Embed Size (px)
Citation preview


COMA AND ALTERED CONSCIOUSNESS

Reference
(PACT (Patient-centred Acute Care Training(, a product of the European Society of Intensive Care Medicine (ESICM(
http://pact.esicm.org/main/newscorm
Authors (Update 2012)
Tarek SharsharDepartment of Intensive Care Medicine, Raymond Poincaré Hospital, Garches, France
Nicolas WeissNeurological Intensive Care, Pitié-Salpêtrière Hospital, Paris, France
Copyright© 2012.European Society of Intensive Care Medicine.

LEARNING OBJECTIVES:
1.In hospital emergency, the clinical analysis of unresponsive and comatose patient is always an urgency.
2.Physician must therefore be prepared to implement a rapid, systematic investigation and need for prompt therapeutic action.
3.Recognise coma and altered consciousness using a brief neurological examination.
4.Manage specific conditions causing altered consciousness.
4.Develop a comprehensive care plan for patients with altered consciousness and prolonged ICU stay.

Introduction
1/ How to recognise and assess the patient with altered consciousness
2/ Early management of the patient with altered consciousness
3/ Altered consciousness - some specific causative conditions
4/ Predicting outcome and managing prolonged altered consciousness in ICU

Introduction*Altered states of consciousness may be the cause or the
result of acute or critical illness and are a common reason for admission to the emergency department (ED( and the intensive care unit (ICU(.
*Neurological examination may be difficult to perform in patients with altered consciousness or who are poorly cooperative and routine tests, commonly used in awake patients, may not be easy to apply. These factors may limit the clinical decision-making process and diagnosis.

*Moreover, repeated neurological evaluation is necessary in patients with altered consciousness to detect complications of both extra-neurological and
systemic diseases occurring in the ICU .
*A structured, logical, and effective approach to manage patients with altered consciousness is required to diagnose, treat and prevent secondary damage to the brain or other organ systems. To be successful this approach requires
simultaneous evaluation and treatment.

•ConsciousnessIs defined as Awareness of self and environment, combined with the ability to respond to environmental factors.
So, The conscious state can be considered as two closely interrelated components:
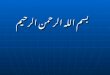
1.Arousal (wakefulness, alertness, or vigilance( is clinically defined as the ability to open the eyes and the presence
of sleep/wake cycles. Arousal is regulated and depends on the intact function of the Ascending Reticular Activating System (ARAS), a large sub-cortical area of the brain located in the brain-stem, the diencephalon (hypothalamus and thalami), the basal forebrain and the projections to the cerebral cortex
Cerebral Cortex
Reticular Activating
SystemBrain Stem

2.Awareness (awareness of self and environment, i.e. the content of consciousness(:
is clinically defined as the ability to obey commands. It is regulated by, and depends on the intact function of cerebral cortex and its sub-cortical (mainly thalamic(
connections.

Grady Coma Scale
Grade State of awareness Responds appropriately to:
Calling
name Light pain Deep pain
I Confused, drowsy, lethargic, un co-operative. Yes Yes Yes
Does not lapse in to sleep when left undisturbed
II Stuporous, un co-operative, disoriented to time, No Yes Yes
place, person, lapse in to sleep if not disturbed.
III Deep Stupor, Requires strong pain to evoke No No Yes
movement.
IV Exhibits decorticate or decerebrate posturing No No No
to deep pain stimulation.
V Does not respond to any stimuli. No No No
From: Chapter 57, Level of Consciousness
http://www.ncbi.nlm.nih.gov/books/NBK380/table/A1733

Coma is clinically defined by a state of unresponsiveness in which the patient does not open their eyes, does not follow commands, cannot be aroused, and has no awareness of self or environment.
•DeliriumA fluctuating change in consciousness and awareness, mainly characterized by an alteration of attention and organization of thinking associated with abnormal sleep–wake cycle, psychomotor activity, perceptions (e.g.,
hallucinations, illusions) and emotional behavior.

