Embed Size (px)
Citation preview
Puneet Bajaj, M.D., M.P.H.Assistant Professor of Medicine
Rheumatic Diseases Division
RA is a chronic, systemic, inflammatory disorder of unknown etiology that primarily involves synovial joints
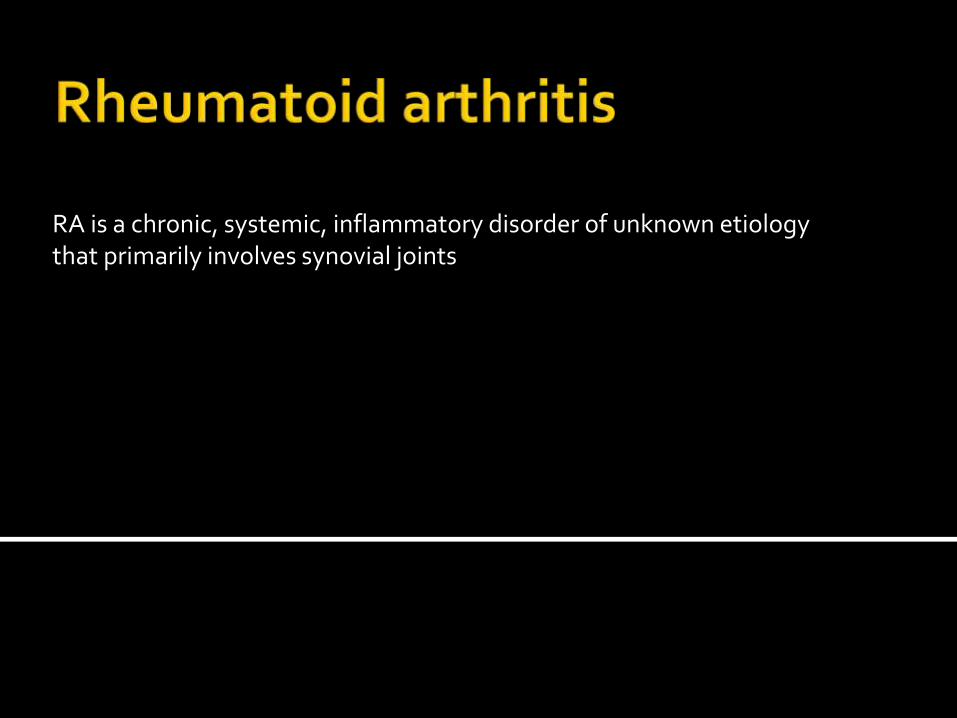
Hereditary Environmental
Triggers:
Eg, cigarette smoking, infection, or trauma
• Inflammatory synovitis
• Palpable synovial swelling or tenderness
• Morning stiffness >1 hour
• Symmetrical and polyarticular
• Typically involves wrists, MCP, and PIP joints
• Typically spares certain joints
▪ Thoracolumbar spine
▪ DIPs of the fingers and IPs of the toes
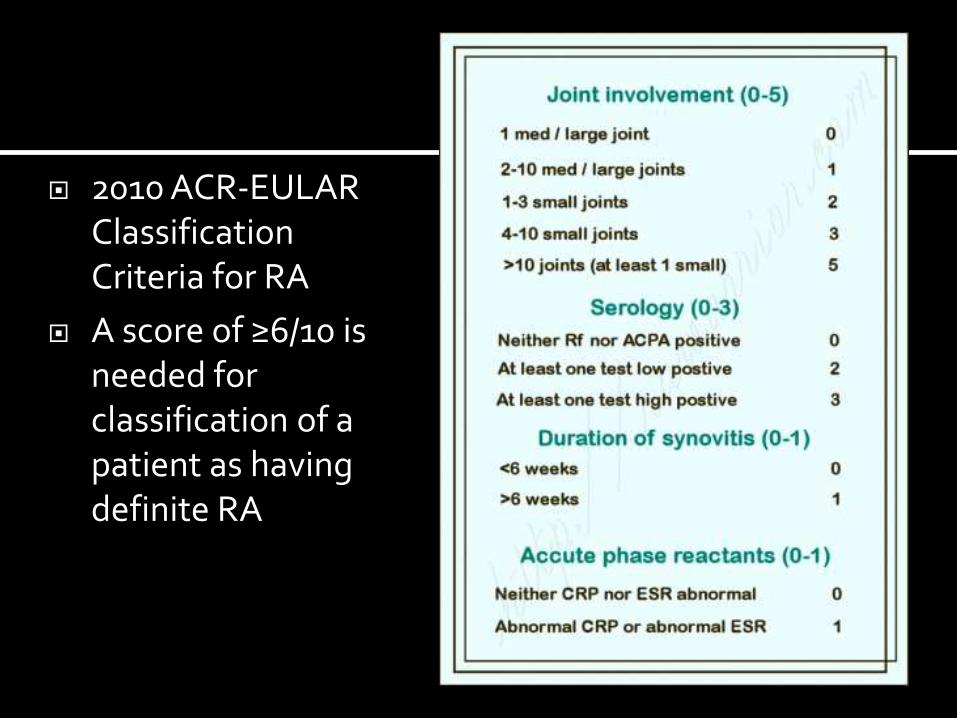
2010 ACR-EULAR Classification Criteria for RA
A score of ≥6/10 is needed for classification of a patient as having definite RA
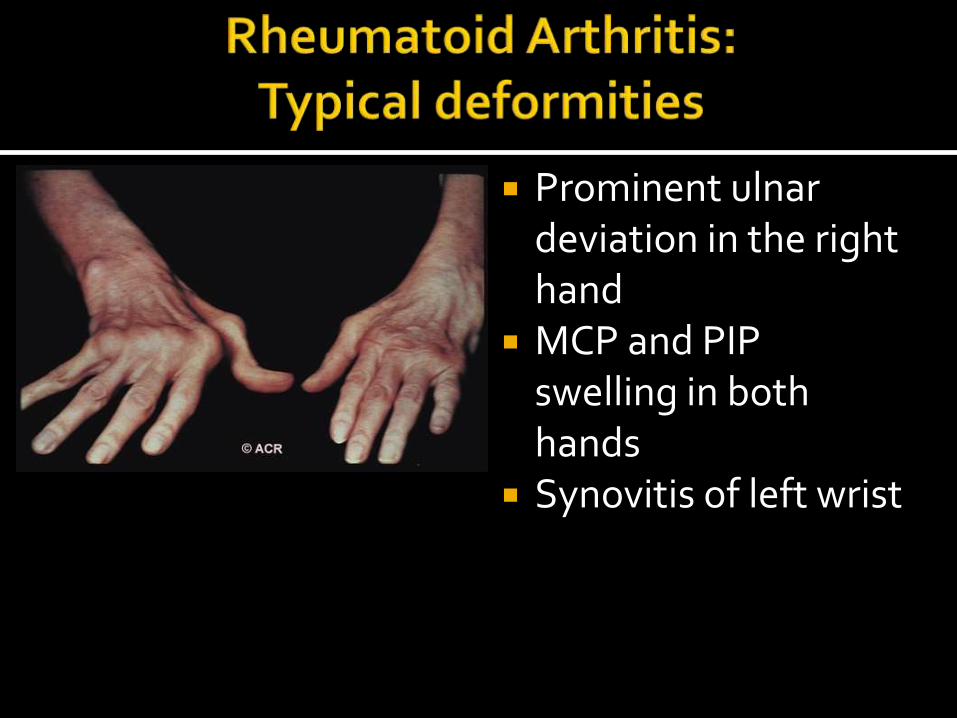
Prominent ulnardeviation in the right hand
MCP and PIP swelling in both hands
Synovitis of left wrist
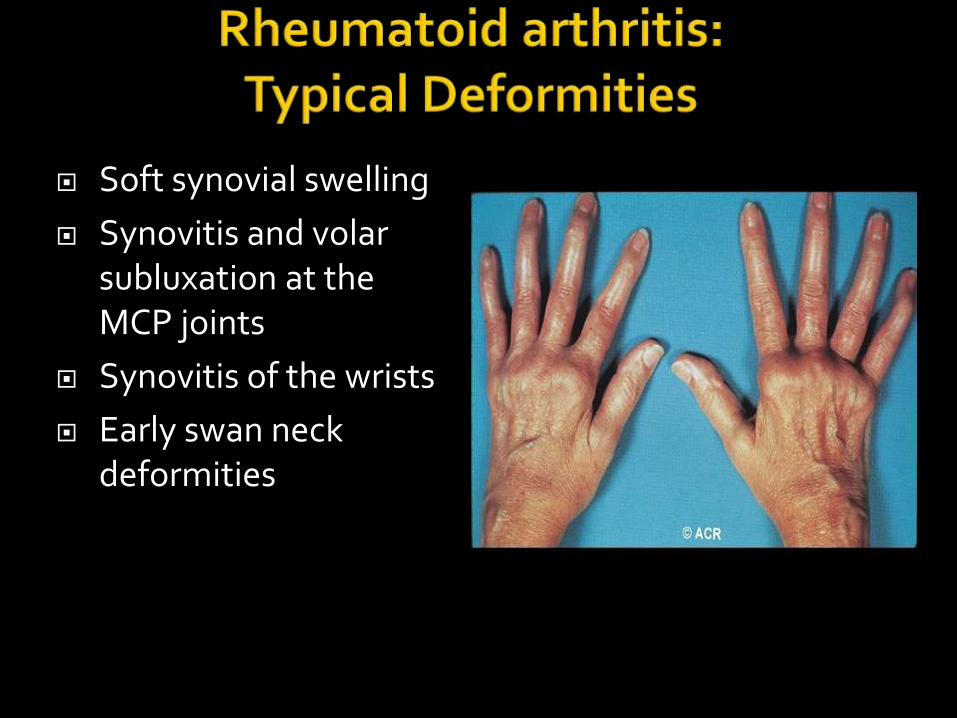
Soft synovial swelling
Synovitis and volarsubluxation at the MCP joints
Synovitis of the wrists
Early swan neck deformities
Rheumatoid nodules Felty’s syndrome (neutropenia, splenomegaly) Rheumatoid vasculitis Eye:
Episcleritis
Scleritis (pain, tenderness, photophobia) Interstitial lung disease Amyloidosis (long-standing poorly controlled
dz) RA is independent risk factor for CAD
• RF (IgM against the Fc portion of IgG)• Specificity approx. 80%
• 45% positive in first 6 months
• 85% positive with established disease
• Not specific for RA• Hep C (mixed cryoglobulinemia)
• Sjögren syndrome
• SLE
• May be present in up to 10% of healthy persons
• Anti-CCP antibodies • more specific – 95%
