Embed Size (px)
Citation preview
Improving the Care of People withLong-Term Conditions who have
joint pain, anxiety and/or depression
Emma Healey
(on behalf of the ENHANCE study team)
Overview
• Background
• Aim of the ENHANCE pilot trial
• Intervention & training development
• Trial design
• Progress to date
• Feedback from CLAHRC SAG
• Next steps

Long Term Conditions (LTCs)
• Majority managed in primary care
• Established systems in place for QOF conditions
• Non-QOF conditions ‘neglected’
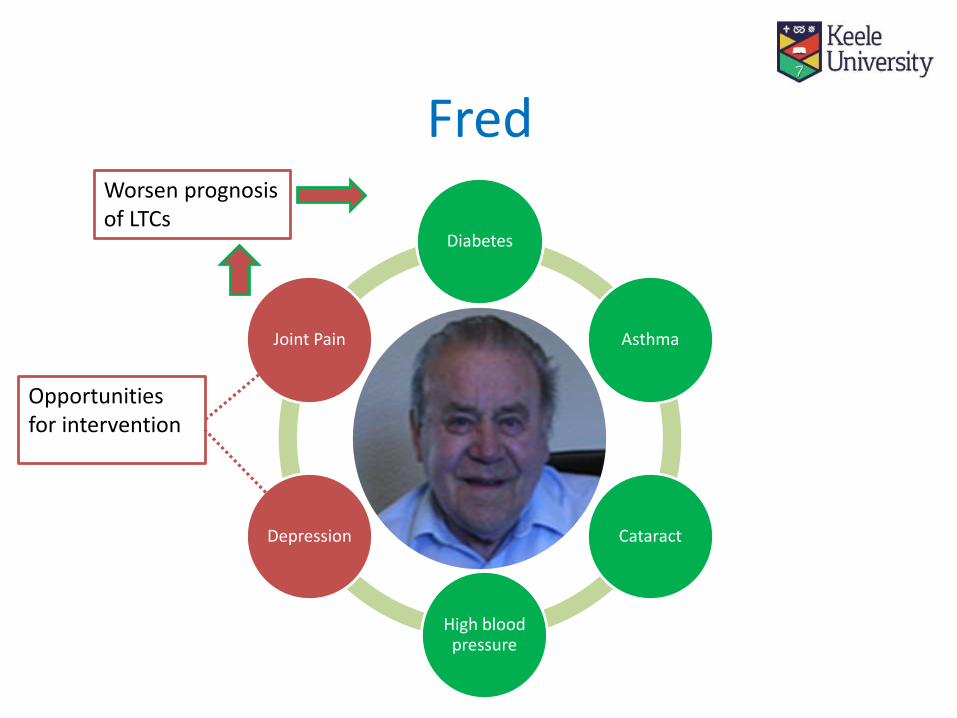
• Osteoarthritis (OA) related pain, anxiety and depression are frequently comorbid with other LTCs yet are seldom prioritised by patient or clinician
• Single disease pathology increasingly uncommon
• May result in higher levels of disability, poorer prognosis and increased health care costs
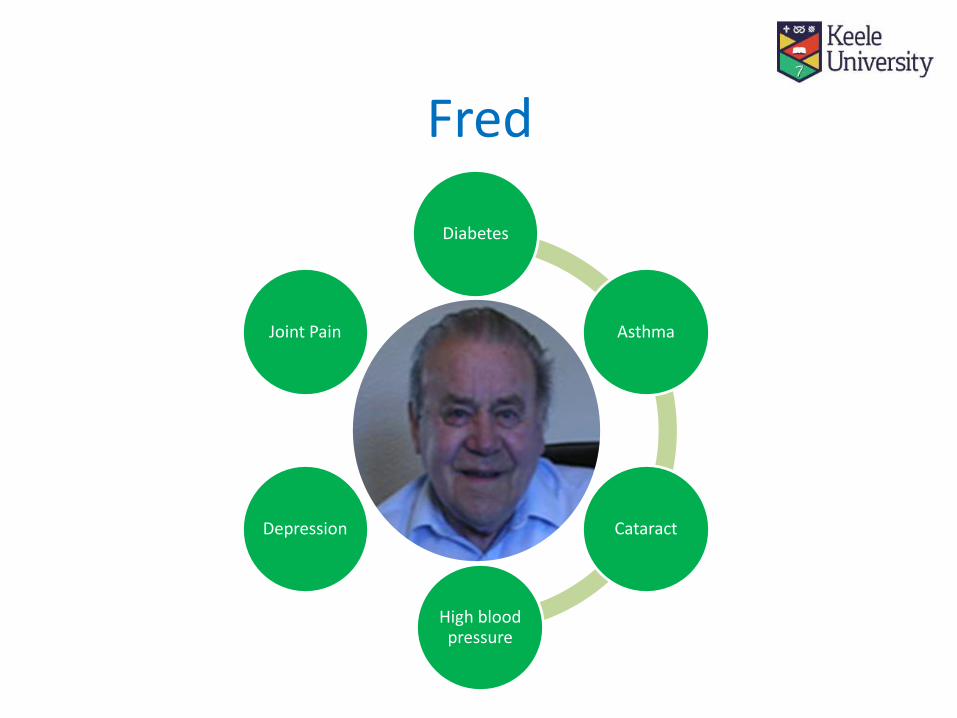
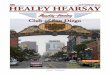
Fred
Diabetes
Asthma
Cataract
High blood pressure
Depression
Joint Pain
Diabetes
Asthma
Cataract
High blood pressure
Depression
Joint Pain
Worsen prognosis of LTCs
Opportunities for intervention
Fred
Hypothesis
The health of people with LTCs can be improved by identifying and initiating treatment of OA related joint pain and / or anxiety and depression at a LTC review

Aim:To examine the feasibility and acceptability of anintegrated approach to LTC management, tackling theunder-diagnosis and under-management of OA-relatedpain and anxiety and/or depression in older adults withother LTCs in primary care.
The ENHANCE pilot trial

Intervention & training development
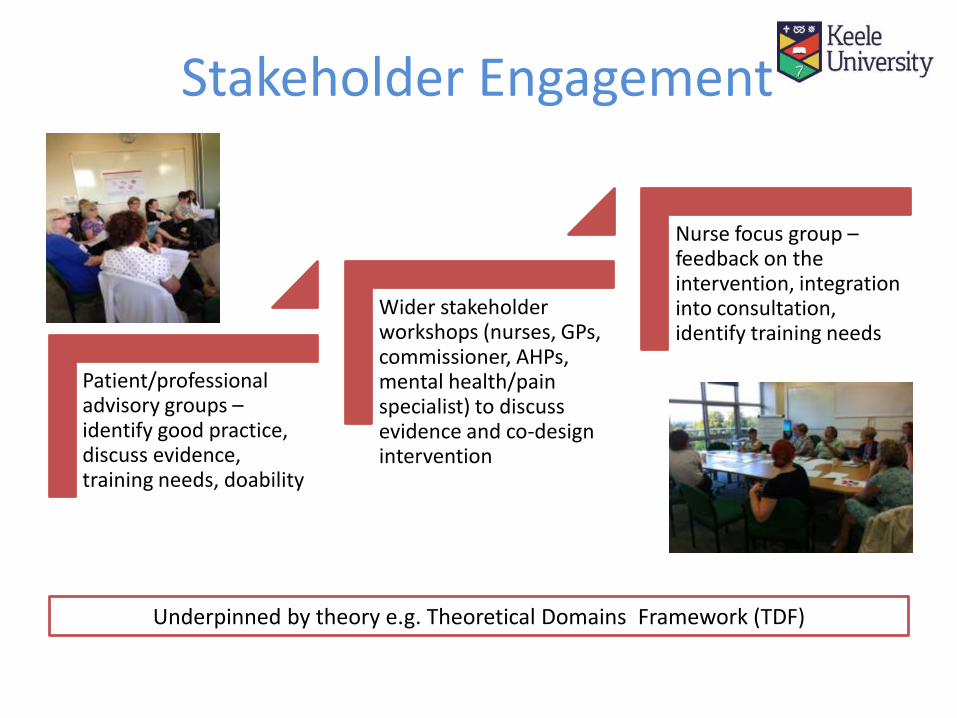
Stakeholder Engagement
