Embed Size (px)
Citation preview
Umar Mohamed
Introduction.Introduction.EmbryologyEmbryologyAnatomyAnatomyPhysiologyPhysiologyMethods to study muscles.Methods to study muscles.The three “M” s :muscle ,malformation ,and malocclusionThe three “M” s :muscle ,malformation ,and malocclusionMuscle as etiology of malocclusionMuscle as etiology of malocclusion “ “The equilibrium theory” The equilibrium theory”
Muscles and its treatment modalities.Muscles and its treatment modalities.conclusionconclusion
•Occlusal
Skeletal
Muscular
•The muscle tone, facial expression & orofacial habits mirror the individuals psychoemotional status.

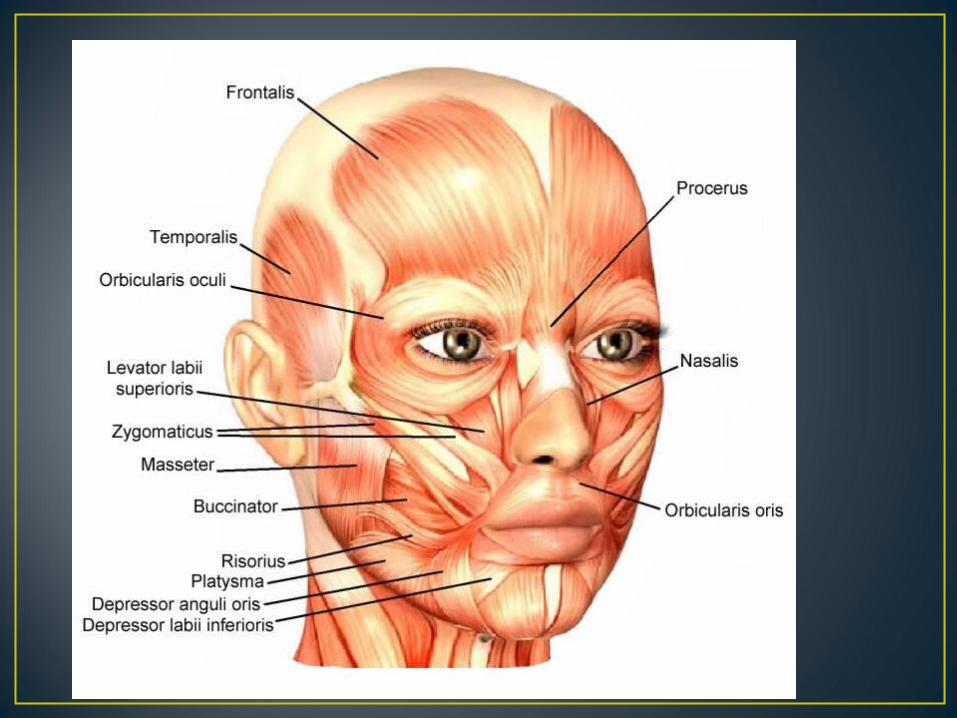
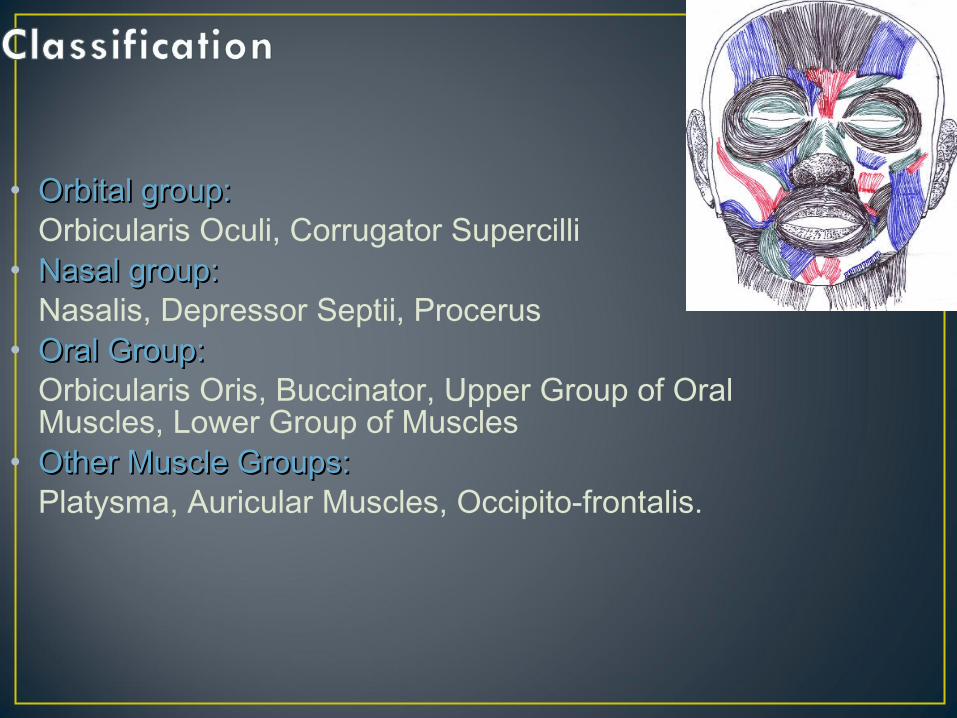
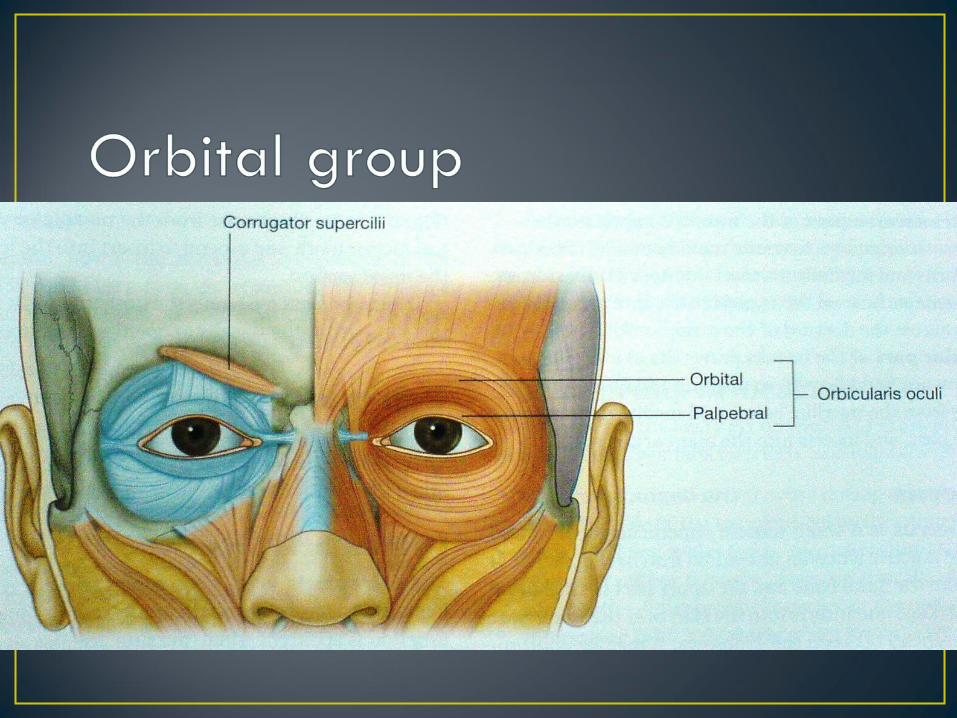
• Orbital group: Orbital group: Orbicularis Oculi, Corrugator Supercilli
• Nasal group:Nasal group: Nasalis, Depressor Septii, Procerus
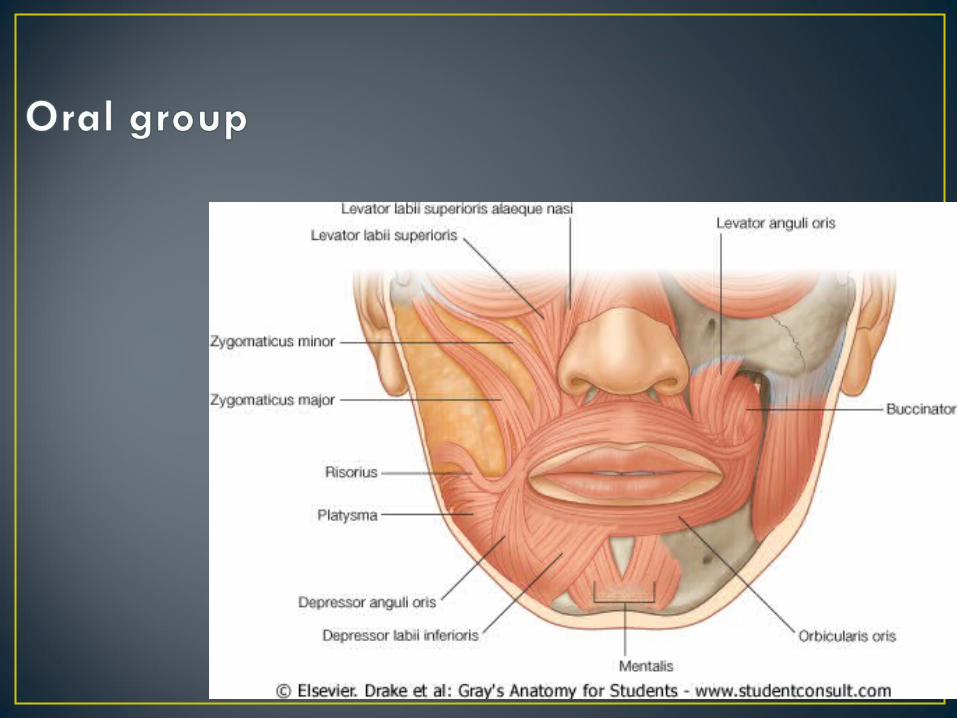
• Oral Group: Oral Group: Orbicularis Oris, Buccinator, Upper Group of Oral Muscles, Lower Group of Muscles
• Other Muscle Groups:Other Muscle Groups: Platysma, Auricular Muscles, Occipito-frontalis.