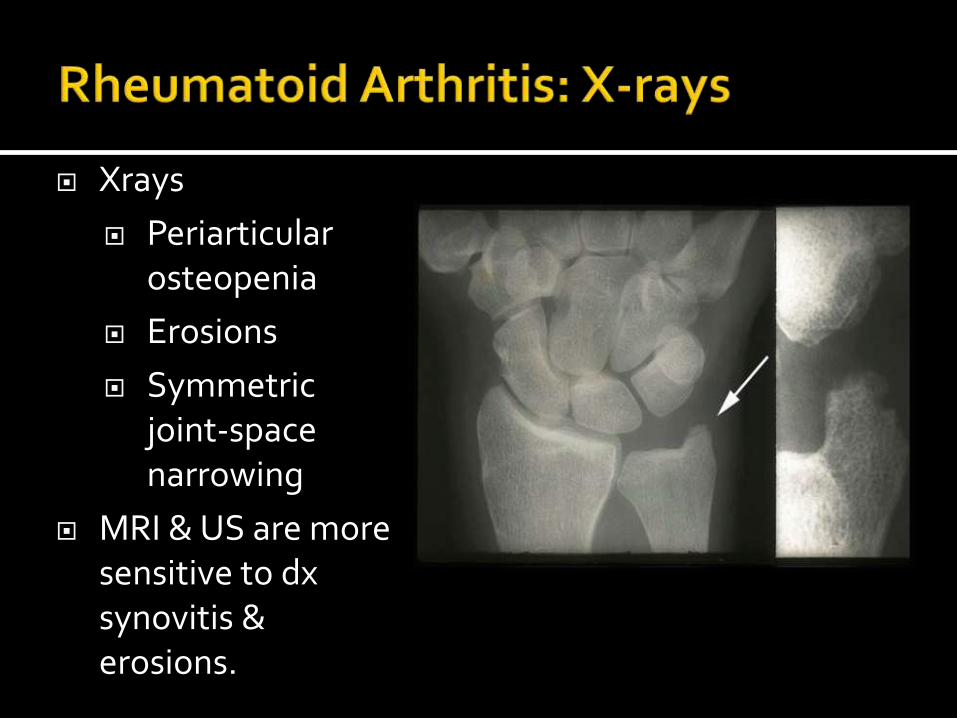
Xrays
Periarticularosteopenia
Erosions
Symmetric joint-space narrowing
MRI & US are more sensitive to dxsynovitis & erosions.
• Long-standing rheumatoid arthritis• May have NO symptoms• Manipulation under anesthesia can cause
spinal cord injury• Flexion and extension X-rays of the C spine
Klippel. Primer on Rheum Dis. 13th edition. 2008:114
• Damage occurs early in most patients
• 50% show joint space narrowing or erosions in the first 2 years
• By 10 years, 50% of young working patients are disabled
• Assess current activity
• Morning stiffness, synovitis, ESR/CRP
• Degree of damage
• X-rays: Joint space narrowing and erosions
• Functional status
• Assess prior Rx responses and side effects
• Education
• Educating the patient about their disease• Exercise/Physical Therapy• Vaccination
• Influenza and pneumococcal vaccines are advised.
• Live vaccines
• should be avoided in patients on biologic therapies
• considered safe with nonbiologic DMARDs and low-dose prednisone
2012 Update of the 2008 American College of Rheumatology recommendations for the use of disease-modifying antirheumaticdrugs and biologic agents in the treatment of rheumatoid arthritis. Arthritis Care Res, 64: 625–639.
• NSAIDs
• Not DMARDs
• Low-dose prednisone (10 mg qd)
• May substitute for NSAID
• Used as bridge therapy
• Intra-articular steroids
• Useful for flares
• Disease modifying drugs (DMARDs)
• Sulfasalazine, hydroxychloroquine
▪ May use in patients with low dz activity
• Methotrexate/Leflunamide
▪ MTX is the gold standard therapy
• Triple Therapy
• HCQ, SSZ & MTX
• Cyclophosphamide
