Embed Size (px)
Citation preview

Joshua E PetrikinJune 26th, 2015

ObjectivesDescribe the fetal circulation and the
normal transitional circulatory changes that occur at birth
Describe the problems that arise when there is maladaptive cardio-respiratory transition at birth
Discuss the pathogenesis of persistent pulmonary hypertension
Discuss the neonatal conditions that predispose to persistent pulmonary hypertension
Describe the management of persistent pulmonary hypertension

ContentsIntroductionFetal and transitional neonatal circulationPathophysiology of PPHNConditions associated with PPHNClinical Presentation & DiagnosisManagement of PPHNPrognosis & Follow-up

IntroductionFetal adaptation to postnatal conditions
requires the transition of the pulmonary circulation from a high resistance state in-utero to a low resistance state
results in a nearly 10 fold increase in pulmonary blood flow (PBF)
Pulmonary Vascular Resistance (PVR) continues to decline after birthnormally reaches 80% of total decrease by 24-
48 hoursreaches nearly adult values around 6 weeks of
life

IntroductionPersistent pulmonary hypertension of the newborn
(PPHN)the failure to achieve or sustain the normal decrease in
PVR at birtha clinical syndrome that can occur in association with
diverse cardio-respiratory disorders
These conditions share common pathophysiologic features, includinghigh pulmonary vascular resistanceextra-pulmonary shunting (right to left) of blood flow
across the ductus arteriosus or foramen ovalemarked hypoxemia

Fetal Circulation

Transitional Circulation- NewbornInflation of the lungs
↓ the resistance to pulmonary blood flow results in ↑ blood flow to the lungs ↓ blood flows through the foramen ovale to the LA
Increased volume of blood returns from the lungs ↑ pressure in the LA
The ↑ LA pressure & ↓ RA pressure (due to ↓ PVR) closes foramen ovale
The ductus arteriosus, closes off shortly after birth replaced by connective tissue
The increased PBF flow distends the vasculature causing a “structural reorganization” of
the vascular wall
Local vasoregulatory mediators play an important role in this transition

Pathophysiology of PPHNHallmarks of PPHN include
sustained elevation of PVRabnormal vasoreactivitystructural remodeling of the pulmonary
vascular bed
Mechanisms leading to failure of postnatal adaptation are poorly understood

Vasoregulation of the Normal Fetal Pulmonary CirculationDue to the high PVR in the normal fetus, the
pulmonary circulation receives ~ 10% of combined ventricular output
Factors that contribute to high basal PVR include: low O2 low basal production of vasodilator products ( PGI2 & NO
Adenosine) increased production of vasoconstrictors (ET1, LT, TBX, PAF ) altered smooth muscle cell reactivity
NO-cGMP cascade important role in vasoregulation of the fetal pulmonary circulation: Modulating basal PVR in the fetus Mediating vasodilator response to physiologic & pharmacologic stimuli Opposing the strong myogenic tone in the normal fetal lung

L-arginine L-citrullineNOS
Endogenous Nitric Oxide (NO) Effects
↑cGMP NO
+cGMP kinase
↓IC Calcium
+sGC
Vasodilation5’GMP
Phosphodiesterase

Developing Lung Circulation
Intrauterine InjuryHemodynamic StressChronic StressInflammationOther (genetic)
Vascular Growth
Abnormal Vascular Reactivity
Altered Vascular Structure
↓ Angiogenesis↓ Alveolarization ?
↓ Vasodilators (NO, PGI2, Adenosine)↑ Vasoconstrictors (ET1, LT, TBX, PAF)Enhanced Myogenic Tone
↑ SMC ProliferationAltered Extracellular MatrixAdventitial thickening
Pathogenesis of PPHN
Pulmonary hypoplasiaCDH
RDS, MAS, GBS
Chronic IU hypoxiaIdiopathic PPHN

Clinical Presentation & Diagnosis- PPHN
Dx considered when hypoxemia is out of proportion to the degree of parenchymal disease severity on the CXR (idiopathic), a positive perinatal hx may be helpful
Physical examinationrespiratory distressCyanosisTachycardiaHypotensionO2 sat differencesingle/loud S2systolic murmur of TRdifference between preductal & postductal
oxygenation

Clinical Presentation & Diagnosis of PPHN
Lability of Oxygenation : wide swings in PaO22DTTEcho
level & direction of shuntPAP estimated (Bernoulli equation)abnormal septal motionflat septum, increase RA
Disease severity suggested by oxygenation indexOI = 100 X (MAP)(FiO2) / PaO2 OI > 25 receive care at ECMO centerOI >40- ECMO

Differential DiagnosisCongenital Heart Disease
PAPVR */ TAPVRPA with intact ventricular septumTransposition of Great Arteries (TGA)Tricuspid Atresia
Pulmonary Alveolar Capillary Dysplasiafailed formation & growth of alveolar capillaries and
medial musculature hypertrophy

Conditions Associated with PPHNMAS( 41%)Idiopathic (17%)RDS (13%)Sepsis/Pneumonia (14%)CDH (10%)Pulmonary Hypoplasia (4%)

