Embed Size (px)
Citation preview
Senior Consultant Neonatology, Rainbow Children Hospital, Delhi.
Dr Naveen Parkash
Gupta
Areas of Interest - Ventilation, Hemodynamics, Care of ELBW
baby
MD Pediatrics, DNB Neonatology, Fellowship in Neonatology (BC
Children Hospital, Vancouver)
Recent Concepts in
Management of RDSDr Naveen Gupta
MD Pediatrics, DNB Neonatology
Fellowship in Neonatology (BC Children Hospital, Vancouver)
Senior Consultant Neonatology
Rainbow Children Hospital, Delhi.
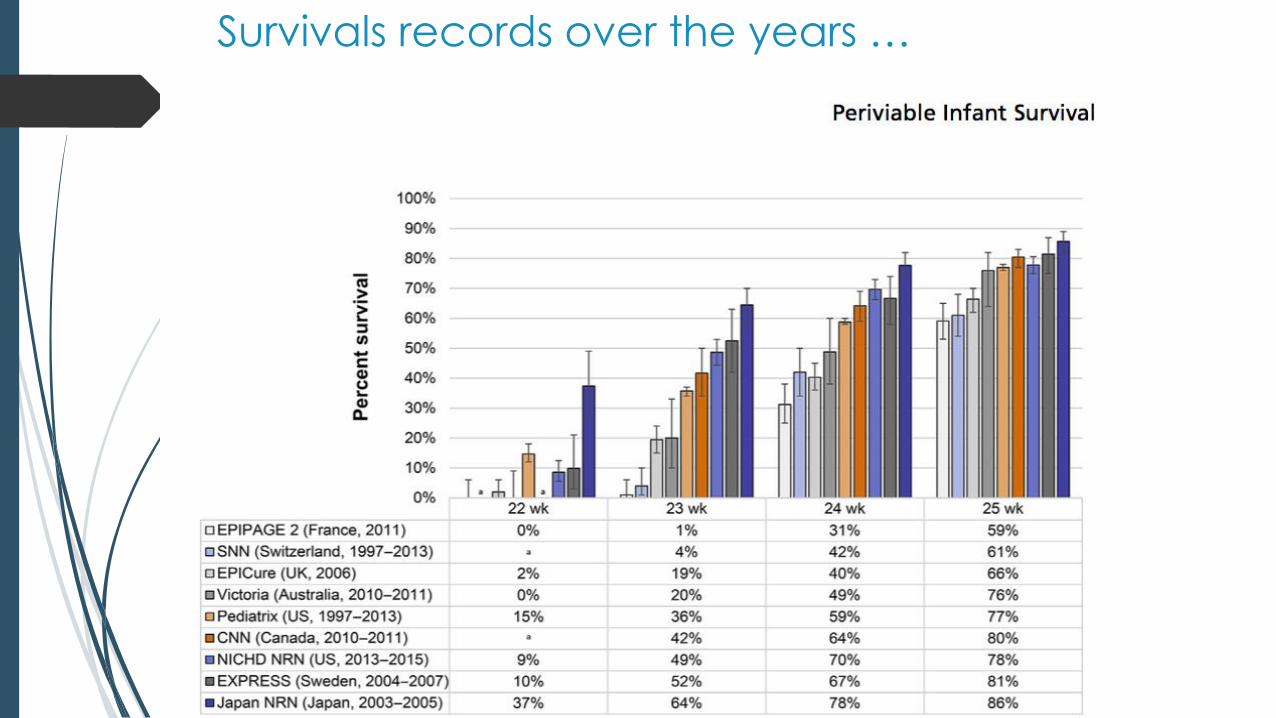
Survivals records over the years …
How common is RDS?
In 2017, VON analyzed data of 8156 babies from
across Europe:
≤ 24 weeks:90% risk of RDS
At 28 weeks:80% risk of RDS
Surfactant required for 55% of VLBW babies
27% in the DR & 29% beyond 2 hrs
of life
18% of VLBW – Bronchopulmonary Dysplasia
(BPD)
Kjell Helenius, MD. PEDIATRICS Volume 140, number 6, December 2017
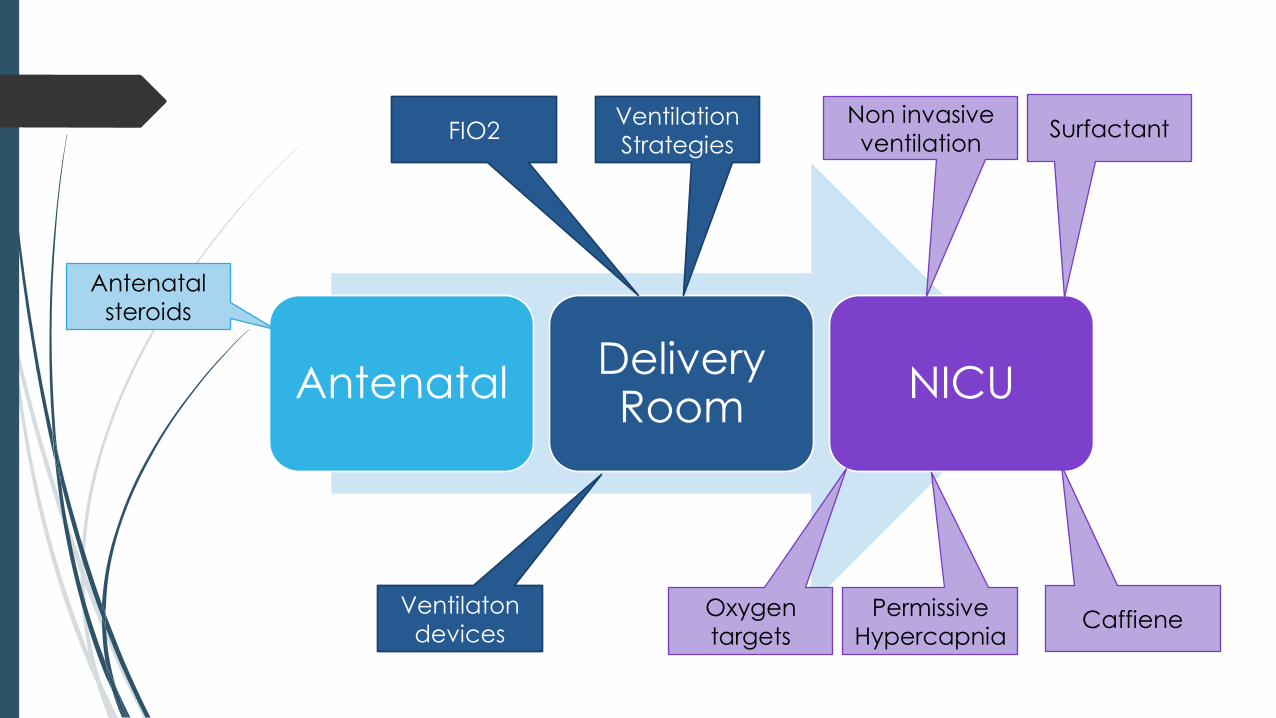
Antenatal Delivery Room
NICU
Antenatal
steroids
FIO2Ventilation
Strategies
Non invasive
ventilationSurfactant
Oxygen
targets
Permissive
HypercapniaCaffiene
Ventilaton
devices
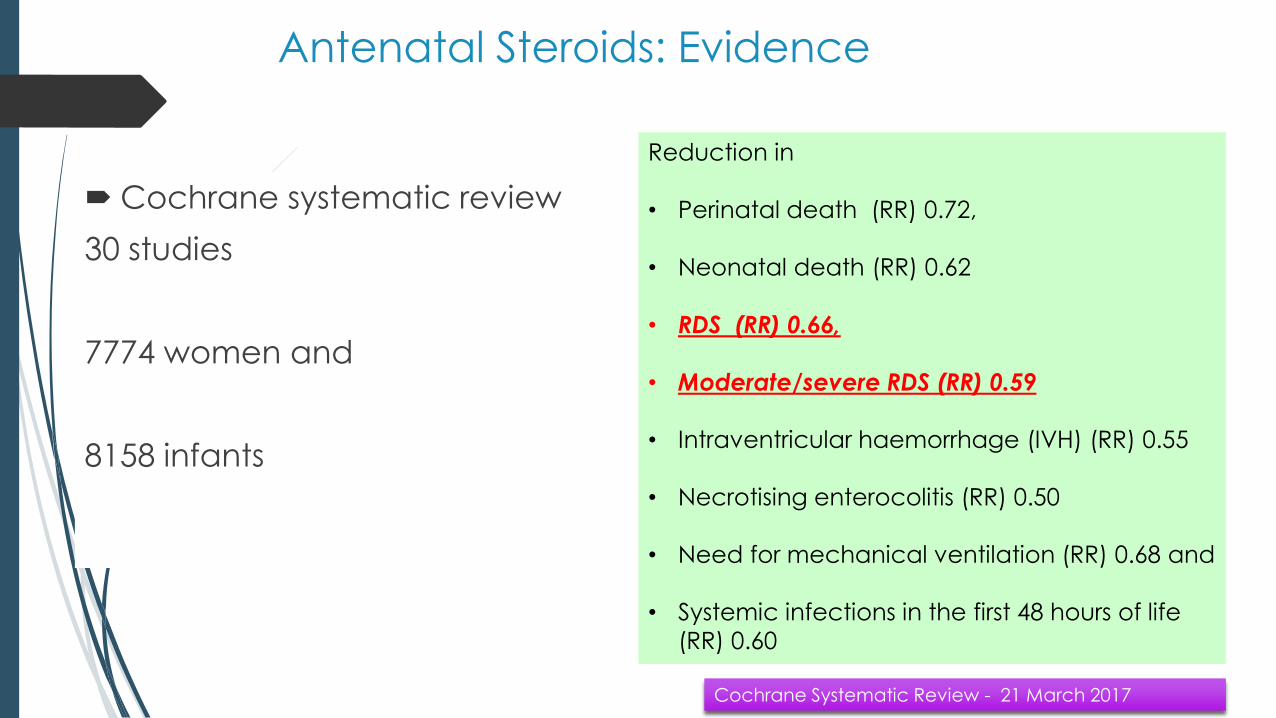
Cochrane systematic review
30 studies
7774 women and
8158 infants
Reduction in
• Perinatal death (RR) 0.72,
• Neonatal death (RR) 0.62
• RDS (RR) 0.66,
• Moderate/severe RDS (RR) 0.59
• Intraventricular haemorrhage (IVH) (RR) 0.55
• Necrotising enterocolitis (RR) 0.50
• Need for mechanical ventilation (RR) 0.68 and
• Systemic infections in the first 48 hours of life
(RR) 0.60
Cochrane Systematic Review - 21 March 2017
Antenatal Steroids: Evidence
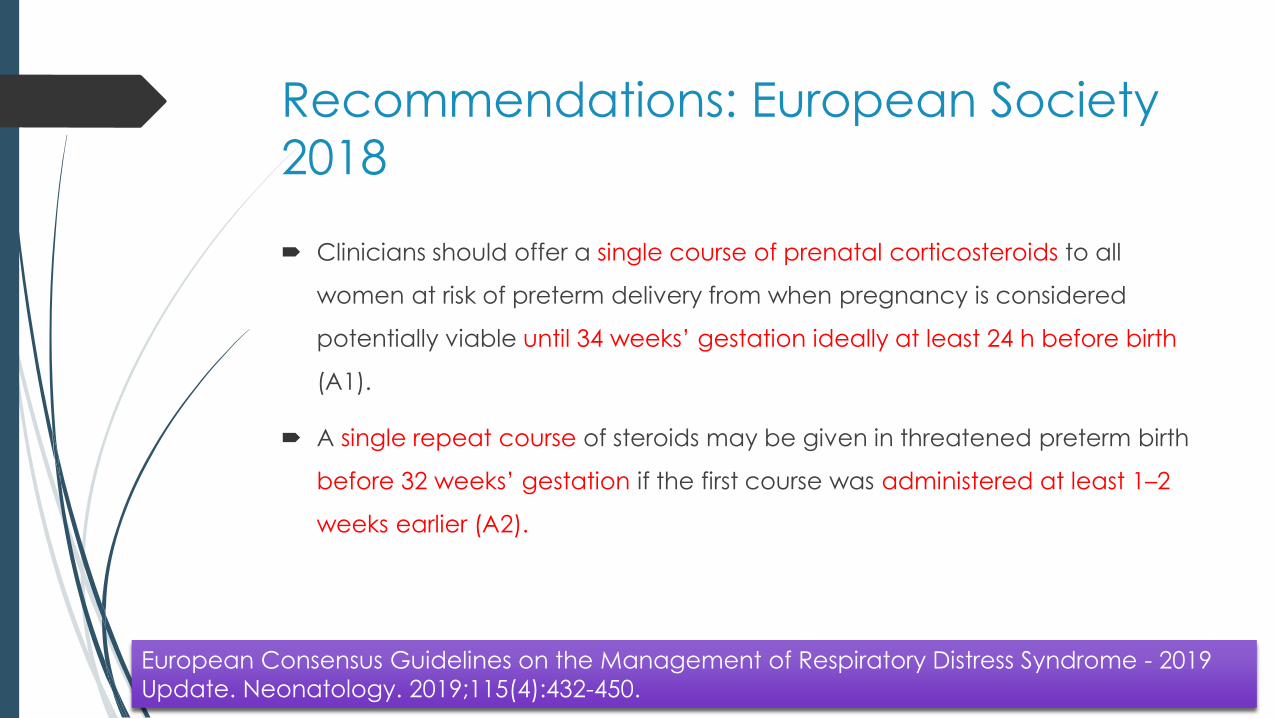
Recommendations: European Society
2018
Clinicians should offer a single course of prenatal corticosteroids to all
women at risk of preterm delivery from when pregnancy is considered
potentially viable until 34 weeks’ gestation ideally at least 24 h before birth
(A1).