Patient/professional advisory groups –identify good practice, discuss evidence, training needs, doability
Wider stakeholder workshops (nurses, GPs, commissioner, AHPs, mental health/pain specialist) to discuss evidence and co-design intervention
Nurse focus group –feedback on the intervention, integration into consultation, identify training needs
Underpinned by theory e.g. Theoretical Domains Framework (TDF)
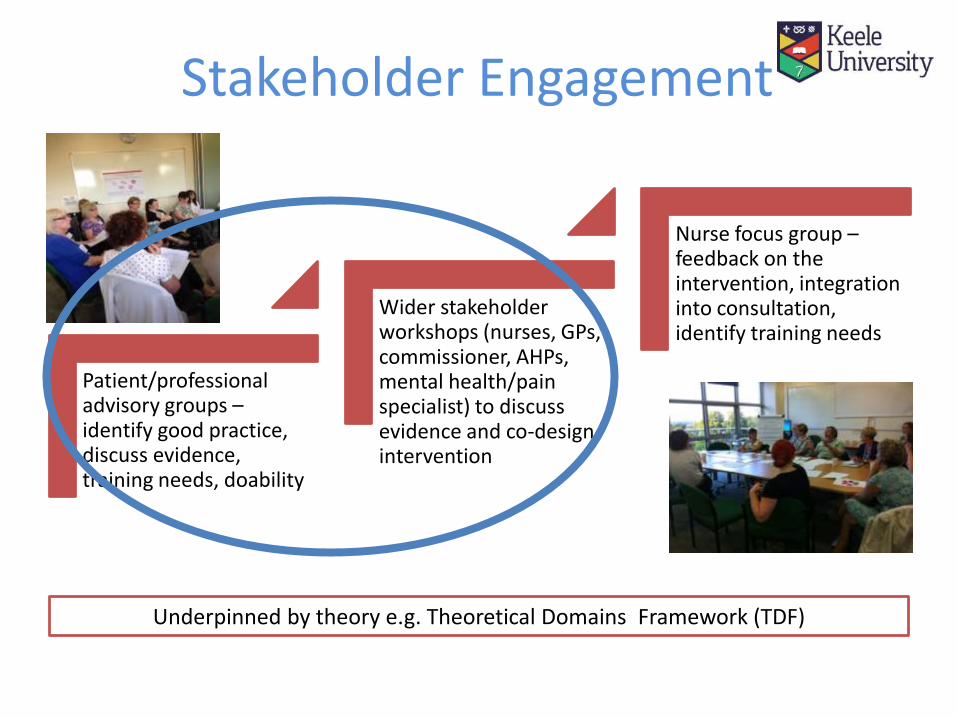
Stakeholder Engagement
Patient/professional advisory groups –identify good practice, discuss evidence, training needs, doability
Wider stakeholder workshops (nurses, GPs, commissioner, AHPs, mental health/pain specialist) to discuss evidence and co-design intervention
Nurse focus group –feedback on the intervention, integration into consultation, identify training needs
Underpinned by theory e.g. Theoretical Domains Framework (TDF)

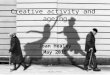
The ENHANCE Review
Nurse led LTC
Review
Initial Management
e.g. Written information, advice, referrals
Case finding
Joint Pain
Anxiety / Depression
Extra 20 minutes funded
The ENHANCE
EMIS Template
Stakeholder Engagement
Patient/professional advisory groups –identify good practice, discuss evidence, training needs, doability
Wider stakeholder workshops (nurses, GPs, commissioner, AHPs, mental health/pain specialist) to discuss evidence and co-design intervention
Nurse focus group –feedback on the intervention, integration into consultation, identify training needs
Underpinned by theory e.g. Theoretical Domains Framework (TDF)

Training development
TDF Domains identified from Focus Group Strategies to address barriers
Training outline• Practice training
Training sessions (plus mentoring)
