Embed Size (px)
Citation preview
PAEDIATRICSKIN LESIONS
Richie ChackoPaediatric & Nonatal Nursing
Skin Lesions
DefinitionA skin lesion is a superficial growth or patch of the skin that does not resemble the area surrounding it
Primary skin lesions
• Primary skin lesions are variations in color or texture that may be present at birth, such as moles or birthmarks, or that may be acquired during a person's lifetime,such as those associated with infectious diseases (e.g. warts, acne, or psoriasis), allergic reactions (e.g. Hives or contact dermatitis), or environmental agents (e.g. sunburn, pressure, or temperature extremes).
Secondary skin lesions
• Secondary skinlesions :are those changes in the skin that result from primary skin lesions, either as a natural progression or as a result of a person manipulating (e.g. scratching or picking at) a primary lesion.
Primary skin lesions• Macule
A macule is an area of color change less than 1.5 cm diameter. The surface is smooth.
• Patch A patch refers to a large area of color change, with smooth surface.
• Papule Papules are small palpable lesions. The usual definition is that they are less than 0.5 cm diameter, although some authors allow up to 1.5 cm. They are usually visibly raised above the skin surface, and may be solitary or multiple.
• Papules may be sessile, pedunculated, filiform, or verrucous
• Plaque A plaque is a palpable flat lesion greater than 0.5 cm diameter. Most plaques are elevated, but a plaque can also be a thickened area without being visibly raised above the skin surface.
• Nodule A nodule is an enlargement of a papule in three dimensions (height, width, length).
• Vesicle Vesicles are small blisters less than 0.5cm diameter. They are fluid-filled papules, and may be single or multiple.
• Pustule A pustule is a purulent vesicle. It is filled with neutrophils, and may be white, or yellow. Not all pustules are infected.
• Bulla A bulla is a large fluid-filled blister. It may be a single compartment or multiloculated.
• Wheal A wheal is an edematous papule or plaque caused by swelling in the dermis. Whealing often indicates urticaria.
• Purpura Purpura is bleeding into the skin. This may be as petechiae (small red or brown spots), or as ecchymoses (bruises).
• Telangiectasia Telangiectasia is the name given to prominent cutaneous blood vessels.
Secondary skin lesions• Scaling
Scaling is an increase in the dead cells on the surface of the skin (stratum corneum). The scale can be psoriatic-type (large white or silver flakes), pityriasis-type (branny powdery scale), or lichenoid (tightly adherent to skin surface).
• Lichenification Lichenification is caused by chronic rubbing which results in palpably thickened skin with increased skin markings and lichenoid scale. It occurs in chronic eczema eg. atopic dermatitis or lichen simplex.
• Exfoliation Exfoliation is the stratum corneum peeling off, usually occurring after acute inflammation.
• Crusting Crust occurs when plasma exudes through an eroded epidermis. It is rough on the surface and is yellow or brown in color. Bloody crust appears red, purple or black.
• Excoriation An excoriation is a scratch mark. It may be a linear erosion or a picked scratch. Excoriations may occur in the absence of a primary dermatosis.
• Erosion An erosion is caused by loss of the surface of a skin lesion, it is a shallow moist or crusted lesion.
• Fissure A fissure is a thin crack within epidermis or epithelium, and is due to excessive dryness.
• Ulcer An ulcer is full thickness loss of epidermis or epithelium. It may be covered with a dark-colured crust called an eschar.
• Erythroderma Erythroderma is a term used to indicate red skin over the entire body.