A single repeat course of steroids may be given in threatened preterm birth
before 32 weeks’ gestation if the first course was administered at least 1–2
weeks earlier (A2).
European Consensus Guidelines on the Management of Respiratory Distress Syndrome - 2019
Update. Neonatology. 2019;115(4):432-450.
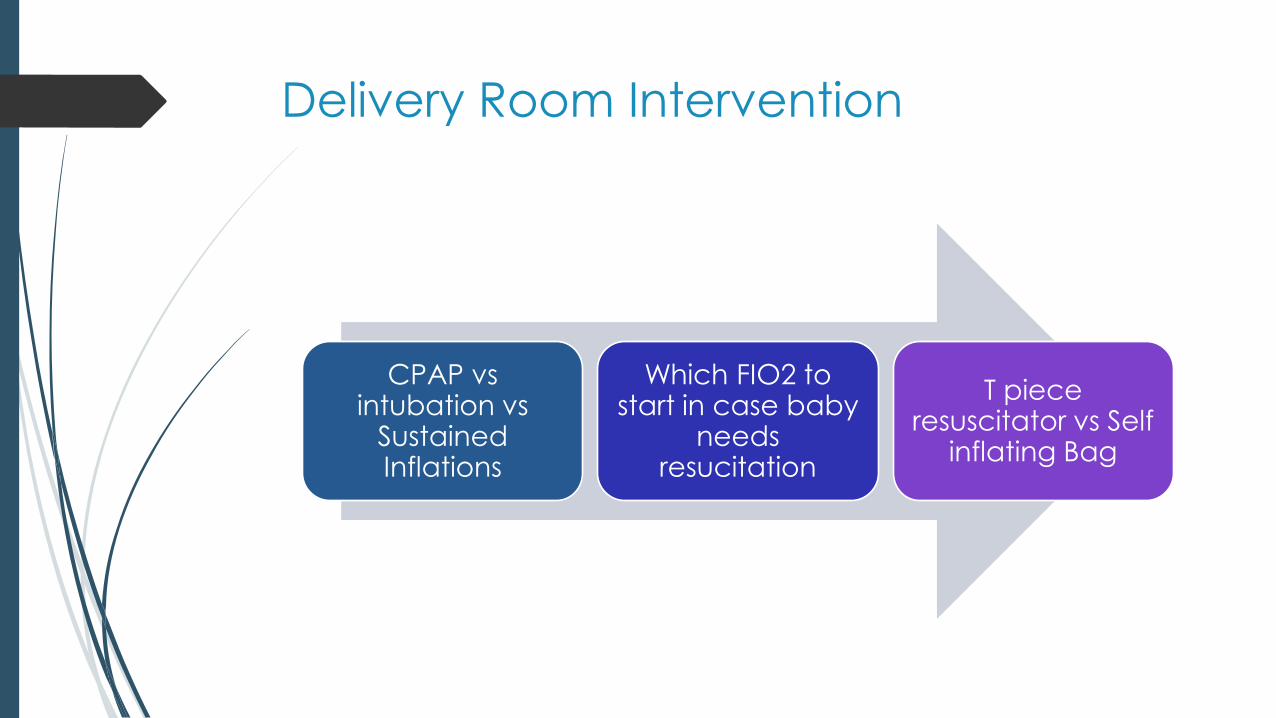
Delivery Room Intervention
CPAP vs intubation vs
Sustained Inflations
Which FIO2 to start in case baby
needs resucitation
T piece resuscitator vs Self
inflating Bag
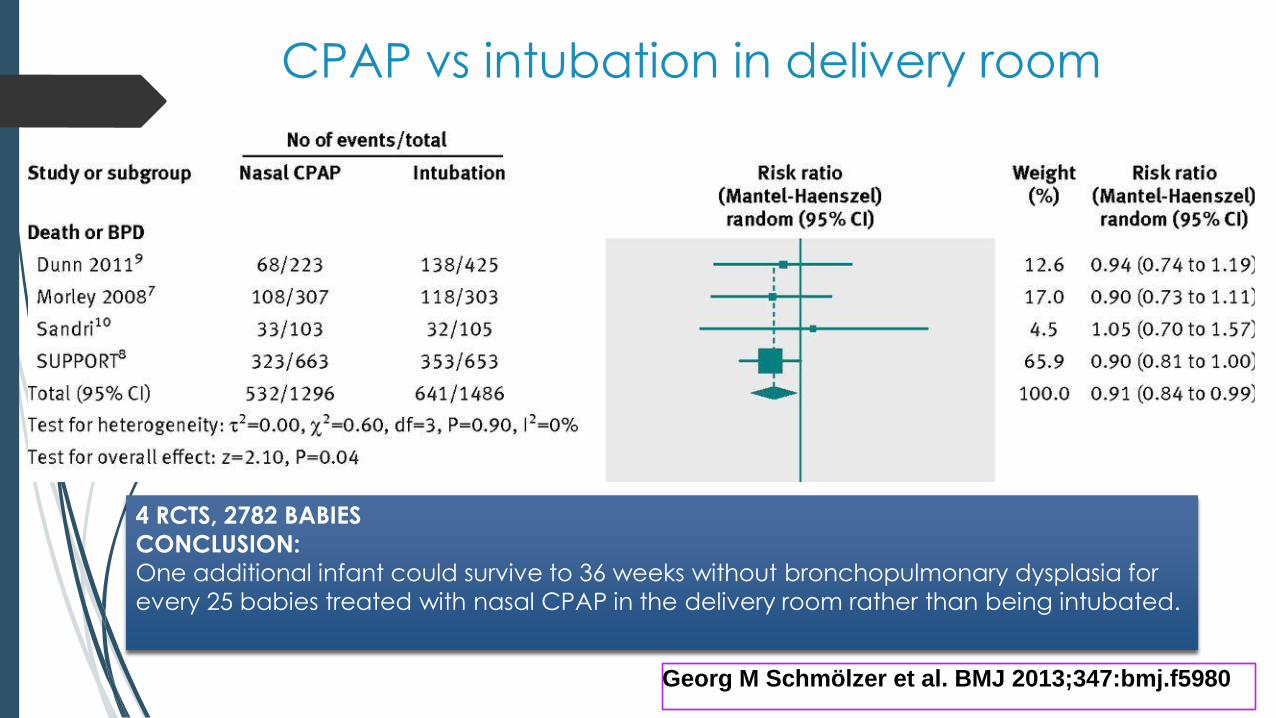
Georg M Schmölzer et al. BMJ 2013;347:bmj.f5980
CPAP vs intubation in delivery room
4 RCTS, 2782 BABIES
CONCLUSION:
One additional infant could survive to 36 weeks without bronchopulmonary dysplasia for
every 25 babies treated with nasal CPAP in the delivery room rather than being intubated.
Study design and characteristics
23 weeks to 26+6 weeks
Were eligible if they require PPV because of inadequate respiratory effort or
HR < 100/min
Sample size – 600 babies
Trial stopped early after enrollment of 426 babies.