These are the muscle slips which control the shape of buccal orifice and the posture of the lips
They include: the retractors and elevators of the upper lip viz:-
1. levator labii superioris 2. the zygomaticus major3. the zygomaticus minor4. risorius5. levator anguli oris
the depressor and retractors of the lower lip viz:- the depressor and retractors of the lower lip viz:- 1. depressor labii inferioris2. depressor anguli oris3. mentalis
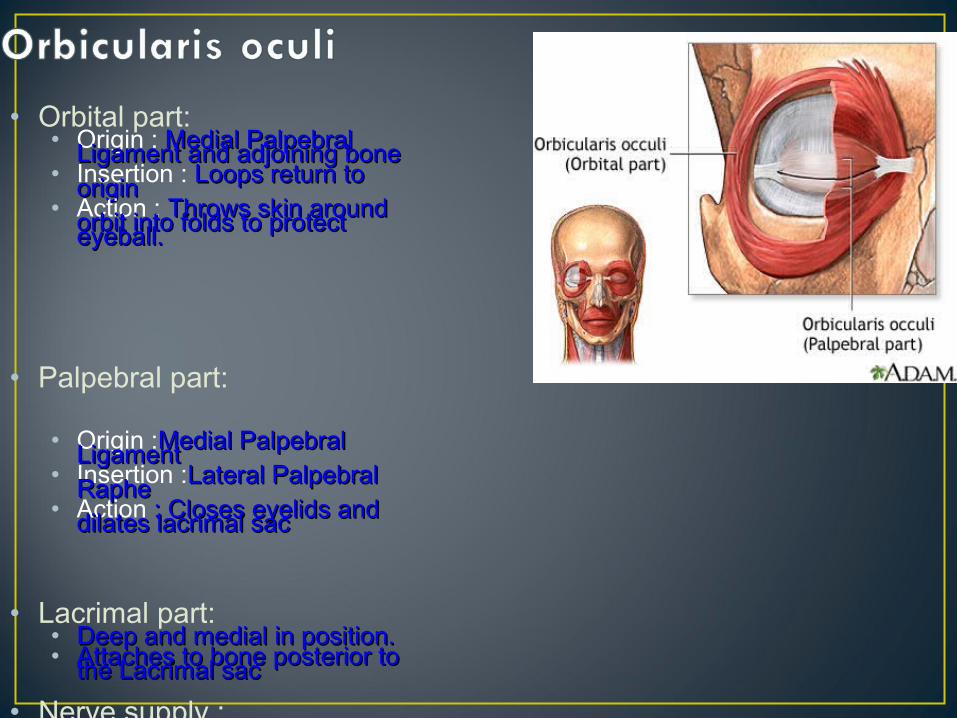
• Orbital part:• Origin : Medial Palpebral Medial Palpebral Ligament and adjoining boneLigament and adjoining bone• Insertion : Loops return to Loops return to originorigin• Action : Throws skin around Throws skin around orbit into folds to protect orbit into folds to protect eyeball.eyeball.
• Palpebral part:
• Origin :Medial Palpebral Medial Palpebral LigamentLigament• Insertion :Lateral Palpebral Lateral Palpebral RapheRaphe• Action : Closes eyelids and : Closes eyelids and dilates lacrimal sacdilates lacrimal sac
• Lacrimal part:• Deep and medial in position.Deep and medial in position.• Attaches to bone posterior to Attaches to bone posterior to the Lacrimal sacthe Lacrimal sac
• Nerve supply : Zygomatic branch and Buccal Zygomatic branch and Buccal branch of Facial Nerve.branch of Facial Nerve.
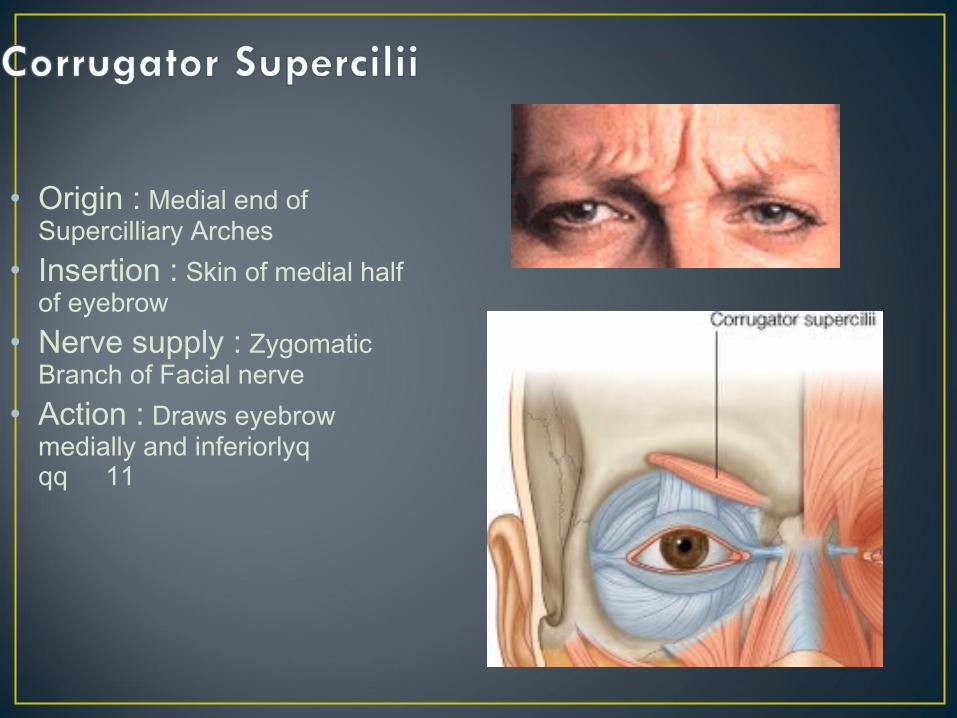
• Origin : Medial end of Supercilliary Arches
• Insertion : Skin of medial half of eyebrow
• Nerve supply : Zygomatic Branch of Facial nerve
• Action : Draws eyebrow medially and inferiorlyqqq 11
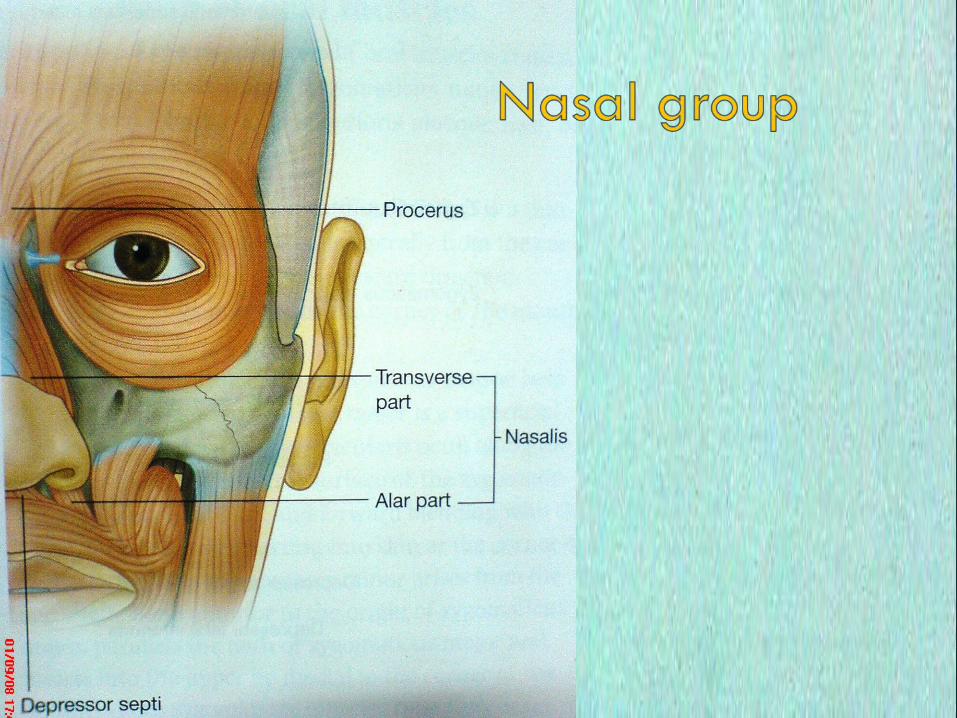
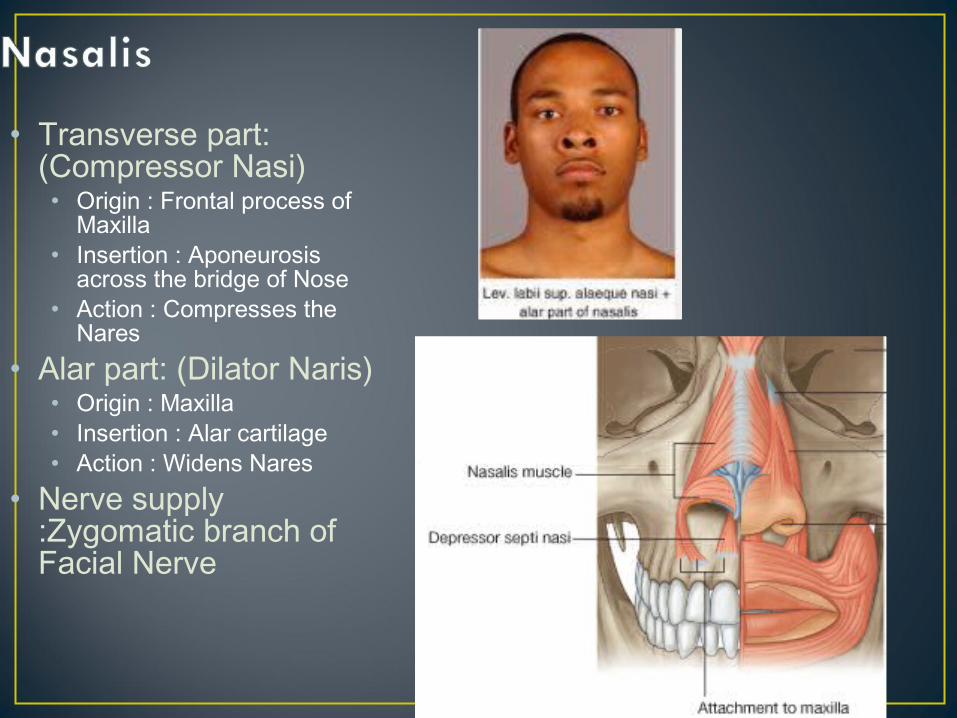
• Transverse part: (Compressor Nasi)• Origin : Frontal process of
Maxilla• Insertion : Aponeurosis
across the bridge of Nose• Action : Compresses the
Nares• Alar part: (Dilator Naris)
• Origin : Maxilla • Insertion : Alar cartilage• Action : Widens Nares
• Nerve supply :Zygomatic branch of Facial Nerve
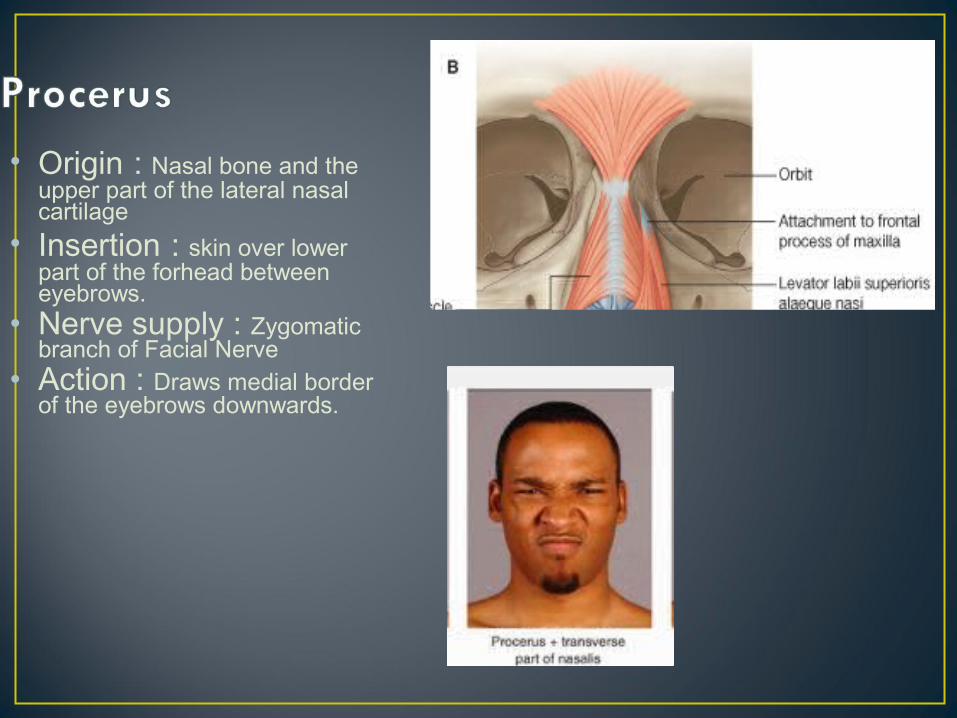
• Origin : Nasal bone and the upper part of the lateral nasal cartilage
• Insertion : skin over lower part of the forhead between eyebrows.
