Embed Size (px)
Citation preview

PRESENTED AT THE RADIOLOGICAL SOCIETY OF
AMERICA (RSNA) 2015 ANNUAL MEETING
CHICAGO IL
DECEMBER 3, 2015
Pediatric Fracture Detection Study:
A Task-Based Observer Study Evaluating Enhanced
Image Presentation and Potential Dose Reduction
p.1
© 2015, Carestream Health

Pediatric Fracture Detection Study:
A Task-Based Observer Study Evaluating
Enhanced Image Presentation and
Potential Dose Reduction
Lynn La Pietra1, Sosamma Methratta2, Samuel Richard1
1. Carestream Health, Inc., Rochester, NY, USA
2. The Milton S. Hershey Medical Center, Hershey, PA, USA
December 3, 2015

Outline
• Background
• Study Goal and Objectives
• Study Design
• Simulated Dose Reduction
• Reader Study Description
• Evaluation and Analysis
• Results and Summary
p.3
© 2015, Carestream Health

Background
• Pilot Study (ESPR 2012, Methratta et al)
• Image quality assessment of 5 reductions in dose using validated, simulated
noise models (Equivalent film speeds: 720, 900, 1440, 2280, 3600)
• Readers evaluated image interpretability using 4 point, RadLex Image Quality
Scale
• Pilot Study Results• Diagnostic quality images of pediatric patients may be captured with DR using
exposures as low as 900 speed
• Digital radiography coupled with multi-frequency image processing may offer the
opportunity to reduce default pediatric exposures
p.4
© 2015, Carestream Health

Background: European Society Pediatric
Radiology (ESPR 2012)
p.5
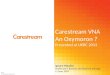
Today’s task-based study explores the previously
reported “Diagnostic” quality of this exposure range

New Study: Goal and Objectives
• Goal
• Reduce digital projection X-ray dose to the pediatric
population while maintaining diagnostic image quality.
• Study Objectives
Given the observer task of finding pediatric fractures:
1. Determine the impact of a simulated reduced dose
rendering on sensitivity.
2. Determine the impact of enhanced skeletal processing on
sensitivity (CARESTREAM ImageView SW, to be released
2016.)
p.6
Standard
Processing
Enhanced Skeletal
Processing
© 2015, Carestream Health

High Level Study Design
• Retrospectively collect de-identified pediatric images
• Generate ground truth from original captures (combination clinical
findings, repeat exam findings, repeat radiologist markings 2x separated by 6
months, for each image with fracture)
• Simulate reduced dose for each study image to an
equivalent 720 film-speed
• Generate:
• Standard of care image rendering for original study and simulated reduced
dose images
• Enhanced skeletal processing for original study and reduced images
• Reader Study: 5 Radiologists mark detected fractures in
each rendering, separated by 2+ weeks, mitigating learning
p.7
© 2015, Carestream Health

p.8
Dose Reduction Simulation Approach*+
AND REDUCE SIGNAL
Structured Noise – fixed pattern noise with
variance proportion to exposure squared
Quantum Noise – shot or Poisson noise with
variance proportional to the exposure
Electronic Noise – exposure-independent or
‘dark’ noise
Automatic Exposure Control or Phototimer
Anatomically Programmed Radiography
*Topfer et al, US 7,480,365 B1, Jan 20, 2009, Dose Reduced Digital Medical Image Simulations.
+Ellinwood et al, US 7,949,098 B2, May 24, 2011, Method for Determining Reduced Exposure Conditions
for Medical Images.

p.9
09 June 2011
Example Original Image, 200 SpeedSimulated Dose 30% of Original, 720 Speed

READER STUDY

p.11
Case Selection:100 cases free of fractures
50 cases with one or more fractures
• CsI or GoS DR
• Default processing for Carestream DR equipment
• 6 exam categories
• 5 age groups
• Chosen sequentially
• Each case consisted of 1, 2 or 3 projections
• 95 fractures in 50 cases
ORIGINAL
100 fx negative;
50 fx positive
< 3
mos
3 mos up
to 1 year
1 - 5
years
6 - 13
years
14 – 18
yearsTotals
Chest 8 12 8 2 1 31
Lower Extremity 8 14 9 4 5 40
Pelvis/Hip 2 2 4 2 2 12
Skull 4 9 5 1 0 19
Spine/Shoulder 3 5 2 2 4 16
Upper Extremity 1 5 7 11 8 32
Totals 26 47 35 22 20 150
© 2015, Carestream Health

Reader Demographics
p.12
Reader # Years
experience
Specialty %Time
Reading
Pediatrics
1 20 Pediatrics 100
2 7 Pediatrics 85
3 40 Pediatrics 100
4 6 Pediatrics 90
5 16 Pediatrics 100
© 2015, Carestream Health

Study Objective #1:
Determine the impact of a simulated
reduced dose rendering on fracture
sensitivity

Experiment Design (150 Cases: Original acquisitions +
150 Simulated Reduced Dose from Same Cases )
p.14
ORIGINAL
100 no fx;
50 with fx
< 3 mos3 mos up
to 1 year
1 -5
years
6 -13
years
14 – 18
years
Chest 8 12 8 2 1
Lower Extremity 8 14 9 4 5
Pelvis/Hip 2 2 4 2 2
Skull 4 9 5 1 0
Spine/Shoulder 3 5 2 2 4
Upper Extremity 1 5 7 11 8
720 Speed
(Same 150 cases)< 3 mos
3 mos up
to 1 year
1 -5
years
6 -13
years
14 – 18
years
Chest 8 12 8 2 1
Lower Extremity 8 14 9 4 5
Pelvis/Hip 2 2 4 2 2
Spine/Shoulder 4 9 5 1 0
Skull 3 5 2 2 4
Upper Extremity 1 5 7 11 8
+
Exam
Data Pool
300 cases
Reader Study – SW
generates a unique list
for each participant with
the same criteria• Every reader sees every case
• Original and Reduced
exposures must be read in
different sessions
Session 1
Session 2
© 2015, Carestream Health