Primary Outcome – Death or BPD
Delivery Room Intervention
Which FIO2 to start in case baby needs resucitation
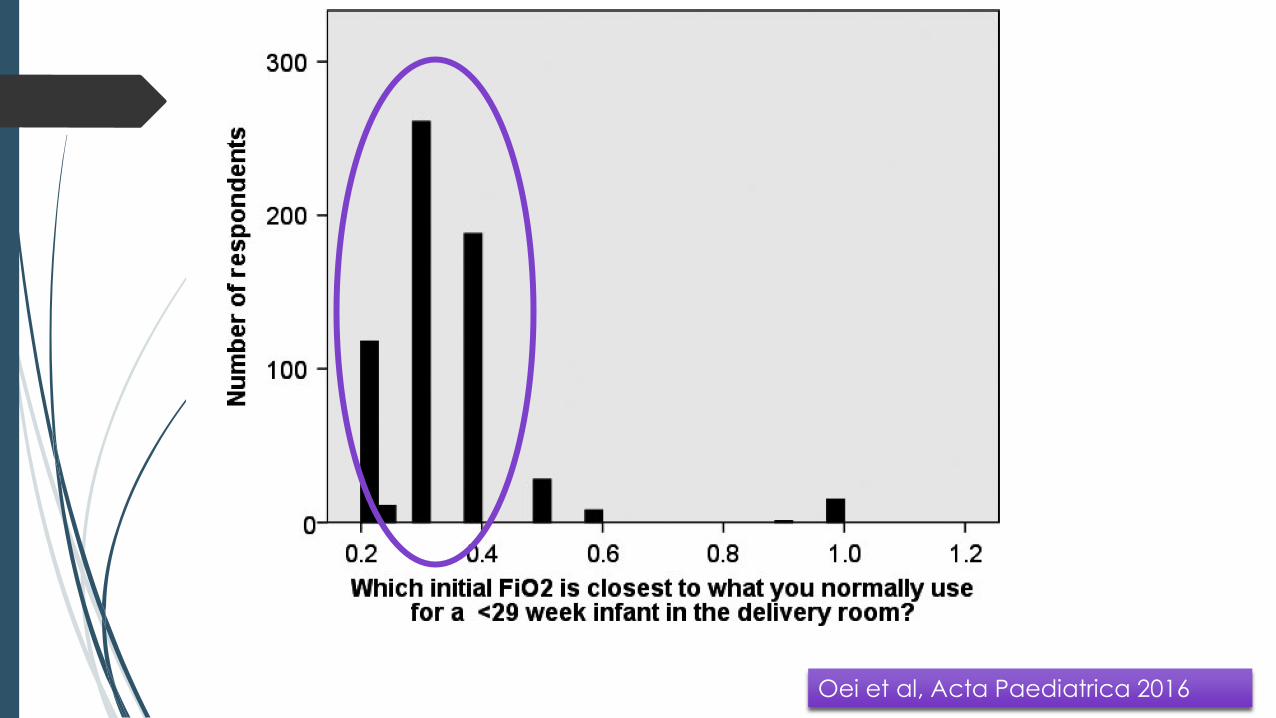
Oei et al, Acta Paediatrica 2016
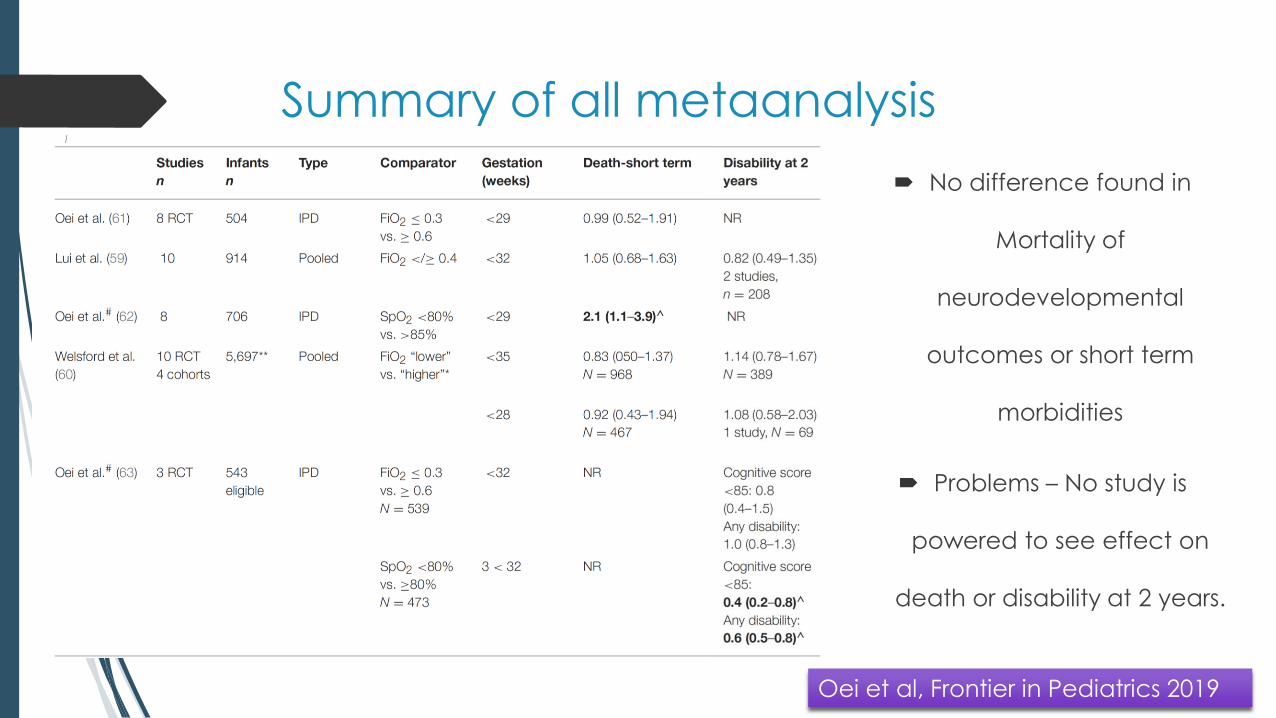
Summary of all metaanalysis
No difference found in
Mortality of
neurodevelopmental
outcomes or short term
morbidities
Problems – No study is
powered to see effect on
death or disability at 2 years.
Oei et al, Frontier in Pediatrics 2019
TO2RPEDO trial
292 babies (<32 wks) were recruited to either room air or
100% O2 which were adjusted to target pulse oximetry of
65 to 95% at 5 min and 85% to 95% until NICU admission
Trial stopped early
Babies < 28 weeks have higher mortality in room air
group (22% vs 6% RR 3.9 (95%CI 1.1-13.4)
It was not a prespecified outcome
Oei et al, Pediatrics 2017

Delivery Room Intervention
T piece resuscitator vs Self inflating Bag
T piece vs Self inflating Bag
1027 babies ≥ 26 weeks gestational age – cluster randomized 2 period cross
over trial
Primary outcome – proportions of newborns with HR ≥ 100/min at 2 min after
birth
Results
Primary outcome same
Less intubations in T piece group as compared to self inflating group.
Szyld E, J Pediatr. 2014 Aug;165(2):234-239.e3.
T piece vs self inflating Bag: Indian
Data
90 babies ≥ 26 week gestation
Quasi randomized trial
Results
Duration of PPV significantly less in TPR group (30 vs 60 sec, p < 0.001)
Higher proportion of babies could be resuscitated with room air only (72.5% vs
38%)
Fewer neonates resuscitated with T piece required invasive ventilation
Thakur et al. Resuscitation. 2015 May;90:21-4.
Recommendations: Delivery Room
Stabilization
1. Gently support breathing using CPAP if possible, and if inflations are
needed avoid excessive tidal volumes.
2. Intubation at birth should be considered only for those not
responding to the above
3. Pulse oximetry can help guide heart rate response to stabilisation.
Start with 21–30% oxygen for 28–31 weeks’ GA and 30% oxygen for
<28 weeks’ GA and titrate up or down as needed according to
