Embed Size (px)
Citation preview

1
Best Practices for Physician Call Coverage
Compensation

Today’s agenda
• MD Ranger intro• A brief history of call coverage• Commercial reasonableness, or: to pay or not to pay?• Paying for call: rates and analysis• Basic elements of coverage agreements• Effective strategies for setting call rates
2
250+ Physician Benchmarks• Call coverage rates• Medical direction payments• Administrative and leadership
services rates• Hospital-based service stipends• Diagnostic testing, etc.• Clinic & hourly rates
Online Platform• Benchmark lookups• Contract proposal tools• Contract reports by facility and service• Total facility costs + benchmarks
Compliance Documentation• Contract-specific FMV documentation
reports• Reports to assist with real-time
monitoring and annual reviews
Research and Support• Resources for education and training• On-call experts to help subscribers
use benchmarks and tools
3

The foundation of your compliance process
Standardize processes and rates
Document FMV
Access 250+ payment
benchmarks
Review contracts and monitor with
easeHave smarter,
data-driven physician
negotiationsMitigate
compliance risks
4
5
Our subscribers
6
Our benchmarks• Call Coverage (55+)• Medical direction (85+)• Hospital-based services (15+)• Administrative• Medical Staff Leadership• Diagnostic/other services e.g.
ROP, autopsy, dialysis• Hospital-based stipends• Clinics, professional services• Telemedicine• Residency/teaching/GME
• Uncompensated care• Meeting attendance, peer review,
IT/EHR and quality initiatives• 13 Pediatric services, with more