▪ Effective for vasculitis, less so for arthritis
Klippel. Primer on Rheum Dis. 13th edition. 2008:133.
• Anti-TNF drugs (First line biologics)• Infliximab
• Etanercept
• Adalimumab
• Golimumab
• Certolizumab pegol• Side Effects of anti-TNF agents.
• Infections (Hep B/TB reactivation)
• CHF exacerbation
• Demyelinating dz
• Drug induced lupus
• Tocilizumab – IL6 inhibitor • Increase lipids, GI perforation, HZ reactivation,
improve anemia.• Abatacept – inhibits T cell co-stimulation
• COPD exacerbation• Tofacitinib – interferes with JAK-STAT
pathway• Increase lipids, HZ reactivation
• Rituximab – anti CD 20 • Risk for developing PML
Most women demonstrate clinical improvement during pregnancy
Flares are common during the postpartum period MTX must be discontinued 3 mths prior to
conception. Leflunomide must be discontinued 2 yrs prior to
conception cholestyramine may be used to hasten the elimination.
SSZ can cause reversible oligospermia; men should discontinue it for 3 months prior to conception
HCQ & SSZ are often used during pregnancy.
A 32 YO woman seeks preconception counseling. She was diagnosed with RA 1 year ago. She has no other pertinent personal or family medical history. Disease activity is controlled with methotrexate. She also takes FA.
On PE, vital signs are normal. On MSK examination, there is no synovitis or bony abnormalities. The remainder of the examination is normal.
Laboratory studies, including ESR and CRP level, are normal; RF and anti-CCP antibodies are positive. Urine pregnancy test results are negative.
Radiographs of the hands, feet, & C spine are normal.
Which of the following is the most appropriate management?