SpO2 targets Aim at SpO2 of 80% or more within 5 min.
European Consensus Guidelines on the Management of Respiratory Distress Syndrome - 2019
Update. Neonatology. 2019;115(4):432-450.
NICU Care
Non invasive mode
Which one
If at all ventilate
then volume or pressure
Surfactant
Saturations and
PaCO2 targets
CaffienePost natal
steroids
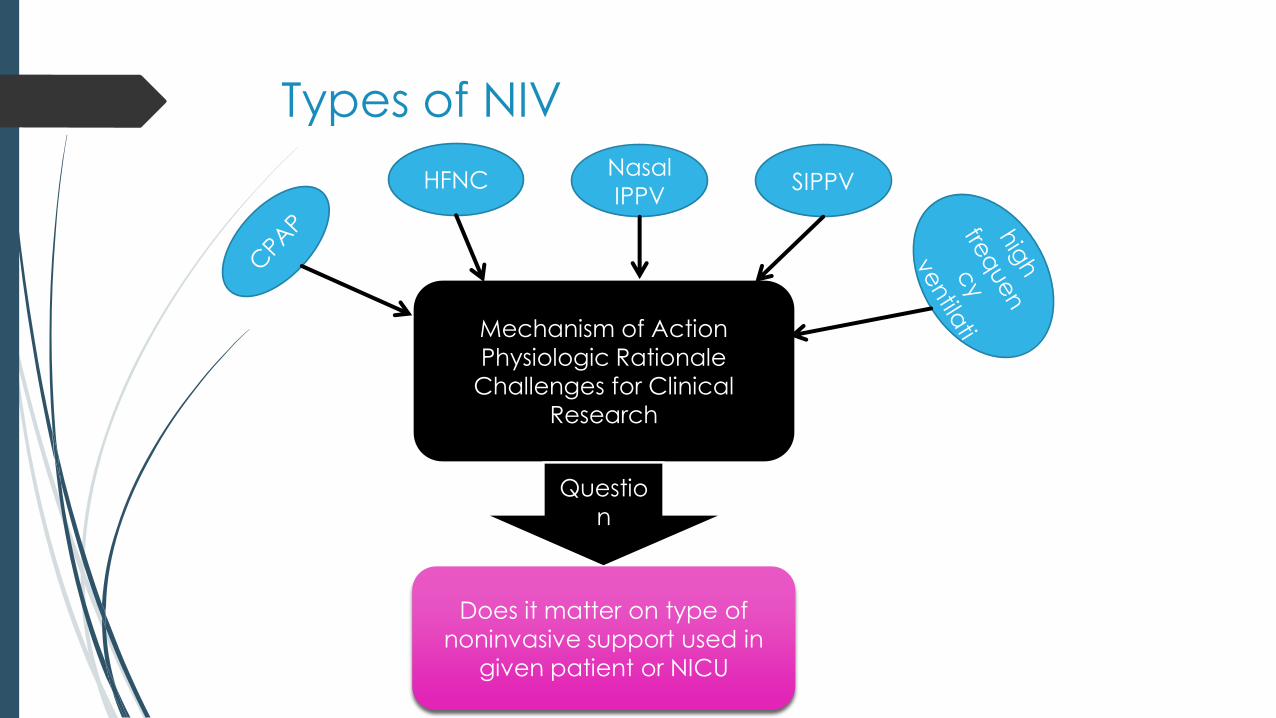
Mechanism of Action
Physiologic Rationale
Challenges for Clinical
Research
Questio
n
Does it matter on type of
noninvasive support used in
given patient or NICU
HFNCNasal
IPPVSIPPV
Types of NIV
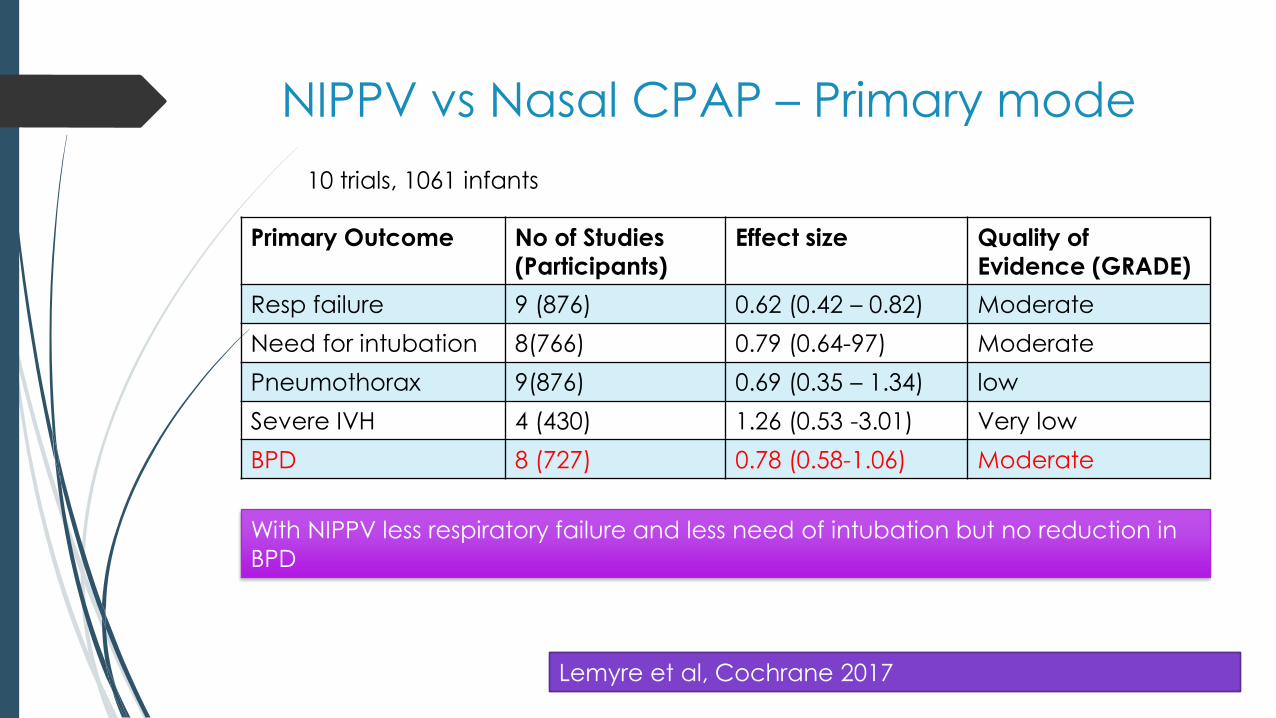
NIPPV vs Nasal CPAP – Primary mode
Primary Outcome No of Studies
(Participants)
Effect size Quality of
Evidence (GRADE)
Resp failure 9 (876) 0.62 (0.42 – 0.82) Moderate
Need for intubation 8(766) 0.79 (0.64-97) Moderate
Pneumothorax 9(876) 0.69 (0.35 – 1.34) low
Severe IVH 4 (430) 1.26 (0.53 -3.01) Very low
BPD 8 (727) 0.78 (0.58-1.06) Moderate
10 trials, 1061 infants
Lemyre et al, Cochrane 2017
With NIPPV less respiratory failure and less need of intubation but no reduction in
BPD
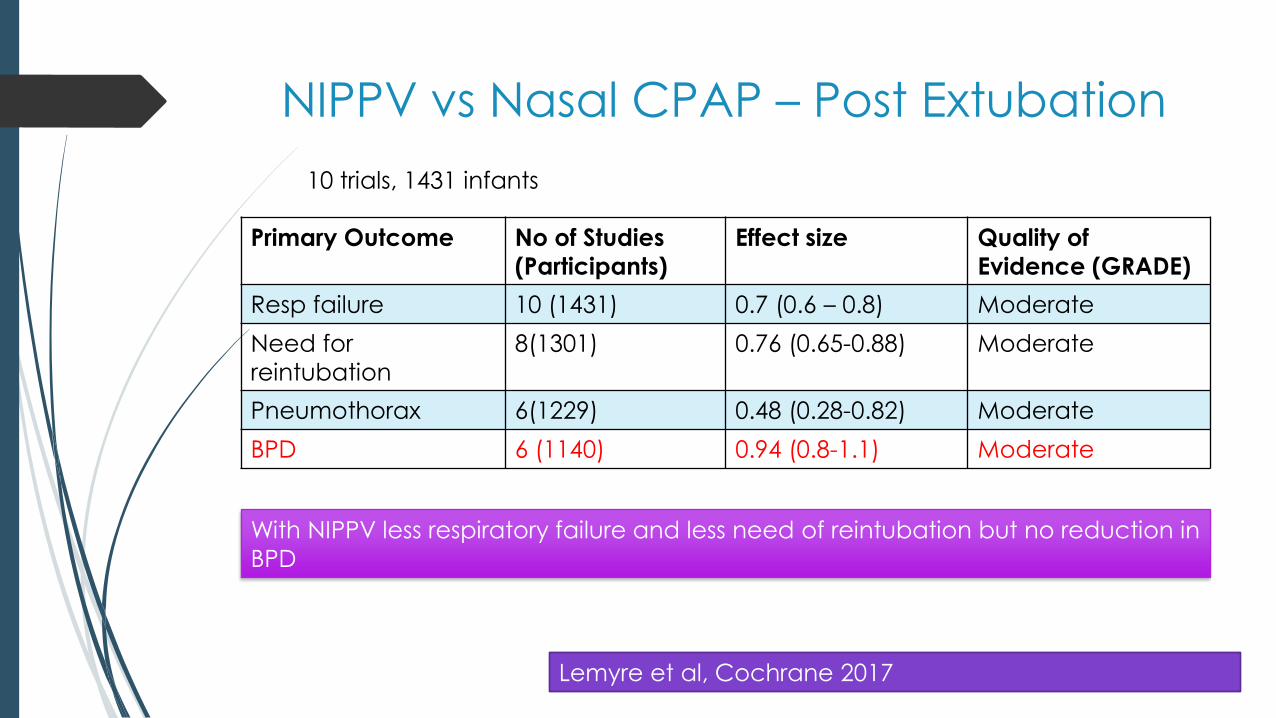
NIPPV vs Nasal CPAP – Post Extubation
Primary Outcome No of Studies
(Participants)
Effect size Quality of
Evidence (GRADE)
Resp failure 10 (1431) 0.7 (0.6 – 0.8) Moderate
Need for
reintubation
8(1301) 0.76 (0.65-0.88) Moderate
Pneumothorax 6(1229) 0.48 (0.28-0.82) Moderate
BPD 6 (1140) 0.94 (0.8-1.1) Moderate
10 trials, 1431 infants
Lemyre et al, Cochrane 2017
With NIPPV less respiratory failure and less need of reintubation but no reduction in
BPD
CPAP The Gold
Standard
HFNC The Contender
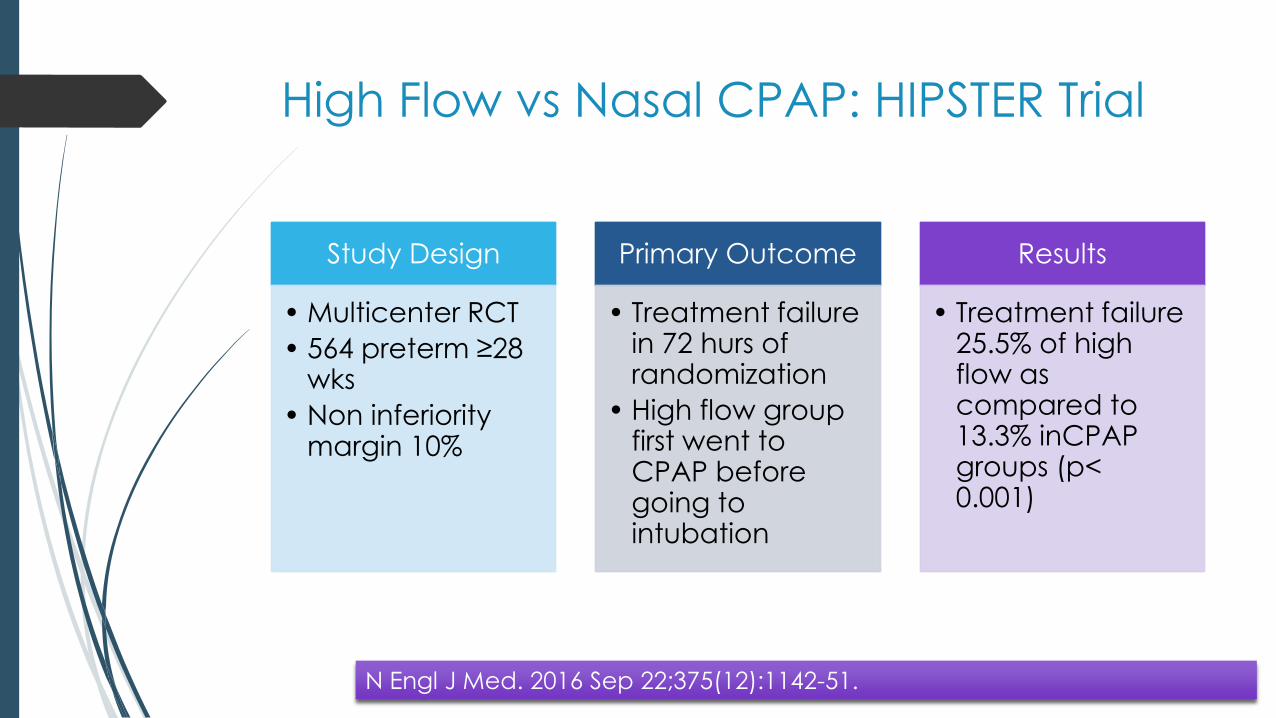
High Flow vs Nasal CPAP: HIPSTER Trial
Study Design
• Multicenter RCT
• 564 preterm ≥28 wks
• Non inferiority margin 10%
Primary Outcome
• Treatment failure in 72 hurs of randomization
• High flow group first went to CPAP before going to intubation
Results
• Treatment failure 25.5% of high flow as compared to 13.3% inCPAPgroups (p< 0.001)
N Engl J Med. 2016 Sep 22;375(12):1142-51.
