Embed Size (px)
Citation preview

www.medicinafetalbarcelona.org/
SGA vs. (late) IUGREduard Gratacós
Maternal-Fetal Medicine DepartmentHospital Clínic, Universidad de Barcelona
www.fetalmedicinebarcelona.org

www.medicinafetalbarcelona.org/
IUGR vs SGA in late-onset cases
Implications for perinatal outcome
Implications for long-term outcome

www.medicinafetalbarcelona.org/
IUGR vs SGA in late-onset cases
Implications for perinatal outcome
Implications for long-term outcome

www.medicinafetalbarcelona.org/
Savchev 2013

www.medicinafetalbarcelona.org/
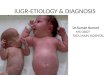
The discovery of UA and hemodynamics of IUGR
Savchev 2013

www.medicinafetalbarcelona.org/
Constitutionally small Placental insufficiency Extrinsic cause
Primary fetal defect
The discovery of UA and hemodynamics of IUGR
IUGR = abnormal UA Doppler
Savchev 2013

www.medicinafetalbarcelona.org/
Constitutionally small Placental insufficiency Extrinsic cause
Primary fetal defect
SGA IUGR
The discovery of UA and hemodynamics of IUGR
IUGR = abnormal UA Doppler
Savchev 2013

www.medicinafetalbarcelona.org/
Constitutionally small Placental insufficiency Extrinsic cause
Primary fetal defect
SGA IUGR
The discovery of UA and hemodynamics of IUGR
IUGR = abnormal UA Doppler
20 30 4025 35 Savchev 2013

www.medicinafetalbarcelona.org/
Constitutionally small Placental insufficiency Extrinsic cause
Primary fetal defect
SGA IUGR
The discovery of UA and hemodynamics of IUGR
IUGR = abnormal UA Doppler
20 30 4025 35
0
N cases
N cases
Savchev 2013

www.medicinafetalbarcelona.org/
Constitutionally small Placental insufficiency Extrinsic cause
Primary fetal defect
SGA IUGR
The discovery of UA and hemodynamics of IUGR
IUGR = abnormal UA Doppler
20 30 4025 35
0
N cases
N cases
Savchev 2013

www.medicinafetalbarcelona.org/
Constitutionally small Placental insufficiency Extrinsic cause
Primary fetal defect
SGA IUGR
The discovery of UA and hemodynamics of IUGR
IUGR = abnormal UA Doppler
20 30 4025 35
0
N cases
N cases
UA Doppler +(EARLY-ONSET)
Savchev 2013

www.medicinafetalbarcelona.org/
Constitutionally small Placental insufficiency Extrinsic cause
Primary fetal defect
SGA IUGR
The discovery of UA and hemodynamics of IUGR
IUGR = abnormal UA Doppler
20 30 4025 35
0
N cases
N cases
UA Doppler +(EARLY-ONSET)
UA Doppler N(LATE-ONSET)
Savchev 2013

www.medicinafetalbarcelona.org/
0"
20"
40"
60"
80"
100"
120"
20" 21" 22" 23" 24" 25" 26" 27" 28" 29" 30" 31" 32" 33" 34" 35" 36" 37" 38" 39" 40" 41"
Num
ber'o
f'cases'
Week's'gesta2on'
UA"abnormal"UA"normal"

www.medicinafetalbarcelona.org/
e<p95
SGA
SGA = constitutionally small?

www.medicinafetalbarcelona.org/
Significant increase in the risk of adverse perinatal outcome
Hershkovitz et al. Ultrasound Obstet Gynecol 2000
Severi et al. Ultrasound Obstet Gynecol 2002
Figueras et al . Eur J Obstet Gynecol Reprod Biol 2008
e<p95
SGA
SGA = constitutionally small?