• Nerve supply : Zygomatic branch of Facial Nerve
• Action : Draws medial border of the eyebrows downwards.
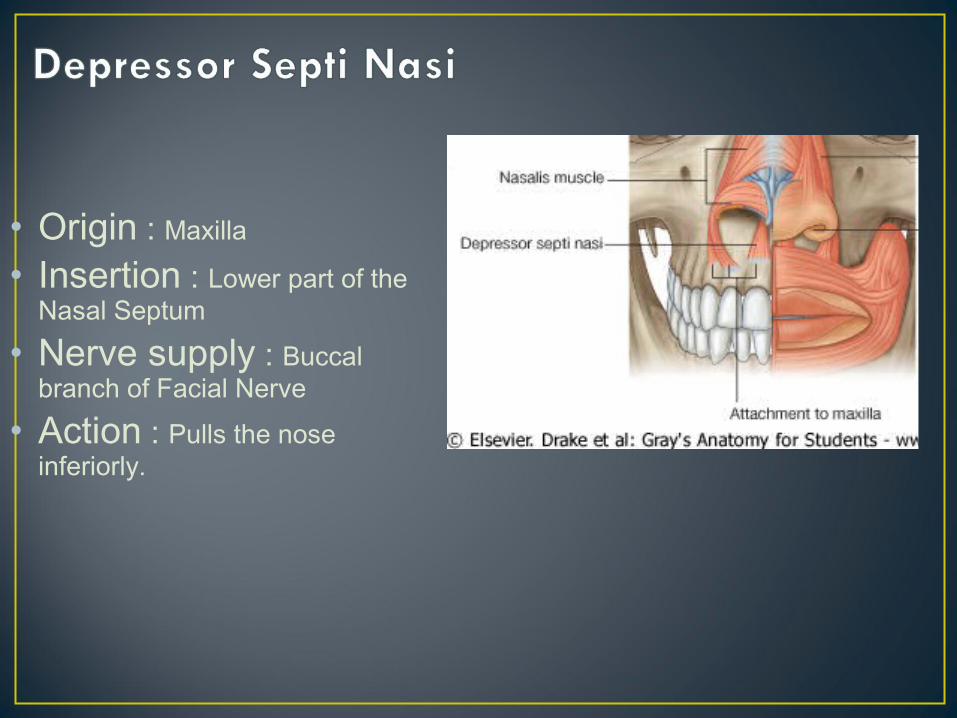
• Origin : Maxilla
• Insertion : Lower part of the Nasal Septum
• Nerve supply : Buccal branch of Facial Nerve
• Action : Pulls the nose inferiorly.
• Distinguishing point between nasal and oral breathers.• Mouth breathers will have disuse atrophy of flaring
muscles of nose.
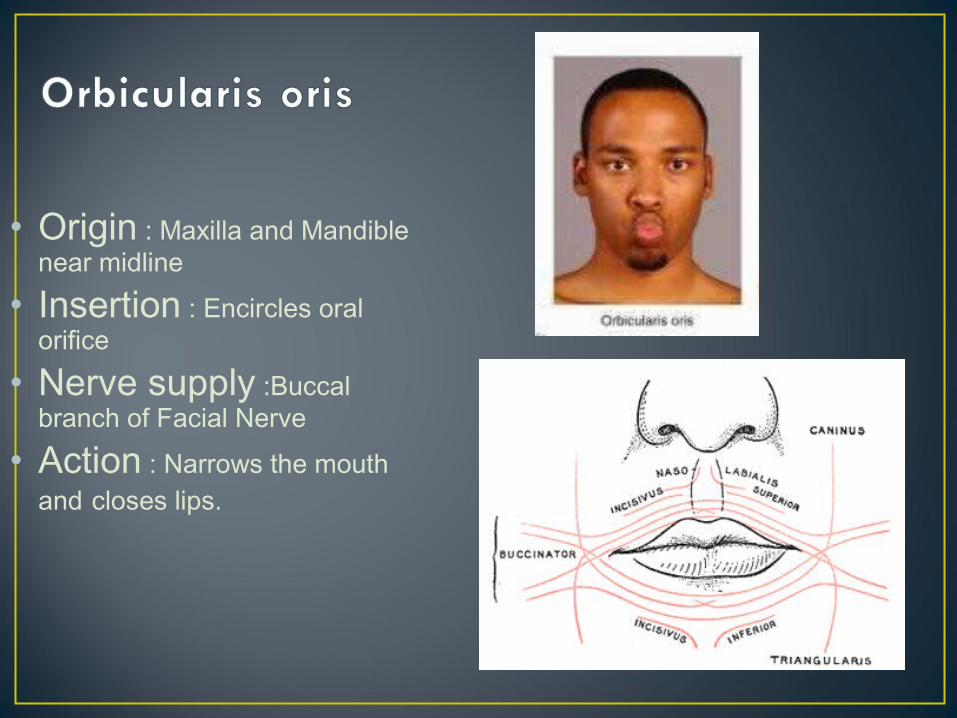
• Origin : Maxilla and Mandible near midline
• Insertion : Encircles oral orifice
• Nerve supply :Buccal branch of Facial Nerve
• Action : Narrows the mouth and closes lips.
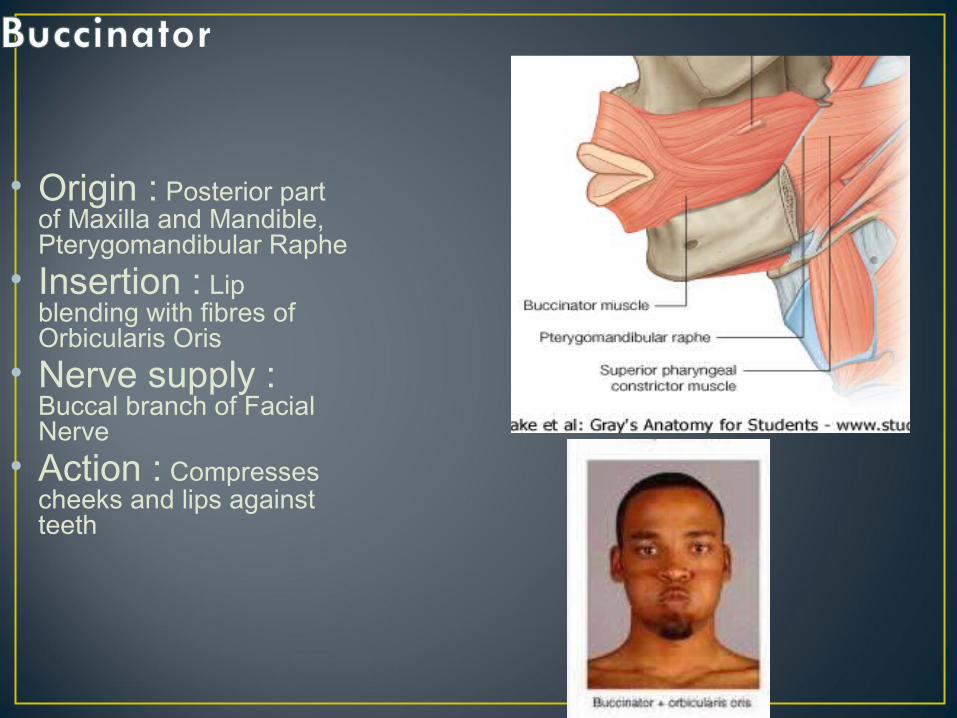
• Origin : Posterior part of Maxilla and Mandible, Pterygomandibular Raphe
• Insertion : Lip blending with fibres of Orbicularis Oris
• Nerve supply : Buccal branch of Facial Nerve
• Action : Compresses cheeks and lips against teeth
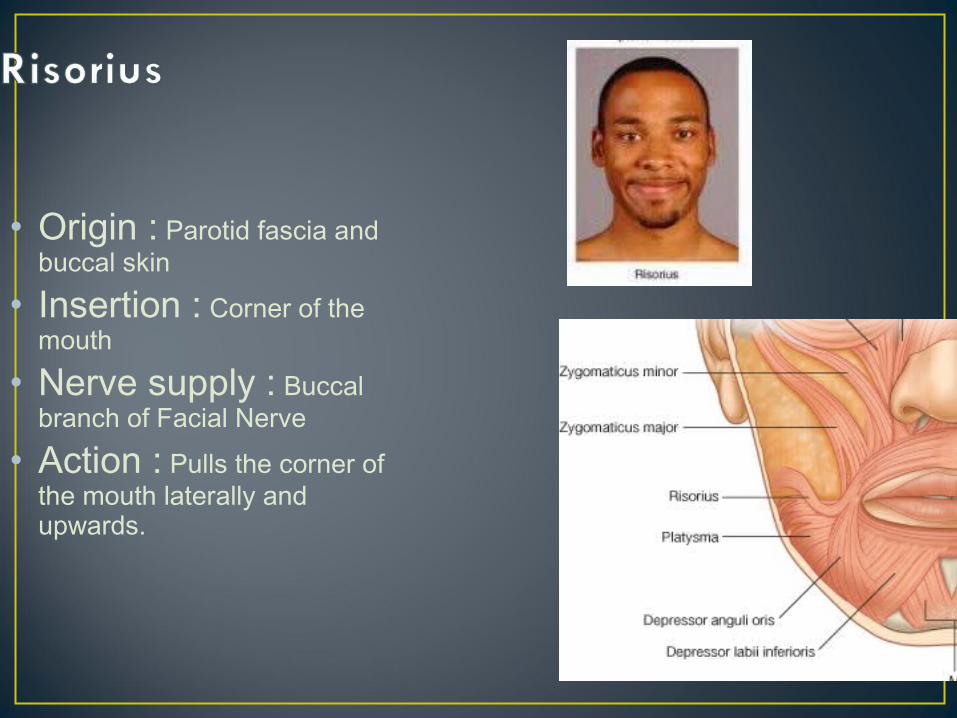
• Origin : Parotid fascia and buccal skin
• Insertion : Corner of the mouth
• Nerve supply : Buccal branch of Facial Nerve
• Action : Pulls the corner of the mouth laterally and upwards.
