Embed Size (px)
Citation preview

Alteration of consciousness and coma
WATUHATAI PAIBOOL, MD
DIVISION OF NEUROLOGY, DEPARTMENT OF PEDIATRICS
KHON KAEN UNIVERSITY

Outline Definition of consciousness & component
Etiology of alternation of consciousness&coma
Clinical evaluation
Investigation
Management
Introduction
One of most common problem in general medicine
Substantial portion of admission to emergency ward
Various etiologies

DefinitionConsciousness is the state of full awareness of the self and one’s
relationship to the environment
Wakefulness Awareness

Component of consciousnessWAKEFULNESS LEVEL
Ascending sensory stimulation
- brainstem
- hypothalamus
- thalamus
- cerebral cortex
Alertness to stimuli
AWARENESS LEVEL
Difficult to localized
- cerebral cortex
- interaction of subcortical nuclei
Awareness of self and environment
Awearness requires wakefulness

Ascending arousal system
Arousal neurotransmitters
- cholinergic system: ACh
- monoamine: noradrenaline
- serotonin(5-HT)
- peptidergic: orexin
- GABA

Alteration of consciousness
Activated mental status
- Confusion
- Hallucination
- Illusions
- Delusions
- Delirium
Reduced mental status - Drowsiness
- Lethargy
- Obtundation
- Stupor
- Coma Along the recovery continumm after
coma- Vegetative state

Activated mental status
Confusion: impaired ability to think and reason, normal development & intellectual
Hallucination: perception of sensory input that are not present
Illusions: misinterpretation of actual sensory stimuli
Delusions: incorrect thoughts or beliefs, do not change by evidence or logical reason
Delirium: activated mental state that include disorientation, irritability, fear, sensory
misperception

Reduced mental status Clouding of consciousness: minimal reduction of wakefulness, difficulty in
maintenance of attention
Drowsiness: dull with sleepiness
Lethargy: difficult to maintain the arousal states
Obtundation: responsive to stimulation other than pain
Stupor: responsive only to pain
Coma: unresponsive to pain (a state of deep, unarousable sustained pathologic unconsciousness with the eyes closed that results from dysfunction of the ascending reticular activating system in the brain stem or in both cerebral hemispheres, persist at least 1 hour to unconsciousness)

EncehalopathyEncephalopathy: a diffuse disorder of the brain in which at least two of the following symptoms are present:
(1) altered states of consciousness
(2) altered cognition or personality
(3) seizures
Brain dysfunction

Encephalitis Encephalitis: an encephalopathy accompanied by inflammation and
usually cerebrospinal fluid pleocytosis.
- infection: mostly virus
- immune: - parainfection: ADEM
- paraneoplasm: Anti NMDAR encephalitis
- autoimmune: SLE, Hashimoto encephalitis

Brain death
Brain death is a clinical diagnosis based on the absence of neurologic function with a known diagnosis that has resulted in irreversiblecoma.
Coma and apnea must coexist to diagnose brain death.
Guidelines for the Determination of Brain Death in In Children; 1987

Etiology

Structural intracranial disordersTrauma: ICH, SAH, hematoma, diffuse axonal injury
Cerebrovascular event: brain infarction/hemorrhage
Infection: meningitis, encephalitis, abscess
Inflammatory process: demyelinating disease
Neoplasm
Hydrocephalus

Toxic or metabolic disordersHypoxic ischemic encephalopathy
Electrolyte or acid-base disorders
- pH disturbance
- hyper/hypoglycemia, Na, Ca
Intoxication
- Medication, drug abuse
- Alcohol
- Heavy metal: lead
- Poisoning
Seizure and postictal state
Organ dysfunction/systemic disorder
- Hepatic encephalopathy
- Uremic encephalopathy
- Hypertensive encephalopathy
- Endocrine disorders
- Inborn error of metabolism
- shock/cardiopulmonary failure
Psychologic conditions

Clinical evaluation Initial management
Identification of cause
History
General physical examination
Neurological examination

Initial management Assure a stable airway, adequate oxygenation, ventilation and circulation
Keep nomothermia and avoid hypoxemia, hypercapnia
Recognize and correct hypoglycemia
Consider specific antedotes for medical overdose
Monitor & treat increased intracranial pressure
Evaluate for seizure and stop
Treat suspected infection
Correct electrolyte and acid-base disturbance