The vegetative state (VS(:
is characterized by arousal without signs of
awareness, a wakeful unconscious state.
A minimally conscious state, unlike a vegetative state, is characterized by some evidence of awareness of self and/or the environment, and patients tend to improve.

A vegetative state is absence of responsiveness and awareness Asthe cortex is severely damaged (eliminating cognitive function), but the reticular activating system (RAS) remains functional (making wakefulness possible). Midbrain or pontine reflexes may or may not be present.Patients may have complex reflexes, including eye movements, yawning, and involuntary movements to noxious stimuli, but show no awareness of self or environment.
It is a chronic condition that preserves the ability to maintain BP, respiration, and cardiac function, but not cognitive function. Hypothalamic and medullary brain stem functions remain intact to support cardiorespiratory and autonomic functions and are sufficient for survival if medical and nursing care is adequate
http://www.merckmanuals.com/professional/neurologic-disorders/coma-and-impaired-consciousness/vegetative-state-and-minimally-conscious-state

Causes of vegetative state:The most common causes are traumatic brain injury and diffuse cerebral hypoxia. However, any disorder that results in brain damage can cause a vegetative state.

Permanent
VS means irreversible and is defined by the Multi-Society Task Force for Persistent VS, as VS present at three months after a non-traumatic or at 12 months after a traumatic brain injury.
As stated by the Multi-Society Task Force for Persistent VS, this condition may be
Transient:
marking a stage in the recovery from severe acute or chronic brain damage.(<1month(
Persistent VS is arbitrarily defined as VS present one month after initial brain injury, but it does not mean that it is irreversible.

Supportive care
Supportive care is the mainstay of treatment and should include the following:
Preventing systemic complications due to immobilization (eg, pneumonia, UTI, thromboembolic disease(
Providing good nutrition
Preventing pressure ulcers
Providing physical therapy to prevent limb contractures
Vegetative state has no specific treatment.
TREATMENT

Coma is clinically defined by a state of unresponsiveness in which the patient does not open their eyes, does not follow commands, cannot be aroused, and has no awareness of self or environment.
•DeliriumA fluctuating change in consciousness and awareness, mainly characterized by an alteration of attention and organization of thinking associated with abnormal sleep–wake cycle, psychomotor activity, perceptions
(e.g., hallucinations, illusions) and emotional behavior.

Causes of COMA
•
Structural Non- Structural(Focal( (Diffuse or
metabolic(




Q. Do all patients with altered consciousness need ICU treatment?
A.No but regardless of the nature of the cause of altered consciousness, patients with altered consciousness need close and constant surveillance to detect a further deterioration in the level of consciousness. Prediction of the clinical course is inexact and close surveillance can normally only be guaranteed in a critical care environment.
Q.What are the criteria for ICU admission in patients with altered consciousness?
A.Admission to the ICU depends also on the severity of the disturbance of the consciousness e.g. a GCS of 8 or less normally warrants tracheal intubation but, even when coma is less severe, a deteriorating state of consciousness provides additional evidence for critical care admission.

1 /How to recognise and assess the patient
with altered consciousness?

The comatose state is a life-threatening condition, therefore application of the ABC (Airway, Breathing, Circulation( algorithm and immediate treatment is essential before further assessment.
Performing a brief neurological examination before sedation administration for intubation or any other reason (e.g. agitation) is important.
Neurological assessment of comatose patients
Neurological examination of comatose patients is preceded by a general examination to reveal evidence of head trauma, meningeal irritation, purpura, elevated intracranial pressure or other diagnostic findings.
Recognising a comatose patient

TechniqueThe technique of evaluation of the patient with an
altered level of consciousness can be divided into three phases:
The first is to determine the level of consciousness itself. Second is evaluation of the patient, searching carefully for hints as to the cause of the confusion or coma.
Third is the presence or absence of focality of the disorder, both in terms of the level of dysfunction within the rostrocaudal neuraxis and specific involvement of cortical or brainstem structures.