A. Discontinue methotrexate before conceptionB. Discontinue methotrexate when conception is
confirmedC. Maintain methotrexate through pregnancy at
current doseD. Maintain methotrexate through pregnancy
with dose adjustment
Women with RA who are taking MTX must discontinue it 3 months before conception.
A 52 YO man is evaluated for an 8-week history of pain and 2 hours of morning stiffness of the hands that improves with activity. The patient has no pertinent personal or FH. He takes no medications.
On PE, vital signs are normal. Synovitis is noted at the MCP joints of the second through fifth digits bilaterally with swelling, tenderness, and pain on range of motion. The remainder of the examination is normal.
Laboratory studies, including CBC, chemistries, LFTs, TSH, CRP, and UA, are normal; ESR is 13 mm/h, and RF is negative. Parvovirus serology results are negative.
Radiographs of the hands are normal.
Which of the following antibody assays is most helpful in establishing this patient's diagnosis?
A. Anti–cyclic citrullinated peptide antibodiesB. Antimitochondrial antibodiesC. Antineutrophil cytoplasmic antibodiesD. Antinuclear antibodies
RF may be negative in early RA. Anti–CCP antibodies are a highly specific marker for RA.
A 64YO man is evaluated during a routine f/u visit for a 5-year h/o RA. Four months ago, he began IV tocilizumab to manage synovitis that was not responding to treatment with etanercept; his last infusion was administered 2 weeks ago. The patient also has hypertension. FH is notable for his father, brother, and uncle with coronary artery disease. Other medications are enalapril, HCTZ, methotrexate, prednisone, and naproxen as needed.
On PE, temperature is 37.0 °C (98.6 °F), BP is 130/84 mm Hg, pulse rate is 80/min and regular, and RR is 16/min. Auscultation of the heart and lungs is normal, and no edema is present. No synovitis is present on MSK examination. The remainder of the examination is unremarkable.
Laboratory studies performed before each infusion reveal normal CBC, LFTs, and serum creatinine levels. A lipid profile obtained 6 months ago revealed a total cholesterol level of 180 mg/dL (4.7 mmol/L) and a LDL cholesterol level of 98 mg/dL (2.5 mmol/L).
Results from a tuberculin skin test obtained before starting tocilizumabtreatment were negative.
Which of the following is the most appropriate test to perform next?
A. EchocardiographyB. ElectrocardiographyC. Lipid profileD. Serum aminotransferase levelsE. Serum immunoglobulin levels
Periodic monitoring for changes in lipid status is indicated for patients receiving tocilizumab.