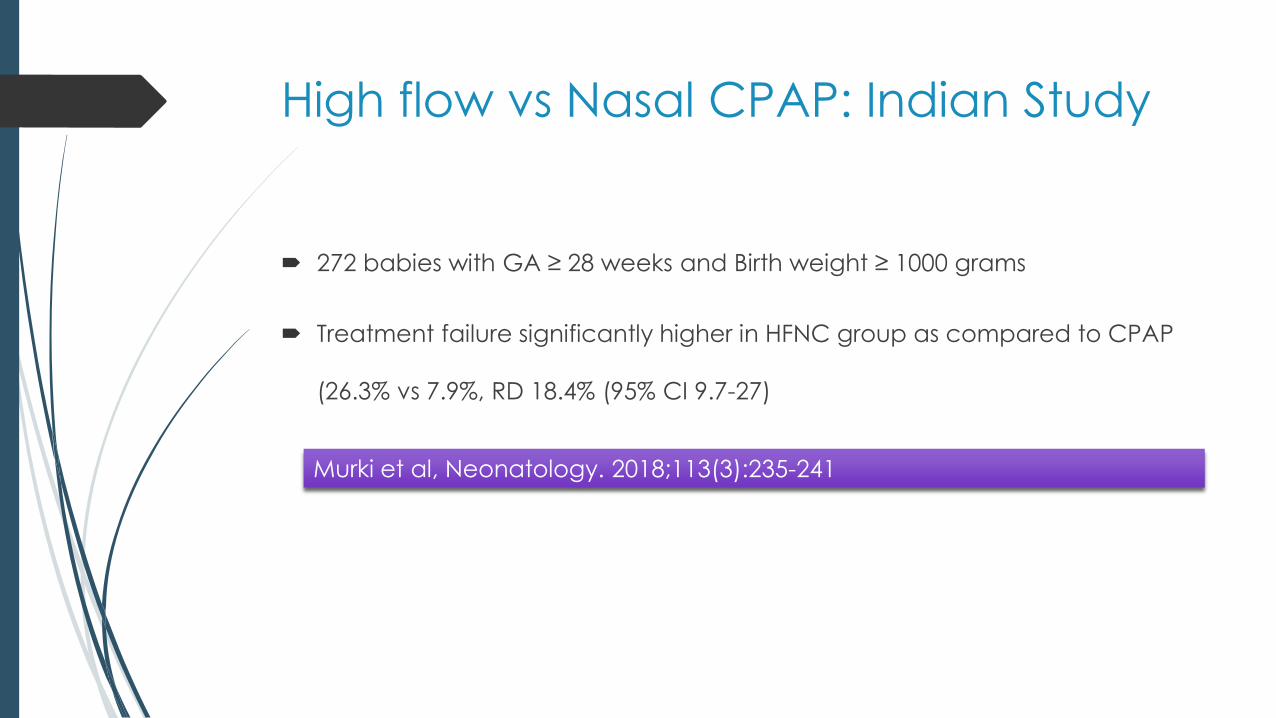
High flow vs Nasal CPAP: Indian Study
272 babies with GA ≥ 28 weeks and Birth weight ≥ 1000 grams
Treatment failure significantly higher in HFNC group as compared to CPAP
(26.3% vs 7.9%, RD 18.4% (95% CI 9.7-27)
Murki et al, Neonatology. 2018;113(3):235-241
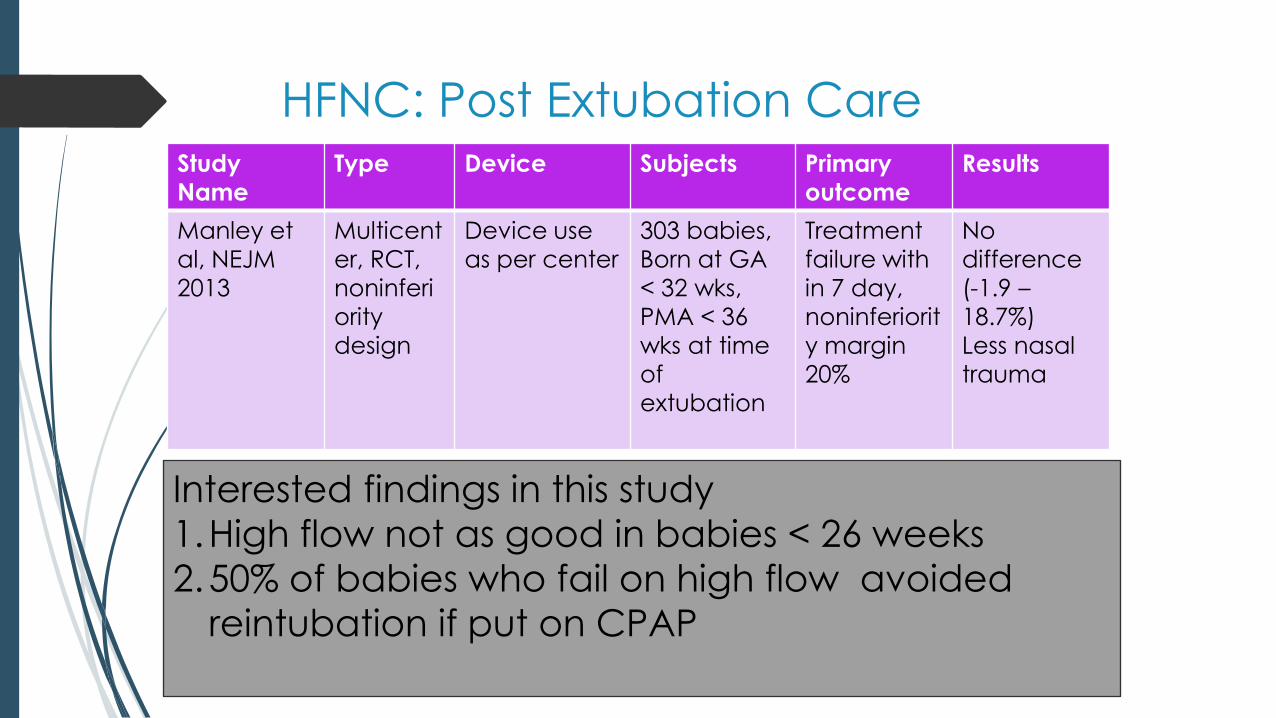
HFNC: Post Extubation CareStudy
Name
Type Device Subjects Primary
outcome
Results
Manley et
al, NEJM
2013
Multicent
er, RCT,
noninferi
ority
design
Device use
as per center
303 babies,
Born at GA
< 32 wks,
PMA < 36
wks at time
of
extubation
Treatment
failure with
in 7 day,
noninferiorit
y margin
20%
No
difference
(-1.9 –
18.7%)
Less nasal
trauma
Interested findings in this study
1.High flow not as good in babies < 26 weeks
2.50% of babies who fail on high flow avoided
reintubation if put on CPAP
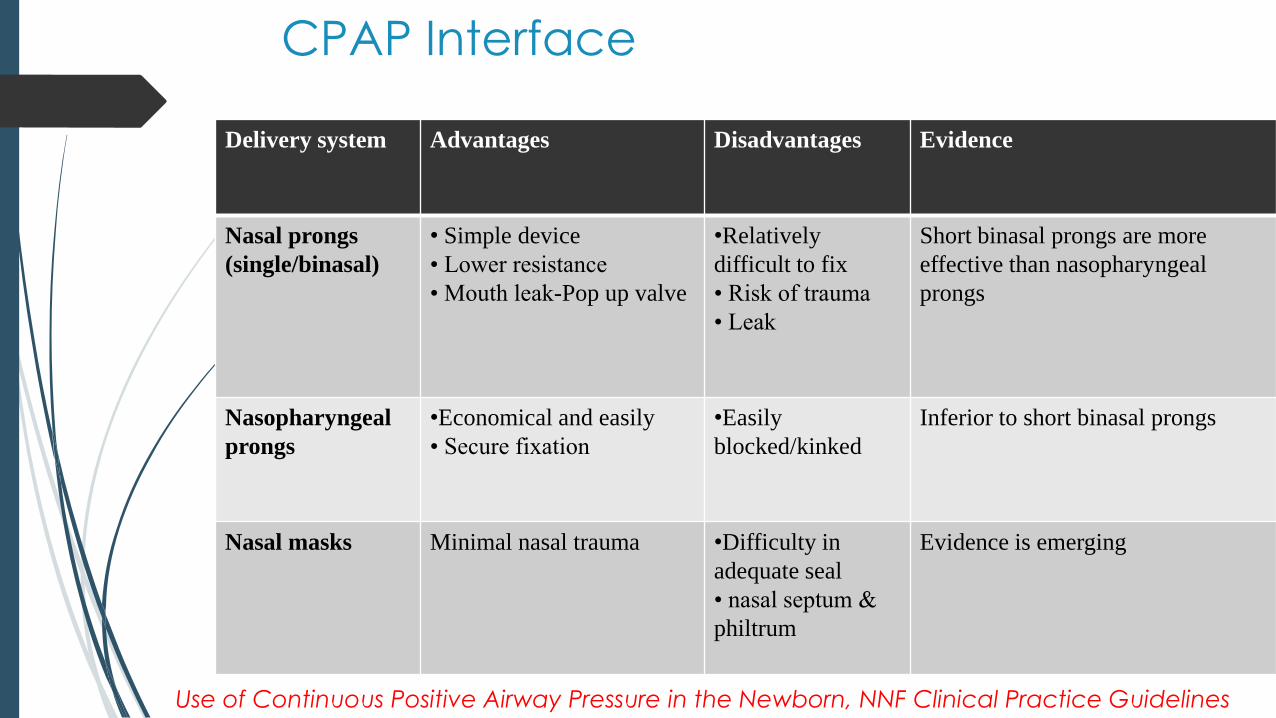
CPAP Interface
Delivery system Advantages Disadvantages Evidence
Nasal prongs
(single/binasal)
• Simple device
• Lower resistance
• Mouth leak-Pop up valve
•Relatively
difficult to fix
• Risk of trauma
• Leak
Short binasal prongs are more
effective than nasopharyngeal
prongs
Nasopharyngeal
prongs
•Economical and easily
• Secure fixation
•Easily
blocked/kinked
Inferior to short binasal prongs
Nasal masks Minimal nasal trauma •Difficulty in
adequate seal
• nasal septum &
philtrum
Evidence is emerging
Use of Continuous Positive Airway Pressure in the Newborn, NNF Clinical Practice Guidelines
Devices and pressure sources for administration of nasal continuous positive
airway pressure (NCPAP) in preterm neonates (Review) De Paoli AG, Davis
PG, Faber B, Morley CJ
Review content assessed as up-to-date: 30 August 2007.
Short binasal prongs are more effective at preventing
re-intubation than single nasal or nasopharyngeal
prongs
RR 0.59 (CI: 0.41, 0.85)
Short Bi-nasal Prongs are more effective
CPAP Interface
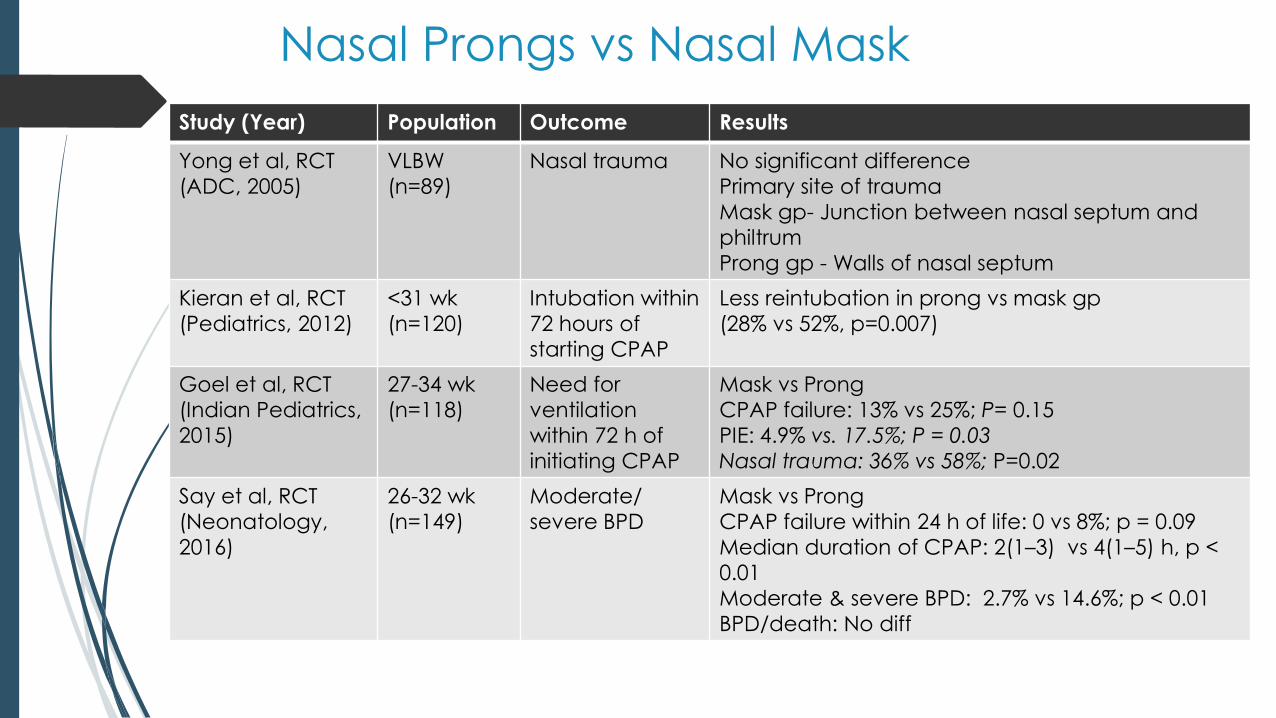
Nasal Prongs vs Nasal Mask
Study (Year) Population Outcome Results
Yong et al, RCT
(ADC, 2005)
VLBW
(n=89)
Nasal trauma No significant difference
Primary site of trauma
Mask gp- Junction between nasal septum and
philtrum
Prong gp - Walls of nasal septum
Kieran et al, RCT
(Pediatrics, 2012)
<31 wk
(n=120)
Intubation within
72 hours of
starting CPAP
Less reintubation in prong vs mask gp
(28% vs 52%, p=0.007)
Goel et al, RCT
(Indian Pediatrics,
2015)
27-34 wk
(n=118)
Need for
ventilation
within 72 h of
initiating CPAP
Mask vs Prong
CPAP failure: 13% vs 25%; P= 0.15
PIE: 4.9% vs. 17.5%; P = 0.03
Nasal trauma: 36% vs 58%; P=0.02
Say et al, RCT
(Neonatology,
2016)
26-32 wk
(n=149)
Moderate/
severe BPD
Mask vs Prong
CPAP failure within 24 h of life: 0 vs 8%; p = 0.09
Median duration of CPAP: 2(1–3) vs 4(1–5) h, p <
0.01
Moderate & severe BPD: 2.7% vs 14.6%; p < 0.01
BPD/death: No diff
NIV: Recommendations
CPAP is modality of choice in preterm babies < 30 weeks at risk of RDS
Data is supportive for NIPPV to be used both as primary mode and in post
extubation phase
Starting CPAP can be 6 to 9 cm H2O
Delivery systems doesnot matter – Bubble CPAP being low cost device can
be preferred system.