HistoryThe events leading to the behavioral change
Drug or toxic exposure
A personal or family history of migraine or epilepsy
Recurrent or concurrent fever, infection disease or systemic illness
A previous personal or family history of encephalopathy

Clues from historySudden onset in normal child: convulsion or hemorrhage
Sleepiness in normal child: ingestion of drug or toxin
Fever: infection
Hx of fever: demyelinating disease-ADEM
Headache: increased ICP, migraine
Trauma: intracranial hemorrhage
DM: hypoglycemia, DKA
Congenital heart disease: infarction, abscess
Intermittent coma: drug, inborn error of metabolism
Salicylate with influenza or chickenpox: Reye syndrome
Behavioral change, sleep disturbance, movement disorder: Anti NMDAR encephalitis

General physical examinationVital signs
- Fever/hypothermia
- Hyper/hypotension
- RR, pattern of respiration
- PR, regular?, full?
General examination: systemic disease

Neurological examinationLevel of consciousness
Pupil, deviation of eyes
Papilledema, retinal hemorrhage
Meningeal signs
Breathing pattern
Cranial nerve examination
Motor response


Pupil size and reactions

Respiratory pattern
Cheyne-Stokes
Central neurogenic hyperventilation
Apneusis
Cluster breathing and ataxic breathing
Apnea

Cranial nerve examination Systematic assessment of brainstem function via reflexes
CN examination
- Papillary light reflex (CN II-III)
- Oculocephalic/calorics (CN III,IV,VI,VIII)
- Corneal reflex (CN V-VII)
- Gag reflex (CNIX-X)

Papillary light reflex (CN II-III)

Oculocephalic reflex (Doll’s eye reflex)
Proprioceptive head-turning lesion
C-spine injury must be excluded before exam
Normal alert person Absent
Coma with intact brainstem function
Conjugated eye movement in opposite direction of head-turning
Brainstem dysfunction Absent

Oculovesibular test (Caloric test)
Cold water with 30° head elevation
Normal person Nystagmus with fast phase away from tested side
Coma with intact brainstem function
Tonic deviation of both eyes toward tested side
Brainstem lesion No response


Motor response
Left hemiparesis
Decorticate posture
Decerebrate posture

Investigation
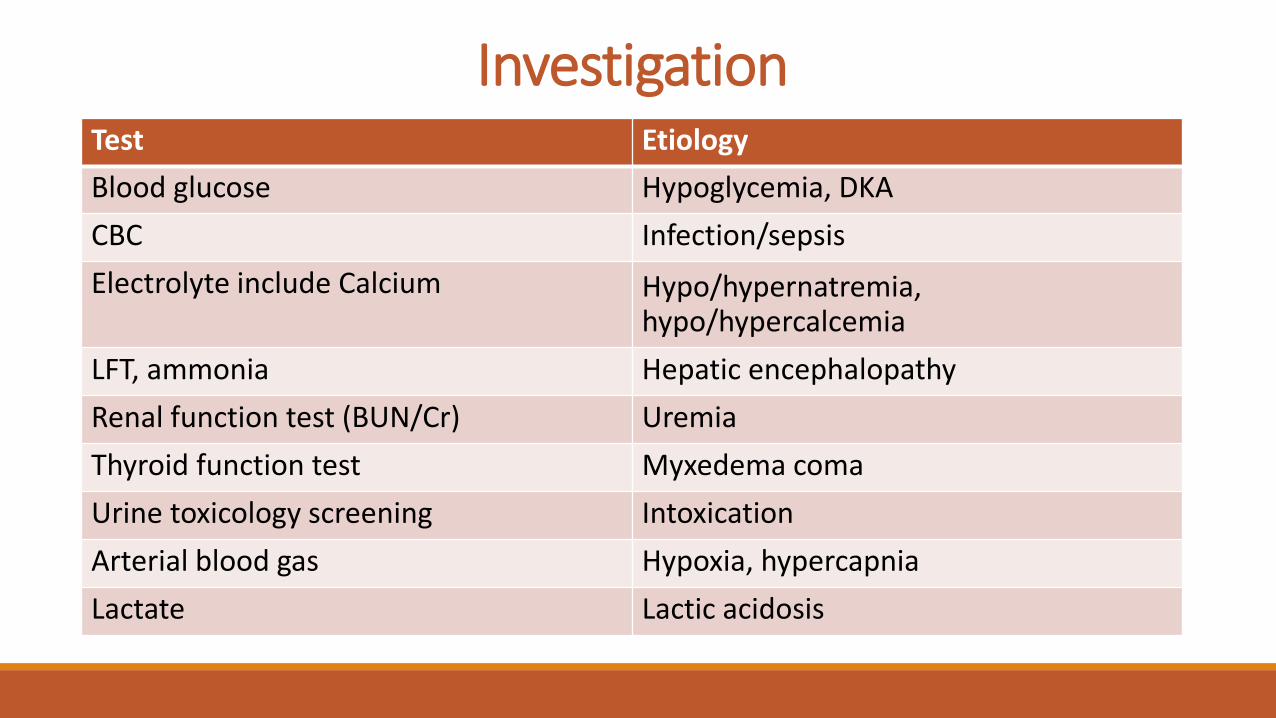
InvestigationTest Etiology
Blood glucose Hypoglycemia, DKA
CBC Infection/sepsis
Electrolyte include Calcium Hypo/hypernatremia, hypo/hypercalcemia
LFT, ammonia Hepatic encephalopathy
Renal function test (BUN/Cr) Uremia
Thyroid function test Myxedema coma
Urine toxicology screening Intoxication
Arterial blood gas Hypoxia, hypercapnia
Lactate Lactic acidosis