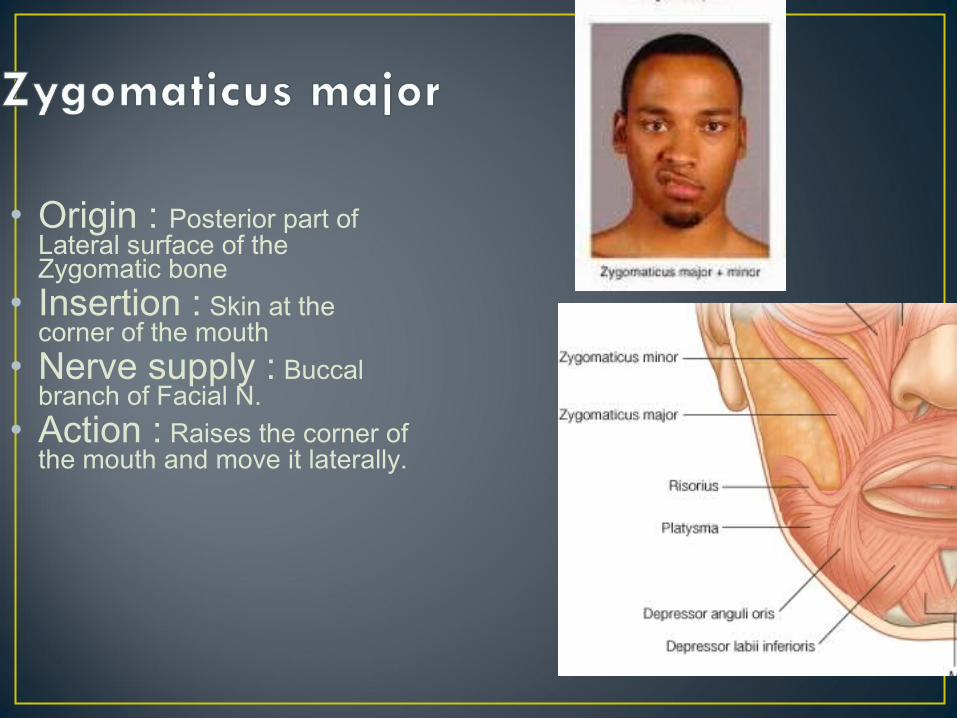
• Origin : Posterior part of Lateral surface of the Zygomatic bone
• Insertion : Skin at the corner of the mouth
• Nerve supply : Buccal branch of Facial N.
• Action : Raises the corner of the mouth and move it laterally.
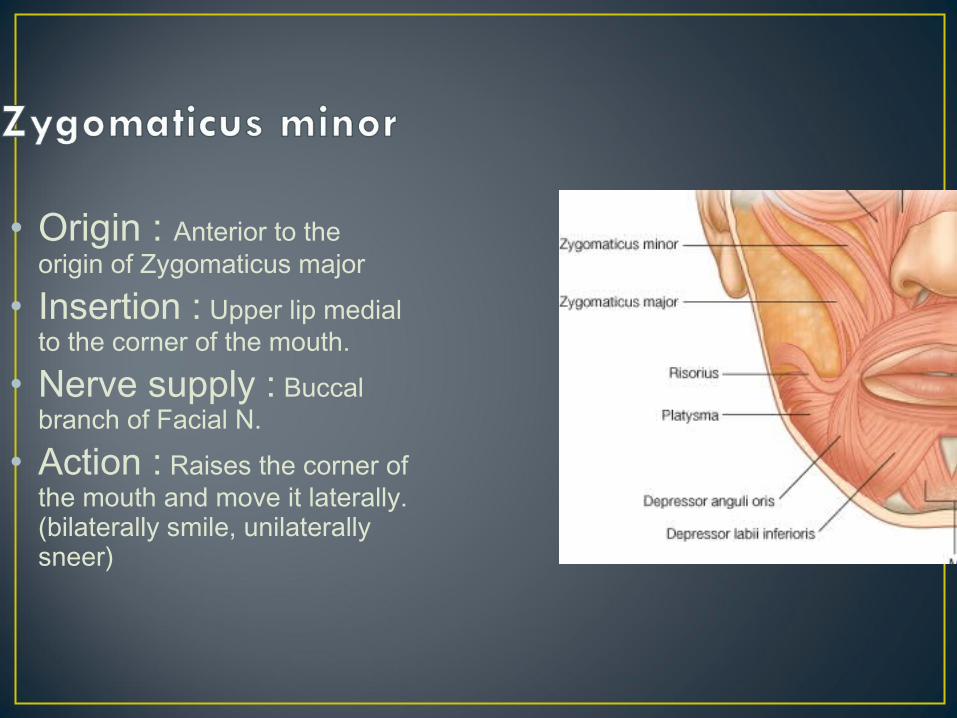
• Origin : Anterior to the origin of Zygomaticus major
• Insertion : Upper lip medial to the corner of the mouth.
• Nerve supply : Buccal branch of Facial N.
• Action : Raises the corner of the mouth and move it laterally.(bilaterally smile, unilaterally sneer)
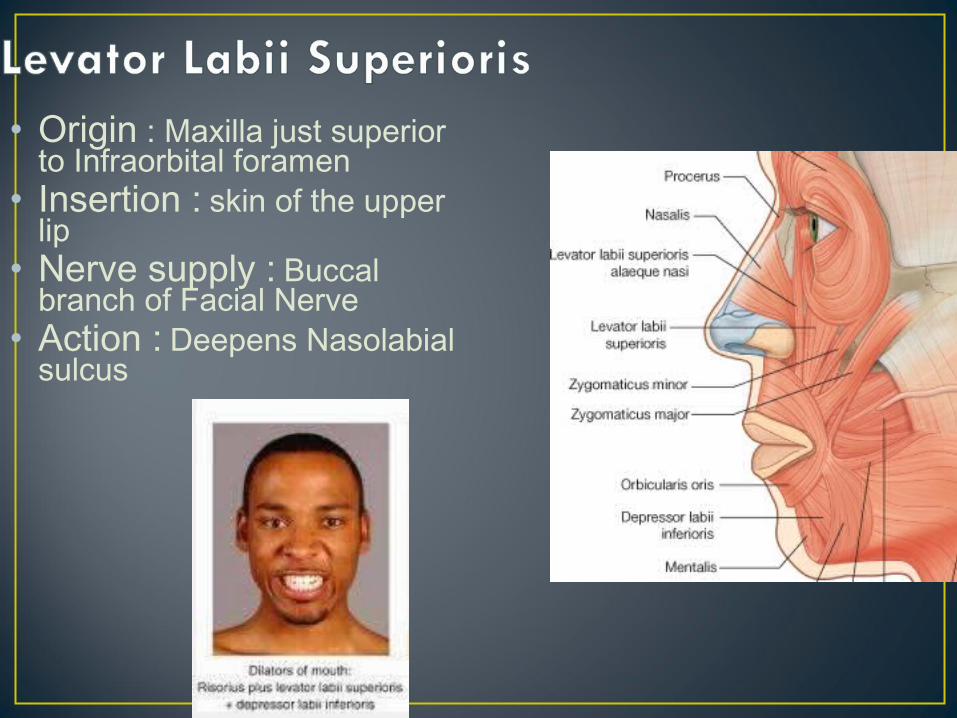
• Origin : Maxilla just superior to Infraorbital foramen
• Insertion : skin of the upper lip
• Nerve supply : Buccal branch of Facial Nerve
• Action : Deepens Nasolabial sulcus
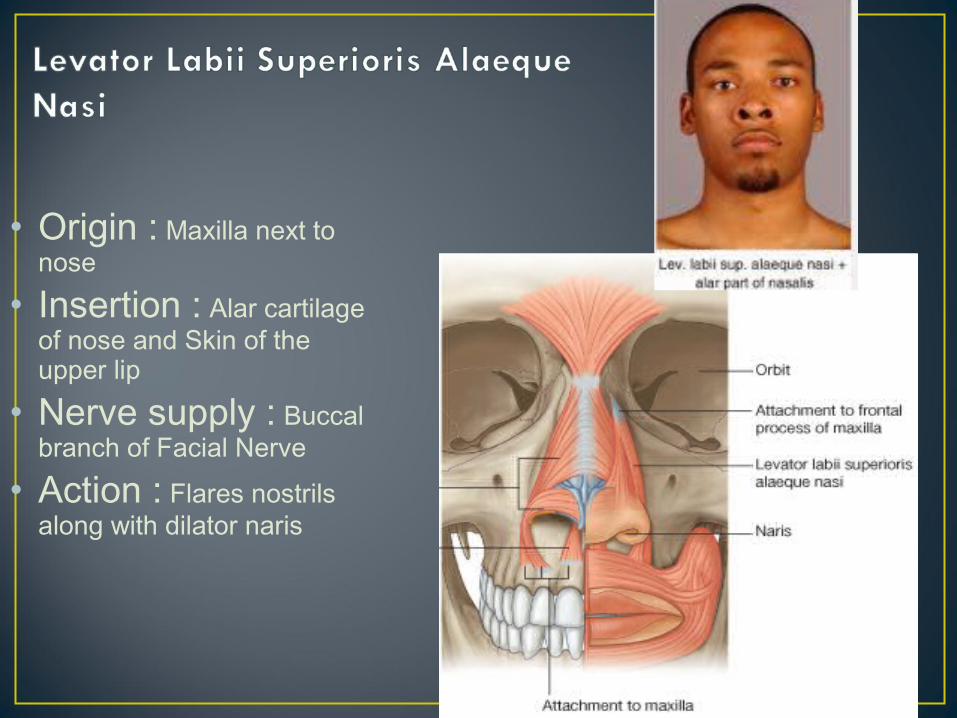
• Origin : Maxilla next to nose
• Insertion : Alar cartilage of nose and Skin of the upper lip
• Nerve supply : Buccal branch of Facial Nerve
• Action : Flares nostrils along with dilator naris
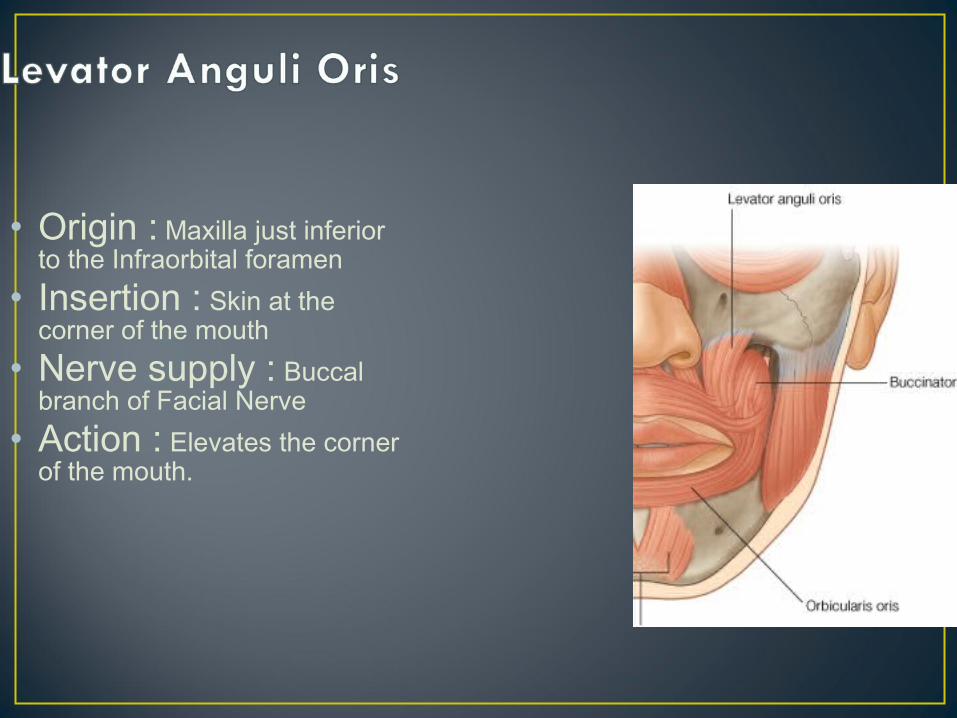
• Origin : Maxilla just inferior to the Infraorbital foramen
• Insertion : Skin at the corner of the mouth
• Nerve supply : Buccal branch of Facial Nerve
• Action : Elevates the corner of the mouth.