Etiology• Affects – >80% of adolescents– >40% of adults over than 25
• Genetics plays a role• Associated with– Disfigurement– Pain– Loss of confidence– Depression
• Effects on quality of life are comparable to those suffering from chronic diseases like asthma, seizures and diabetes
Risk Factors
• Friction and manipulation• Occlusive products• Close fitting sports equipment• Medications: – Steroids– Antiepileptics– Progestin only contraceptives
• Controversial link between diet and acne although many patients believe that their acne is influenced by certain foods
• Western diet may be associated with acne• Skim milk is associated with acne in teenage
girls• Stress: acne among university students was
associated with exam stress
PATHOPHYSIOLOGYfollicular hyperkeratinization
proliferation +
decreased desquamation of keratinocytes
hyperkeratotic plug(microcomedone)
Sebaceous glands enlarge
Sebum production increases
Growth medium for P. Acnes
plugs provide anaerobicLipid-rich environment
Bacteria thrive
Inflammation results
Chemotactic factors attract neutrophils
Depending on conditions
Non-inflammatory open/closed comedones
Inflammatory papule/pustule/nodule
CLINICAL FEATURESMild acne• Comedomes:– Closed (whiteheads) are closed flesh colored papules 1-
3mm in size– Open (blackheads) are open and the contents of the
comedome oxidizes upon expose to the light (tyrosine is oxidized to melanin)
Moderate acne• Comedomes/Papules/PustulesSevere acne• Papules/Pustules/Nodulocystic lesions
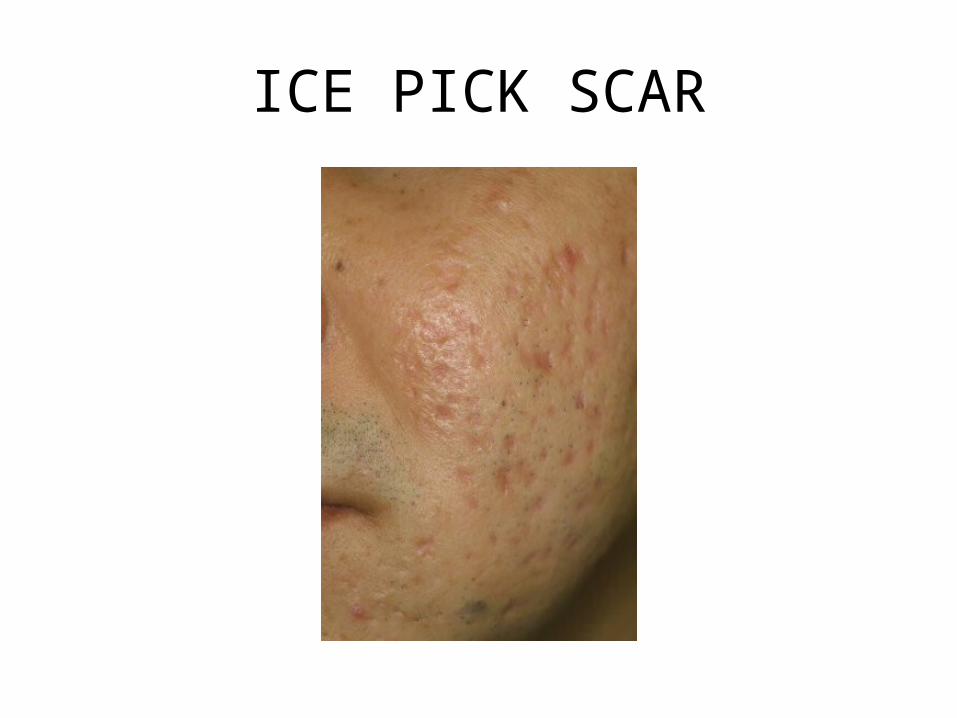
ICE PICK SCAR

THUMBPRINT SCARS
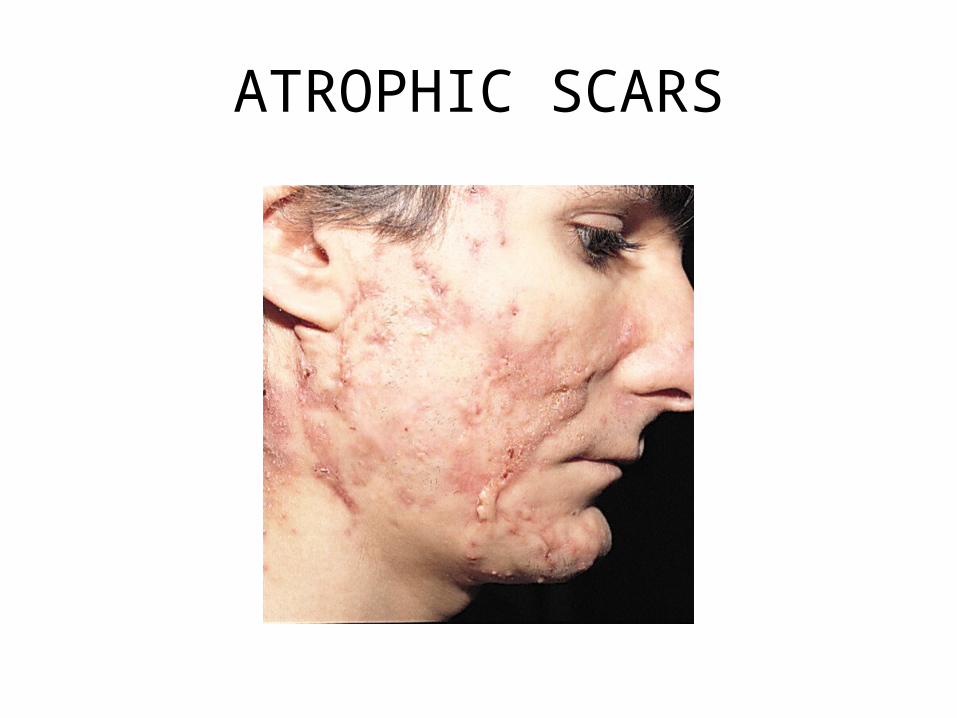
ATROPHIC SCARS
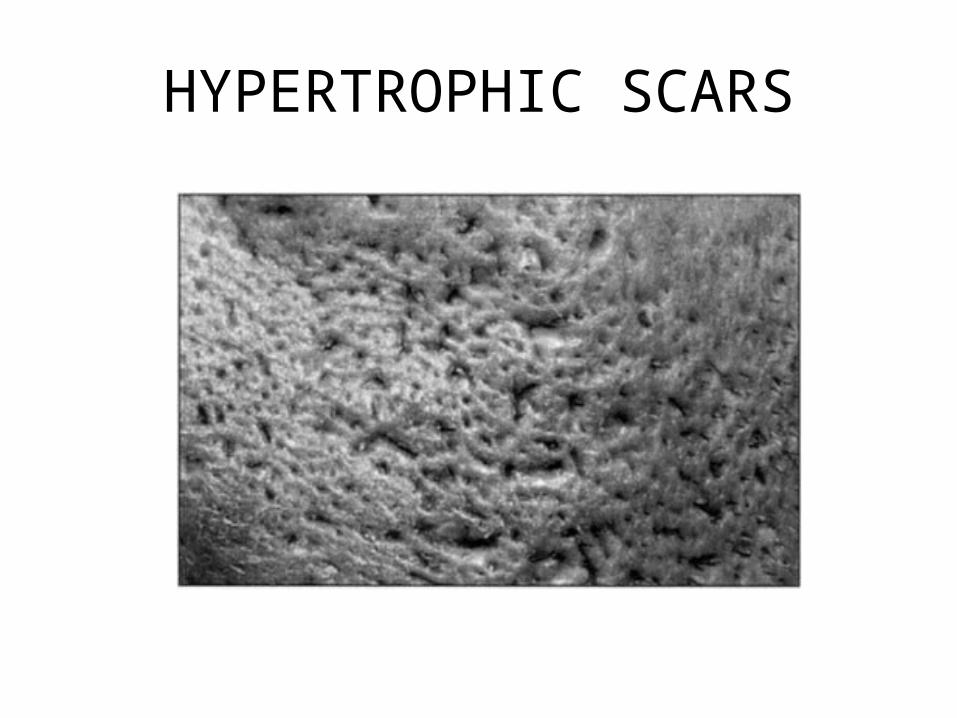
HYPERTROPHIC SCARS
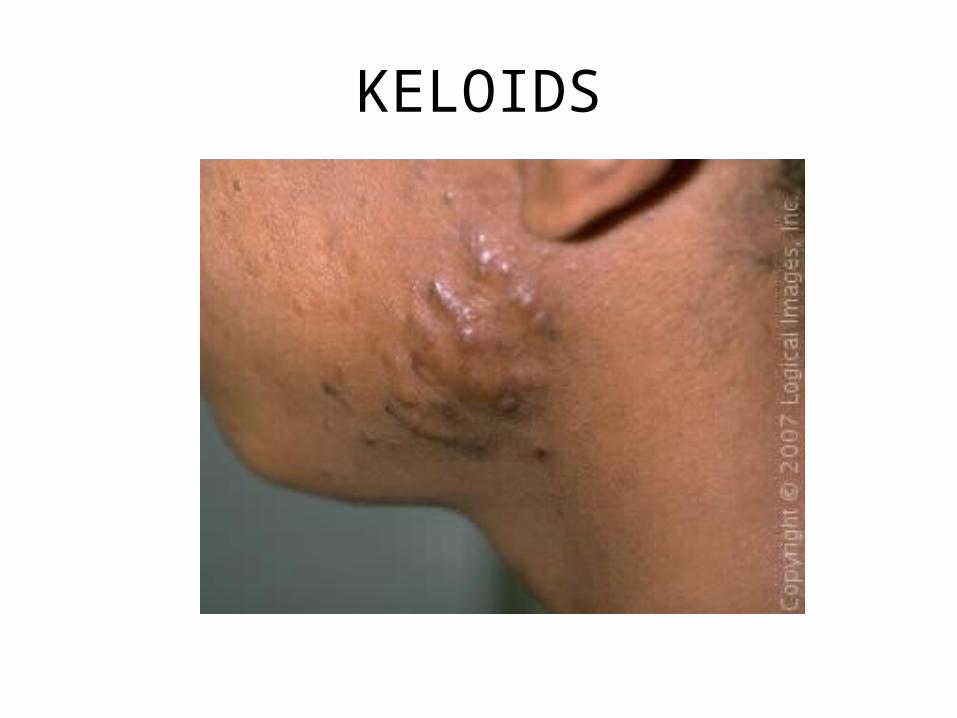
KELOIDS
SEVERE ACNE
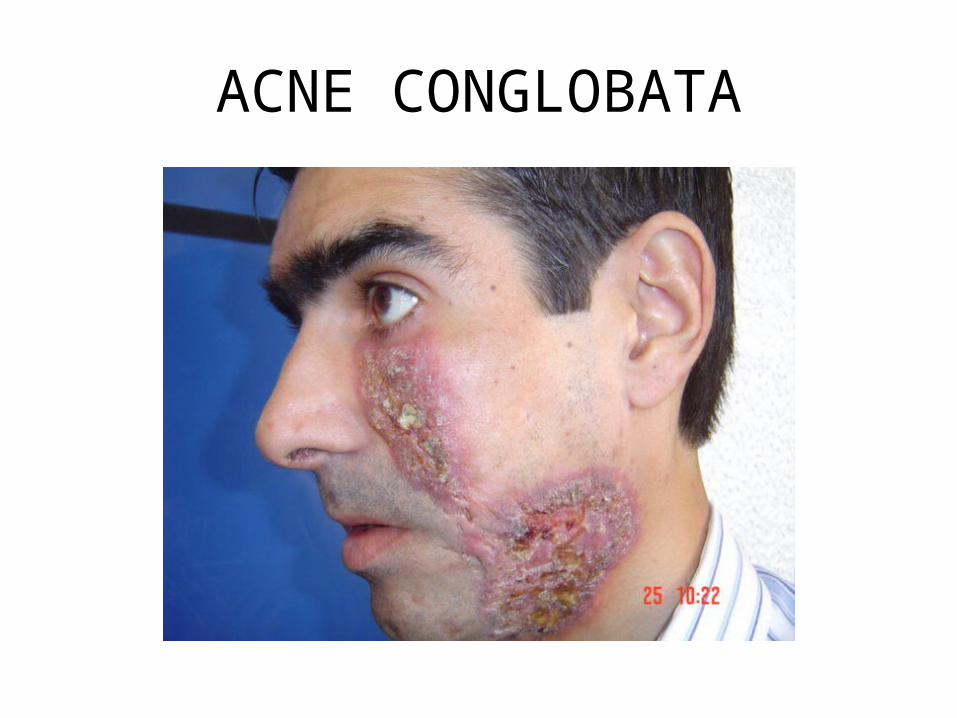
• Acne fulminans– Severe acne in young males in association with
fever, arthritis • Acne conglobata– Comedomes, pustules, foul smelling cysts, sinus
tracts, atrophic and keloid scarring• Treat with high dose steroids