www.medicinafetalbarcelona.org/
Significant increase in the risk of adverse perinatal outcome
Hershkovitz et al. Ultrasound Obstet Gynecol 2000
Severi et al. Ultrasound Obstet Gynecol 2002
Figueras et al . Eur J Obstet Gynecol Reprod Biol 2008
e<p95
SGA
SGA = constitutionally small?
Significant increase in the risk of adverse neurodevelopment
Eixarch et al. Ultrasound Obstet Gynecol 2008
Severi et al. Ultrasound Obstet Gynecol 2002
Figueras et al . Eur J Obstet Gynecol Reprod Biol 2008

www.medicinafetalbarcelona.org/
0
10
20
30
40
Neonatal acidosis CS for distress Abnormal NBAS Any
%
Figueras 2011
SGA: proportion of perinatal adverse outcomes in 376 consecutive cases

www.medicinafetalbarcelona.org/
IMPACT OF NON-DETECTED IUGR ON LATE FETAL MORTALITYHospital Clínic Barcelona2005-2010
0%
10%
20%
30%
40%
50%
FGR Unknown Others
25%30%
45%
Relevant Condition ReCoDe

www.medicinafetalbarcelona.org/
IMPACT OF NON-DETECTED IUGR ON LATE FETAL MORTALITYHospital Clínic Barcelona2005-2010
0%
10%
20%
30%
40%
50%
FGR Unknown Others
25%30%
45%
Relevant Condition ReCoDe
Classification of stillbirth by relevant condition at birth (ReCoDe): population-based cohort studyGardosi et al. BMJ 2005
N=2625 stillbirths
IUGR as relevant condition identified in 43-60%

www.medicinafetalbarcelona.org/
FETAL DETERIORATION IN PLACENTAL INSUFFICIENCY EARLY VS LATE IUGR (>34s)
PLACENTAL DISEASE COMPENSATED HYPOXIA DECOMPENSATED HYPOXIA SERIOUS INJURYDEATH
cardiac ischemiaDiastolic failure
Systolic cardiac failure
Centralization
Increment placental impedance
growth
MIDDLE CEREBRAL A.
UMBILICAL A.
DUCTUS VENOSUS
CTG / BPP ABNORMAL
UTERINE ARTERY

www.medicinafetalbarcelona.org/
FETAL DETERIORATION IN PLACENTAL INSUFFICIENCY EARLY VS LATE IUGR (>34s)
PLACENTAL DISEASE COMPENSATED HYPOXIA DECOMPENSATED HYPOXIA SERIOUS INJURYDEATH
cardiac ischemiaDiastolic failure
Systolic cardiac failure
Centralization
Increment placental impedance
growth
MIDDLE CEREBRAL A.
UMBILICAL A.
DUCTUS VENOSUS
CTG / BPP ABNORMAL
Placental injury <30%
UTERINE ARTERY

www.medicinafetalbarcelona.org/
FETAL DETERIORATION IN PLACENTAL INSUFFICIENCY EARLY VS LATE IUGR (>34s)
PLACENTAL DISEASE COMPENSATED HYPOXIA DECOMPENSATED HYPOXIA SERIOUS INJURYDEATH
cardiac ischemiaDiastolic failure
Systolic cardiac failure
Centralization
Increment placental impedance
growth
MIDDLE CEREBRAL A.
UMBILICAL A.
DUCTUS VENOSUS
CTG / BPP ABNORMAL
Placental injury <30%
UTERINE ARTERY

www.medicinafetalbarcelona.org/
FETAL DETERIORATION IN PLACENTAL INSUFFICIENCY EARLY VS LATE IUGR (>34s)
PLACENTAL DISEASE COMPENSATED HYPOXIA DECOMPENSATED HYPOXIA SERIOUS INJURYDEATH
cardiac ischemiaDiastolic failure
Systolic cardiac failure
Centralization
Increment placental impedance
growth
MIDDLE CEREBRAL A.
UMBILICAL A.
DUCTUS VENOSUS
CTG / BPP ABNORMAL
Placental injury <30%
mild hypoxiano cardiovascular adaptation
UTERINE ARTERY

www.medicinafetalbarcelona.org/
FETAL DETERIORATION IN PLACENTAL INSUFFICIENCY EARLY VS LATE IUGR (>34s)
PLACENTAL DISEASE COMPENSATED HYPOXIA DECOMPENSATED HYPOXIA SERIOUS INJURYDEATH
Centralization
Increment placental impedance
growth
MIDDLE CEREBRAL A.
UMBILICAL A.
CTG / BPP ABNORMAL
Placental injury <30%
mild hypoxiano cardiovascular adaptation
UTERINE ARTERY