During weaning HFNC can be used as an alternative to nasal CPAP for
some babies with advantage of less nasal trauma
European Consensus Guidelines on the Management of Respiratory Distress Syndrome - 2019
Update. Neonatology. 2019;115(4):432-450.
NICU Care: Surfactant
Best mode of administration
Nebulized Surfactant
Surfactant + Budesonide
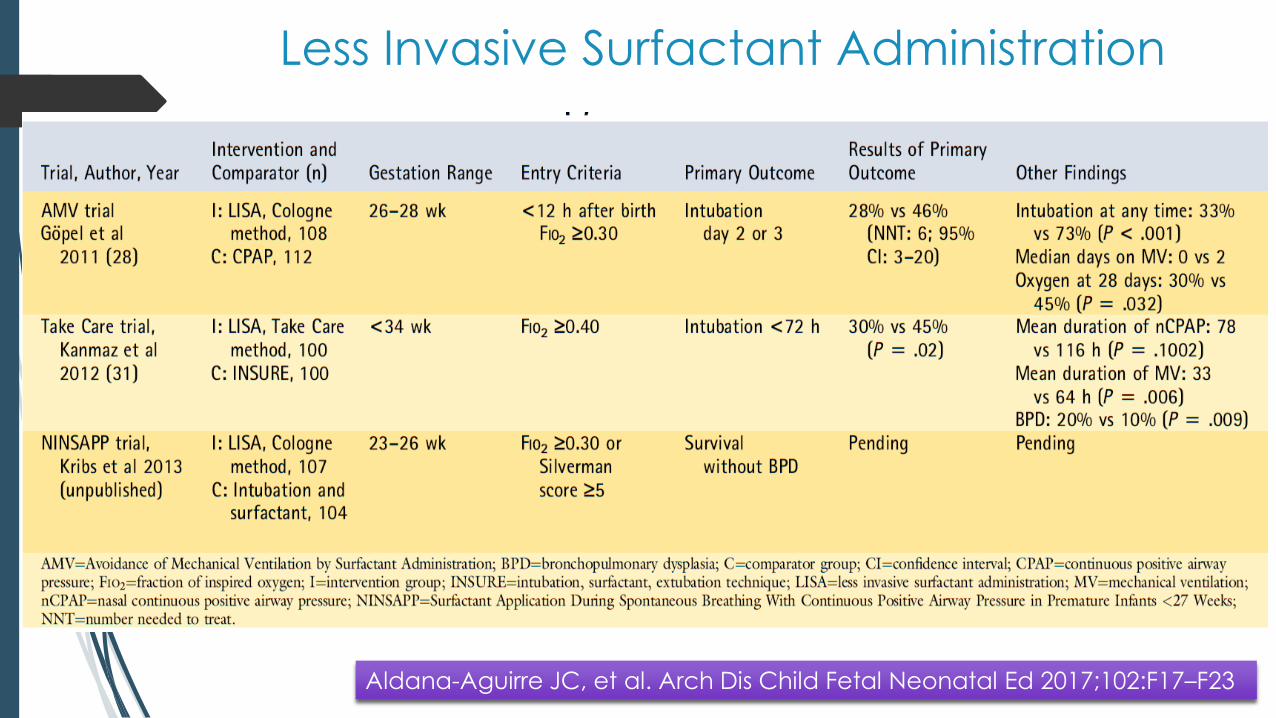
Aldana-Aguirre JC, et al. Arch Dis Child Fetal Neonatal Ed 2017;102:F17–F23
Less Invasive Surfactant Administration
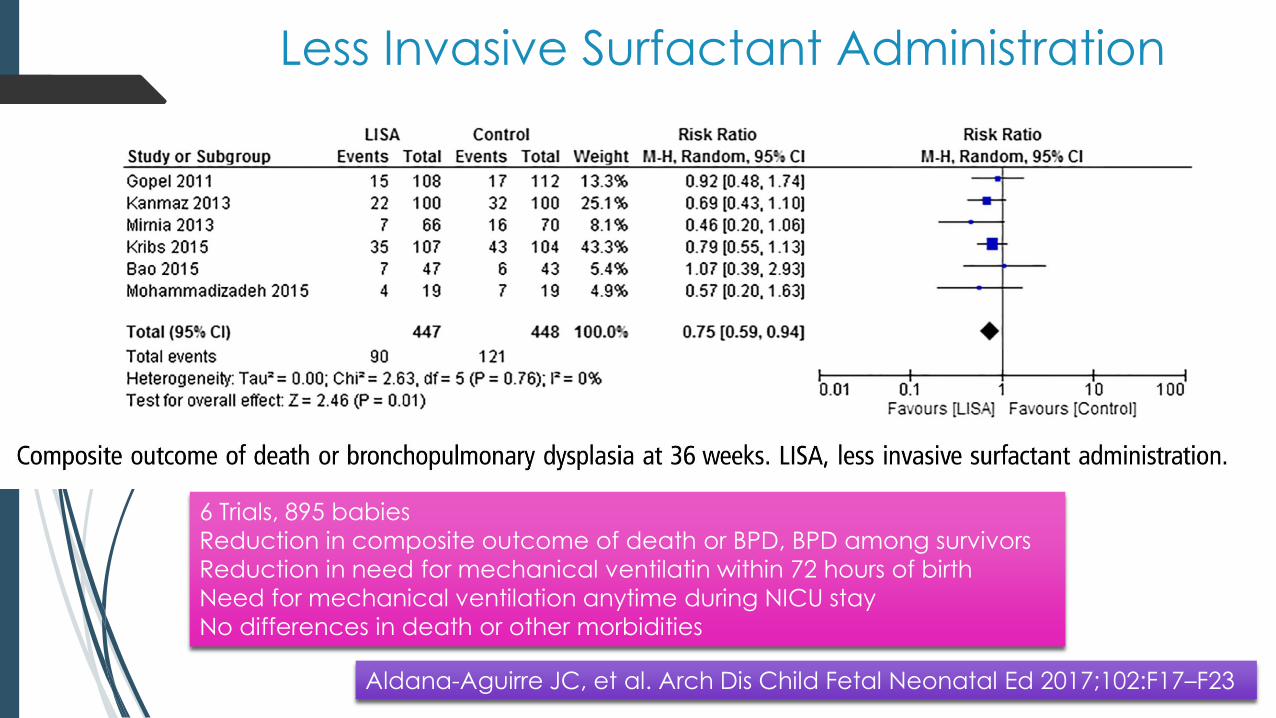
Less Invasive Surfactant Administration
6 Trials, 895 babies
Reduction in composite outcome of death or BPD, BPD among survivors
Reduction in need for mechanical ventilatin within 72 hours of birth
Need for mechanical ventilation anytime during NICU stay
No differences in death or other morbidities
Aldana-Aguirre JC, et al. Arch Dis Child Fetal Neonatal Ed 2017;102:F17–F23
Sur E or In Sur E
4 centers
Preterm babies < 34 weeks with RDS requiring CPAP were
either given surfactant by SurE (without intubation) or In
Sur E (with intubation)
175 babies in each group.
Need for MV in first 72 hours significantly low in Sur E
group (19% vs 40%, p < .01)
BPD was also significantly less
Jeena,et al. Pediatr Pulmonol. 2019 Nov;54(11):1747-1752.
Unanswered Questions with LISA
Need for sedation/analgesia
Fear of regurgitation of surfactant
Different studies have used different catheters (no comaprision yet)
Can we be more non invasive (Nebulized Surfactant)
European Consensus Guidelines on the Management of Respiratory Distress Syndrome - 2019
Update. Neonatology. 2019;115(4):432-450.


Study design
•RCT single centerin Australia
•Preterm 29 to 33 weeks < 4 hrs requiring 22 – 30% O2
Intervention
•Randomized to Bubble CPAP or Bubble CPAP with nebulized poractant (200 mg/kg) using a customised vibrating membrane nebuliser (eFlowneonatal)
Results
•64 babies
•Reduced need of intubation with in 72 hours
•Conclusion
•Nebulized surfactant reduces need of intubation in 72 hrs in babies with mild RDS
Minocchieri S, et al. Arch Dis Child Fetal Neonatal Ed 2018;0:F1–F7.
Surfactant: Recommendations
Animal derived surfactant
When – FIO2 needs > 30% on nasal CPAP
How – LISA
Which one – Poractant alpha in dose of 200 mg/kg is superior than
Poractant alpha 100 mg/kg or Beractant 100 mg/kg
Early rescue
If baby needs intubation in delivery room, give it as early as possible.
European Consensus Guidelines on the Management of Respiratory Distress Syndrome - 2019
Update. Neonatology. 2019;115(4):432-450.
What happens when our earnest efforts
go in vain and baby is intubated?
Can we still improve outcomes?