A 42 YO man is evaluated for morning stiffness of the wrists lasting up to 1 hour. He was diagnosed with RA 4 months ago and was started on methotrexate and titrated to maximum dose 3 months ago with partial response. He also takes prednisone as needed for joint pain and FA daily.
On PE, vital signs are normal. MSK examination reveals swelling, tenderness, and pain on range of motion of the wrists. No rash or joint deformities are noted. The remainder of the examination is normal.
Laboratory studies reveal a CRP of 3.1 mg/dL; anti–CCP antibodies are positive.
Which of the following is the most appropriate treatment?
A. Add adalimumabB. Discontinue folic acidC. Discontinue methotrexate; begin infliximabD. Discontinue methotrexate; begin
sulfasalazineE. Maintain current regimen
Use of methotrexate with a TNF α inhibitor is associated with further reductions in disease activity and radiographic progression
Age: 75% of persons over age 70 have OA Female sex Obesity (most important modifiable risk
factor) Hereditary Trauma Neuromuscular dysfunction Metabolic disorders
Pain is related to use Pain gets worse during
the day Minimal morning
stiffness (<20 min) and after inactivity
Range of motion decreases
Joint instability Bony enlargement Crepitus Variable swelling
and/or instability
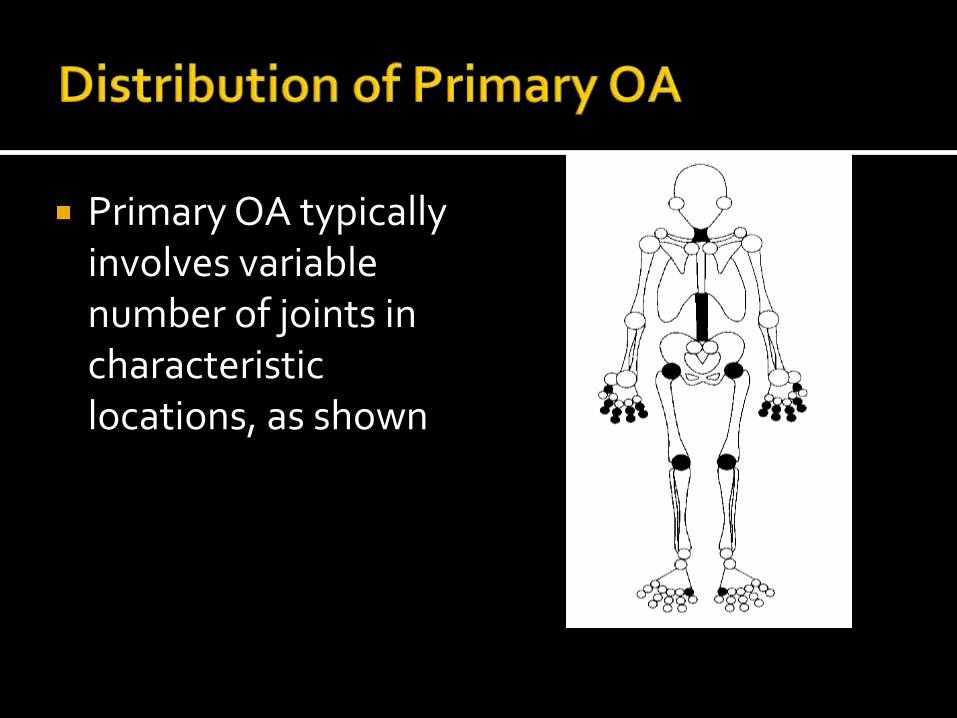
