Embed Size (px)
Citation preview
Mr Alasdair Barrie
CT1 Trauma and Orthopaedics
24/3/15
Content Torsion
Exomphalos
Gastroschisis
Oesophageal atresia
Pyloric stenosis
Intussusception
Hischprung’s
Muconeum ileus
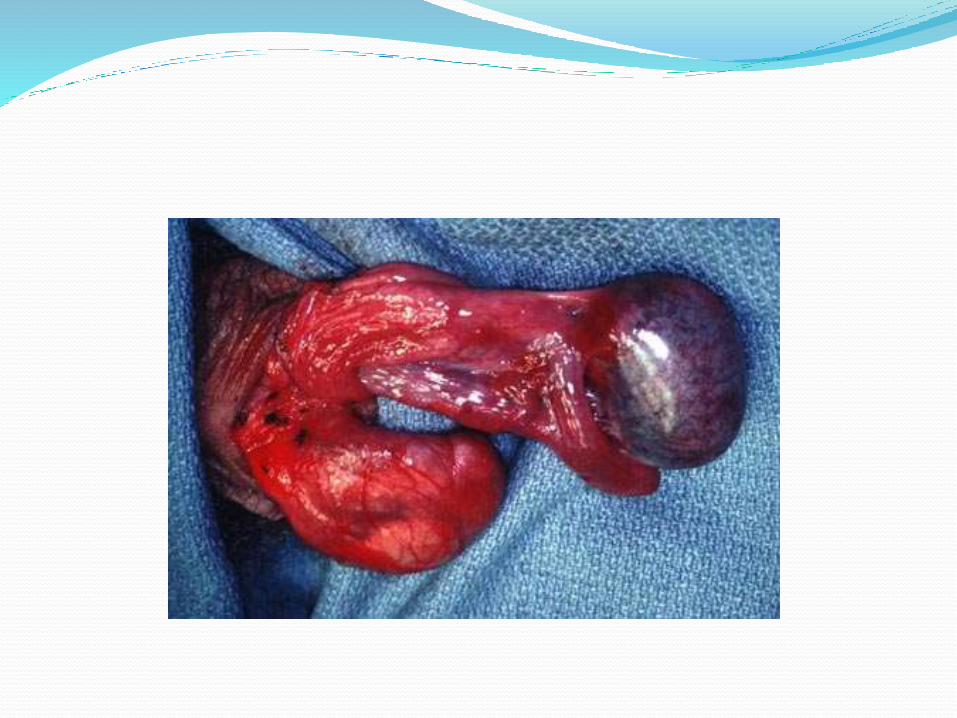
Testicular Torsion Testicular torsion can occur at any age, but is most
common in the neonatal and peripubertal periods.
Presents with severe testicular pain / abdominal pain.
Testicular viability is reduced with increasing time from the onset of symptoms.
Following reduction of a torsion 3-point fixation with an non-absorbable suture should be performed.
The contralateral testis should also be fixed.
Exomphalos An exomphalos (ompalocele) has a sac formed by
perietal peritoneum protruding through a defect in the abdominal wall.
The sac contains intestinal loops, liver and spleen.
It is associated with major congenital anomalies and the prognosis depends on these associated lesions.