Neurological examination should at least include examination of (1( the best motor responses to noxious stimuli, (2( brain-stem reflexes, (3( respiratory pattern and (4( reflexes.
(1( Best motor responses:The recommended noxious stimuli are pressure to:•the supraorbital ridge,• the nail beds of the fingers and the toes, •the sternum and the temporomandibular joints.

Motor responses:
-Spontaneous,
-purposeful or
non-purposeful movements,
- withdrawal or posturing reflexes ,
-including any evidence of lateralization of signs, to noxious stimuli .
-Eye opening, if not present to voice or spontaneously, in response to the noxious stimulus is also noted.

(2 (Brain-stem reflexes:Testing of brain-stem reflexes should at least include
1.pupillary responses 2. ocular motility.
3.Corneal reflex 4 .cough reflex.
Ocular motility can easily be tested by holding the eyelids open to observe eye position and movements. Most comatose patients have only a slight exophoria, so the position of both eyes should be conjugate. Disconjugate eye positions suggest the presence of a brain-stem lesion.
OCULO-CEPHALIC REFLEXAlso called Doll`s-eye movement.Elicited by briskly turning or tilting the head.
Response in coma of metabolic origin or that due to bihemispheral structural lesions consist of conjugate movements of eyes in the opposite direction.
Positive response indicates- loss of cortical inhibition on brainstem that normally holds these movements in checkAbsent reflex indicates damage within brainstem but also can be due to
profound overdose of sedatives or anticonvulsants .

29

Vestibulo-ocular responses tested by lateral head movement (‘doll’s eyes manoeuvre’) may be used to elicit eye movements if they are not present spontaneously, but should be avoided if a fracture or dislocation of the cervical spine is possible. In these cases, cold caloric testing is preferred,
provided that the tympanic membrane is intact and not obscured .
3.Corneal reflex testing is rapid and may have a considerable prognostic value.
4.cough reflex
Tracheal suctioning in mechanically ventilated patients allows testing of the

• (3( Respiratory patternThe pattern of respiration helps to determine both the level of brain damage and the cause of coma (Cheyne–Stokes, bradypnoea, apneustic breathing, ataxic breathing(. However, the need for stabilising vital functions and the urgent need for mechanical ventilation may decrease their value. For more informationTHINK: The evaluation of the respiratory pattern may provide clues to the cause of the coma and of the localisation of the brain pathology. However, this is not highly specific. Kussmaul breathing, deep and rapid regular breathing
suggest a metabolic origin of coma, such as diabetic ketoacidosis .
• (4( ReflexesExamination of deep tendon reflexes and plantar responses can be informative particularly when lateralization of pathology is suggested.
.

Standardised assessment and follow-up
Neurological assessment of comatose patients should be reproducible and
standardized so that the evolution of neurological abnormalities can be followed.
The bedside detailed neurological examination of coma should be assessed using
validated scales.

Glasgow Coma Scale
Graham and Bryan, Neurosurgery professors developed this scale in 1974 at the University of Glasgow.
15 point scale - Initially used to assess the level of consciousness.
GCS is used to test best motor response (6(, best verbal response (5( and best eye response (4(.
Score ranges from 3 (deep coma or death( to 15 (fully awake(.


Motor Response (total score = 6(
Score 6 – Obeys commands:
Highest level of motor response
Accurate response to instruction (twice(
eg: raise eyebrows, stick out tongue.

SCORE 5 - LOCALISING PAIN :
RESPONSE TO PAIN STIMULUS – MOVEMENT OF LIMB AS TO
ATTEMPT TO REMOVE THE STIMULUS.
1 .STERNAL RUB
2.SUPRA ORBITAL PRESSURE
3 .TRAPEZIUS SQUEEZE
4 .NAIL BED PRESSURE

Score 4 - Withdrawal from Pain :
o Normal flexion in response to central pain stimuli, but failing to locate source of pain.
o Pulls limb away from painful stimulus.