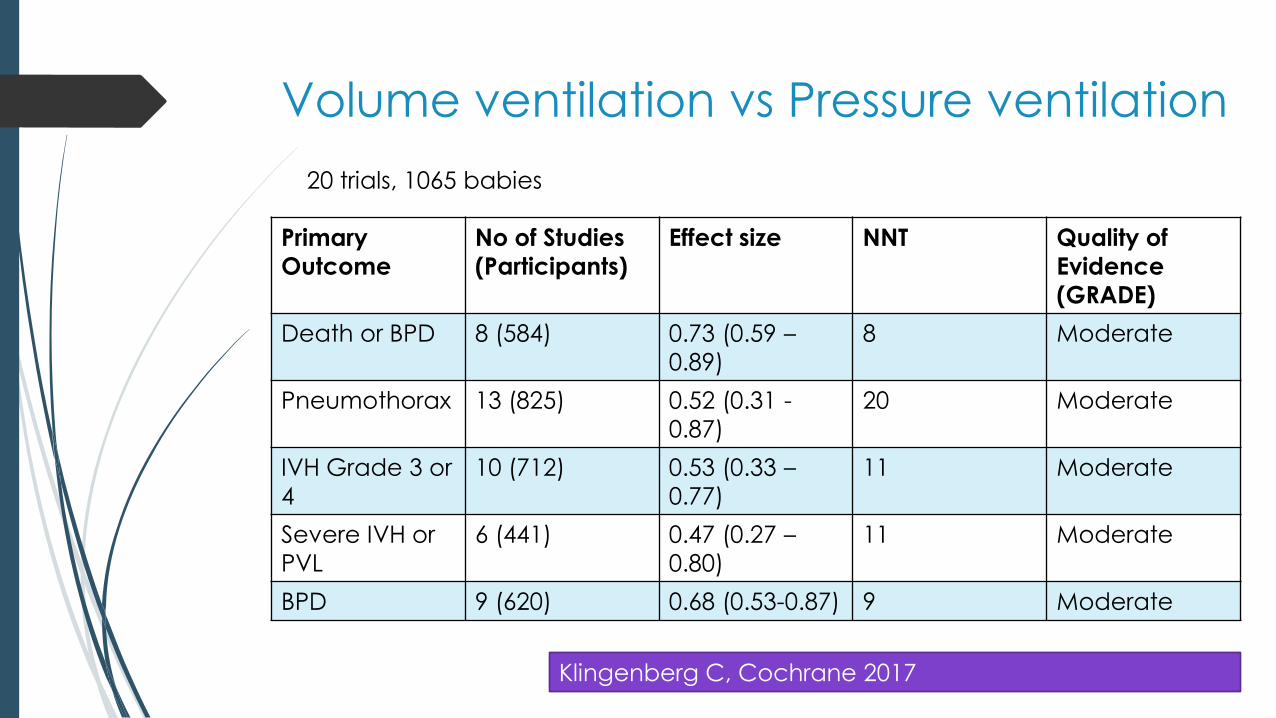
Volume ventilation vs Pressure ventilation
Primary
Outcome
No of Studies
(Participants)
Effect size NNT Quality of
Evidence
(GRADE)
Death or BPD 8 (584) 0.73 (0.59 –
0.89)
8 Moderate
Pneumothorax 13 (825) 0.52 (0.31 -
0.87)
20 Moderate
IVH Grade 3 or
4
10 (712) 0.53 (0.33 –
0.77)
11 Moderate
Severe IVH or
PVL
6 (441) 0.47 (0.27 –
0.80)
11 Moderate
BPD 9 (620) 0.68 (0.53-0.87) 9 Moderate
20 trials, 1065 babies
Klingenberg C, Cochrane 2017
HFOV vs Conventional as primary
mode of RDS
19 studies, 4096 infants
No difference found in important outcomes.
At present consensus is put baby on conventional
mode first
Use HFOV as rescue therapy.
Cools F, Cochrane 2015
NICU Care
Non invasive mode Which
one
If at all ventilate
then volume or pressure
SurfactantSaturations and PaCO2
targetsCaffiene
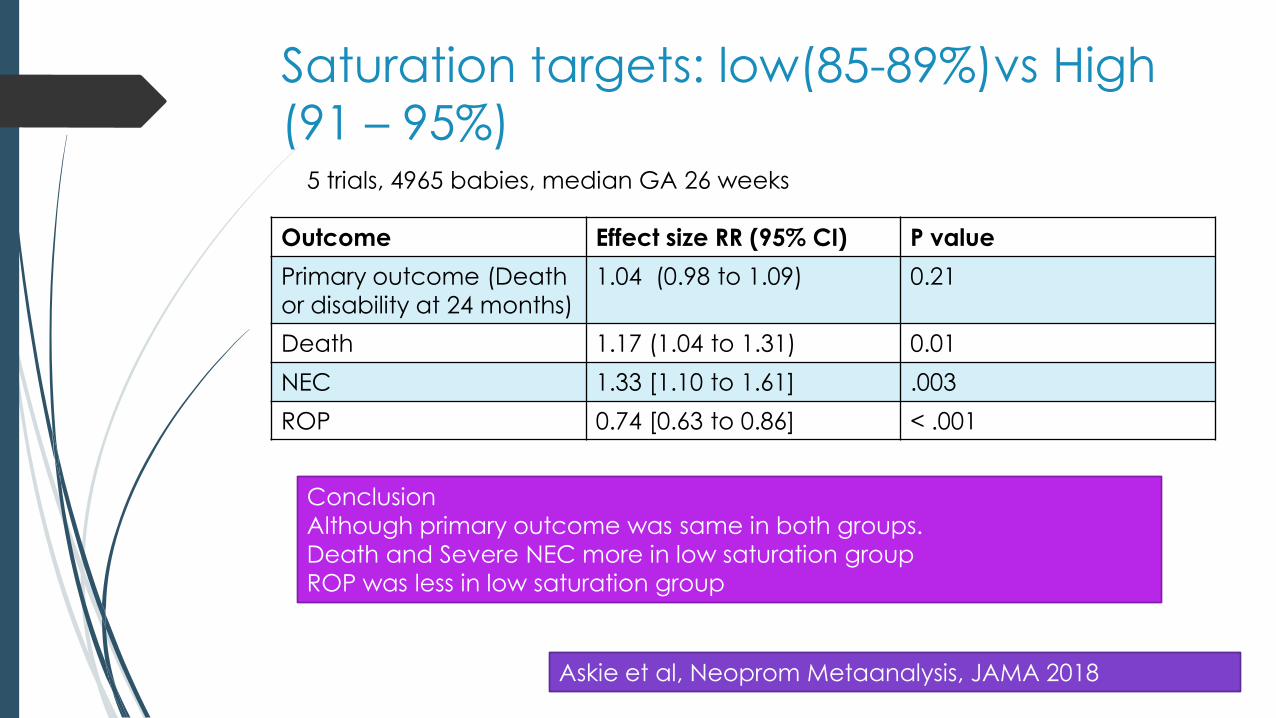
Saturation targets: low(85-89%)vs High
(91 – 95%)
Outcome Effect size RR (95% CI) P value
Primary outcome (Death
or disability at 24 months)
1.04 (0.98 to 1.09) 0.21
Death 1.17 (1.04 to 1.31) 0.01
NEC 1.33 [1.10 to 1.61] .003
ROP 0.74 [0.63 to 0.86] < .001
5 trials, 4965 babies, median GA 26 weeks
Askie et al, Neoprom Metaanalysis, JAMA 2018
Conclusion
Although primary outcome was same in both groups.
Death and Severe NEC more in low saturation group
ROP was less in low saturation group
Recommendations
Target Saturations in NICU – 90-94%
Alarm limits 89% and 95%
European Consensus Guidelines on the Management of Respiratory Distress Syndrome - 2019
Update. Neonatology. 2019;115(4):432-450.
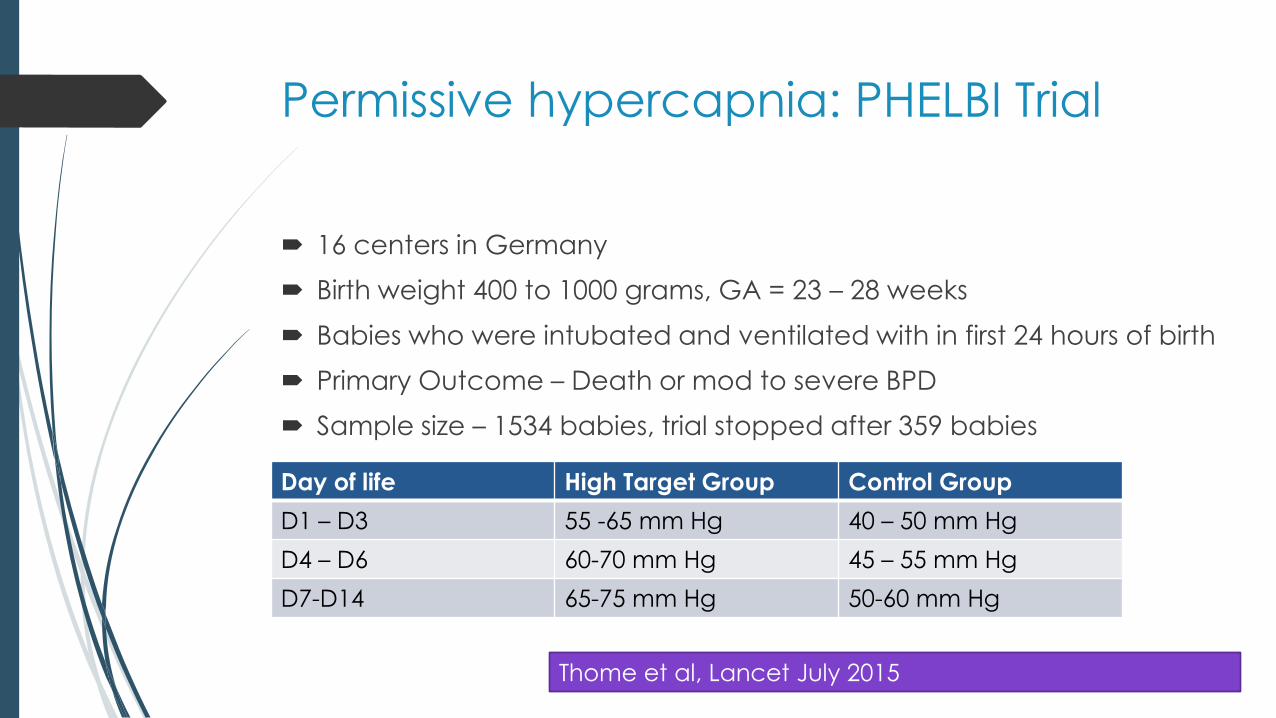
Permissive hypercapnia: PHELBI Trial
16 centers in Germany
Birth weight 400 to 1000 grams, GA = 23 – 28 weeks
Babies who were intubated and ventilated with in first 24 hours of birth
Primary Outcome – Death or mod to severe BPD
Sample size – 1534 babies, trial stopped after 359 babies
Day of life High Target Group Control Group
D1 – D3 55 -65 mm Hg 40 – 50 mm Hg
D4 – D6 60-70 mm Hg 45 – 55 mm Hg
D7-D14 65-75 mm Hg 50-60 mm Hg
Thome et al, Lancet July 2015
PHELBI trial: Results
Primary outcome – same
Mortality (14% vs 11%, p= 0.32) and Grade 3 or 4 IVH
(15%vs 12%, p= 0.3) were higher in high target group
though not statistically significant
Follow up data at 2 years – No difference in
neurodevelopmental outcome.
Thome UH et al, Lancet July 2015
Thome UH et al, ADC Fetal and Neonatal edition 2017
NICU Care
Non invasive mode Which
one
If at all ventilate
then volume or pressure
SurfactantSaturations and PaCO2
targetsCaffiene
CAP trials till date
2006 babies between 500 grams to 1250 grams randomly assigned to
receive either Caffiene or placebo
Short term Results (36 weeks PMA)
Decrease Bronchopulmonary Dysplasia (36 vs 47%, OR 0.63 (95 CI 0.52-0.76,
p<0.001)
18-21 months data
Improves Rate of Survival without neurodevelopmental Disability at 18 to 21
months of age (40.2% vs 46.2%), OR 0.77 (95% CI 0.64-0.93), P=0.008
N Engl J Med. 2006 May 18;354(20):2112-21
N Engl J Med. 2007 Nov 8;357(19):1893-902.