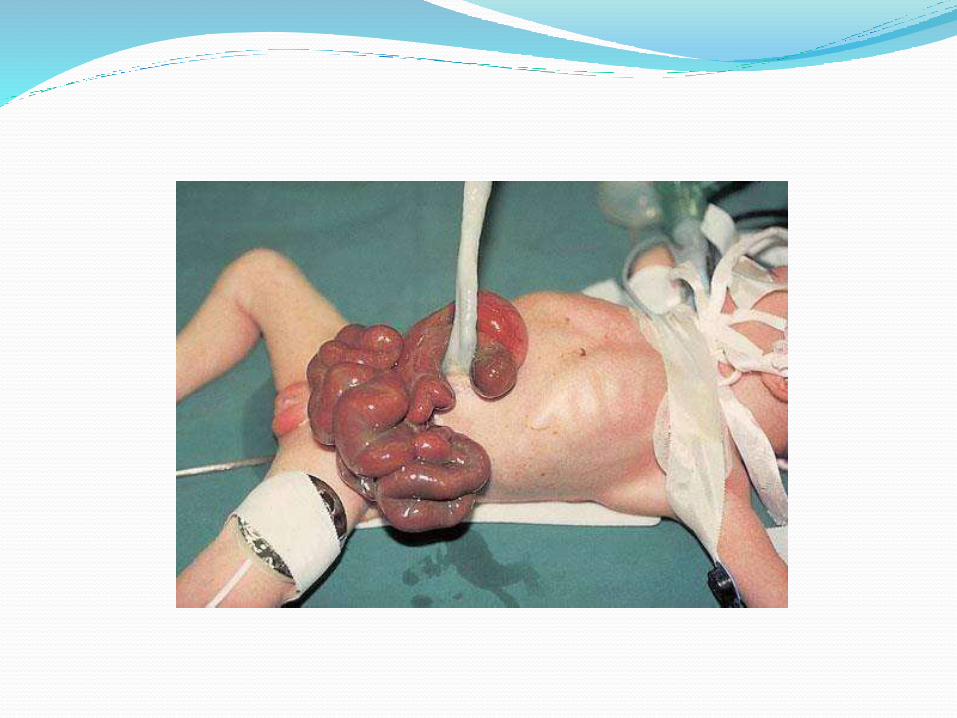
Gastroschisis A gastroschisi never has a sac and the umilical cord
arises from the normal site on the abdominal wall.
It is rarely associated with other congenital anomalies and the prognosis is better than for exomphalos.
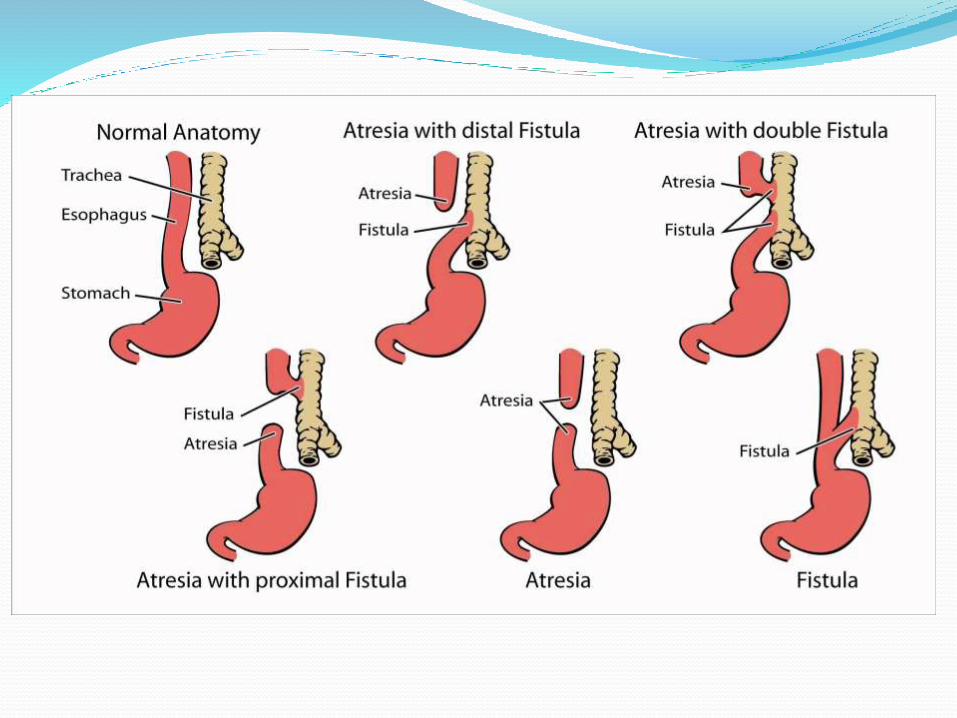
Oesophageal atresia Suspected in a newborn with excessive drooling and in
that is frequently accompanied by choking, coughing and sneezing.