Score 3 - Flexion to Pain:o Decorticate posturing: due to a block in motor
pathway between cerebral cortex and brain stemo Slower responseo Flexing upper arm & rotating of wrist & thumb
through fingers and extension of lower limb

Score 2 - Extension to Paino Decerebrate posturing: occurs due to
blockage/damage within brainstem.o Straightening of elbow & internal rotation of
shoulder and wrist; leg extension
Score 1- No Motor Response:-Brain incapable of processing any sensory input & motor
activity
- Rigid to all pain stimuli

Verbal Response (total score = 5(
Score 5 – OrientedAwareness of the self and the environment.
(Who, Where, When, Why(
Score 4 – Disoriented
Responses to questions with presence of confusion and disorientation.

Score 3 – Inappropriate words
Speech in a random way.
No conversational exchange
Score 2- Incomprehensible sounds
Moaning and Groaning
Score 1- No verbal response
No response to any deep or vigorous stimuli

Eye Response (total score = 4
Score 4 – Spontaneous
Indicates activity of brainstem arousal mechanisms, but not necessary patient is attentive.
Score 3 – To Speech
Tested by any verbal approach (spoken or shouted) ,
Not necessary the command to open the eyes.

Score 2 – To pain
Tested by a stimulus in the limbs.
) supra- ortibal pressure may cause grimacing(
Score 1 – No Eye response
No response to speech or pain

Q.The Glasgow Coma Scale is a standard means of evaluating patients with altered consciousness. What physiological
conditions must be fulfilled for the GCS to be reliable?
A.The result of GCS testing is only reliable when the patient is stable i.e. in the absence of hypotension and/or hypoxaemia.
Q.Drugs used in the acute/critical care circumstances influence the GCS. Outline two categories of such drugs and their effects on the GCS
A.
1.Sedatives, and even intense analgesia (with opiate drugs), may decrease the GCS.
2.Neuromuscular blocking agents (in ventilated patients) are particularly
relevant as they invalidate the GCS completely.

•The Glasgow Coma Scale (GCS( remains the most widely used coma assessment scale but :
•First, GCS may not always be reliable in mechanically ventilated patients, particularly with regard to the verbal component.
•Second, GCS lacks assessment of an important component of coma assessment in ICU patients, i.e. testing of brain-stem reflexes.

The Full Outline of UnResponsiveness score (FOUR) is a relatively new coma assessment scale that includes brain-stem reflexes. Four components of brain function (eye response, motor response, brain-stem reflexes, and respiration pattern) are tested and it has been validated in mechanically ventilated ICU patients.
Other scales, e.g. the Glasgow–Liège Scale, the Reaction Level Scale-85 or the Innsbruck Coma Scale, that include brain-stem reflexes testing have been proposed but have never gained wide acceptance.


2 /Early management of the patient with altered consciousness
Early management of the comatose patient
All alterations in arousal are acute life-threatening emergencies. Therefore apply the ABC algorithm and perform immediate treatment as needed.


AirwayEvaluate the airway and protect the cervical spine, if there is a possibility of cervical spine injury. Check for signs of upper airway obstruction and open airway; administer oxygen immediately. Check the oxygen saturation by pulse oximetry. If ventilation remains inadequate despite clearing the upper airway by suctioning, perform mask ventilation and proceed to tracheal intubation.
Always remember that the cervical spine could be injured due to accident or fall during loss of consciousness.
Hypoxia is the number one killer, and hypoxia with hypotension is the main cause of secondary brain injury.

Q.Why do patients with a Glasgow Coma Scale score equal to or less than 8 points need
intubation?
A.A Glasgow Coma Scale score equal to or less than 8 indicates deep coma with probable loss of protective reflexes such as swallowing, coughing, and the ability to
maintain a clear airway.A. Also,Because of the risk of hypoventilation, which may
elevate PaCO2 and so may exacerbate intracranial hypertension.