emerging each year
Hospital-characteristics drill down for ADC, bed size, trauma status, urban/rural, stroke centers, and more.
Used in academic medical centers, integrated delivery systems, and hospital organizations.

Our methodology: key differences
• Providers vs. facilities• Verified data• Thorough data audits• Physician contract experts on-
call to review/advise on challenging contracts
• Comprehensive scope of benchmarks based on full hospital contracting practices
7
Meeting the unique challenges of healthcare organizations
Make data-driven decisions for your organization
Stop relying on poor data sources
Streamline documentation and ensure you are protected against costly settlements
8

Value for consulting firms
Benchmarks for 250 physician services, most of which can be found no where else, at your fingertips.
Benchmarks for making strategic financial and operational choices, like total call coverage costs and benchmarks on number of positions
Online platform for organizing and tracking your clients' performance, as well as easy, on the go lookup tools for MD Ranger physician comp benchmarks
9

About me
10
• Chief Marketing Officer at MD Ranger
• Decade plus experience in health care, specifically pertaining to the hospital/physician relationship
• Fueled by serving our subscribers, black coffee, and snuggles from my toddler
11
A BRIEF HISTORY OF CALL COVERAGE

Once upon a time
35+ years ago….• Physicians on the medical staff took call as a part of
their privileges• Seen as a way to build their independent practices
12
Shifts in emergency care