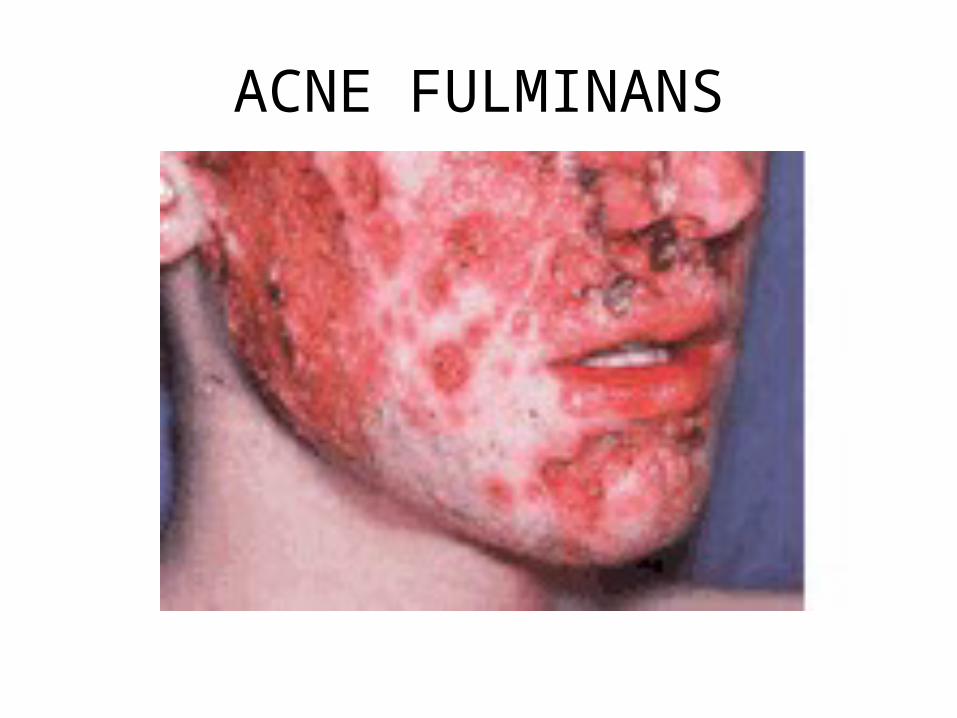
ACNE FULMINANS
DIAGNOSIS
• patient history, physical examination• characteristics of the lesion,• where and how it appears on the patient's body• scrapings or swab samples from lesions forexamination under a microscope• immunofluorescence test• bacterial, fungal, or viral cultures• contrast lighting and subdued lighting test
MEDICAL TREATMENT• Basic skin care– No washing, scrubbing or picking– Cleanse with a gentle soap, may contain salicylic acid,
glycolic acid or benzoyl peroxide– If moisturize use noncomedogenic agent
• Based on skin type, choose appropriate vehicle for topical treatments– Oily (solutions, gels, pledgets)– Combination (lotions)– Dry (cream, ointment)
TOPICAL RETINOIDS• Tretinoin (Retin A), Adapalene (Differin),
Tazarotene (Tazorac)TOPICAL ANTIBIOTICS• Erythromycin, ClindamycinBENZOYL PEROXIDEAZELAIC ACIDSYSTEMIC ANTIBIOTICS• Tetracyclin, Doxycyclin, MinocyclinHORMONAL CONTROL
NURSING MANAGEMENT• Assess the client for the presence of cutaneous lesions• Assess bony prominences, perineum, and dependent and
pruritic areas for pallor, redness, and breakdown.• Implement measures to treat existing cutaneous conditions• Implement measures to prevent additional tissue breakdown• If tissue breakdown occurs or existing breakdown progresses:1. notify appropriate health care provide2. perform care of involved areas as ordered or per standard
hospital procedure.
WARTS
• Warts are a very common, harmless skin infection caused by a virus. For reasons that are not entirely clear, children seem to develop warts more often than adults. This is NOT a sign of a problem with the immune system. the spread can be lessen by discouraging picking, biting or scratching.
Etiology
• Caused by viruses from the human papillomavirus (HPV)
• contagious and commonly found in school-aged children
• They rarely occur in children younger than 2 years.
Pathophysiology• The HPV virus infects the epithelium
• systemic dissemination of the virus does not occur.