Breathing
Use inspection, palpation, percussion and auscultation to rule out or confirm any pathology that may interfere with oxygenation and/or ventilation, such as pneumothorax, haemothorax or flail chest. If there is any relevant pathology it should be treated before proceeding to an assessment of the circulation.
Circulation
Hypotension is a major cause of secondary brain injury. While awaiting final diagnosis of the cause of coma, mean arterial pressure should be maintained at least >70 mmHg in an attempt to ensure an adequate cerebral perfusion pressure.
Isotonic saline is a suitable solution to restore circulating volume. A systolic arterial pressure equal to or higher than 100 mmHg is adequate and safe for most patients.
When obtaining venous access, blood samples should be collected for laboratory tests

Severe hypotension itself can cause loss of consciousness, even in the absence of primary cerebral
pathology.
Volume resuscitation
All comatose patients should receive isotonic solutions for resuscitation, preferably 0.95% saline. An exception to this rule is the bolus administration of glucose to hypoglycaemic patients.

Simultaneous evaluation and treatment
Patient historyAfter the life-saving ABC, collect further information from the
paramedics, police, bystanders, relatives, or friends. Relevant information is important and can help you narrow your differential diagnosis and rationally order your diagnostic steps. The history should include the following:
Was a witness present?
The onset of comatose state? (sudden or rapidly progressive onset)
Accompanying complaints? (headache, thunderclap headache, vomiting, fever, seizures)
General medical history (including psychiatric history)
Recent medical history (surgical procedures, infections, current medication)
Presence of empty medicine bottles or access to drugs (illicit drugs, sedatives, narcotics, psychotropic drugs).

Hypoglycaemia
Hypoglycemic coma is common and the benefits of immediate administration of glucose outweigh the theoretical risks of additional harm to the brain if hyperglycaemic, hyperosmolar or anoxic coma is the underlying pathology.If there is no immediately available blood glucose testing (fingerstick glucose or quick stat lab blood glucose( a 25G bolus of glucose (50 mL glucose 50% i.v. push( should be given without waiting for confirmation of hypoglycaemia.
SeizuresRepeated generalised seizures damage the brain and must be terminated as soon as possible. Initial treatment is with intravenous benzodiazepines; lorazepam is currently considered to be the agent of choice.
3 /Altered consciousness – some specific causative conditions

Drug overdose is the most common cause of coma presenting to Accident andEmergency Departments, being responsible for 30% of cases. If you have any suspicion of opioid or benzodiazepine overdose, you should assess and treat before proceeding to other investigations, unless the patient has traumatic brain injury or any other obvious explanation for coma.
Diagnostic strategy

Laboratory studies

Laboratory studies

Communication:

4/ Predicting outcome and managing prolonged altered consciousness in ICU
Predicting the likely clinical course, including brain death
Several situations associated with altered consciousness or unconsciousness can culminate in brain death. A confident diagnosis of death depends on defining the point at which these processes become irreversible.
Situations causing brain death

Brain death
Brain death is loss of function of the entire cerebrum and brain stem, resulting in coma, no spontaneous respiration, and loss of all brain stem reflexes. Spinal reflexes, including deep tendon, plantar flexion, and withdrawal reflexes, may remain. Recovery does not occur.
The concept of brain death developed because ventilators and drugs can perpetuate cardiopulmonary and other body functions despite complete cessation of all cerebral activity. The concept that brain death (ie, total cessation of integrated brain function, especially that of the brain stem) constitutes a person’s death has been accepted legally and culturally in most of the world.

Serial determination of clinical criteria
Apnea testing
Sometimes EEG, brain vascular imaging, or both
For a physician to declare brain death, a known structural or metabolic cause of brain damage must be present, and use of potentially anesthetizing or paralyzing drugs, especially self-administered, must be ruled out. if status epilepticus is suspected, EEG should be done. Sequential testing over 6 to 24 h is typically done
Guidelines for Determining Brain Death (in Patients > 1 Yr)
Diagnosis
The commonest causes of brain-stem death are traumatic brain injuries,
subarachnoid haemorrhage, intracerebral haematoma,
global cerebral hypoxia, and brain ischaemia.