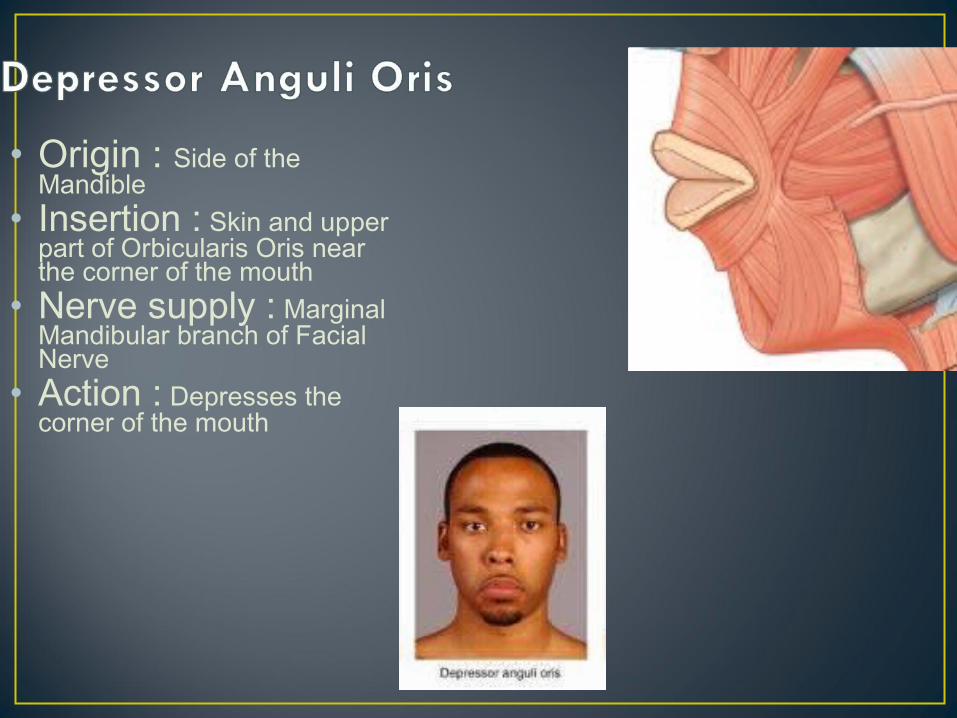
• Origin : Side of the Mandible
• Insertion : Skin and upper part of Orbicularis Oris near the corner of the mouth
• Nerve supply : Marginal Mandibular branch of Facial Nerve
• Action : Depresses the corner of the mouth
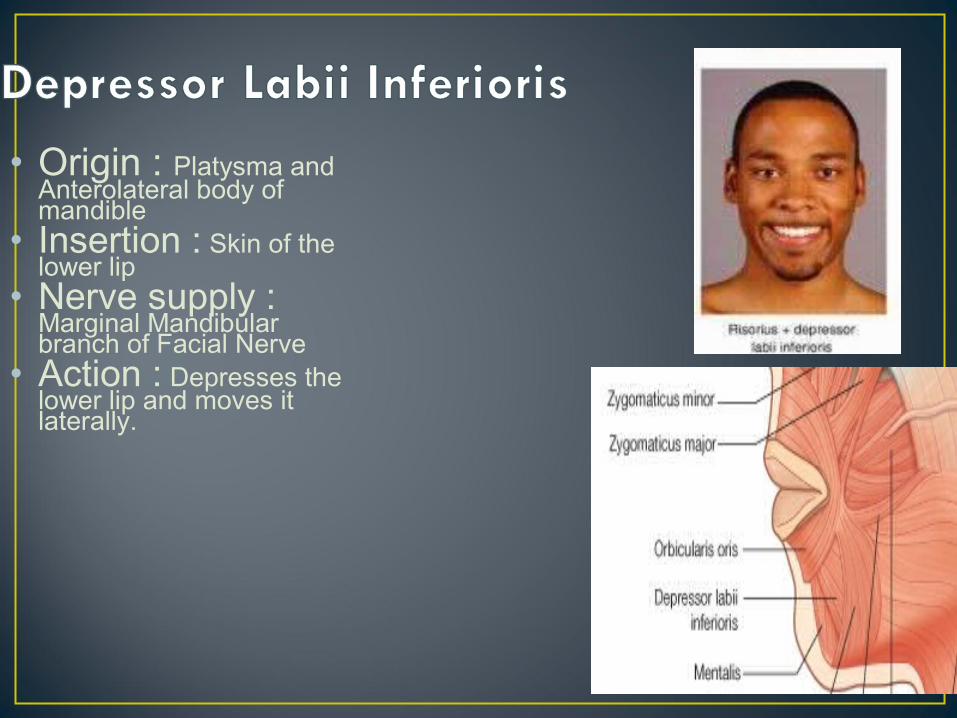
• Origin : Platysma and Anterolateral body of mandible
• Insertion : Skin of the lower lip
• Nerve supply : Marginal Mandibular branch of Facial Nerve
• Action : Depresses the lower lip and moves it laterally.
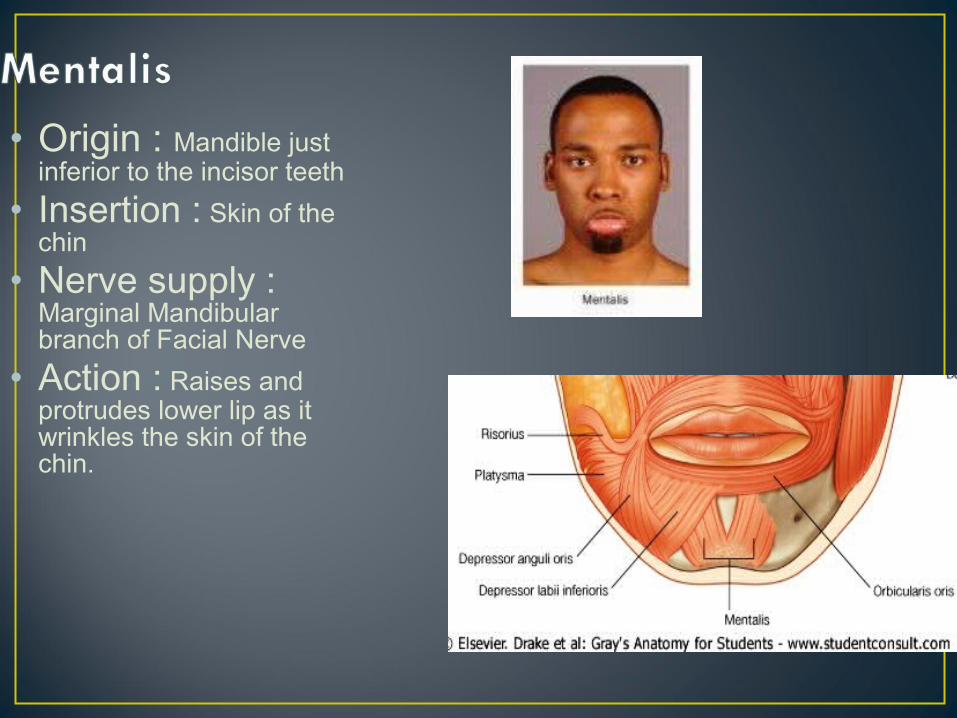
• Origin : Mandible just inferior to the incisor teeth
• Insertion : Skin of the chin
• Nerve supply : Marginal Mandibular branch of Facial Nerve
• Action : Raises and protrudes lower lip as it wrinkles the skin of the chin.
The superficial and the lateral cervical muscles:-
These include viz:-1. The platysma 2. The trapezius 3. The sterocleidomastoid muscles
• Frontalis- normal horizontal wrinkles of the forehead.
• Corrugator supercilli- frowning & making vertical wrinkles of the forehead.
• Orbicularis oculi- tight closure of the eyes.• Orbicularis oris- whistling & pursing the mouth.• Buccinator- puffing the mouth & then blowing
forcibly• Platysma- forcible pulling of the angles of the
mouth downwards & backwards forming prominent vertical folds of the skin on the side of the neck. The platysma contracts along with the risorius.
The primary function is expression of the emotions.emotions.
The facial muscles are capable of performing 7000 expressions7000 expressions according to Coleman.
-Paresis Paresis of the orbicularis oculiorbicularis oculi leads to the droopingdrooping of the lower eyelid.