www.medicinafetalbarcelona.org/
FETAL DETERIORATION IN PLACENTAL INSUFFICIENCY EARLY VS LATE IUGR (>34s)
PLACENTAL DISEASE COMPENSATED HYPOXIA DECOMPENSATED HYPOXIA SERIOUS INJURYDEATH
Centralization
Increment placental impedance
growth
MIDDLE CEREBRAL A.
UMBILICAL A.
CTG / BPP ABNORMAL
Placental injury <30%
mild hypoxiano cardiovascular adaptation
minimal tolerance to hypoxia
UTERINE ARTERY

www.medicinafetalbarcelona.org/
FETAL DETERIORATION IN PLACENTAL INSUFFICIENCY EARLY VS LATE IUGR (>34s)
PLACENTAL DISEASE DECOMPENSATED HYPOXIA SERIOUS INJURYDEATH
Centralization
Increment placental impedance
growth
MIDDLE CEREBRAL A.
UMBILICAL A.
CTG / BPP ABNORMAL
Placental injury <30%
mild hypoxiano cardiovascular adaptation
minimal tolerance to hypoxia
UTERINE ARTERY

UtA >p95
CPR <p5 EFW CENTILE <3
Prognostic criteria of “poor outcome”-SGACS for distress and/or neonatal acidosis
N=447 SGA + 447 controls
Figueras 2012

UtA >p95
CPR <p5 EFW CENTILE <3
Prognostic criteria of “poor outcome”-SGACS for distress and/or neonatal acidosis
N=447 SGA + 447 controls
Figueras 2012

UtA >p95
CPR <p5 EFW CENTILE <3
0%
10%
20%
30%
40%
50%
Controls All normal Any abnormal
Prognostic criteria of “poor outcome”-SGACS for distress and/or neonatal acidosis
N=447 SGA + 447 controls
Figueras 2012

UtA >p95
CPR <p5 EFW CENTILE <3
0%
10%
20%
30%
40%
50%
8%
Controls All normal Any abnormal
Prognostic criteria of “poor outcome”-SGACS for distress and/or neonatal acidosis
N=447 SGA + 447 controls
Figueras 2012

UtA >p95
CPR <p5 EFW CENTILE <3
0%
10%
20%
30%
40%
50%
8%11%
Controls All normal Any abnormal
Prognostic criteria of “poor outcome”-SGACS for distress and/or neonatal acidosis
N=447 SGA + 447 controls
Figueras 2012

UtA >p95
CPR <p5 EFW CENTILE <3
0%
10%
20%
30%
40%
50%
8%11%
40%
Controls All normal Any abnormal
%
Prognostic criteria of “poor outcome”-SGACS for distress and/or neonatal acidosis
N=447 SGA + 447 controls
Figueras 2012

www.fetalmedicinebarcelona.org/
Distribution of cases when IUGR = abnormal CPR or UtA or EFW<p3
Savchev 2013

Neurodevelopment
-20
-10
0
10
20
Choline Creatine Glutamine PheAla Tyrosine Valine Leucine
* *
*
*
* *
*
**
** *
*
*
Metabolomics in cord blood of different types of IUGR/SGA Percentage of variation in comparison with normally grown fetuses
early IUGRlate IUGRSGA
Sanz, PLoS One 2013
Placental transport
Hypercatabolic state
Acute vs. chronic starvation

www.medicinafetalbarcelona.org/
IUGR vs SGA in late-onset cases
Implications for perinatal outcome
Implications for long-term outcome

www.medicinafetalbarcelona.org/docencia
Late-onset intrauterine growth restriction vs. small-for-gestational age(submitted)

www.medicinafetalbarcelona.org/docencia
Late-onset intrauterine growth restriction vs. small-for-gestational age(submitted)
SGA
40% of late-SGA with 11 % risk (14% of all adverse outcomes)

www.medicinafetalbarcelona.org/docencia
Late-onset intrauterine growth restriction vs. small-for-gestational age(submitted)
Late-IUGR
SGA
60% of late-SGA with 40% risk (86% of all adverse outcomes)
40% of late-SGA with 11 % risk (14% of all adverse outcomes)