– Initial 1hr update session in practice • GPs, Practice nurse(s), Practice Manager
• Focus on OA, anxiety and depression
– 2 half day sessions in practice• Delivery of the ENHANCE review and use of the ENHANCE template
• Developed and delivered by study training team
• Dr Andrew Finney, Dr Val Tan, Dr Mark Porcheret, Prof Carolyn Chew-Graham, Dr Vince Cooper, Simon Wathall, Julie Shufflebotham
• Local IAPT and physiotherapy service training
Pilot trial overview
• 4 General Practices
• Patients attending chronic disease reviews with the practice nurse
−asthma
−COPD
−cardiovascular diseases
−diabetes
• Recruit 300 patients over 6 months
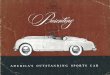
• Stepped wedge design

• Stepped wedge design with 4 steps
July 2015Week
Jan 2016
1 - 6 7-11 12-16 17-21 22-27
Practice Step 1 Step 2 Step 3 Step 4
1
2
3
4
control periodintervention periodin-house training
Study Design

Data collection
• Mixed methods approach
• Self-reported patient questionnaires
⁻ Phase 1 (post consultation), Phase 2 (6 weeks) and Phase 3 (6 months)
• Medical record review (MRR)
• Qualitative interviews and audio-recording of the ENHANCE review
Success criteria• Engage GP practices to participate and stay in the trial through
follow-up (4 practices)
• Deliver the training to at least two practice nurses per practice
• Recruit (at least 50% of those invited) and retain (75% of those that consent) sufficient patients to the research evaluation
• Satisfaction of patients who received the ‘ENHANCE’ LTC review should be at least as acceptable as that of those who received usual care (by comparing mean scores on the GPAQ)
