Embed Size (px)
Citation preview

Intra Uterine Growth Retardation
By Dr. VARSHA DESHMUKH

Small for Gestational AgeSmall for Gestational Age
Healthy small baby:Healthy small baby: In accurately dated In accurately dated pregnancies, approximately 80–85% of pregnancies, approximately 80–85% of fetuses identified as SGAfetuses identified as SGA are are constitutionally small but healthy, constitutionally small but healthy,
‘ ‘True’ IUGR :10–15% True’ IUGR :10–15%
5–10% of fetuses are affected by 5–10% of fetuses are affected by chromosomal/structural anomalies or chromosomal/structural anomalies or chronic intrauterine infection.chronic intrauterine infection.

Small for Gestational AgeCauses:
Small for Gestational AgeCauses:
• Incorrect dating of the pregnancy Incorrect dating of the pregnancy
• Constitutionally small size Constitutionally small size
• Genetic/Chromosomal defects in the fetus Genetic/Chromosomal defects in the fetus
• Intrauterine infectionIntrauterine infection
• Intrauterine growth restriction (IUGR) Intrauterine growth restriction (IUGR) related to an inadequacy in the supply of related to an inadequacy in the supply of nutrients and/or oxygen to the fetus nutrients and/or oxygen to the fetus through the uteroplacental unit.through the uteroplacental unit.

Currently Accepted Classification as per birth-weight percentiles
• Very small for gestational age (<3rd percentile),
• Small for gestational age (SGA, <10th percentile),
• Appropriate for gestational age (AGA, 10th to 90th percentile) or
• Large for gestational age (>90th percentile)
Drawback:
• Birth-weight percentiles do not distinguish between the small neonate who is normally grown given his genetic potential, and the neonate who is growth restricted owing to a disease process hence use other USG criteria

6 to 10 times greater than AGA.
120 per 1,000 for all cases of IUGR
80 per 1,000 [after excluding congenital
malformations]
53 percent of preterm stillbirths are IUGR
26 percent of term stillbirths are growth
restricted.
* AGA - appropriate for gestational age
Perinatal Mortality in IUGR:

* Ethnic group
* Parity
* Weight
* Height
Determinant of birth weight such as maternal

MORTALITY & MORBIDITY
• Fetal demise• Birth asphyxia• Meconium
aspiration• Neonatal
hypoglycemia
• Hypothermia• Abnormal neurological
development• Higher risks of
degenerative diseases (eg. hypertension, medical renal disease, vascular disease, diabetes Barkers hypothesis) in adulthood.*
Barker DJP. The long term outcome of retarded fetal growth. Clin Obst Gynecol 1997;40:853–63.

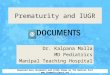
A late pregnancy insult such as
placental insufficiency would
affect cell size.
Asymmetrical Symmetrical
An early insultdue to :
chemicalviral
aneuploidyaffect Cell size & Cell
num.
Types of IUGR

In asymmetrical IUGR The
ratio of brain weight to liver
weight in the last 12 wk of
pregnancy is increased to
5/1 or more

Detection of IUGR:Clinical methods:
• Abdominal palpation, • Weekly measurement of symphyseal fundal
height[SFH]
• Abdominal girth.
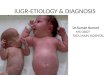
There is enough evidence that SFH measurement performs better if the charts used to plot SFH are customised to match particular variables affecting fetal growth in fetuses of different mothers

Customised charts Mrs SmallMrs Small Mrs BigMrs Big

Role of Ultrasound: USG biometric parameters:
• Abdominal circumference[AC]
• estimated fetal weight[EFW],
• Femoral length[FL],
• head circumference[HC],
• Biparietal diameter[BPD]
USG Prognostic parameters:
•Growth velocity,
•Amniotic fluid volume[AFV],
•Uterine artery Doppler,
•Cerebral artery Doppler
•umbilical artery Doppler,
•Umbilical venous Doppler,
• biophysical profile.
The growth velocity is the most sensitive indicator of fetal growth. for symmetric and asymmetric IUGR AC is a good indicator
[sensitivity of > 95% when AC is <2.5th percentile]Customiosed charts are available for most parameters

• Umbilical artery Doppler[UAD]: primary surveillance tool. When an anomaly scan and umbilical artery Doppler are normal, the small fetus is likely to be a ‘normal small fetus’
• Amniotic fluid volume[AFI] measurement: Reference range for AFI has been devised for Indian subset of population.*
• Biophysical Profile[BPP] There is evidence from uncontrolled observational studies that biophysical profile in high-risk women has good negative predictive value, fetal death is rare in women with a normal biophysical profile
• Use of cardiotocography [CTG] antepartum to assess fetal condition is not associated with better perinatal outcome; however daily NST is practiced in many centers with its own efficiency.
Monitoring IUGR pregnancy
*Khadilkar SS, Desai SS, Tayade SM, Purandare CN. Amniotic fluid index in normal pregnancy: an assessment of gestation specific reference values among Indian women.J Obstet Gynaecol Res. 2003 Jun;29(3):136-41

Management
Once a SGA is suspected ,
intensive effort should be made
to determine if IUGR is present
and if so, its type and etiology.