• EMTALA (1986)• State laws• Growth in burden of uninsured and Medicaid in the
ED
13
(Additional) federal regulations
• Seventies: AKS• Eighties: Stark
14

Market forces and hospital/physician relationships
• Attitudes shift for coverage and leadership duties
• Market consolidation of both physicians and hospitals
• Hospital pressures to reduce costs
15
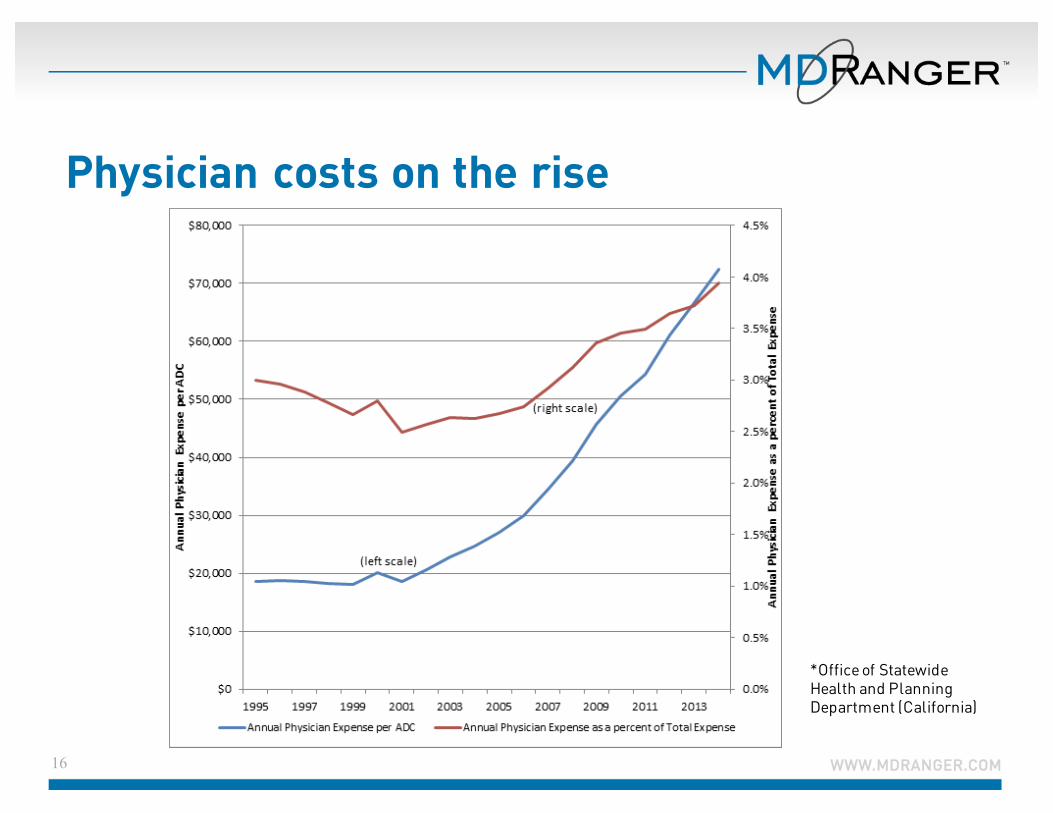
Physician costs on the rise
16
*Office of Statewide Health and Planning Department (California)
TO PAY OR NOT TO PAY
17
Much to consider
ü Is coverage for the position necessary and does it meet commercial reasonableness tests?
ü Should you factor opportunity cost?ü What’s the market rate for the service?ü What is current hospital policy for paying for coverage?ü How much will paying for coverage in this service impact
other physicians on the medical staff?ü Does the position significantly reduce a physician’s
potential compensation related to her practice?ü What’s the ED volume?
18
Not all positions should be paid
• Not all coverage positions should be paid, even services that are most commonly paid
• There are likely good arguments for paying or not paying a physician to take call
19
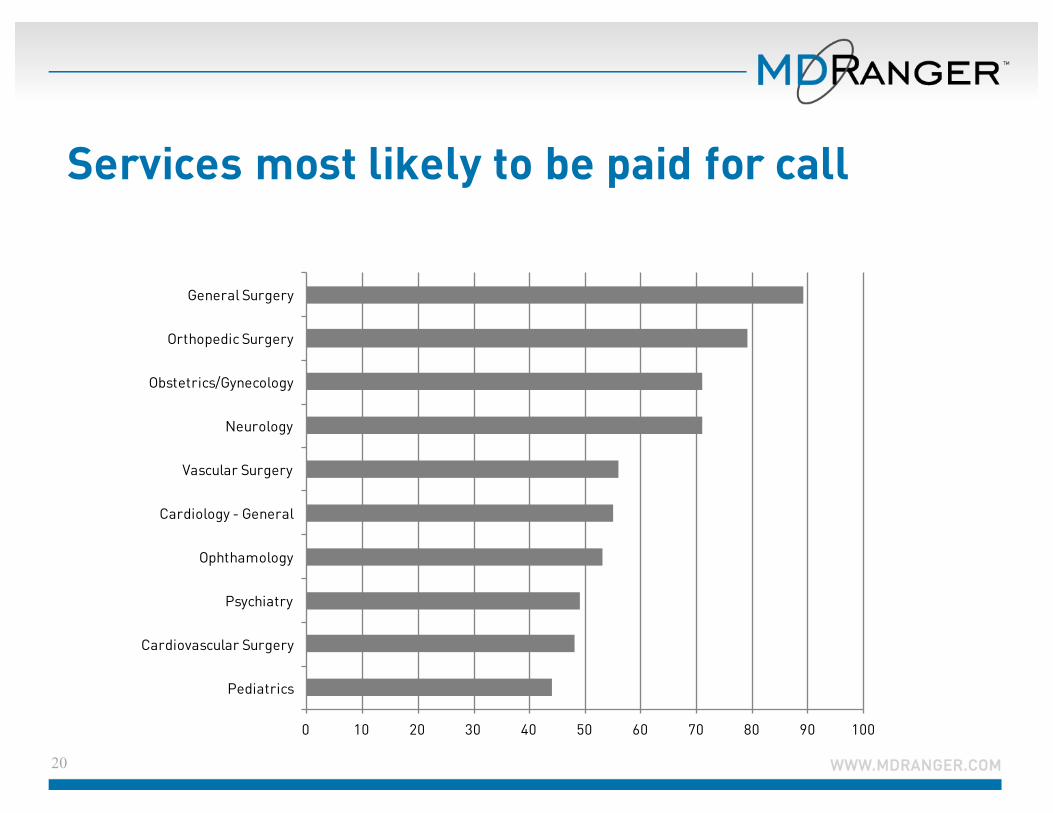
Services most likely to be paid for call
20
0 10 20 30 40 50 60 70 80 90 100
Pediatrics
Cardiovascular Surgery
Psychiatry
Ophthamology
Cardiology - General
Vascular Surgery
Neurology
Obstetrics/Gynecology
Orthopedic Surgery
General Surgery
Understand everyone’s perspectives
• What is the physician asking for? What is the underlying causes of the payment request?