• Recruitment and follow-up rates should be similar in both arms of the study (a difference in recruitment or follow-up rate of up to 10% to represent an acceptable level of deviation)
Progress to date• Nurse training programme developed and delivered
• Training delivered to local IAPT and physiotherapy services
• Recruitment complete
• 6 month follow-up data collection ongoing
• Interviews complete:
– 8 nurses and 1 GP
– 20 patients
• 24 consultation recordings

Recruitment and Follow up
• 319 recruited, 207 are control and 112 are intervention
• Baseline packs returned 67%; Consent to follow up 88%
• 6 week follow up 93%; 36 (5%) MDCs sent out
• 6 month follow up 88%; 31 MDCs (6%) sent out
Next Steps
• Complete data collection
– Patient questionnaires: Phase 3 (6 months)
– Medical record review (MRR)
• Data analysis
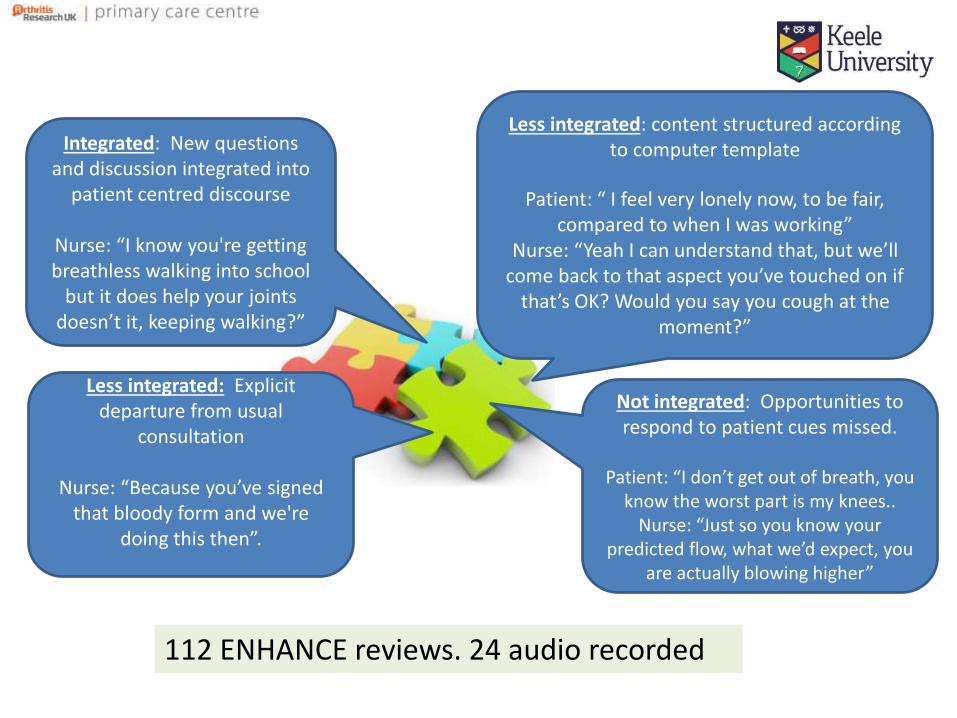
Less integrated: Explicit departure from usual
consultation
Nurse: “Because you’ve signed that bloody form and we're
doing this then”.
112 ENHANCE reviews. 24 audio recorded
Integrated: New questions and discussion integrated into
patient centred discourse
Nurse: “I know you're getting breathless walking into school
but it does help your joints doesn’t it, keeping walking?”
Not integrated: Opportunities to respond to patient cues missed.
Patient: “I don’t get out of breath, you know the worst part is my knees..
Nurse: “Just so you know your predicted flow, what we’d expect, you
are actually blowing higher”
Less integrated: content structured according to computer template
Patient: “ I feel very lonely now, to be fair, compared to when I was working”
Nurse: “Yeah I can understand that, but we’ll come back to that aspect you’ve touched on if
that’s OK? Would you say you cough at the moment?”