Meconium Aspiration Syndrome (MAS)Most severe condition associated with
meconium passage in utero
MAS occurs in 2-5% of infants with meconium stained amniotic fluid (MSAF) Meconium in utero may be a response to stress
chronic hypoxia, acidemia or infection Most infants with MSAF are asymptomaticMSAF rarely occurs before 38 weeks gestation
incidence increases with longer gestations 30% of newborns born at 42 weeks have MSAF
Diagnosis based on clinical history of MSAFmeconium aspirated from below the vocal cordsan infant with respiratory distresscoarse opacification seen on CXR

Meconium Aspiration SyndromeMechanism of respiratory distress leading to
PPHN includeblockage of the airwayinactivation of surfactantdirect damage to the lung parenchymaatelectasis & V-Q mismatch
Infants usually present with mild to moderate respiratory distress, but rapidly progress to respiratory failure with cyanosis & PPHN
These infants are prone to air leaks- pneumothorax

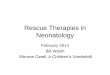
Meconium Aspiration SyndromeCXR shows
coarse infiltrateswidespread consolidationhyperinflationpneumothoraxpneumomediastinum
Treatment includessupplemental O2ventilatory strategies to prevent air-
trappingtherapy for PPHN- iNO & ECMO

Meconium Aspiration Syndrome
bilateral patch opacity with hyperinflation & air leak

Meconium Aspiration Syndrome
Rt pneumothorax

Idiopathic Persistent Pulmonary Hypertension (“black lung”)
Profound hypoxemia & hyperlucent lung fields
Constriction of ductus in-utero > exposure to NSAID
Exposure to SSRIDown SyndromeUnknown factors-
genetic or biologic susceptibility

Congenital Diaphragmatic Hernia (CDH)Developmental defect in the diaphragm
allows abdominal viscera (liver, spleen, stomach, intestine) to herniate into the thoracic cavity
secondary to persistence of the pleuroperitoneal canal in the posterolateral portion of the diaphragm
90% on left through foramen of Bochdalek10% on right through foramen of Morgagni
1: 2200 live birthsPulmonary hypoplasia and abnormal
vascular development withDecreased bronchial and pulmonary arterial
branchingPulmonary arterial muscle hyperplasia leading to
PPHN

Congenital Diaphragmatic Hernia (CDH) Affected neonates present in first a few
hours of life with respiratory distress CXR- postnatally is diagnosticMay be asymptomatic in newborn periodDefinitive treatment – surgical
not emergentelective repair when hemodynamically stable &
PPHN resolved/under control
With advent of antenatal Dx & improvement in neonatal care, survival has improved, but remains significant risk of death (population-based studies no improvement in survival)

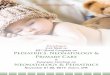
Congenital Diaphragmatic Hernia (CDH)

Congenital Diaphragmatic Hernia (CDH)
pattern of bowel in the left hemithorax. There is mediastinal shift to the right.

Congenital Diaphragmatic Hernia (CDH)

Congenital Diaphragmatic Hernia (CDH) Prenatal Dx, monitoring, labor induced in
controlled setting at 38-39weeksAt delivery, minimize bag-mask ventilation and
intubateInsert NG tube for gastric decompression
Maintain adequate systemic blood pressureAvoid barotrauma to the hypoplastic lungs
Contributes to CDH mortalityAttempt to ventilate with low peak pressure
(<25cmH2O) to minimize/ prevent lung injury Sedation as needediNO and surfactant of unproven benefitiNO frequently used as a bridge to ECMO

Pulmonary HypoplasiaCan occur in association with
Oligo/anhydramniosbilateral dysplastic kidneyssevere PUVCDH Other congenital abnomalities
Arrest of lung development & differentiation
Potters Syndrome: bilateral renal agenesis & pulmonary hypoplasia

Term gestation, posterior urethral valves
Post ECMO , Post Dialysis

Respiratory Distress Syndrome (RDS)Terminology
RDS: a clinical diagnosis Hyaline Membrane Disease (HMD) a pathological
diagnosis Surfactant Deficiency: describing the typical
appearances on CXR
Most common respiratory disorder observed in premature infantsAlso occurs in near term & term infants
A leading cause of morbidity & mortality in newborn period

Respiratory Distress Syndrome (RDS)
Caused by relative or total lack of surfactant
Deficiency of surfactant ---> ↓ FRC---> atelectasis & V-Q mismatch
ABG: low PaO2, high PaCO2 & acidosis

Clinical Risk Associated with RDSPrematurity (term & near- term))Gender
male > femalesandrogen- delayed surfactant maturation
Race- Black infants lower incidenceCesarean section- before onset of laborBirth depressionUncontrolled maternal diabetes- delayed
surfactant maturationGenetic- SP B deficiency/ more likely in
siblingsTwins- 2nd twin more likelyHypothermia- surfactant function impaired in
cold

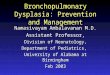
Respiratory Distress Syndrome (RDS)
Diffuse reticulogranular pattern, air bronchograms & atelectasis