When fed, these infants swallow normally but begin to cough and struggle as the fluid returns through the nose and mouth.
Oesophageal atresia is often associated with tracheo-oesophageal fistula (90%).
Diagnosis my be confirmed by the inability to pass a nasogastric tube more than 10 cm.
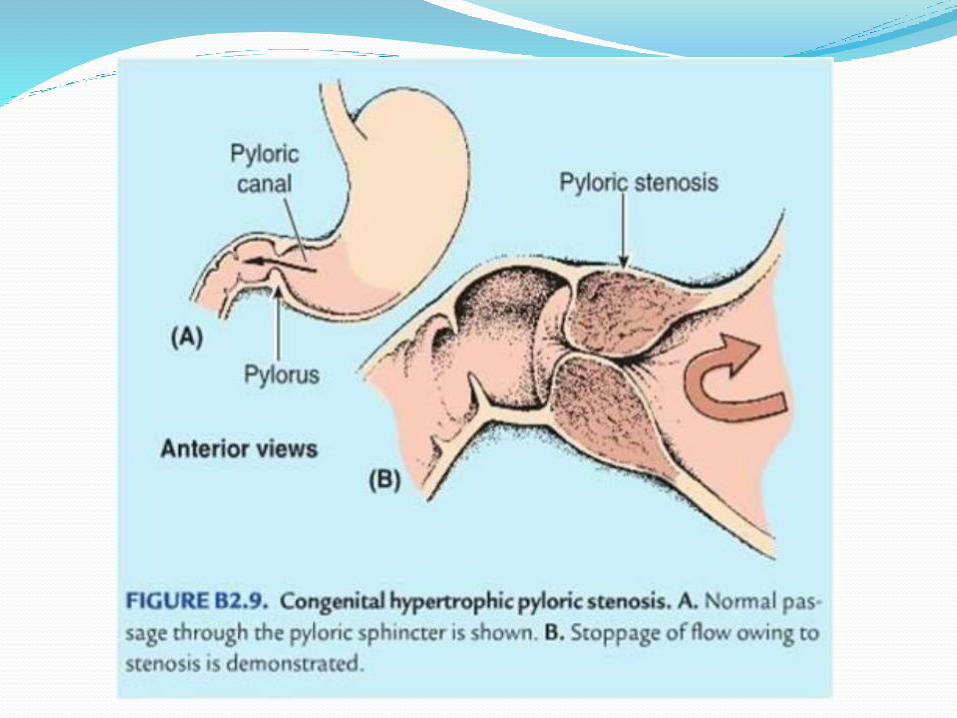
Pyloric stenosis Infantile hypertrophic pyloric stenosis present most
commonly at approximately 6 weeks of age. Patients present with projectile vomiting that is not bile-
stained. It is more common in boys with a male : female ratio of 4:1. There is a strong familial predisposition with 5% of affected
infants having a mother who also developed the problem. Caused by hypertrophy the circular muscle layer in the
pylorus. “Olive shaped mass” Following resuscitation and correction of any electrolyte
abnormality, surgical treatment is by pyloromyotomy(Ramstedt's Operation).