Main trial design
• Stepped wedge vs cluster
• Pragmatic vs efficacy
• Value of disease/condition focus
• Intervention components for LTC care
• Participant recruitment: selection bias
• Primary outcome measure
Funder• NIHR Health Services and Delivery Research
(HS&DR) – aim spring 2017
• Feedback
– Within scope, relevant and links to previous call
– Demonstrate “immediate practice utility”
– Focus on generalizability
– Link to and build upon HS&DR portfolio
– Detail development work and pilot trial
– Knowledge transfer and mobilisation is a priority
– Include cost effectiveness
– Include service and workforce outcomes
AcknowledgementsNorth Staffordshire Clinical Partners:
North Staffs / Stoke / South Staffs / Shropshire CCGStaffordshire and Stoke-on-Trent Partnership Trust
ENHANCE Patient and Nurse Advisory GroupsKeele Research Users’ Group
Keele CLAHRC Team: Professor Christian Mallen, Dr Clare Jinks, Dr Emma Healey, Professor
Carolyn Chew-Graham, Dr Mark Porcheret, Dr Val Tan, Dr Vince Cooper, Sarah Lawton, Simon Wathall, Dr Andrew Finney, Elaine
Nicholls, Dr Irena Zwierska, Professor Krysia Dziedzic, Dr Jenny Liddle, Dr Martyn Lewis, Julie Shufflebotham, Jo Jordan, Professor Elaine Hay
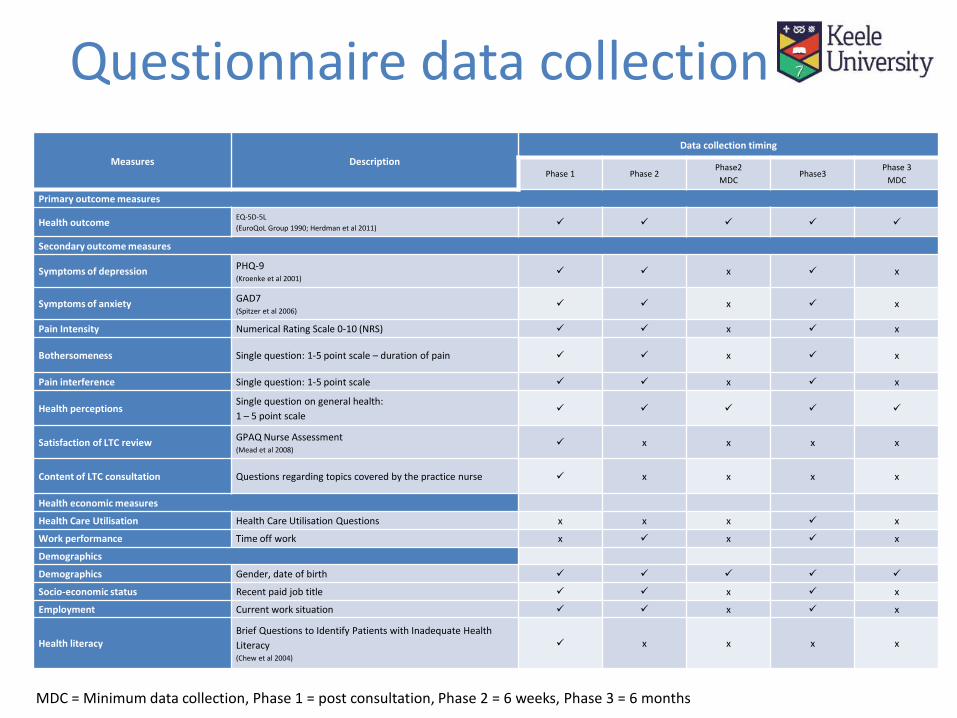
Questionnaire data collection
Measures Description
Data collection timing
Phase 1 Phase 2Phase2
MDCPhase3
Phase 3
MDC
Primary outcome measures
Health outcomeEQ-5D-5L
(EuroQoL Group 1990; Herdman et al 2011)
Secondary outcome measures
Symptoms of depressionPHQ-9(Kroenke et al 2001)
x x
Symptoms of anxietyGAD7(Spitzer et al 2006)
x x
Pain Intensity Numerical Rating Scale 0-10 (NRS) x x
Bothersomeness Single question: 1-5 point scale – duration of pain x x
Pain interference Single question: 1-5 point scale x x
Health perceptions Single question on general health:
1 – 5 point scale
Satisfaction of LTC reviewGPAQ Nurse Assessment(Mead et al 2008)
x x x x
Content of LTC consultation Questions regarding topics covered by the practice nurse x x x x
Health economic measures
Health Care Utilisation Health Care Utilisation Questions x x x x
Work performance Time off work x x x
Demographics
Demographics Gender, date of birth
Socio-economic status Recent paid job title x x
Employment Current work situation x x
Health literacy Brief Questions to Identify Patients with Inadequate Health
Literacy(Chew et al 2004)
x x x x
MDC = Minimum data collection, Phase 1 = post consultation, Phase 2 = 6 weeks, Phase 3 = 6 months