CAP trials till date
5 years follow up data (1640 babies)
Neonatal caffeine therapy was no longer associated with a significantly
improved rate of survival without disability in children with very low birth weights
who were assessed at 5 years.
11 years follow up data
Reduced risk of motor impairment in 11-year-old children with very low birth
weight. No significant effect on combined motor, academic and behaviour
impairments.
JAMA. 2012 Jan 18;307(3):275-82.
JAMA Pediatr. 2017 Jun 1;171(6):564-572.
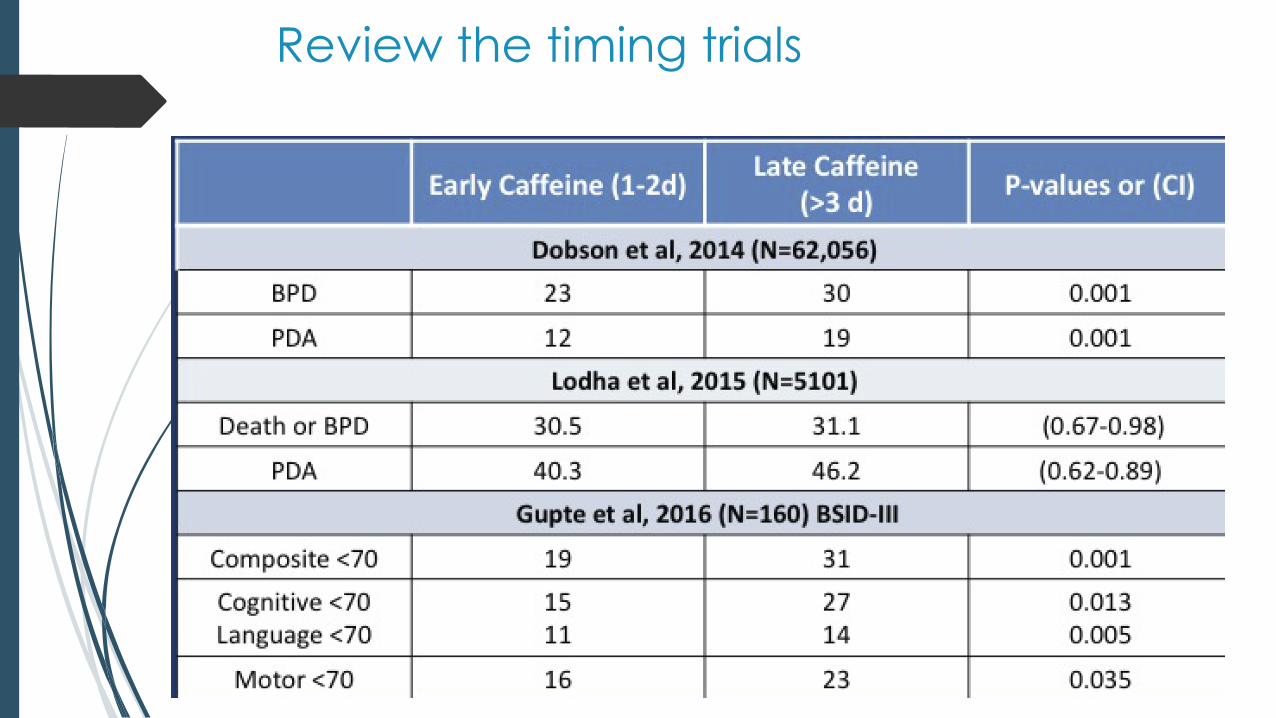
Review the timing trials
Problems with exisiting data on early vs
late caffiene
Only retrospective trials
High risk of bias and changes in practice despite adjusting for confounders
Difficult to do prospective trials
Providers unlikely to withhold caffeine for 3 days
Majority of US units are using caffeine between 2 to 12 hours (VON Data)
Increasing non invasive ventilation encourages earlier use of caffiene
High vs low dose
High (40 mg/kg loading followed by 20 mg/kg maintainence) vs Low (20 mg/kg loading followed by 10 mg/kg maintainence)
A total of 120 neonates (60 in each group) were enrolled.
High-dose caffeine
Significant reduction in extubation failure in mechanically ventilated preterm infants (p<0.05), the frequency of apnea (p<0.001), and days of documented apnea (p<0.001)
Need to be studied more.
Eur J Pediatr. 2015 Jul;174(7):949-56.
NICU Care
Non invasive mode
Which one
If at all ventilate
then volume or pressure
Surfactant
Saturations and
PaCO2 targets
CaffienePost natal
steroids
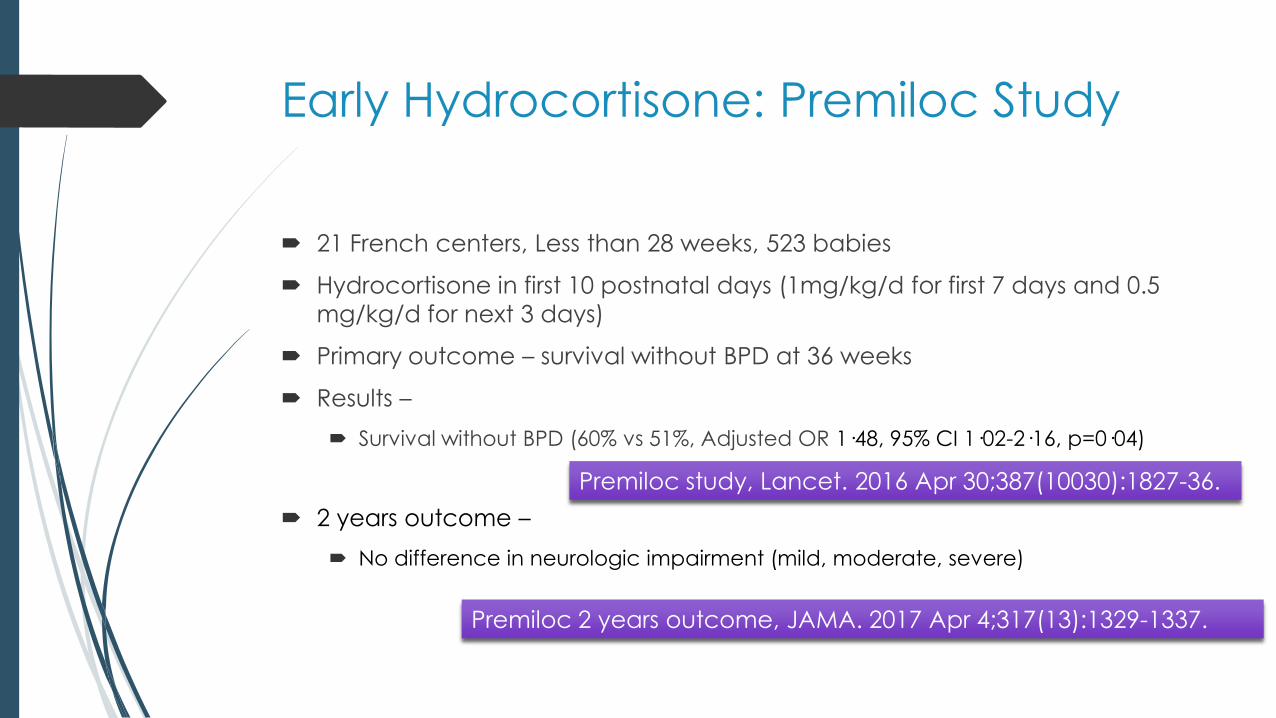
Early Hydrocortisone: Premiloc Study
21 French centers, Less than 28 weeks, 523 babies
Hydrocortisone in first 10 postnatal days (1mg/kg/d for first 7 days and 0.5
mg/kg/d for next 3 days)
Primary outcome – survival without BPD at 36 weeks
Results –
Survival without BPD (60% vs 51%, Adjusted OR 1·48, 95% CI 1·02-2·16, p=0·04)
2 years outcome –
No difference in neurologic impairment (mild, moderate, severe)
Premiloc study, Lancet. 2016 Apr 30;387(10030):1827-36.
Premiloc 2 years outcome, JAMA. 2017 Apr 4;317(13):1329-1337.
Hydrocortisone 7 to 14 days of life
Double Blind RCT in 19 NICUs in Netherland and Belgium,
< 30 weeks, Birth weight < 1250 grams
22 days course of hydrocortisone (cumulative dose 72.5 mg/kg)
Primary outcome – Death or BPD at 36 weeks
372 babies randomized
Results –
No difference in Death or BPD at 36 weeks
Hydrocortisone given between 7-14 days doesnot decrease Death or BPD at 36 weeks
Onland W, Stop BPD Study Group, JAMA. 2019 Jan 29;321(4):354-363..
Inhaled Budesonide
Metanalysis of 17 trials of inhaled budesonide
1807 babies
Significant Reduction in BPD (RR 0.79 (0.68-0.92)
Neurosis Trial
Same results but trend of increased mortality in inhaled budesonide group
was worrying.
Shah VS, Cochrane 2017
Bassler D, Neurosis trial. N Engl J Med. 2015 Oct 15;373(16):1497-506.
Surfactant with Budesonide –
Metaanalysis of 2 studies
381 babies from 2 studies
Surfactant + Budesonide was given every 8 hrly in intervention group vs
surfactant only every 8 hrly in control group
Results
Less BPD (RR 0.57 with 95% CI 0.43-0.76, NNT = 5)
Mortality same
40% reduction in composite outcome of death or BPD (RR 0.6 with 95% CI 0.49-
0.74, NNT = 3)
Large trials need to be done before reaching conclusions
Venkataraman R, Pediatr Pulmonol. 2017 Jul;52(7):968-975.
Summary of Recommendations:
Delivery Room
1. Gently support breathing using CPAP if possible, and if inflations are
needed avoid excessive tidal volumes.
2. Pulse oximetry can help guide heart rate response to stabilisation. Start with
21–30% oxygen for 28–31 weeks’ GA and 30% oxygen for <28 weeks’ GA
and titrate up or down as needed according to SpO2 targets.
3. Aim at SpO2 of 80% or more within 5 min.
4. Intubation at birth should be considered only for those not responding to
the above
Summary of Recommendations: NICU
1. An animal-derived surfactant should be used and given as early as possible
in the course of RDS.
2. Treatment threshold of FiO2 0.30 on CPAP pressure of 6 cm H2O seems
reasonable. Repeat doses of surfactant may be required if there is ongoing
evidence of RDS.
3. If possible, administer surfactant using the LISA method
4. If intubated, babies can often be extubated to CPAP, HFNC or NIPPV
immediately following surfactant, and judgement needs to be made if an
individual baby will tolerate this.
5. For those who require MV, use volume-targeted ventilation and saturation
alarm limits set at 89 and 95%.
Caffeine therapy should be used routinely to minimise need for ventilation.
Babies should be maintained on non-invasive respiratory support in
preference to MV if possible.
After 1–2 weeks, systemic steroids should be considered to facilitate
extubation if the baby remains ventilated.
In preterm babies receiving oxygen, the saturation target should be
between 90 and 94%. To achieve this, suggested alarm limits should be 89
and 95%.
Summary of Recommendations: NICU