Embed Size (px)
Citation preview

Cannulation &
Recirculation IN VV ECMO
Assistant ProfessorCritical Care Medicine
Cairo University
Dr. Akram Abdelbary, MD

Access

Options For Cannulation in VV ECMO
Two Cannulas One double-lumen cannula
D Brodie, M Bacchetta; N Engl J Med 2011; 365:1905-14.

• Drainage cannula– As central as possible– Not too close to the
return cannula• Return cannula
– Close to the tricuspid valve
– But not too close to the drainage cannula
Cannula Placement


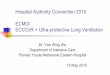
Significantly less flow was required during Femoro-Atrial VV ECMO
Cardiopulmonary Support and PhysiologyA Prospective Comparison of Atrio-Femoral and Femoro-Atrial Flow in Adult Venovenous Extracorporeal Life Support
Preston B. Rich, MD; Samir S. Awad, MD; Stefania Crotti, MD; Ronald B. Hirschl, MD, MS; Robert H. Bartlett, MD; Robert J. Schreiner, MD
Flow required to maintain equivalent SvO2


Fem – Fem Cannulation
IndicationCannulation
in jugular vein not possible.
Higher risk for femoral vein/caval
thrombosis(?)

Cannula
Choice

Influence of ECMO Flow
Schmidt et al., Intensive Care Med., 2013.

Pedersen et al., Ann Thorac Surg 1997
Hemolysis & Cannula Diameter

Q =DP p r4
8 h L
Flow is proportional to the power of 4 of radius
inversely proportional to tubing length and viscosity
1797-1869
Poiseuille’s Law

Joseph-Frédéric-Benoît Charrière 1803-1876
1 Charrière = 1 Fr = 1/3 mm

29 Fr.
25 Fr.
23 Fr.
21 Fr.
19 Fr.Drainage cannula
French size, Flow tables

23 Fr.
21 Fr.
19 Fr.
17 Fr.15 Fr.
Return cannula
French size, Flow tables



AdmissionReturn
Double Lumen Cannula

– Less Recirculation.
– Single access.
– Possible ambulation.
– Bigger cannula and smaller lumen.
– Image guidance is mandatory.
Double Lumen Cannula
Avantages:
Drawbacks:

Cannulation
Two Cannulas
Double-lumen

Specific Details Bi-Caval Dual Lumen

Mobilization: ECMO Devices
Mobilization is possible .
It probably reduces critical illness polyneuropathy, delirium and muscle atrophy.
It may reduce time on ventilation and improve outcome post lung transplantation.

Double-Lumen NovaPort Femoral
Size: 24 Fr. Bloodflow approx. 2.0 L/min. Recirculation. Indication: CO2 removal.
Also available: 18 Fr, 22 Fr jugular.

Insertion

Percutaneous insertion
Guide-wire – Dilators – Cannulas: Use the right tools

188 cannulation attempts.
11 cannulation failures.
3 arterial punctures.
• One leading to distal necrosis.
1 SVC laceration VCS.
1 fatal hemothorax.
• SVC perforation by Reinfusion Cannula.
Venovenous Extracoporeal Life Support Via Percutaneous Cannulation in 94 Patients*
Thomas Pranikoff, MD; Ronald B. Hirschl, MD’; ‘Robert Remenapp, RRT; Fresca Swaniker, MD and Robert H. Bartlett, MD, FCCP
Chest 1999; 115:818-822.

Transesophageal Echocardiographic Guided Placement of a Right Internal Jugular Dual-Lumen
Venovenous Extracorporeal Membrane Oxygenation (ECMO) Catheter
Mazzeffi M J Cardiothorac Vasc Anesth, 2013
Mid-esophageal four-chamber TEE view with white arrow
showing improperly positioned cannula in the right ventricle.
Modified mid-esophageal bicaval TEE view using color Doppler
compare mode showing return blood flow in the center of the
right atrium directed towards the tricuspid valve. (Color version of
figure is available online).

Dolch et al, ASAIO, 2011.

Always use ultrasound guidance…
Ultrasonic locating devices for central venous cannulation: meta-analysis
Daniel Hind, Neill Calvert, Richard McWilliams, Andrew Davidson, Suzy Paisley, Catherine Beverley, Steven Thomas

Complications

Damage to Vessel and Tamponade

Malpositioning

Dislocation of Cannula

Risk of Thrombosis
78 post-mortem examinations in VA-
ECMO:
Venous thrombosis in 25 patients.
Fatal PE in 2 patients.
“The true incidence of thromboembolic
events is highly underestimated by
clinical evaluation”.
Rastan AJ et al., Int J Artif Organs 2006; 29:1121-31.

Further Problems
infection
Air

Recirculation with
VV ECMO

Limitations to Oxygenation
Blood flow / drainage.
Fraction of oxygen delivered through membrane.
Membrane function / efficiency.
Recirculation.

What is Recirculation?
Abrams et al, ASAIO 2014
Proportion of oxygenated blood captured by the ECMO system and reinjected into the ECMO circuit, instead of being pumped
Does not share in patient oxygenation

Increasing Spre O2 without other clinical change
Spre O2 > Peripheral SaO2
When to suspect Recirculation?

O2 post oxy
venous O2 Without ECMO
O2 preoxy
How to calculate Recirculation?
FR = Recirculation flow Drained blood flow

Recirculation =
SpreO2 - SvO2
SpostO2 - SvO2
Anderson et al., Trans, 1989

SvO2 = SmvO2
CVL method – venous sat from SVC or IVC.
SvO2 method – Turning off sweep gas
while maintaining patients’ SaO2 via
ventilator.
Limited role in practice.
Van Heijst ASAIO, 2001

Ultrasound
Dilution

Darling et al., ASAIO 2006.