• What is your organization’s position on call compensation? Is there a precedent or medical staff bylaw requirements?
21
Comfortable paying? Now what?
• Is it commercially reasonable to do so?
• What is commercial reasonableness, and how can you determine if the position and situation in question is commercially reasonable to pay?
22
Commercial reasonableness
An arrangement that is a sensible, prudent business arrangement, from the perspective of both parties involved, even in the absence of potential referrals.
23
Using market data to establish commercial reasonableness
• How common is it for hospitals to pay?• If many or most hospitals pay for coverage, data can
be used as part of the argument that payment is necessary.
• If you believe you must pay for the service given your market, though others aren’t, build the case based on facts that differentiate your facility and consider a valuation that demonstrates commercial reasonableness.
24
Remember: FMV and commercially reasonable do not mean the same thing
• FMV and commercial reasonableness are not the same• A payment rate may be within fair market value but not be
commercially reasonable
25
PAYING FOR CALL: RATES AND ANALYSIS
26
Each hospital is unique (but similar enough)
• Each hospital is different (size, service offerings, market, payer mix, etc.)
• Hospitals are similar enough that one can look to peer hospitals for guidance in setting rates. Market data is a good way to do this, as long as it is high quality and detailed enough for your needs.
27
Frequently called services
There are services across organizations that are utilized more frequently for emergencies
• General surgery• Internal/hospital medicine• Orthopedic surgery• Gastroenterology• Cardiovascular services
28
Median coverage per diem rates for frequently paid services:
• General surgery: $800• Internal/hospital medicine: $500• Orthopedic surgery: $980• Gastroenterology: $500• Cardiovascular services:
• $600 general cardiology• $850 for cardiovascular surgery• $600 for interventional/STEMI
29
Significant factors that influence rates
30
• Specialty • Restricted/Non-restricted (e.g., trauma surgery:
$2,310 per diem)• Number of campuses covered• Hospital size• Trauma status
Factors that do not have a statistically significant impact on rates include urban/rural, DSH, Medicare percentage, major geographic region, and ownership status
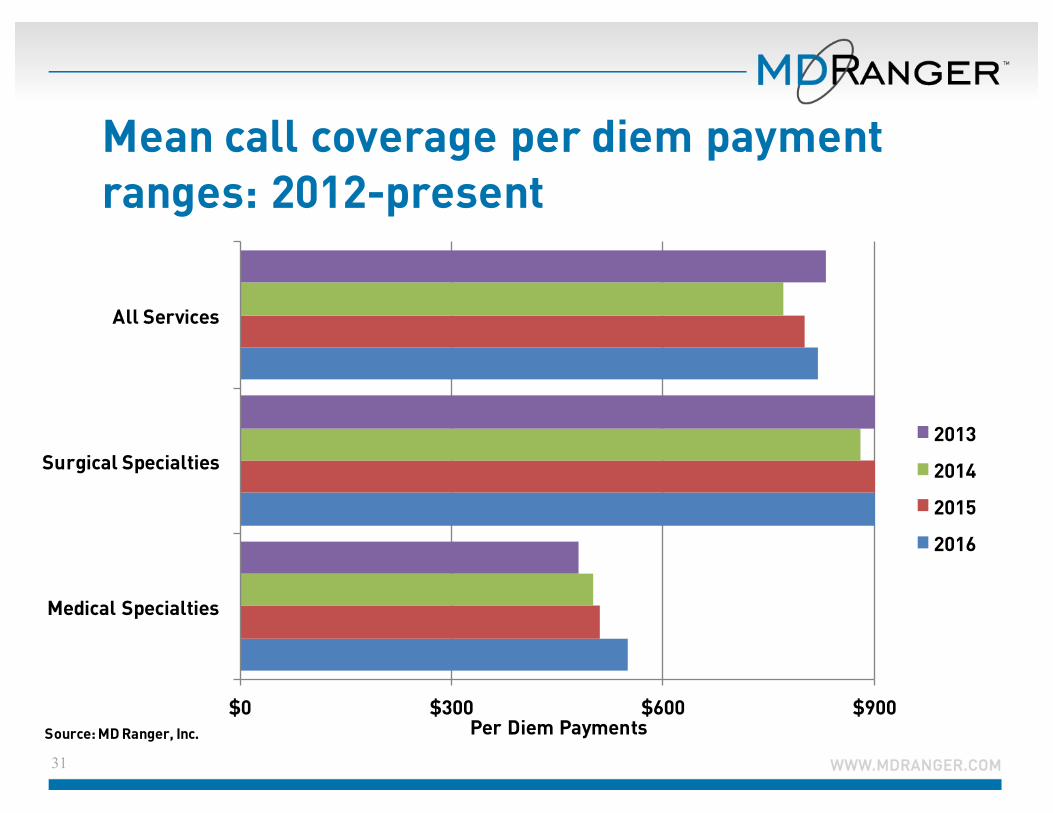
Mean call coverage per diem payment ranges: 2012-present
31
$0 $300 $600 $900
Medical Specialties
Surgical Specialties
All Services
Per Diem Payments
2013
2014
2015
2016
Source: MD Ranger, Inc.
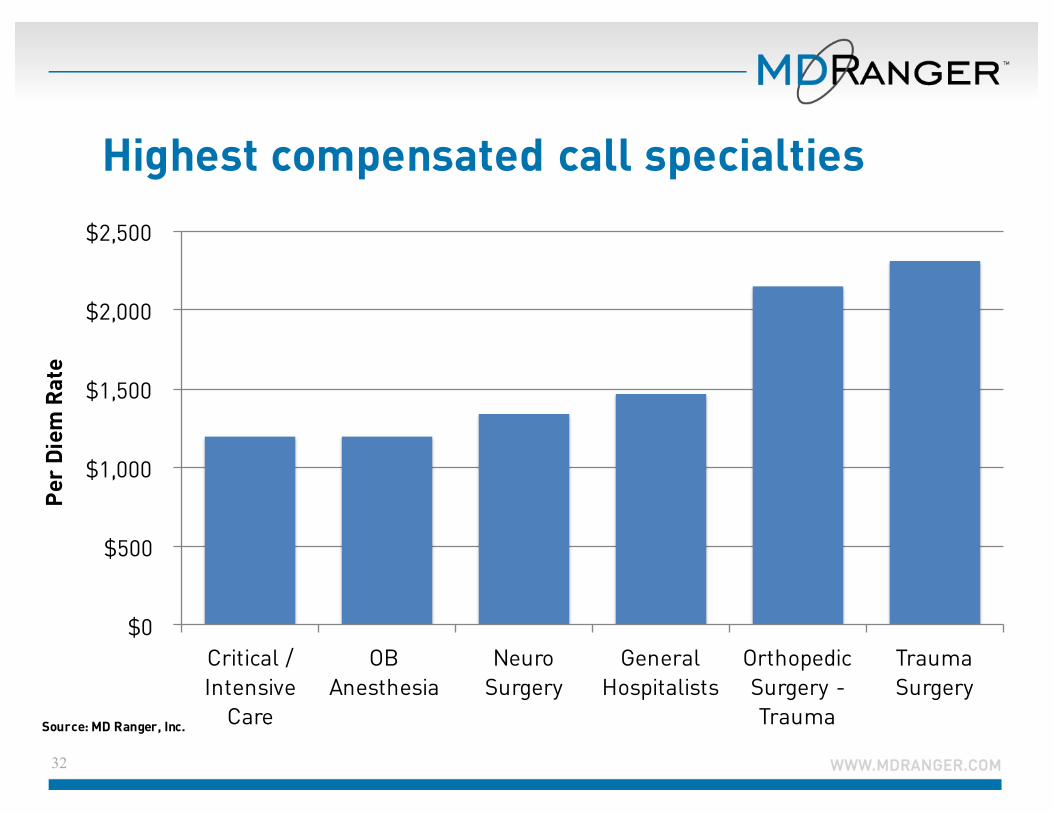
Highest compensated call specialties
32
$0
$500
$1,000
$1,500
$2,000
$2,500
Critical / Intensive
Care
OB Anesthesia
Neuro Surgery
General Hospitalists
Orthopedic Surgery -Trauma
Trauma Surgery
Per
Diem
Rat
e
Source: MD Ranger, Inc.
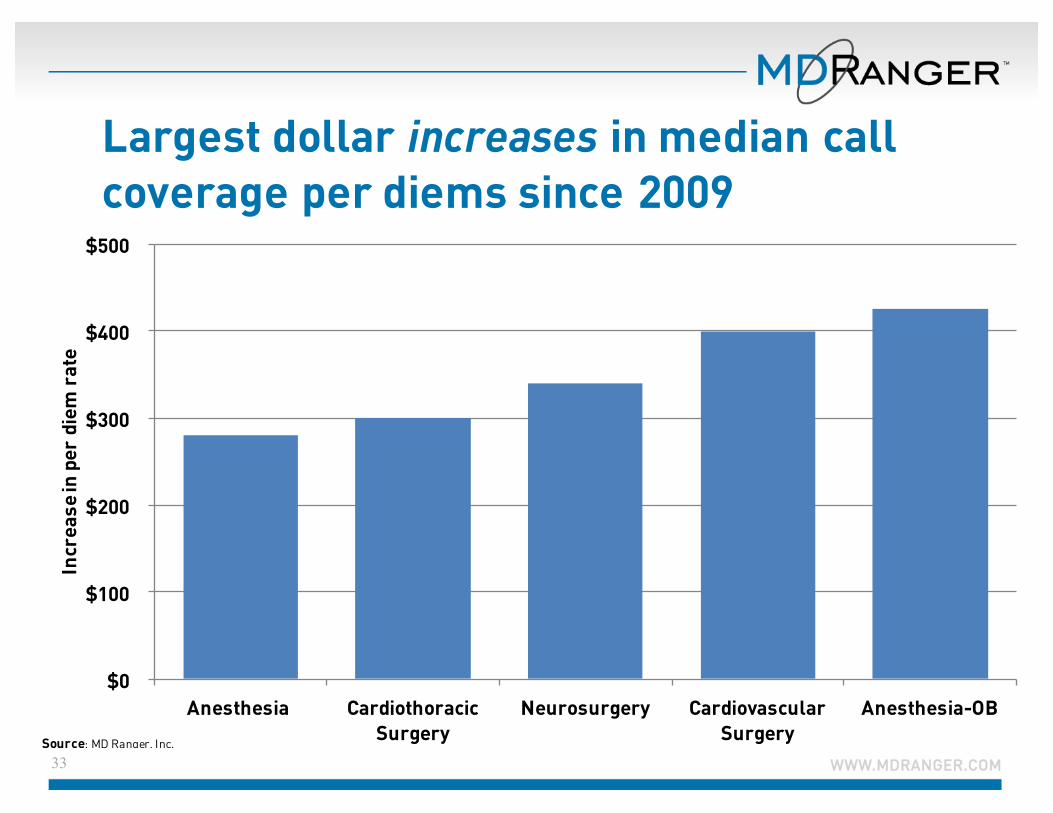
Largest dollar increases in median call coverage per diems since 2009
33
$0
$100
$200
$300
$400
$500
Anesthesia Cardiothoracic Surgery
Neurosurgery Cardiovascular Surgery
Anesthesia-OB
Incr
ease
in p
er d
iem
rat
e
Source: MD Ranger, Inc.