-ParalysisParalysis of the orbicularis orisorbicularis oris will lead to angular cheliosis and the drooling.drooling.
The facial muscle also contributes to stabilizationstabilization of the mandible mandible during the infantile swallowing and chewing and swallowing in the occlusally compromised adults.
They are also responsible for the maintenance of the postureposture of the facial structures.
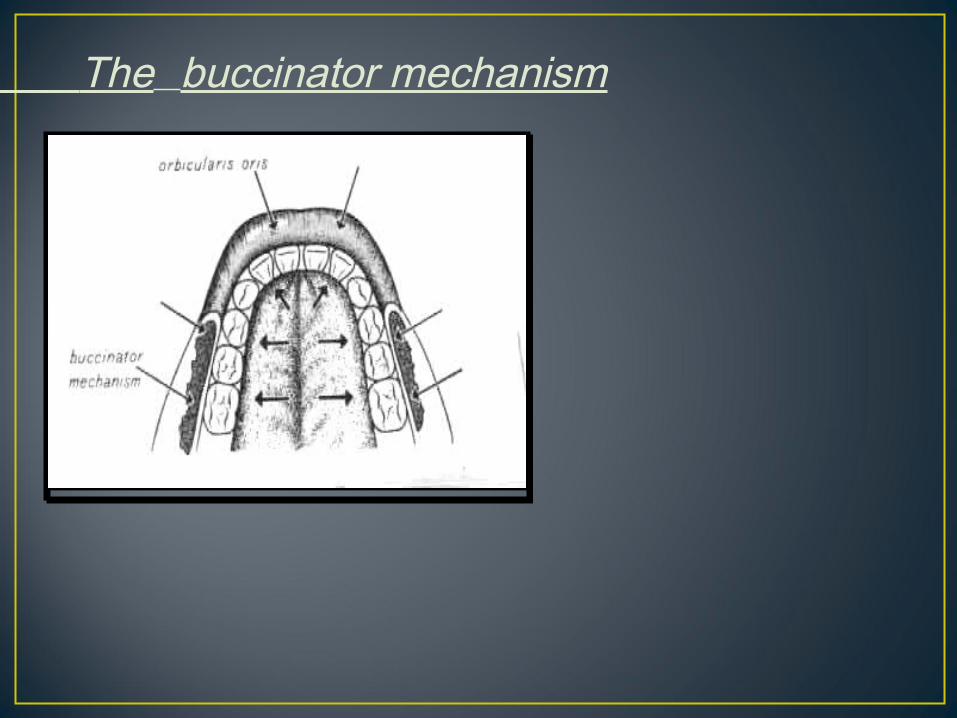
The buccinator mechanism
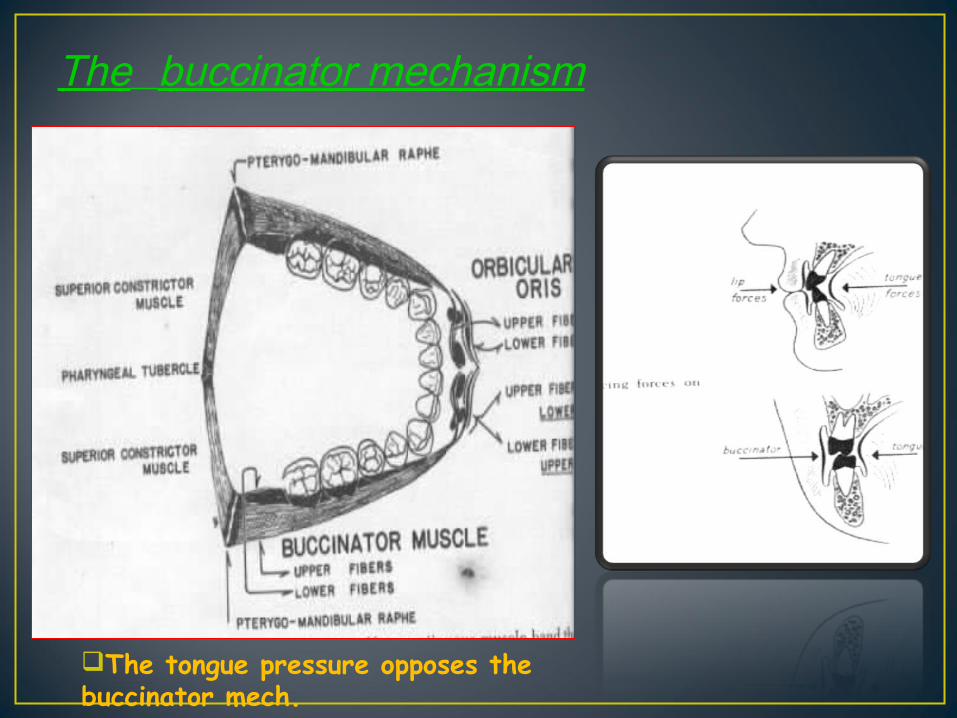
The buccinator mechanism
The tongue pressure opposes the buccinator mech.
• The Commisure smile:- It is seen in 67% of the population. It forms a Cupid’s bow. The corners of the mouth turn upward
because of the pull of zygomaticus major.
• It is seen in 31% of the population.• Upper lip is elevated uniformly
without corners of the mouth turning upwards.
• The upper lip moves superiorly as in the
• Canine smile ,but lower lip also moves inferiorly in similar fashion.
Tension: - two types
1. Active2. Passive
Active tension:Active tension: - the tension resulting from the contraction of the muscle tissue
e.g:-stretch reflex, it can be also increased by willed contraction of muscles
as in volitional clenching of the teeth.Passive tensionPassive tension:: - tension which results from the physical
properties (viscoelastic) alone of the tissues is called passive tension.
e.g:- in facial muscles
In many muscles the elongation will increase both active as well as the passive tension.
The sum of both the tension is called as the total tension.
• Electromygraphy provides a more objective and definitive means of appraising muscle activity before, during and after orthodontic therapy.
The measurementmeasurement can be done by measuring either the heightheight of the action potential or the frequency frequency of the individual action potential.
MoyersMoyers was the first one to study the orofacial muscles using the EMG.
Significance:
In orthodontics this can be used in the pre, mid and post to analyze the appraisal of the muscle activity.
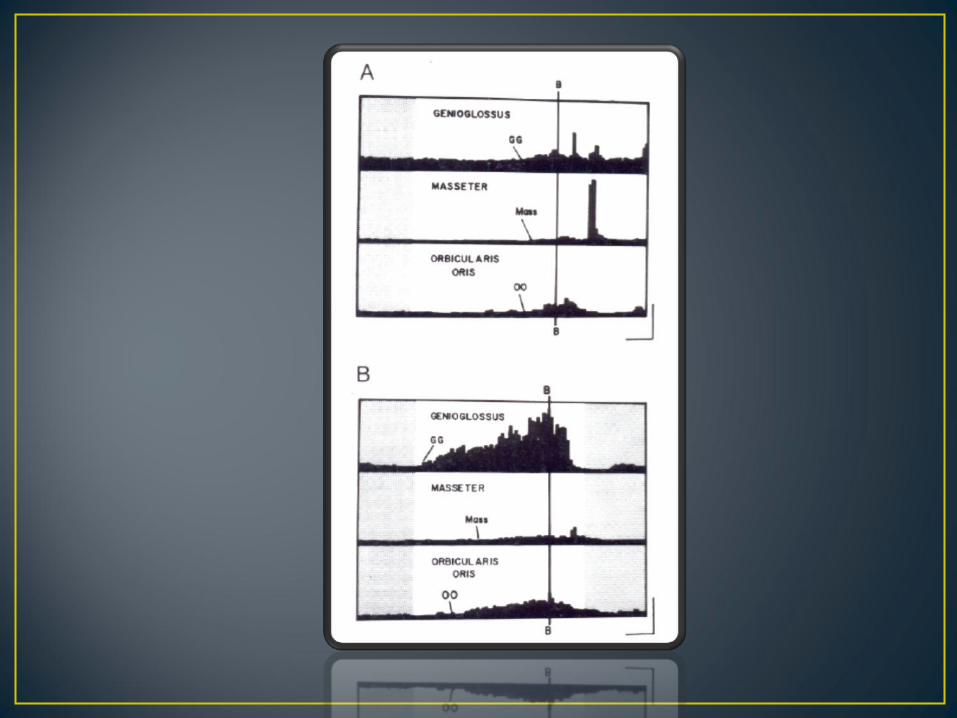
Study by Lowe and Johnston
• Summary• A change in muscle function can be initiate
morphologic variation in the normal configuration of the teeth and supporting bone.
• The structural abnormality is increased by compensatory muscle activity to extend that a balance is reached between pattern, environment and physiology
• Orthodontic therapy in such a manner that the finished result reflect structural balance between the structural changes obtained and the functional force acting on the teeth and investing tissue .
Equilibrium theory
.The duration of aduration of a forceforce, be c a us e o f the bio lo g ic re s p o ns e is m o re im p o rta nt tha n its m a g nitud e .
.
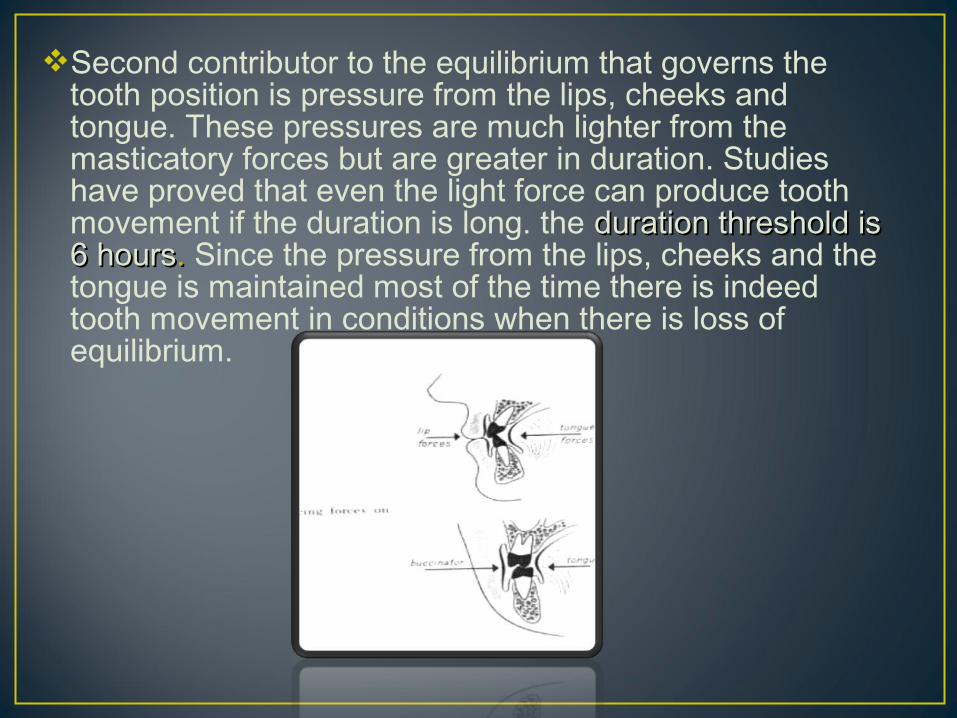
Second contributor to the equilibrium that governs the tooth position is pressure from the lips, cheeks and tongue. These pressures are much lighter from the masticatory forces but are greater in duration. Studies have proved that even the light force can produce tooth movement if the duration is long. the duration threshold is duration threshold is 6 hours6 hours.. Since the pressure from the lips, cheeks and the tongue is maintained most of the time there is indeed tooth movement in conditions when there is loss of equilibrium.