www.medicinafetalbarcelona.org/
Prediction of cesarean section for fetal distress after labor induction in term SGA fetuses with Doppler signs of brain sparing (N=202)
Cruz et al, 2010
(OVERALL RISK OF CS AFTER INDUCTION 80 %)
0"
10"
20"
30"
40"
50"
60"
70"
Cesarean"sec1on"for"distress"
Neonatal"acidosis"
AGA"
SGA"normal"MCA"
SGA"abnormal"MCA"

www.fetalmedicinebarcelona.org/
c
Spontaneous/Induction
Labor Induction
Induction/Elective CSLate
-IUGR
SGA>
p3
Late-onset IUGR vs SGAProtocol for management of delivery
4/21
36-3
737
-38
37-4
1

www.medicinafetalbarcelona.org/docencia
650 SGA >37 weeks
Induction versus expectant monitoring for intrauterine growth restriction at term: randomised equivalence trial (DIGITAT). BMJ 2011
12/21
Authors’ conclusionDespite lack of differences, it is rational to choose induction to prevent possible neonatal morbidity and stillbirth.

www.medicinafetalbarcelona.org/
IUGR vs SGA in late-onset cases
Implications for perinatal outcome
Implications for long-term outcome

Neurobehavioral performance of term SGA newborns
* **
**
* p <0.05Adjusted for GA, maternal age, socioeconomic status and smoking
Satchev, 2012Geva 2008
Figueras 2008Eixarch 2010
N=120 SGA vs 100 AGA
* * *
Bay
ley
Sco
re
20
40
60
80
100
120
cognitive language motor socio-emotional adaptivebehavior
* * *

Neurobehavioral performance of term SGA newborns
* **
**
* p <0.05Adjusted for GA, maternal age, socioeconomic status and smoking
Satchev, 2012Geva 2008
Figueras 2008Eixarch 2010
N=120 SGA vs 100 AGA
* * *
Bay
ley
Sco
re
20
40
60
80
100
120
cognitive language motor socio-emotional adaptivebehavior
* * *
No differences in relation with prenatal prognostic factors
(EFW<p3, CPR or UtA Doppler)

control IUGR
Crispi 2010
Impact of prenatal severity on cardiovascular programming in late-IUGR

control IUGR
Crispi 2010
Impact of prenatal severity on cardiovascular programming in late-IUGR
Fetuses EFW<p10 evaluated at 5 years
Classified by CPR, p3 and UtA Doppler:•All normal: SGA•Any abnormal: late-IUGR

control IUGR
Crispi 2012
Crispi 2010
Impact of prenatal severity on cardiovascular programming in late-IUGR
Fetuses EFW<p10 evaluated at 5 years
Classified by CPR, p3 and UtA Doppler:•All normal: SGA•Any abnormal: late-IUGR

EFW<p10
(HYPOTHESIS ON) DEGREES OF SEVERITY IN LATE-ONSET IUGR

EFW<p10
CPR (UA/MCA)Uterine ArteryEFW Centile
(HYPOTHESIS ON) DEGREES OF SEVERITY IN LATE-ONSET IUGR

Findings Perinatal Outcome Long Term Outome
EFW<p10
CPR (UA/MCA)Uterine ArteryEFW Centile
(HYPOTHESIS ON) DEGREES OF SEVERITY IN LATE-ONSET IUGR

Findings Perinatal Outcome Long Term Outome
All normal(good reserve)
“Normal” Abnormal
EFW<p10
CPR (UA/MCA)Uterine ArteryEFW Centile
(HYPOTHESIS ON) DEGREES OF SEVERITY IN LATE-ONSET IUGR

Findings Perinatal Outcome Long Term Outome
All normal(good reserve)
“Normal” Abnormal
One or more abnormal(no reserve)
Higher risk poor outcome Abnormal
EFW<p10
CPR (UA/MCA)Uterine ArteryEFW Centile
(HYPOTHESIS ON) DEGREES OF SEVERITY IN LATE-ONSET IUGR