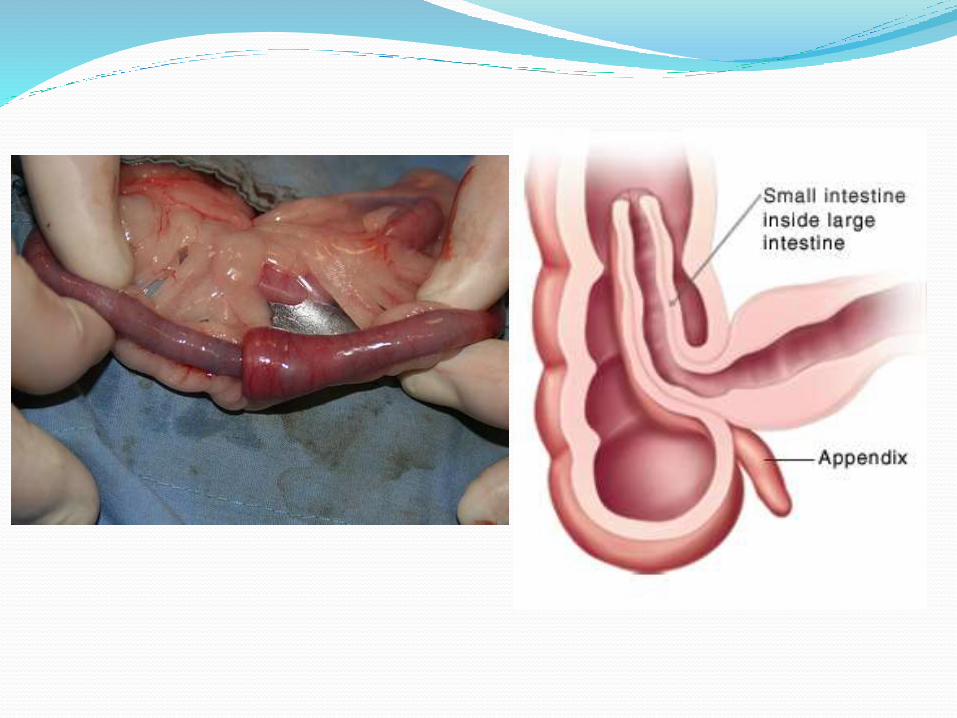
Intussusception Intussusception is the commonest cause of intestinal
obstruction in the 6 to 18 month age group.
The infants usually present with severe intermittent colic, bile-stained vomiting.
‘Redcurrent jelly’ stool.
'sausage-shaped' abdominal mass.
Diagnosis can often be confirmed by a 'doughnut' appearance on ultrasound.
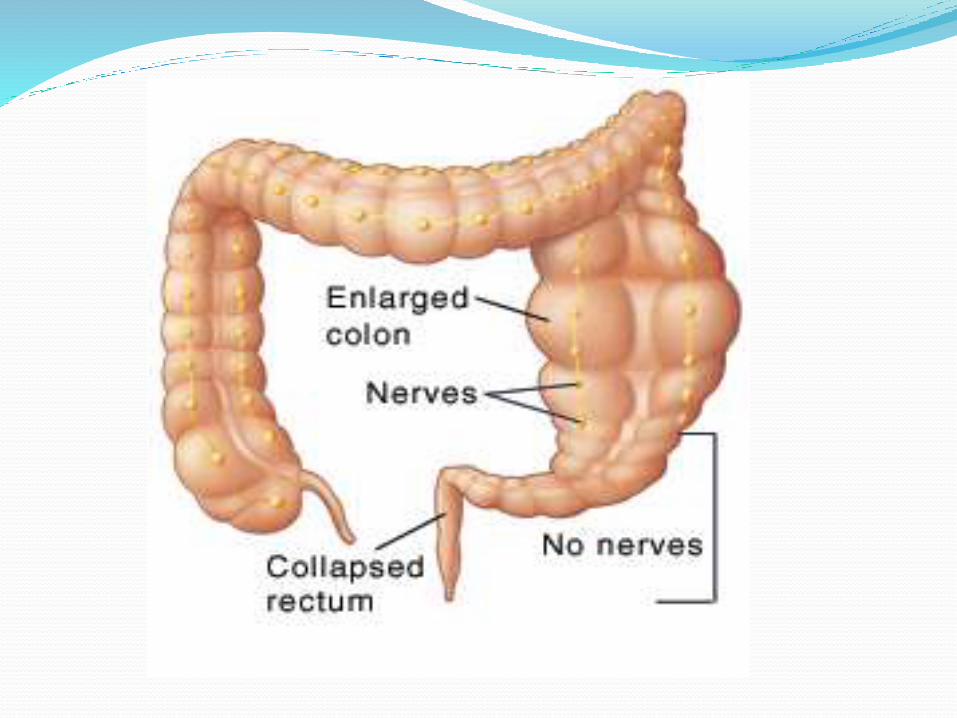
Hirschsprung's Hirschsprung's disease is a common cause of neonatal large
bowel obstruction. Green or brown vomit, explosive stools after a doctor inserts
a finger into the rectum. Failure of migration of ganglion cells to the affected
segment of bowel. This always involves the distal colon but the proximal
extent of the involvement is variable. The segment lacking neurons (aganglionic) becomes
constricted, causing the normal, proximal section of bowel to become distended with feaces.