In cases with the orthodontic appliances for e.g. If arch expansion plate is given, and after certain time, the lips and cheeks pressure tends to increase,but there will be balance of forces until the plate is there. once that is removed there is unbalance and the teeth would collapse lingually until a new position of balance is achieved.
With a habit for e.g. Thumb sucking. If habit like these creates pressure for more than 6hrs than teeth will move but if more force is applied for less duration than there will be no effect.
• Muscle function is usually normal in cases of class I malocclusion.
• The teeth are in a state of balance with environmental forces.
• Class I open bite problems may be attributed to thumb and finger sucking habits.
• Hyperactive mentalis activity.
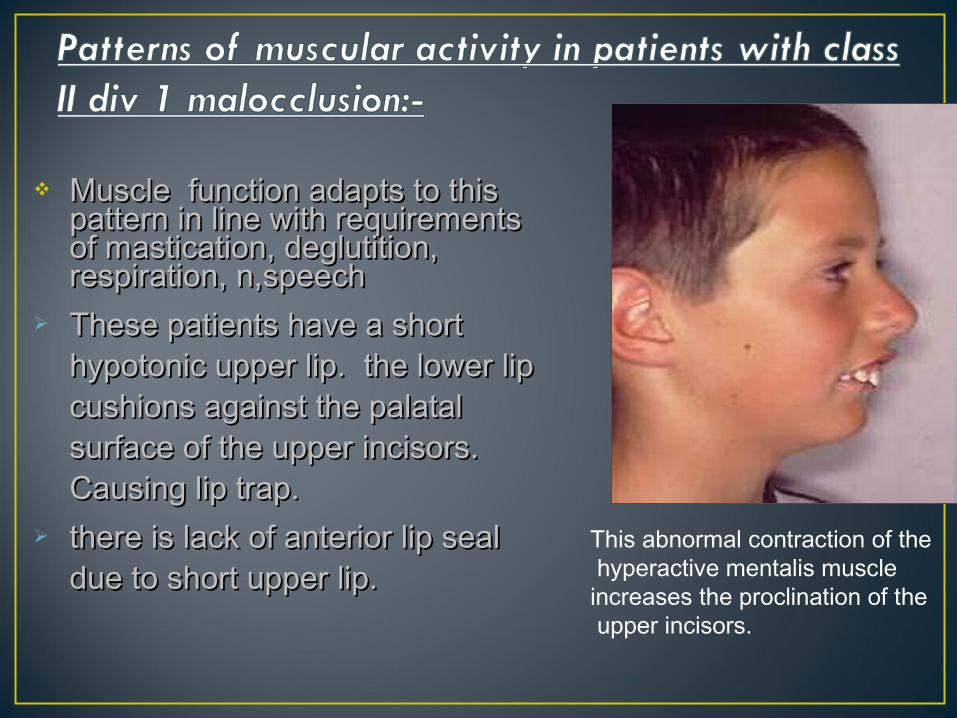
Muscle function adapts to this Muscle function adapts to this pattern in line with requirements pattern in line with requirements of mastication, deglutition, of mastication, deglutition, respiration, n,speechrespiration, n,speech
These patients have a short These patients have a short hypotonic upper lip. the lower lip hypotonic upper lip. the lower lip cushions against the palatal cushions against the palatal surface of the upper incisors. surface of the upper incisors. Causing lip trap.Causing lip trap.
there is lack of anterior lip seal there is lack of anterior lip seal due to short upper lip.due to short upper lip.
This abnormal contraction of the hyperactive mentalis muscle increases the proclination of the upper incisors.
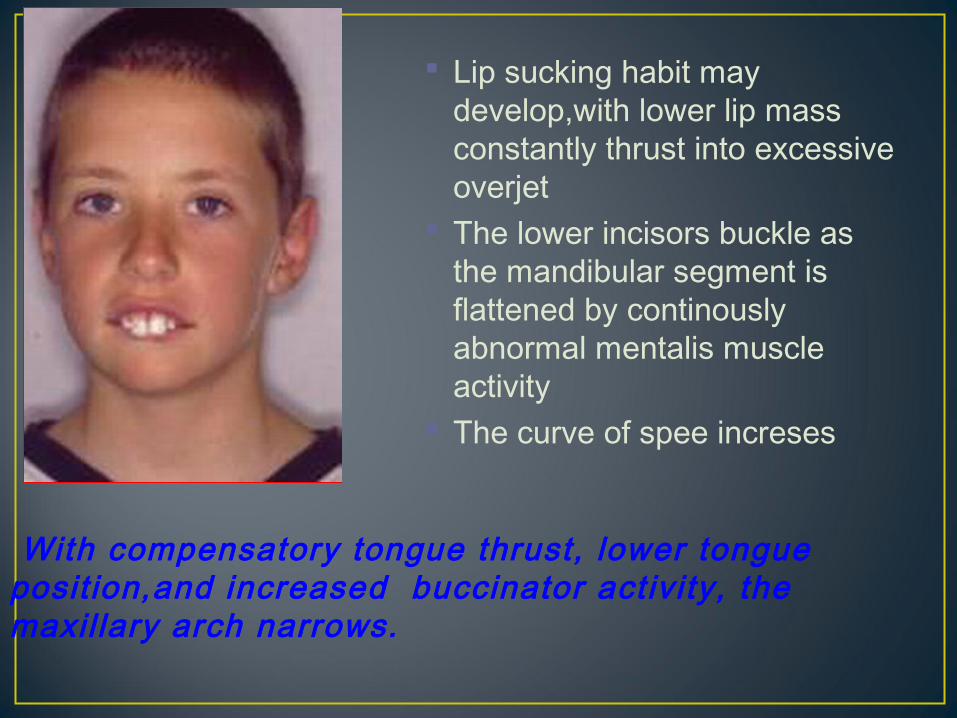
Lip sucking habit may develop,with lower lip mass constantly thrust into excessive overjet
The lower incisors buckle as the mandibular segment is flattened by continously abnormal mentalis muscle activity
The curve of spee increses
With compensatory tongue thrust, lower tongue posit ion,and increased buccinator activity, the maxil lary arch narrows.
Many clinicians hypothesize that retroclination of the maxillary central incisors in class II, div 2 is caused by increased resting lip pressure against these teeth.
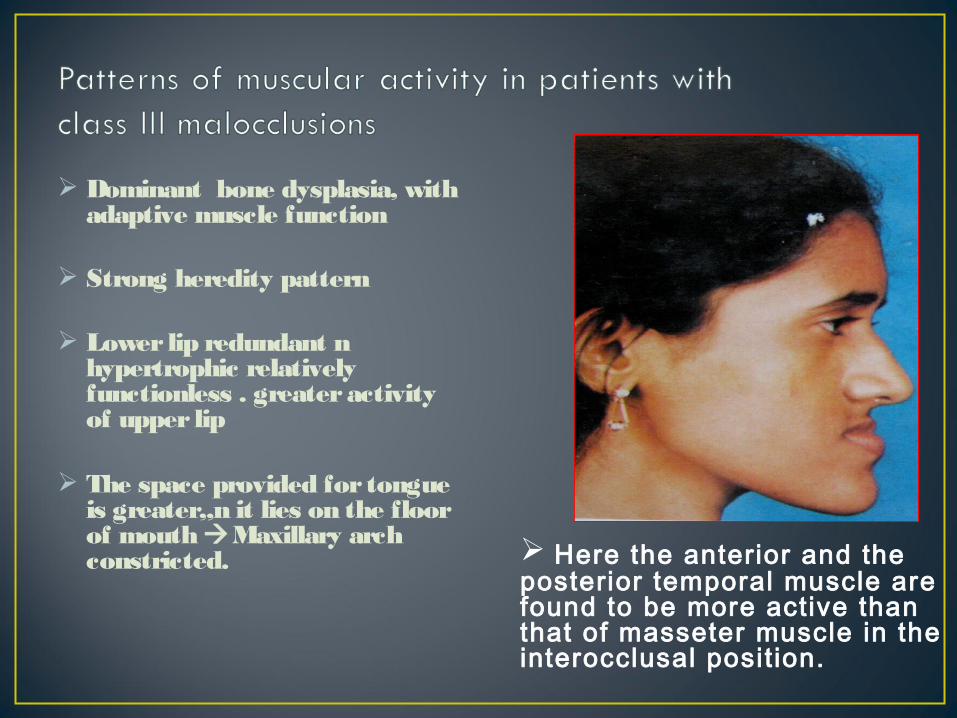
Dominant bone dysplasia, with adaptive muscle function
Strong heredity pattern
Lower lip redundant n hypertrophic relatively functionless . greater activity of upper lip
The space provided for tongue is greater,,n it lies on the floor of mouth Maxillary arch constricted. Here the anterior and the
posterior temporal muscle are found to be more active than that of masseter muscle in the interocclusal posit ion.
• Thumb sucking:-• Abnormal lip & tongue activity is frequently
associated with the finger habit.• The upper lip is no longer called upon to engage
in sphinter-like activity in contact with the lower lip; it remains hypotonic, functionless and appears retracted or short.
• In an attempt to create lip seal, there is strong contraction of the orbicularis oris mentalis complex.