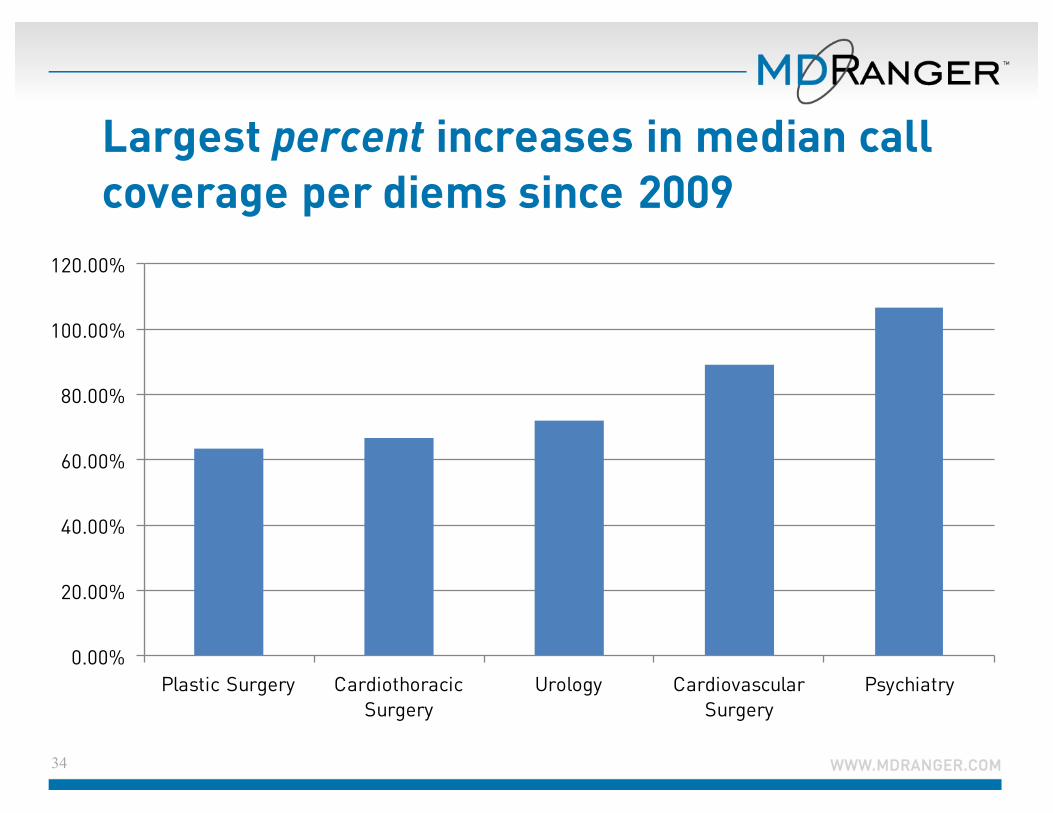
Largest percent increases in median call coverage per diems since 2009
34
0.00%
20.00%
40.00%
60.00%
80.00%
100.00%
120.00%
Plastic Surgery Cardiothoracic Surgery
Urology Cardiovascular Surgery
Psychiatry
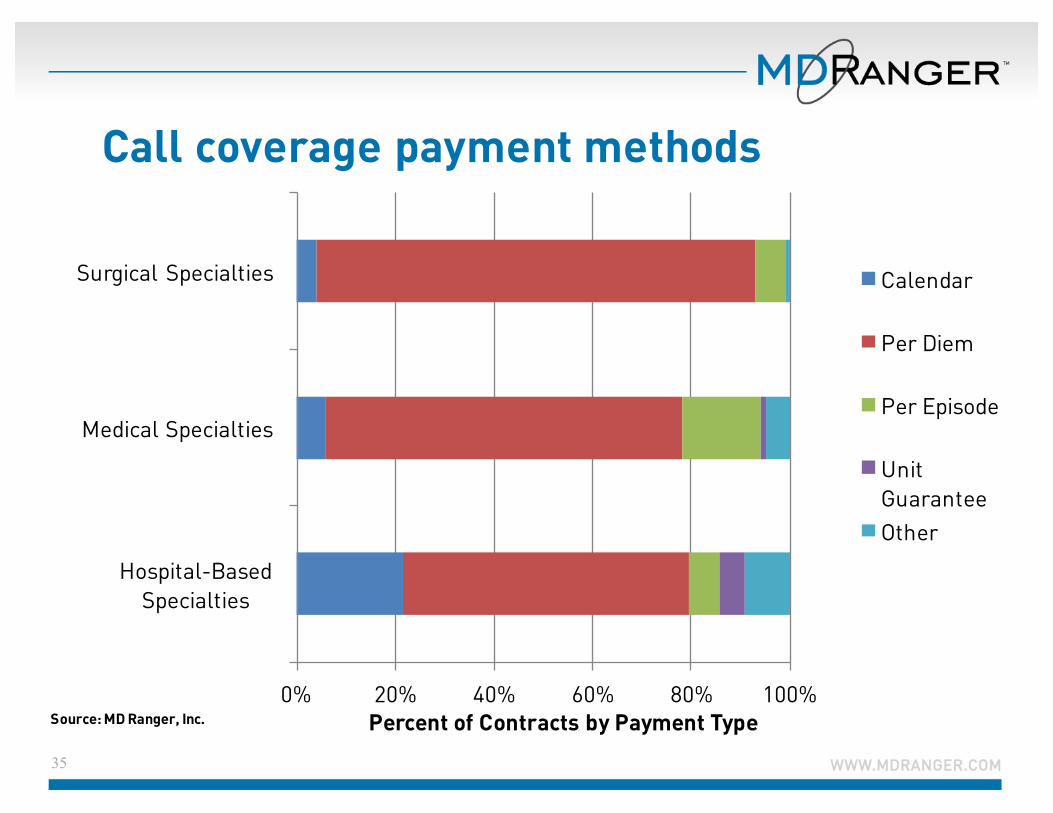
Call coverage payment methods
35
0% 20% 40% 60% 80% 100%
Hospital-Based Specialties
Medical Specialties
Surgical Specialties
Percent of Contracts by Payment Type
Calendar
Per Diem
Per Episode
Unit GuaranteeOther
Source: MD Ranger, Inc.
BASIC ELEMENTS OF COVERAGE AGREEMENTS
36

Key elements of coverage agreements
• Specify which one (or more) of the following mechanisms of compensation are used: per diem payment, per episode payment, or uncompensated care payments
• Clarify whether service includes coverage of in-house referrals from other physicians for unassigned patients (in addition to ED coverage)
37
Key elements of coverage agreements
• State whether or not there are restrictions on the physicians activities
• Identify in the agreement if there is a second on-call physician, and discuss how payment will be handled if yes
• Establish who is responsible for the schedule to ensure continuous coverage and name the individual (or party) in the contract
38
Key elements of coverage agreements
• State in the agreement if exclusive rights are granted to the panel or to the medical group
• Decide if it’s best to have a panel in which physicians are restricted from any material private practice income generating activities—this can be reasonable to ask if specialization in acute inpatient care leads to better clinical outcomes.
39

40
EFFECTIVE STRATEGIES FOR SETTING CALL RATES
Creating a standard, simple-to-use physician contracting process is more important than ever
• Your process should have straightforward policies and procedures.
• Try sticking to one or two templates to more easily monitor compliance instead of having different compensation frameworks for each physician contract.