Diagnosed with biopsy. Treated with resection of affected bowel.
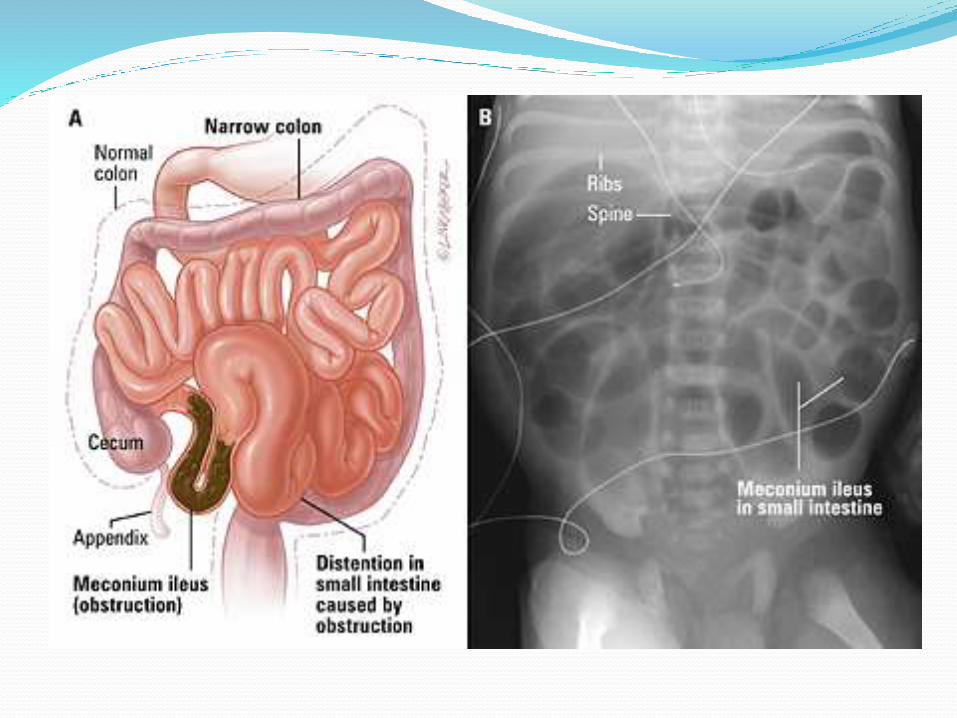
Muconeum ileus Common cause of neonatal intraluminal intestinal
obstruction.
90% of babies pass their first meconium within 24 hours, and 99% within 48 hours.
Over 80% of cases are associated with cystic fibrosis.
In these patients, pancreatic secretions are abnormally viscid and the meconium becomes inspissated in the distal ileum.
Bile-stained vomiting.
A plain abdominal x-ray will show dilated ileal loops and intraluminal 'ground glass' appearance.
Treat with enemas / surgery.
Questions?