An apnea test of a minimum of 8 min shows no respiratory movements with a documented increase in Pa co 2 of > 20 mm Hg from pretest baseline.
PROCEDURE: Apnea testing is done by disconnecting the ventilator from the endotracheal tube. O 2 (6 L/min) can be supplied by diffusion from a cannula placed through the endotracheal tube. Despite the ventilatory stimulus of the passively rising Pa co 2 , no spontaneous respirations are seen over an 8- to 12-min period.
N ote : The apnea test should be done with extreme caution to minimize risks of hypoxia and hypotension, particularly in potential organ donors. If arterial BP falls significantly during the test, the test should be stopped, and an arterial blood sample drawn to determine whether Pa co 2 has risen either to > 55 mm Hg or has increased by > 20 mm Hg. This finding validates the clinical diagnosis of brain death.

All 9 items must be confirmed to declare brain death:
1. Reasonable efforts were made to notify the patient’s next of kin or another person close to the patient.
2. Cause of coma is known and sufficient to account for irreversible loss of all brain function.
3. CNS depressant drugs, hypothermia (< 35° C(, and hypotension (MAP < 55 mm Hg( have been excluded. No neuromuscular blockers contribute to the neurologic findings.
4. Any observed movements can be attributed entirely to spinal cord function.
5. The cough reflex, pharyngeal reflexes, or both are tested and shown to be absent.
6. Corneal and pupillary light responses are absent.
7. No caloric responses follow ice water siphoned against the tympanic membrane.
8. An apnea test of a minimum of 8 min shows no respiratory movements with a documented increase in Pa co 2 of > 20 mm Hg from pretest baseline.
PROCEDURE: Apnea testing is done by disconnecting the ventilator from the endotracheal tube. O 2
(6 L/min( can be supplied by diffusion from a cannula placed through the endotracheal tube. Despite the ventilatory stimulus of the passively rising Pa co 2 , no spontaneous respirations are seen over an
8- to 12-min period.
N ote : The apnea test should be done with extreme caution to minimize risks of hypoxia and hypotension, particularly in potential organ donors. If arterial BP falls significantly during the test, the test should be stopped, and an arterial blood sample drawn to determine whether Pa co 2 has risen
either to > 55 mm Hg or has increased by > 20 mm Hg. This finding validates the clinical diagnosis of brain death.
9. At least one of the following 4 criteria has been established:
a. Items 2–8 have been confirmed by 2 examinations separated by at least 6 h.
Guidelines for Determining Brain Death (in Patients > 1 Yr)

b. Items 2–8 have been confirmed AND
An EEG shows electrocortical silence.
A 2nd examination at least 2 h after the 1st confirms items 2–8.
c. Items 2–8 have been confirmed AND
Conventional angiography, transcranial Doppler ultrasonography, or technetium-99m hexamethylpropyleneamine oxime brain scanning shows no intracranial blood flow.
A 2nd examination at least 2 h after the first confirms items 2–8.
d. If any of items 2–8 cannot be determined because the injury or condition prohibits evaluation (eg, extensive facial injury precludes caloric testing(, the following criteria apply:
Items that are assessable are confirmed.
Conventional angiography, transcranial Doppler ultrasonography, or technetium-99m hexamethylpropyleneamine oxime brain scanning shows no intracranial blood flow.
A 2nd examination 6 h after the first confirms all assessable items.
MAP = mean arterial pressure.
Adapted from the American Academy of Neurology Guidelines (1995(.
Guidelines for Determining Brain Death (in Patients > 1 Yr)

Communication with the relatives of a brain-injured patient is clearly very important, and their desire for information about the outcome is understandable. Nevertheless, it is necessary to impress upon families that:
•The comatose patient may or may not awaken,
•Even if the patient awakens they may have major sequelae that may or may not improve
•And that the recovery process can take months or years and is filled with uncertainty.

The flow chart for altered consciousness