41
Creating a standard, simple-to-use physician contracting process is more important than ever
• Standardize benchmark levels across specialties and require administrative and board review and sign-offs
• Consistently use externally validated benchmarks• Routinely review contract rates and documentation
42
Three approaches to determining call coverage rates
• Market data• Internal or external
proprietary formulas• Internal or external ad hoc
FMV opinions (cost method)
43
Most hospitals use a combination of two or all three methods
All approaches have strengths and weaknesses
• Market Data:• Pros: cost effective, flexible, easy to scale, immediate access• Cons: doesn’t work in all cases, like when there’s no market
data available
• Proprietary formulas:• Pros: easy to scale, immediate access• Cons: aren’t transparent to the parties involved, setting up
can be expensive
• FMV Opinions:• Pros: most detailed and specific• Cons: difficult to scale, expensive, slow turn around
44
MD Ranger subscribers:
• Use market data for the vast majority of physician contracts, including call coverage
• Pull in valuation firms or experts for more complex agreements, again, not typically call coverage
• Always document their rates with proof of FMV, whichever method they choose
45
Consider alternatives:
• Not paying• Uncompensated care payments• Per episode payments• Combination payments
46
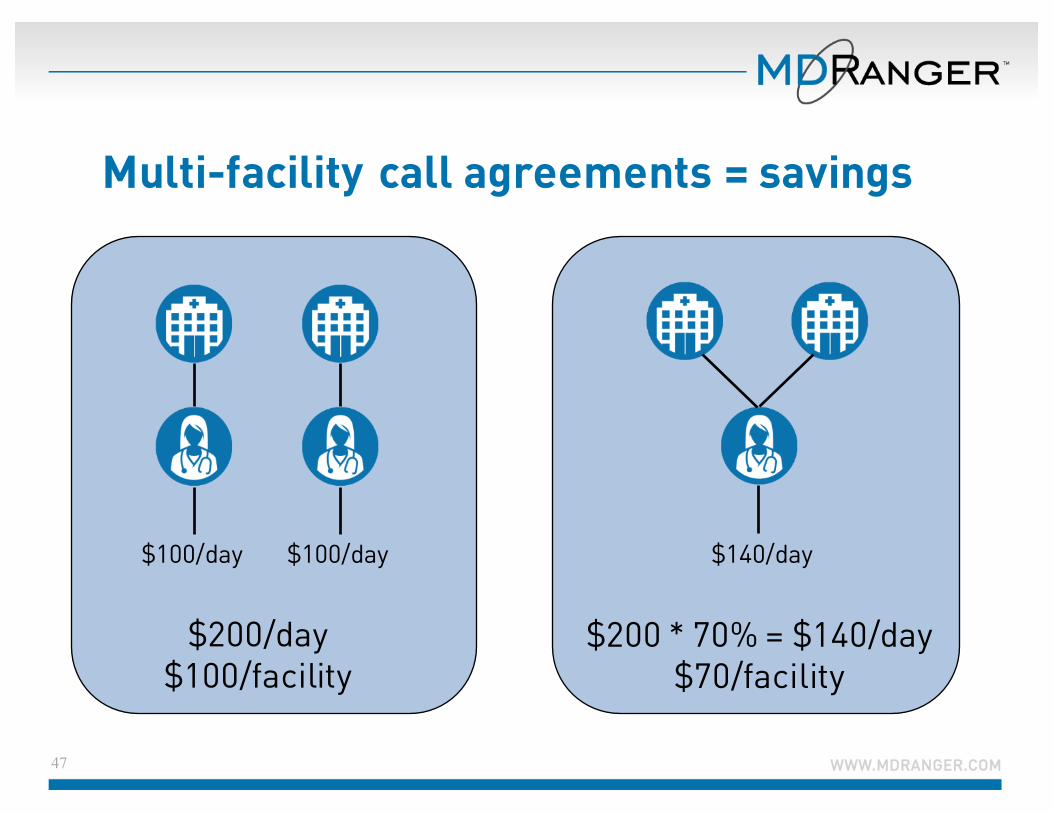
Multi-facility call agreements = savings
47
$100/day $100/day
$200/day$100/facility
$140/day
$200 * 70% = $140/day$70/facility

Need help setting call coverage payment rates and documenting FMV? Call us.
48
Ø Do you feel confident in your organization’s physician contracting and FMV documentation process?
Ø Are you confused how much to pay physician leaders for their time?
Ø Do you feel like your organization has risky agreements?
We can help! Reach out: [email protected] or 650-692-8873