Findings Perinatal Outcome Long Term Outome
All normal(good reserve)
“Normal” Abnormal
One or more abnormal(no reserve)
Higher risk poor outcome Abnormal
MCA <p5(hypoxia)
Risk CS >80% Abnormal
EFW<p10
CPR (UA/MCA)Uterine ArteryEFW Centile
(HYPOTHESIS ON) DEGREES OF SEVERITY IN LATE-ONSET IUGR

www.fetalmedicinebarcelona.org/
• 5-7% newborns• detection < 50%• > 40% late pregnancy IUFD• Neurological, cardiovascular and
metabolic impact• diagnosis SGA vs. Late-IUGR
IUGR
SGA?
20 30 4025 35
0
3
3%

www.fetalmedicinebarcelona.org/
• 5-7% newborns• detection < 50%• > 40% late pregnancy IUFD• Neurological, cardiovascular and
metabolic impact• diagnosis SGA vs. Late-IUGR
IUGR
SGA?
20 30 4025 35
0
3
3%
LATE FETAL SMALLNESS (<P10)CLINICAL PROBLEMS
# 1: DIAGNOSISdetection <50%
# 2: POOR PERINATAL OUTCOME (∼50%)• A “Late-IUGR subset” with poorer perinatal
outcome can be identified
# 3: POOR LONG TERM OUTCOME (∼50%)Fetal programming
No means to select high risk groups

www.fetalmedicinebarcelona.org/
• 5-7% newborns• detection < 50%• > 40% late pregnancy IUFD• Neurological, cardiovascular and
metabolic impact• diagnosis SGA vs. Late-IUGR
IUGR
SGA?
20 30 4025 35
0
3
3%
LATE FETAL SMALLNESS (<P10)CLINICAL PROBLEMS
# 1: DIAGNOSISdetection <50%
# 2: POOR PERINATAL OUTCOME (∼50%)• A “Late-IUGR subset” with poorer perinatal
outcome can be identified
# 3: POOR LONG TERM OUTCOME (∼50%)Fetal programming
No means to select high risk groups
signs adaptation/
severity
yes
no

www.fetalmedicinebarcelona.org/
• 5-7% newborns• detection < 50%• > 40% late pregnancy IUFD• Neurological, cardiovascular and
metabolic impact• diagnosis SGA vs. Late-IUGR
IUGR
SGA?
20 30 4025 35
0
3
3%
LATE FETAL SMALLNESS (<P10)CLINICAL PROBLEMS
# 1: DIAGNOSISdetection <50%
# 2: POOR PERINATAL OUTCOME (∼50%)• A “Late-IUGR subset” with poorer perinatal
outcome can be identified
# 3: POOR LONG TERM OUTCOME (∼50%)Fetal programming
No means to select high risk groups
poorer
perinatal outcome
normal
signs adaptation/
severity
yes
no

www.medicinafetalbarcelona.org/
Late-onset small (EFW<p10) fetuses
Two groups: normal vs poor perinatal outcomesSGA + (EFW<3th, abnormal CPR, UtA or UV flow)=IUGR:
manage as IUGR with abnormal UA
However, long term outcome is similarly poorer.

EFW<p10
SGA IS ASSOCIATED WITH POORER SHORT AND LONG-TERM PROGNOSIS

EFW<p10
Exclusion of primary causes
SGA IS ASSOCIATED WITH POORER SHORT AND LONG-TERM PROGNOSIS

Today: identification of cases with poorer perinatal outcomeSGA + (EFW<3th, abnormal CPR or UtA)=IUGR:
manage as IUGR with abnormal UA
(Tomorrow: improve identification/classification + prediction of long term outcome)
EFW<p10
Exclusion of primary causes
SGA IS ASSOCIATED WITH POORER SHORT AND LONG-TERM PROGNOSIS

MANAGING LATE ONSET IUGR
Eduard GratacósMaternal-Fetal Medicine Department
Hospital Clínic, Universidad de Barcelona
www.medicinafetalbarcelona.org
MANAGING LATE ONSET IUGR
Eduard GratacósMaternal-Fetal Medicine Department
Hospital Clínic, Universidad de Barcelona
www.medicinafetalbarcelona.org