Investigation Lumbar puncture
if suspected CNS infection
Brain imaging (CT, MRI)
if positive focal neurological deficit, sign of increased ICP
; HSV, JE encephalitis, mass, intracranial hemorrhage
EEG
if suspected seizure (subclinical or NCSE), degree of encephalopathy

Management Initial management : ABC , maintain vital sign
Investigate and treat cause
Prevent & intervene anticipation of complication & sequelae
- Brain edema & increased ICP
- Infection: pneumonia, pressure ulcer, etc.
- Joint contracture
- Deep vein thrombosis

แหลงขอมลเพมเตม1. Berger JR. Stupor and Coma. In: Bradley WG, Daroff RB, Fenichel GM, Jankovic J, editors. Neurology in clinical practice. 6th ed. Philadelphia: Butterworth-Heinemann; 2012. p. 37-55.
2. Ropper AH. Coma. In: Longo DL, Fauci AS, Braunwald E, Kasper DL, Hauser SL, Jameson JL, Loscalzo J, editors. Harrison’s principles of internal medicine.18th ed. McGraw Hill: NY; 2011. p. 2247-53.
3. Posner JB, Saper CB, Schiff ND, Plum F. Plum and Posner’s diagnosis of stupor and coma, 4th ed. New York: Oxford University Press; 2007.
4. สมศกด ลพธกลธรรม. ภาวะโคมา. ใน: รงโรจน พทยศร, ธรธร พลเกษม,กนกรรณ บญญพสฏฐ, สมบต มงทวพงษา, บรรณาธการ. ต าราประสาทวทยาคลนก. กรงเทพฯ: สมาคมประสาทวทยาแหงประเทศไทย; 2556. หนา 112-31.
5. Rajajee V, Riggs B, Seder DB. Emergency neurological life support: Airway, Ventilation, and Sedation. Neurocrit Care
2017;27(Suppl 1):4-28.

Thank you

![Severe Malaria: North American Perspective...aggressively. The Glasgow coma scale in adults and Blantyre coma scale in children is useful for determining the level of impaired consciousness.[1]](https://img.pdfslide.us/doc/110x75/5e6c4948e97f9a3cc14d24a1/severe-malaria-north-american-perspective-aggressively-the-glasgow-coma-scale.jpg)

![Can the Assessment of Malaria Severity be Simplified for ......The status of consciousness was assessed using Blantyre coma scale [22] and the revised Glasgow coma scale (scores 3](https://img.pdfslide.us/doc/110x75/5e6c4945e97f9a3cc14d248d/can-the-assessment-of-malaria-severity-be-simplified-for-the-status-of-consciousness.jpg)
















![Can the Assessment of Malaria Severity be Simplified for ... · The status of consciousness was assessed using Blantyre coma scale [22] and the revised Glasgow coma scale (scores](https://img.pdfslide.us/doc/110x75/5aef9dfb7f8b9a572b8e61ec/can-the-assessment-of-malaria-severity-be-simplified-for-status-of-consciousness.jpg)