Management of PPHN: Investigations
CBC with manual diffABGBMP,Glucose, Ca2+, Mg, LFTBlood Culture, viral studiesCoagulation profileCXREchoHUSRenal US

Management of PPHN: ObjectivesCorrect the underlying cause of PPHN (if
known)
Maintain adequate systemic BP
Decrease pulmonary vascular resistanceOxygenAlkalosis (at least avoid acidosis)iNO
Maintain optimal oxygen delivery to tissues
Minimize ventilator-induced lung injury

Management- PPHN
Proven therapy Unproven therapy
HyperventilationGentle ventilationAlkali infusionIV VasodilatorsHFVSurfactant*INOECMO
XXXXXX
XX
Therapeutic options for PPHN are varied with wide range of variations in their use

INO TherapyIndications PPHN or hypoxemic respiratory failureOI 15, reversible pulmonary disorderECHO -no evidence of CHDDosage : > 20ppm no additional benefit (optimal
lung inflation & adequate CO)Treatment Failure : OI >25 transfer, OI > 40
ECMODiscontinuation : OI < 10 , 2-6 days of iNOContraindications (No benefit in CDH)

Management of PPHN ECMO : Baseline ECMO criteria
≥ 34 weeksWt > 2000g (‘cannulas fit’)no major ICH on HUS (no > Gr II)reversible lung diseaseNo evidence of lethal congenital anomalies or
inoperable cardiac disease
UK trial impact of ECMO : survival ECMO group 68% compared to 41% in the control group

PPHN: Management SummaryConfirm Diagnosis
Echo helpful to rule out congenital heart disease, assess cardiac function
Maintain systemic BP and assist cardiac function as neededDopamineMilrinone
Oxygen & a conservative ventilation strategyaim for PaO2 60-90 mmHg
Modest hyperventilationpH 7.35-7.50, PaCO2 40-50mmHgAvoid acidosis
Sedatives as neededPhosphodiesterase inhibitorsSurfactant: consider in individual patientInhaled nitric oxideECMO for iNO non-respondersAlkali infusion & paralysis no longer first line
strategies

Post Recovery Issues & CareFeeding Problems
BPD
Withdrawal - narcotic
Neurological evaluation
Hearing exam

PROGNOSIS & FOLLOW-UPNINOS : INO not associated with an increase
in neurodevelopmental, behavioral or medical abnormalities at 2 yrs of age
Conservative Mx without induced alkalosis & paralysis : no hearing loss and good outcome (Marron et al)

PROGNOSIS & FOLLOW-UPMortality varies by diagnosisWith all available therapies MR < 20-25%MAS survival close to 100%CDH- survival variable
Morbidities linked to severity of clinical course, diagnosis and complicationsAt risk for neuro-developmental abnormalitiesHearing Loss: high risk of late onset sensorineural
hearing lossPulmonary recovery typically excellent if MASHigh risk for late pulmonary hypertension if CDH

REFERENCES
1. AAP, Committee on Fetus & Newborn Use of Inhaled NO. Peds, 2000;106(2).2. Clark RH, et al. Use of INO in Neonates with Hypoxemic Respiratory Failure. Summary of a Consensus Conference. Crit Care Int, 2000; 10:8-10.3. Walsh MC, et al. PPHN of the newborn. Rational therapy based on pathophysiology. Clin of Perin, 2001; 28(3).4. Walsh-Sukys MC, et al. PPHN of the newborn in the era before NO: Practice variation and outcomes. Peds, 2000; 105(1).5. Marron MJ, et al. Hearing and neurodevelopmental outcome in survivors of PPHN of the newborn. Peds, 1992;90(3).6. Ellington M, et al. Child health status, neurodevelopmental outcome and parental satisfaction in a RCT of NO for PPHN of the newborn. Peds, 2001;107(6).7. Steinhorn RH. PPHN- newborn. e-medicine (online).8. Keszler M, Durand DJ. Neonatal HFV. Clin of Perin, 2001; 28(3)9. Schumacher RE, Baumgart S. ECMO 2001. Clin of Perin, 2001;28(3).10. Abman S. Abnormal vasoreactivity in the pathophysiology of PPHN of the newborn. Neoreviews, Nov 1999.11. Konduri G. Modulation of NO release in perinatal lung. Neoreviews 2001; 2(3).12. Kinsella JP. Clinical trials of INO therapy in the newborn. Neoreviews, Nov 1999.13. Finer N, et al. INO in term & near term infants: Neurodevelopmental follow-up of the NINOS. J Peds, 2000;136(5).14. Davidson D, et al. Safety of withdrawing INO therapy in PPHN of the newborn. Peds, 1999; 31(4).15. Davidson D. INO for PPHN of the newborn : current evidence for safe and effective guidelines. Neonatal Respiratory Distress, 2000; 10(2).16. Steudel W, et al. INO : Basic biology and clinical applications. Anes, 1999; 91(4).17. Adams JM, Stark AR. Persistent Pulmonary Hypertension of the Newborn, Up to Date 2007.18.Steinhorn RH, Farrow KN. Pulmonary Hypertension in the Newborn. Neoreviews, Jan 2007.