking or
possibly even stopping, please tell us as soon as possible. We
really want to learn from your experience, including from failure.
You should expect were going to ask why you think it needs
changing. If we can, we may connect you with someone else whos done
something similar and had a different result, to see if that helps
you or we can learn more about the conditions for success. But
failing to get every idea to work without any tweaking is not
failure, its innovation. In fact, its life. We must not fail
@robertvarnam #PMChallengeFund Learn from it!