Study Objective #2:
Determine the impact of enhanced
skeletal view on sensitivity

Experiment Design Software Control
Add Companion View: Enhanced Skeletal Rendering
p.16
Standard
Processed Case
may include 1, 2,
or 3 projections
Enhanced
Case may
include 1, 2, or
3 projections
Presented with
Standard
Processing of
Case Y.
Reader indicates
fx or advances to
next view.
Once Reader
advances to
Enhanced view,
detections on
Standard view
are frozen.
Presented with
Enhanced View
of Case Y.
Reader indicates
fx or advances to
next view. Reader
can toggle to
Standard View
and use as a
reference only.
Once Reader
advances to next
case, detections
on previous case
are frozen.
Start Session 1
Reader XNext Case
© 2015, Carestream Health

Evaluation Procedure
• Images displayed on diagnostic quality monitor
• 3MP, grayscale, GSDF calibrated, reduced ambient lighting
• Presentation sequence randomized among readers
• “Reason for image” displayed on control monitor
• Reader performs fracture detection task – in software, draw
rectangle around detected fx(s). Specify if same fx in
multiple projections
• GT compared with detection – Reader centroid must fall
within GT boundaries to count as true positive
• Calculate Sensitivity and Specificity per reader and
aggregate reader
p.17
© 2015, Carestream Health

Analysis
• Sensitivity = probability of a positive test among patients
with skeletal fracture =
• Specificity = probability of a negative test among patients
without skeletal fracture =
p.18
Fracture exists No Fracture in
Case
Test Positive a (TP) b (FP)
Test Negative c (FN) d (TN)
ca
a
db
d
© 2015, Carestream Health

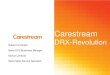
Example Femur Exam: Reduced Exposure Standard
(RES) Processing Paired with Enhanced Processing
(REE)Reduced Exposure Standard Processing
Lateral Projection PA Projection
Reduced Exposure Enhanced Processing
Lateral Projection PA Projection

Example Femur Exam: Reduced Exposure Standard
(RES) Processing Paired with Enhanced Processing
(REE)
Reduced E
xposure
Sta
ndard
(R
ES
)
Reduced E
xposure
Enhanced
(RE
E)
*
**
*
*
FN no Fx marking
TP (RES)
TP Fx found in 2nd
rendering (REE)
FP no GT Fx TP both
(RES) and
(REE)
TP (RES)

Example Chest Exam: Original Exposure Standard
(OES) Processing Paired with Enhanced Processing
(OEE)
Origin
al E
xposure
Sta
ndard
(O
ES
)
Orig
inal E
xp
osure
Enhanced
(O
EE
)

Reader#
Original Exposure Standard
(OES)
Reduced Exposure Standard
(RES)
Original Paired with Enhanced
Processing (OEE)
Reduced Paired with Enhanced
Processing (REE)
1 0.6842 0.3368 0.9684 0.8842
2 0.2105 0.2421 0.4316 0.4316
3 0.4105 0.5474 0.7368 0.7158
4 0.5053 0.3684 0.7895 0.7579
5 0.3368 0.5684 0.8211 0.7368
Average 0.4295 0.4126 0.7495 0.7053
Results: Sensitivity
© 2015, Carestream Health

Results: Specificity
Reader#
Original Exposure Standard
(OES)
Reduced Exposure Standard
(RES)
Original Paired with Enhanced
Processing (OEE)
Reduced Paired with Enhance
Processing (REE)
1 0.8426 0.8846 0.7008 0.7692
2 0.8889 0.8922 0.7706 0.8426
3 0.7615 0.7387 0.6641 0.6772
4 0.7167 0.9091 0.5745 0.7632
5 0.7232 0.7339 0.5248 0.5597
Average 0.7866 0.8317 0.6470 0.7224
© 2015, Carestream Health

Summary
• Diagnostic quality images of pediatric patients may be captured with DR
using exposures at least as low as 720 speed.
• DR coupled with the Enhanced Skeletal Processing offers the opportunity
to reduce default pediatric exposures targeting fracture detection.
• Viewing Reduced Exposure (RES) paired with the Enhanced View (REE)
may improve Sensitivity over use of the Original Exposure Standard
(OES) view only, while detecting fractures in DR images.
• Viewing Reduced Exposure paired with the Enhanced View
is comparable to use of the Original Exposure paired with the Enhanced
View, for detecting fractures in DR images.
• Viewing Reduced Exposure paired with the Enhanced View yields
slightly reduced Specificity over use of the OES view only, with
increased Sensitivity over OES.
p.24
© 2015, Carestream Health

Summary (Continued)
The addition of some noise may increase a reader’s ability to see details.
Though, reasonable attempts were made to provide appropriate context to
the readers during the study. i.e.
• Orthogonal views were presented when available
• A “reason for exam” was provided for each exam
The Study was a challenge to perform given:
• Some information was not available to the readers during the study, such
as prior exams, previous diagnoses, and full skeletal surveys
• Learning curve to use the new SW tools
• SW behaviors differed from day to day viewing operations
For these reasons, we focused on changes to sensitivity given the four
treatment pairings.
p.25
© 2015, Carestream Health

www.caretream.com/medical
p.26
© 2015, Carestream Health