Primary OA typically involves variable number of joints in characteristic locations, as shown
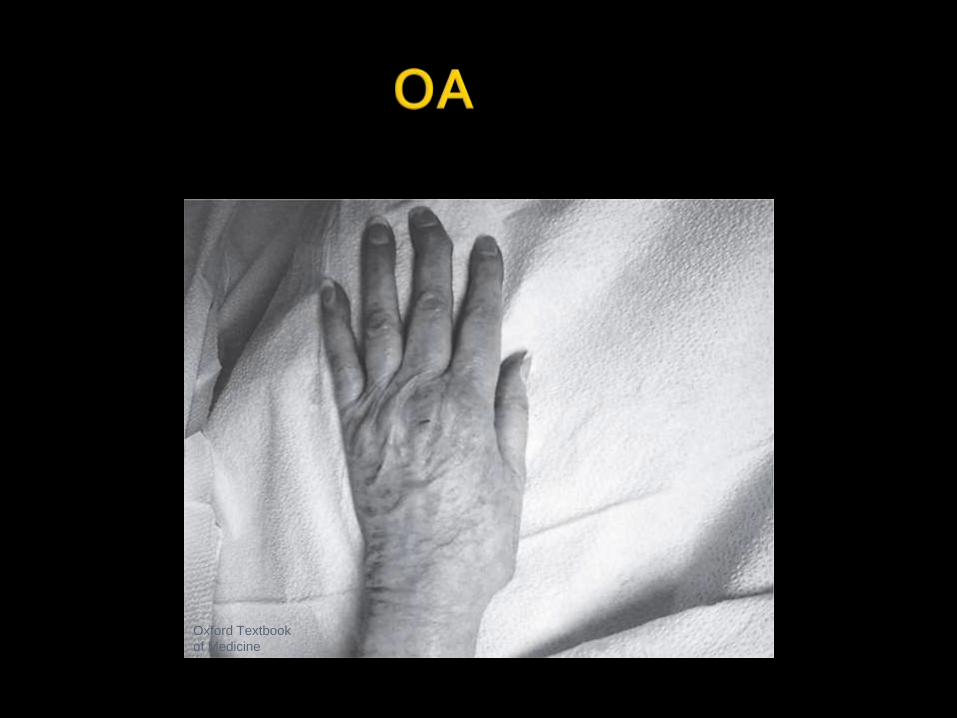
Oxford Textbook
of Medicine
No specific tests No associated laboratory abnormalities;
eg, sedimentation rate
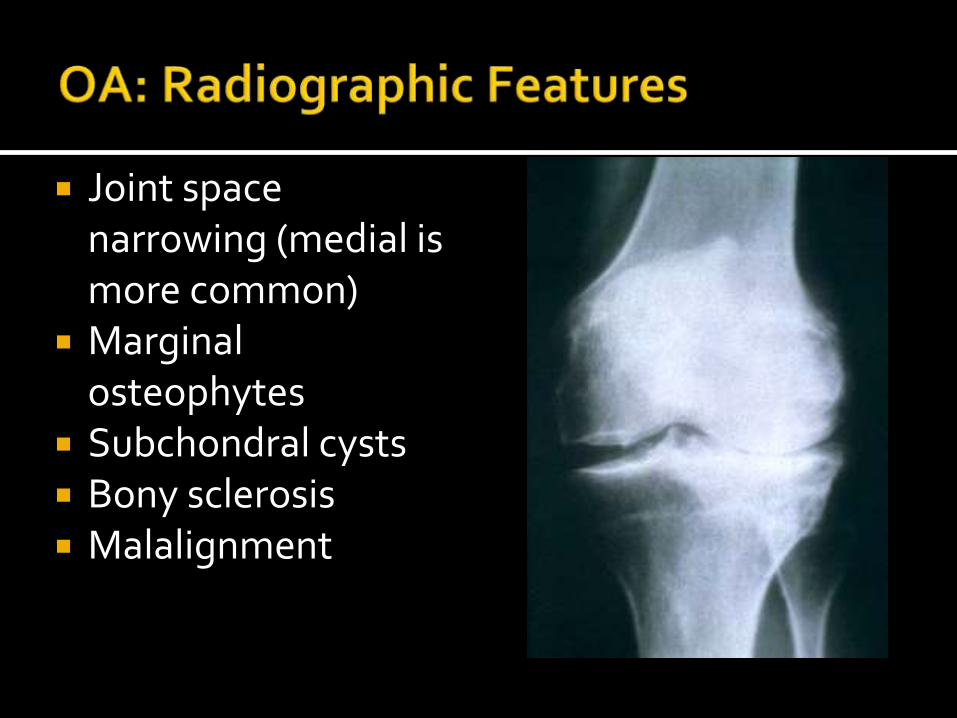
Joint space narrowing (medial is more common)
Marginal osteophytes
Subchondral cysts Bony sclerosis Malalignment
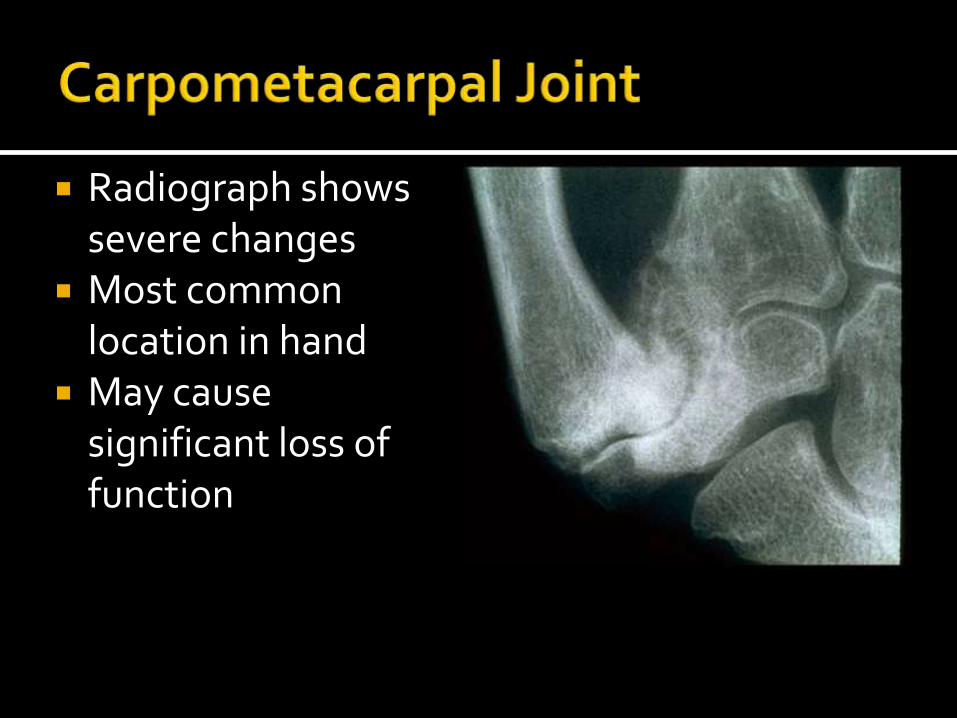
Radiograph shows severe changes
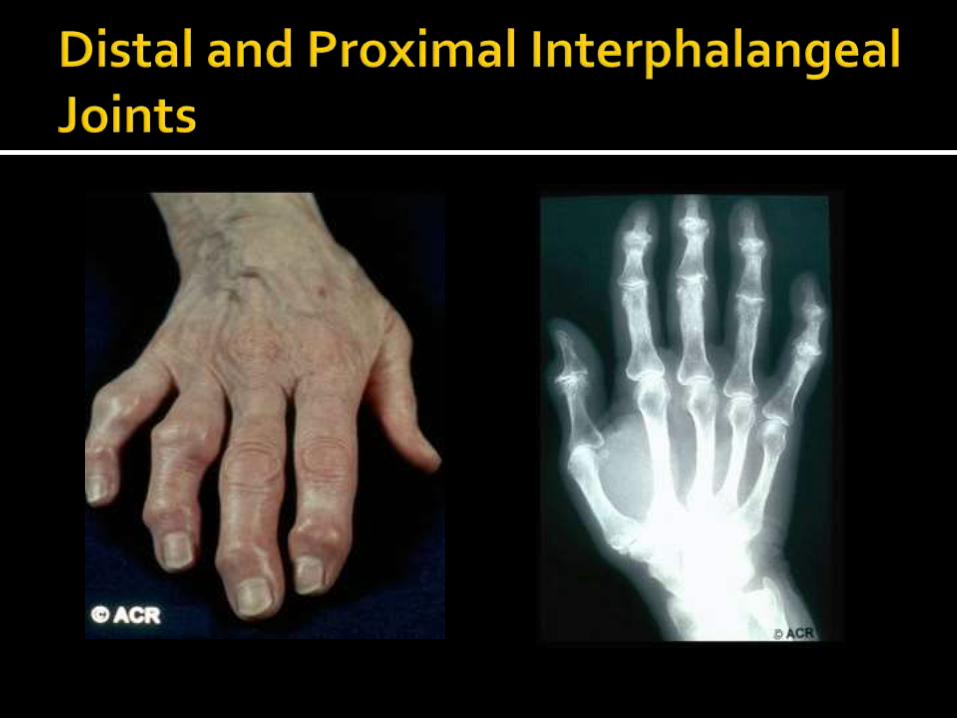
Most common location in hand
May cause significant loss of function
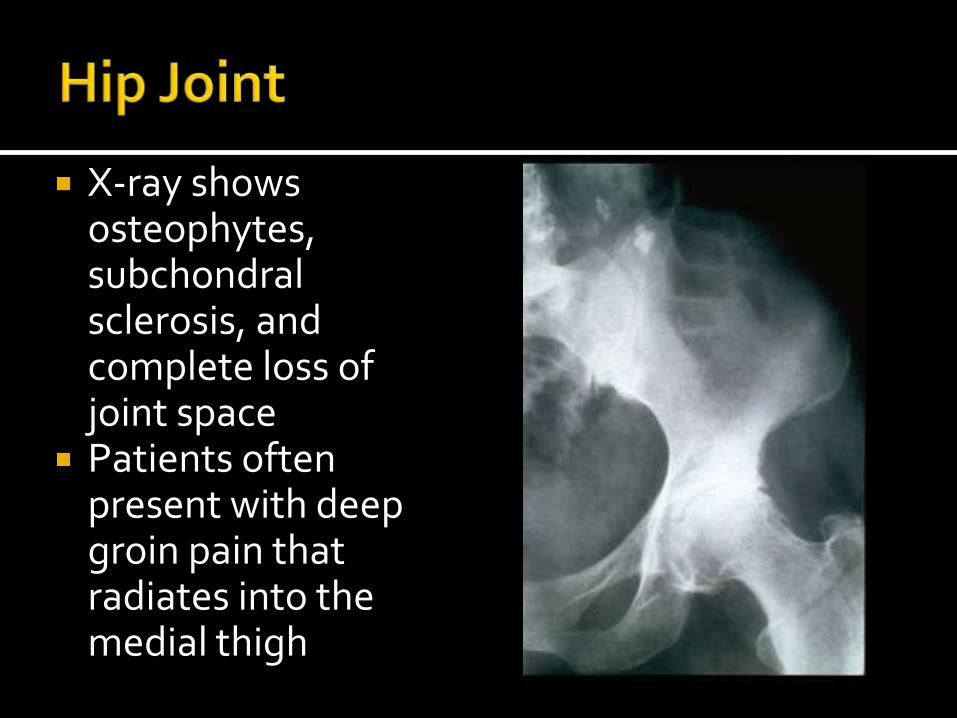
X-ray shows osteophytes, subchondralsclerosis, and complete loss of joint space
Patients often present with deep groin pain that radiates into the medial thigh
• Consider secondary causes of OA
• Previous trauma and/or overuse
• Neuromuscular disease, especially diabetic or other neuropathies
• Metabolic disorders,
• CPPD (calcium pyrophosphate deposition disease)
• Hemochromatosis• MCPs with hook like osteophytes
• Order iron studies
• Genetic tests: HFE mutations (C282Y)
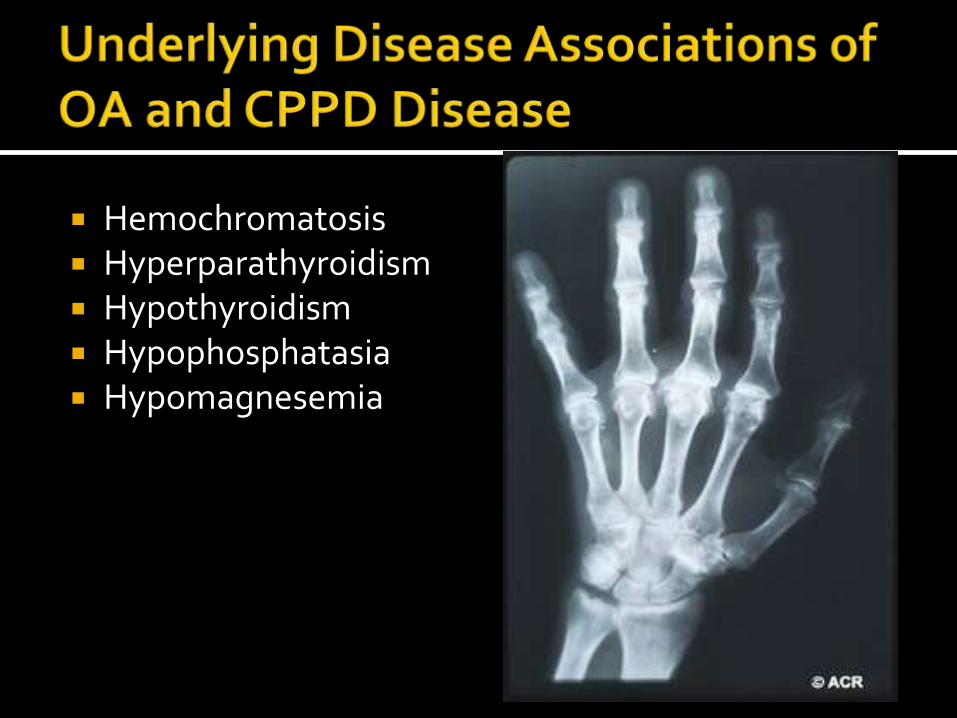
Hemochromatosis Hyperparathyroidism Hypothyroidism Hypophosphatasia Hypomagnesemia
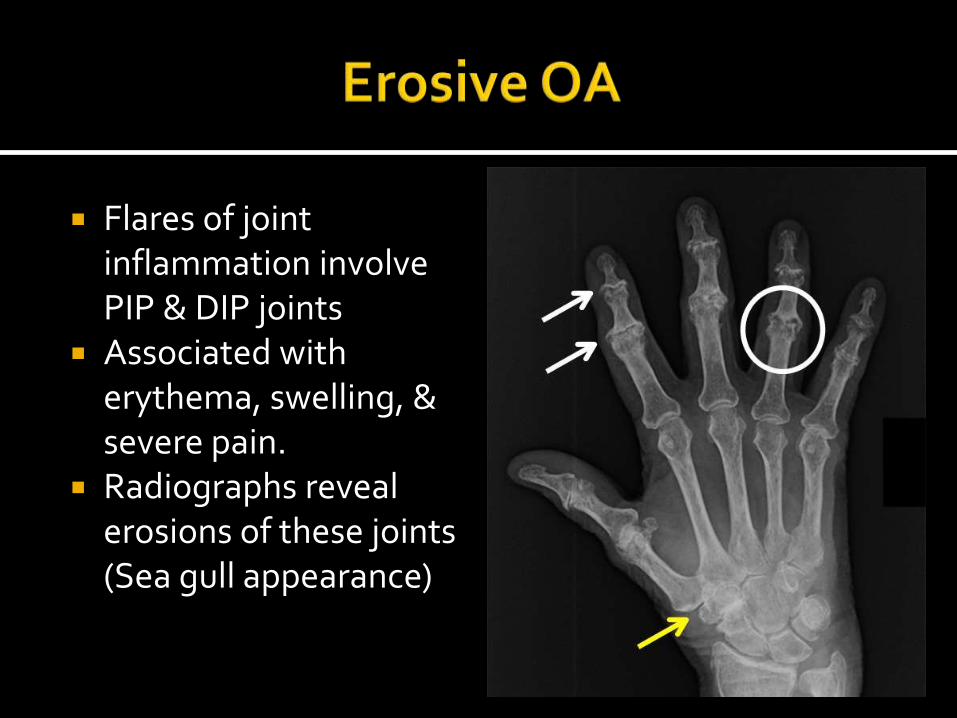
Flares of joint inflammation involve PIP & DIP joints
Associated with erythema, swelling, & severe pain.