Cannula type.
Cannula position.
Pump Flow
Volume status.
Cardiac function.
Patient Position.
Factors Affecting Recirculation

210 410 610 76002468
1012141618
0
8
17
13
2
9
17.5
11
Dilutional Ul-trasound
Pump Flow Rate (ml/min)
NS
NS
NS
NS

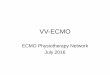
Recirculation Fraction at Different Flow Rates in Nine Animals*
Nine lambsUnicaval dual-lumen cannula
CVL Method (%)
SvO2 Method (%)
Ultrasound Dilution
Method (%)
Flow Rate (ml/kd –
min)
62.5+6.9 45.0+6.9 36.0+12.8 150
54.8+13.5 39.3+9.5 32.8+9.3 125
39.1+17.6 31.7+8.2 24.6+9.4 100
29.5+15.7 24.5+12.6 20.2+6.5 75
29.6+15.7 12.4+10.0 13.0+4.0 50

Extra drainage cannula can help achieve
target flow at less RPMs
Ichiba, Ann Thorac Surg 2000

J Artif Organ 14
Impact Of Bypass Flow Rate And Catheter Position In Veno-venous Extracorporeal Membrane
Oxygenation On Gas Exchange In VivoKonomi Togo, Yoshiaki Takewa, Nobumasa Katagiri

J Artif Organ 14
Impact Of Bypass Flow Rate And Catheter Position In Veno-venous Extracorporeal Membrane
Oxygenation On Gas Exchange In VivoKonomi Togo, Yoshiaki Takewa, Nobumasa Katagiri

J Artif Organ 14
Impact Of Bypass Flow Rate And Catheter Position In Veno-venous Extracorporeal Membrane
Oxygenation On Gas Exchange In VivoKonomi Togo, Yoshiaki Takewa, Nobumasa Katagiri

A novel strategy to improve systemic oxygenation in venovenous extracorporeal membrane oxygenation: The “X-configuration”
Massimo Bonacchi, MD; Guy Harmelin, MD; Adriano Peris, MD and Guido Sani, MD
The Journal of Thoracic and Cardiovascular Surgery, November 2011

A novel strategy to improve systemic oxygenation in venovenous extracorporeal membrane oxygenation: The “X-configuration”
Massimo Bonacchi, MD; Guy Harmelin, MD; Adriano Peris, MD and Guido Sani, MD
The Journal of Thoracic and Cardiovascular Surgery, November 2011

RCT of 30 patients with severe ARDSX-configuration (n = 16)
VsStandard 2-site setup (n = 14)
Less recirculation – 5.3% vs 29.4%
Higher SaO2
Facilitated less ventilator support

V-RV Configuration
Recirc at 4L/min: 8.4% vs 37.9%∆ Recirc per L/min: 2.9% vs 11.1%
Lindstrom, perfusion 2012
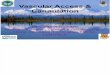
Oxygenated return blood
Tricuspid valve
prevents recirculation
Venous drainage (to
circuit)
Mixed drainage (to
circuit)
Recirculation
Effective flow
Oxygenated return
blood

Bicaval Dual-Lumen Cannula
Abrams et al., 2014

Wang-Zwische Double Lumen Cannula – Toward a Percutaneous and Ambulatory Paracorporeal Aritificial Lung
Dongefang Wang, Xiaoqin Zhou, Xiaojun Liu, Biu Sidor, James Lynch, and Joseph B. Zwischenberger
ASAIO Journal, 2008
DLC tip in IVC DLC tip dislodged into RA0
10
20
30
40
50
60
Rec
ircu
lati
on
(%
)

ICM, 2012
Quantification Of Recirculation As An Adjuvant To Transthoracic Echocardiography For Optimization Of Dual-lumen Extracorporeal
Erik P.J. Körver Yuri M. Ganushchak Antoine P. Simons Dirk W. Donker Jos G. Maessen Patrick W. Weerwind

Management
Trend SpreO2 and peripheral SaO2.
Reposition cannulae and patient.
Dual-lumen cannulae when feasible.

Q 3+0.5 ml/min/m2
FmO2 100%-SGF adapted for normal pH & PCO2
SaO2 88-92% - Ultraprotective ventilation
Reduced QECMO+Hemolysis
Adaquate QECMO
SaO2 < 88%
SvmO2 > 60%
Excessive recirculation
Cannula replacement
Fibrin depositionPmO2/FmO2 < 300
Oxygenator dysfunction
High VO2
QECMO
Lung contribution (PEEP/FiO2)
Hb CO?
Kicking?Fluctuating QECMO?
High inflow pressure?
Kicking of the lines?
Mechanical Problem
Cannulas/membrane thrombosis
Change circuit+ check for cannulas permeability
Recannulation
Inadequate venous drainage
HypovolemiaCannulas malposition
Pneumothorax/Tamponade

Summary
Cannula Choice: The bigger the better. Careful positioning preferably
ultrasound gided. Transesophageal echocardiography or
fluoroscopic guidance is advisable (esp. Avalon).
Good monitoring to avoid complications.

Summary
Recirculation compromises ECMO efficiency
Ultrasound dilution may help quantify recirculation.
Development of bicaval dual-lumen cannulae have helped minimize recirculation.
Efforts to decrease recirculation are helpful in maximizing oxygen delivery.