• Viral replication occurs in differentiated epithelial cells
• viral particles can be found in the basal layer
• They cause thickening of the stratum layers and large blood vessels.
Symptoms
• Small, fleshy, grainy bumps• Flesh-colored, white, pink or tan• Rough to the touch• Sprinkled with black pinpoints, which are
small, clotted blood vessels
Tests and diagnosis
• Examining the wart• Scraping off the top layer of the wart to check
for signs of dark, pinpoint dots — clotted blood vessels — which are common with warts
• Removing a small section of the wart (shave biopsy) and sending it to a laboratory for identification of HPV and analysis to rule out other types of skin growths
Treatments and drugs
• Stronger peeling medicine (salicylic acid).• Freezing (cryotherapy)• Other acids (bichloroacetic or trichloroacetic
acid)• Laser treatment.
Prevention• To reduce your risk of common warts:• Avoid direct contact with warts. This includes your own warts.• Don't pick at warts. Picking may spread the virus.• Don't use the same emery board, pumice stone or nail clipper
on your warts as you use on your healthy skin and nails.• Don't bite your fingernails. Warts occur more often in skin that
has been broken. Nibbling the skin around your fingernails opens the door for the virus.
• Groom with care. Use a disposable emery board. And avoid brushing, clipping or shaving areas that have warts. If you must shave, use an electric razor.
• Wash your hands carefully after touching your warts or surfaces such as shared exercise equipment.
SCABIES
Human scabies is an intensely pruritic skin infestation caused by the host-specific mite Sarcoptes scabiei hominis. Approximately 300 million cases of scabies are reported worldwide each year.

Definition/ Etiology
• Human scabies is an intensely pruritic skin infestation caused by the host-specific mite Sarcoptes scabiei var hominis.
Pathophysiology
• Transmission of scabies is predominantly through direct skin-to-skin contact
• The mite does not penetrate deeper than the superficial layer of the epidermis
• Within 10 weeks the symptoms of primary infection occurs
Signs and symptoms
• Itching, mainly at night: Itching is the most common symptom.
• Rash: Many people get the scabies rash.• Sores: Scratching the itchy rash can cause sores.• Thick crusts on the skin: Crusts form when a person
develops a severe type of scabies called crusted scabies.
• They appear as serpiginous, grayish, threadlike elevations in the superficial epidermis, ranging from 2-10 mm long.
Nodular scabies• Nodules occur in 7-10% of patients with scabies,
particularly young children. In neonates unable to scratch, pinkish brown nodules ranging in size from 2-20 mm in diameter may develop.
Crusted scabies• In crusted scabies, lesions are often hyperkeratotic and
crusted and cover large areas. Marked scaling is common, and pruritus may be minimal or absent. Nail dystrophy and scalp lesions may be prominent. The hands and arms are the usual locations for lesions, but all sites are vulnerable.
Secondary lesions• These lesions result from scratching, secondary infection,
and/or the host’s immune response against the scabies mites and their products.
Diagnosis
• History collection and Physical examination.-pruritic rash and characteristic linear burrows.• The diagnosis is confirmed by light microscopic
identification of mites, larvae, ova, or scybala (feces) in skin scrapings.
• In rare cases, mites are identified in biopsy specimens
• elevated immunoglobulin E (IgE) titers and eosinophilia
Management• administration of a scabicidal agent (eg, permethrin,
lindane, or ivermectin).• appropriate antimicrobial agent if a secondary
infection has developed.• Pruritus may be partially alleviated with an oral
antihistamine, such as hydroxyzine hydrochloride ,diphenhydramine hydrochloride or cyproheptadine hydrochloride.
• Antihistamine: To control the itch and help you sleep.• Steroid cream: To ease the redness, swelling, and itch.
Nursing Interventions
• Monitor for signs and symptoms of infection• Monitor susceptibility to infection• Limit visitors when necessary• Instruct visitors to wash their hands when
visiting remedy and after leaving the patient• Maintain aseptic environment during the
installation of equipment
• Instruct the patient to wear loose• Keep the skin clean to keep them clean and dry• Monitor the skin will be reddish• Bathe the patient with warm water and soap• Give skin care in the area epidema• Inspection of skin and mucous membranes of
the redness, heat• Inspection of the wound condition• Provide antibiotic therapy if necessary• Teach how to avoid infection