If LMP not sure:• First ANC visit SFH•First trimester ultrasound scanning (USS) with an accuracy to within 5 days,
•Second trimester scanning should be accurate to within 10 days.
Accurate dating of the pregnancy is essential in the use of any parameter. In the absence of reliable dating, serial scans at two- or three-week intervals must be performed to identify IUGR. It should always be remembered that each parameter measured has an error potential of about one week up to 20 gestational weeks, about two weeks from 20 to 36 weeks of gestation, and about three weeks thereafter.
Certainty of Gestational Age

Significant oligohydraminos is
indication for delivery if G.A has reached>34 wk. Gestation Specific AFI chart in Indian women have been devised
by Khadilkar et al 2003

Gestation specific reference range for AFI values in normal pregnancy amongst Indian women :
Khadilkar SS,Desai SS, Tayade SM,PurandareCNJ.Obstet.Gynaecol Res vol29,no.3:136-141,June 2003
Gestation specific percentile values of AFI in Indian Women
Weeks of Gestation
5th 50th 95th Number of cases
16--19 80 130 180 19 20 84 132 184 15 21 87 139 194 10 22 88 142 196 12 23 88 145 198 12 24 90 147 200 16 25 92 157 212 20 26 93 158 214 30 27 93 169 219 20 28 92 162 224 22 29 88 150 221 19 30 84 148 218 24 31 83 146 213 32 32 83 144 199 45 33 80 140 195 33 34 76 142 190 28 35 74 138 185 23 36 72 135 183 14 37 70 128 182 36 38 68 122 176 20 39 61 115 168 24 40 59 113 166 24
41--42 54 111 152 19 Total
n= 517
[gestation specific values< than 5th percentile: oligohydramnios and > 95thpercentile: polyhydramnios ]

Birthweight gestation
specific charts

Fetal weight percentiles throughout gestation.

If the fetus is in the lower centiles
but continues to grow within those
centiles, this is reassuring but if
growth is slow and the fetus is
falling into lower centiles, this is
cause for concern.

IUGR. REMOTE FROM TERM
before 34 wkNormal Amniotic volumeNormalfetal surveillance
Observation
USG is repeated at interval of 2 wk

Rarely amniocentesis for
assessment of pulmonary
maturity may be helpful in
clinical decision making.

Many clinicians advised a
program of modified rest in
the lateral recumbent
position in which placental
perfusion is maximized.
Many clinicians advised a
program of modified rest in
the lateral recumbent
position in which placental
perfusion is maximized.

Early anti platelet therapy with low dose aspirin may prevent
uretroplacental thrombosis
placental infarction
idiopathic IUGR in women with a
history of recurrent severe IUGR

LABOR AND
DELIVERY

There is general consensus that
delivery is indicated when the
risk of fetal death or significant
morbidity from continued
intrauterine existence is greater
than the risk of prematurity.

Hospitalisation, bed rest, oxygen therapy, plasma volume expansion.Maternal nutrient therapy: Macronutrients. Balanced protein energy supplementation. High protein diet/ IV amino acids, Glucose powder intake, DHA supplementation
Micronutrients Vitamins and mineral supplementation. Betamimetics, Calcium channel blockers,Hormonal therapy
Empirical treatment

Delivery room:
It should be equipped with Intrapartum monitoring with continuous
cardiotocography
ppropriate neonatal staff and facilities to care for the IUGR affected
newborn [NICU].
The mode of delivery
It is based on the gestation, fetal condition, and cervical status
In cases where there is evidence of fetal academia, caesarean section may
be appropriate.
The Growth Restriction Intervention Trial (GRIT)* concluded that, in
general, at gestations less than 31 weeks, delivery is best delayed. The
GRIT has not provided evidence to date that ‘early delivery to pre-empt
severe hypoxia and acidosis reduces any adverse outcome’. Resnik R. Fetal growth restriction: Management. 2005 UpToDate. Available at: www.uptodate.com
Delivery :

IUGR is the result of insufficient
placental function
↓A.F cord compression
breech presentation
↑c/s

When to deliver?Individualised approach most appropriate
General guidelines:
Indications for delivery:• (PED)end diastolic flow is absent or reversed, admission,
close surveillance and administration of steroids are required.
• If other surveillance results are abnormal (poor biophysical profile, pulsations on venous Doppler),
• If growth is static between two scans 2 weeks apart in a fetus more than 32 weeks, (once steroids have been administered to those 34 weeks).
• If gestation is over 34 weeks, even if other results are normal, delivery may be considered.
Continuation of pregnancy• (PED), end diastolic flow normal: delay delivery until at least
37 weeks, provided other surveillance findings are normal.

Prolonged symmetrical IUGR is likely to be
followed by slow growth after birth.
The asymmetrically GR is more likely to catch
up after birth.
Postnatal Development of the IUGR Baby

* Accurate dating is essential to allow careful monitoring
* Customisation of fetal growth assessment SFH, birth
weight, AC, AFI charts assists in distinguishing the
healthy small fetus from one affected by IUGR.
* Empirical treatment helps to some extent but no
enough evidence exists
* Balancing the risks and benefits of continuation of
pregnancy to attain maturity
* Ensure delivery of the baby at the optimal time,
Conclusion

Source:
RCOG guideline no.31 ,1-16 , 2003,
The Investigation and Management Of
The Small-For-Gestational-Age Fetus