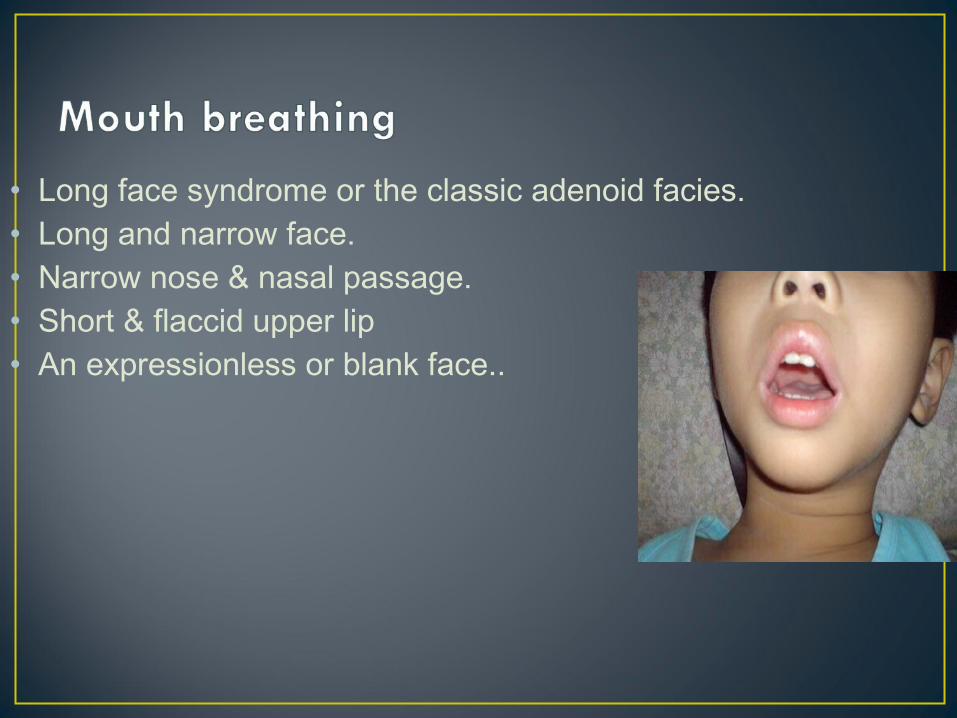
• Long face syndrome or the classic adenoid facies.• Long and narrow face.• Narrow nose & nasal passage.• Short & flaccid upper lip• An expressionless or blank face..
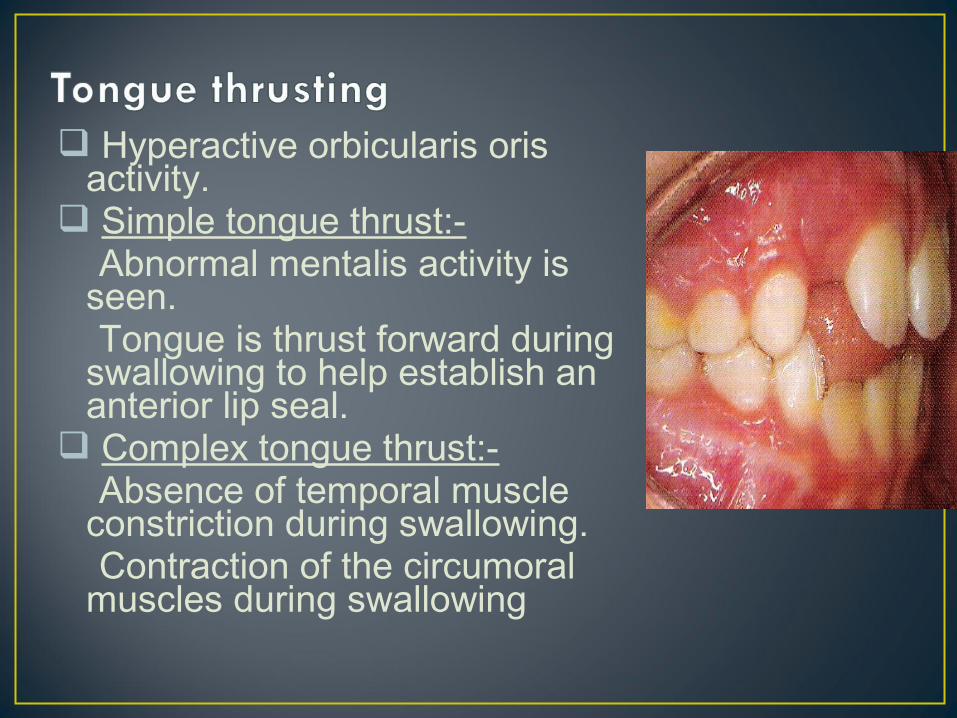
Hyperactive orbicularis oris activity.
Simple tongue thrust:- Abnormal mentalis activity is
seen. Tongue is thrust forward during
swallowing to help establish an anterior lip seal.
Complex tongue thrust:- Absence of temporal muscle
constriction during swallowing. Contraction of the circumoral
muscles during swallowing
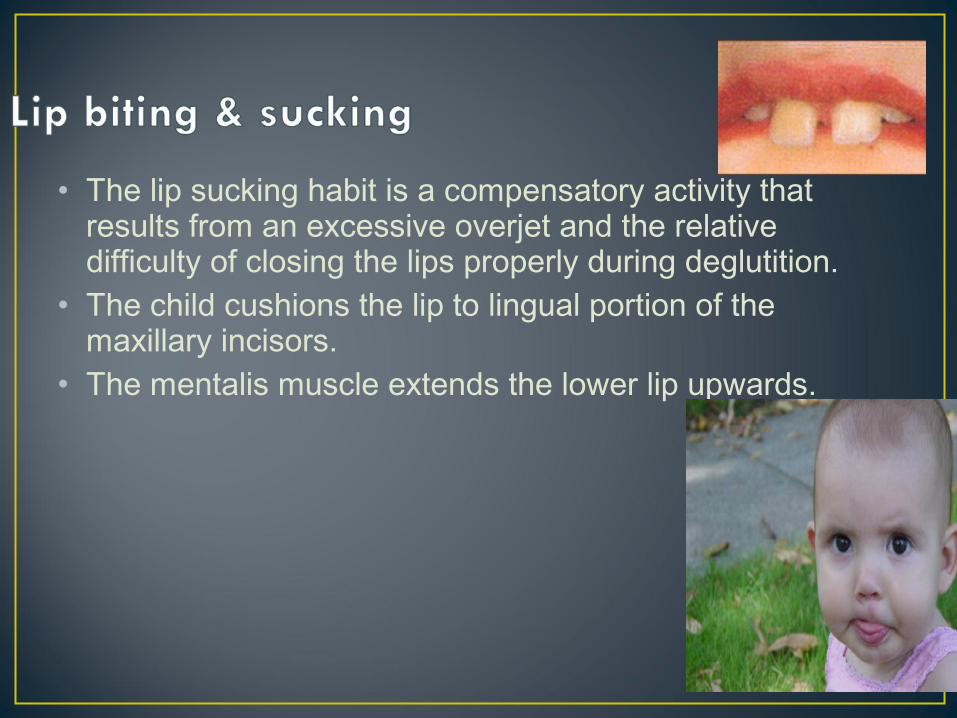
• The lip sucking habit is a compensatory activity that results from an excessive overjet and the relative difficulty of closing the lips properly during deglutition.
• The child cushions the lip to lingual portion of the maxillary incisors.
• The mentalis muscle extends the lower lip upwards.
Graber classifies functional orthodontic appliances broadly into 3 categories
• Group IGroup I: : transmit muscle forces directly to teeth .e.g:inclined planes,oral screens
• Group IIGroup II :reposition mandible downward n forward . resultant force created not only to teeth but also to associated structures.eg:activator n its modificatiions
• Group IIIGroup III: : major operating area in vestibule outside dental arches.supportinng bone n teeth influenced by changing muscle balance .eg:frankles functional regulator
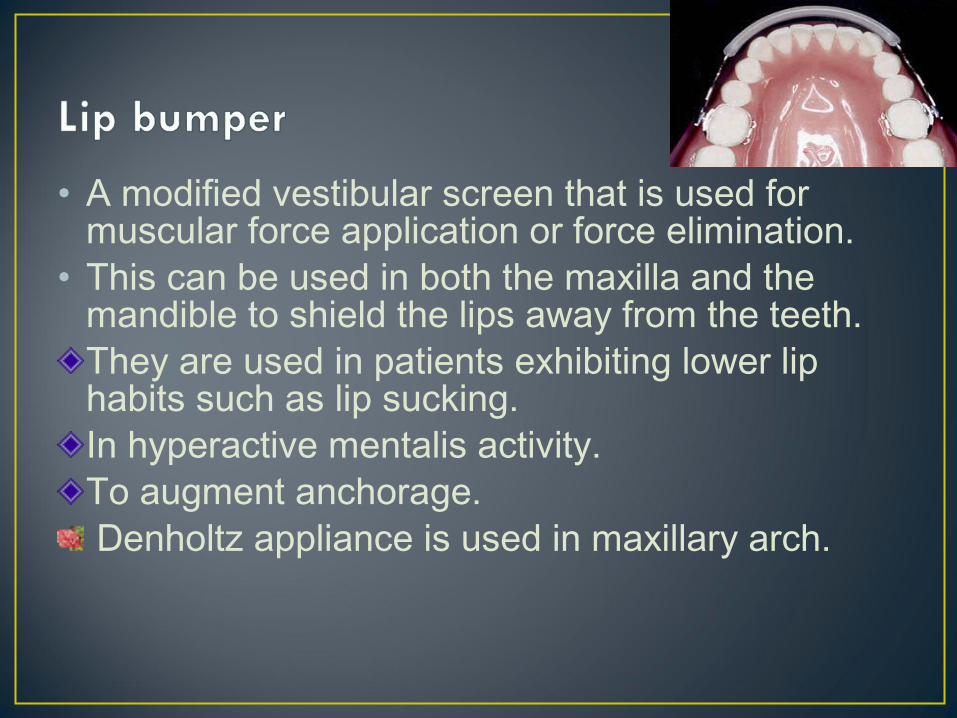
• A modified vestibular screen that is used for muscular force application or force elimination.
• This can be used in both the maxilla and the mandible to shield the lips away from the teeth.They are used in patients exhibiting lower lip habits such as lip sucking.In hyperactive mentalis activity.To augment anchorage. Denholtz appliance is used in maxillary arch.
• As skin ages, the collagen & elastin fibers in the dermis break down, reducing skin ability to ‘snap back’ from smiles & other facial expressions.
• Dynamic movements that cause the skin to repeatedly crease in the same place, such as smiling, will wear down the underlying tissue in that specific spot, creating a line that remains after muscle relaxes.
• We are in the present Era where we are moving from Angel’s paradigm which is occlusion centered to the soft tissue paradigm, where we cannot afford to overlook the soft tissues.
• Muscles have to be given its due importance not only forming a integral part of your diagnosis but also have a role to play in your treatment planning, and not only in the treatment planning but also the kind of retention being planned for the patient.

• Hand book of ‘orthodontics’- Moyers• Problems & procedures in Dentofacial orthopaedics –
Vander Linden• Current controversiesin orthodontics – Birte Melsen• Facial growth – Enlow• Dentofacial Orthopedics with Functional Appliances –
Thomas M. Graber, Thomas Rakosi, Alexandre G. Petrovic.
• Contemporary Orthodontics – Proffit• Smile Wikipedia – Free Encyclopedia• Gray’s Anatomy for students by Richard & Drake.• Principles of Anatomy & Physiology by Tortora &
Grabowski.• Graber• en.wikipedia.org/wiki/Bell's_palsy