Radiographs reveal erosions of these joints (Sea gull appearance)
• Goal: decrease pain to increase function• Progressive exercise to
• Increase function
• Increase endurance and strength
• Reduce fall risk
• Patient education:
• Weight loss
• Heat/cold modalities
Use of a cane can significantly unload a knee /hip & improve gait, mobility, & pain.
Proper Positioning Placed in the hand contralateral to the symptomatic
joint.
The top of your cane should reach to the crease in your wrist when you stand up straight.
Elbow should bend a bit (10-15 deg.) when holding the cane.
Walking Cane & injured leg swing & strike the ground at the
same time.
Nonopioid analgesics Topical agents Intra-articular agents Opioid analgesics
• Surgery
• Arthroscopy
• Osteotomy
• Total joint replacement
• Decision is based on the patient's sx & quality of life, rather than the radiographic severity
A 76 YO woman is evaluated for a 3-month history of left knee pain of moderate intensity that worsens with ambulation. She reports minimal pain at rest & no nocturnal pain. There are no clicking or locking symptoms. She has tried naproxen and ibuprofen but developed dyspepsia; acetaminophen provides mild to moderate relief. The patient has HTN, HLD, and chronic stable angina. Medications are lisinopril, metoprolol, simvastatin, low-dose aspirin, and nitroglycerin as needed.
On PE, VS are normal. BMI is 32. ROM of the left knee elicits crepitus. There is a small effusion without redness or warmth & tenderness to palpation along the medial joint line. Testing for meniscal or ligamentous injury is negative.
Lab studies, including CBC & ESR, are normal.
Radiographs of the knee reveal medial tibiofemoral compartment joint-space narrowing and sclerosis; small medial osteophytes are present.
Which of the following is the next best step in management?
A. Add celecoxibB. Add glucosamine sulfateC. MRI of the kneeD. Weight loss and exercise
Obesity is the most important modifiable risk factor for knee OA.
A 58 YO man is evaluated for a 6-year history of hand pain accompanied by morning stiffness lasting 30 minutes & a 2-year history of bilateral hip pain. He takes naproxen, which moderately relieves the pain.
On PE, VS are normal. There is tenderness of both wrists and the MCP joints and pain on flexion and internal rotation of the hips. The wrists and hips have limited range of motion.
Radiographs reveal joint-space narrowing at the hips, MCP joints, and proximal interphalangealjoints; osteophytes are seen at the MCP and hip joints.
Which of the following tests is likely to confirm diagnosis?
A. Antinuclear antibody assayB. Rheumatoid factorC. Serum transferrin saturationD. Serum uric acid level
Secondary OA involving the MCP joints should specifically raise suspicion for hemochromatosis.
A 72 YO woman is evaluated for a 6-month history of increasing pain and swelling of the hands and fingers associated with a 20-year history of OA. The pain is worse with activity, and she now has difficulty opening jars and buttoning her shirt. She states that diclofenac no longer provides relief.
On PE, temperature is 37.0 °C (98.6 °F), BP is 148/78 mm Hg, PR is 88/min, and RR is 18/min. MSK exam reveals bilateral firm swelling and tenderness of the second and third proximal IP joints. The left third distal IP joint is swollen and red. The remainder of the examination is unremarkable.
Laboratory studies reveal an ESR of 36 mm/h.
Radiographs of the hands reveal joint-space narrowing of the proximal and distal IP joints with multiple osteophytes; erosive changes of the distal IP joints are noted.
Which of the following is the most likely diagnosis?
A. Erosive hand osteoarthritisB. Psoriatic arthritisC. Rheumatoid arthritisD. Tophaceous gout
Erosive hand OA involves proximal and distal IP joints that are associated with erythema, swelling, and severe pain. Erosions in DIPs should raise suspicion for erosive OA or PsA.
American College of Rheumatology (ACR) ACR: Image Bank ACR: Rheum2Learn
https://www.rheumatology.org/education/training/Rheum2Learn.asp
Primer on Rheumatic Diseases ACP – MKSAP 16




![BATF regulates collagen-induced arthritis by regulating T ......that predispose toward OA (i.e., aging) are important causes of OA pathogenesis [6, 7]. In contrast, RA is an inflammatory](https://img.pdfslide.us/doc/110x75/613b4597f8f21c0c8268e813/batf-regulates-collagen-induced-arthritis-by-regulating-t-that-predispose.jpg)