Embed Size (px)
Citation preview
Implementing the Care Act: Policy in
Practice
Implementation challenges and priorities for 1 April 2015
16/17 reform (funding and appeals)
Andrew Burridge, NW Care Act
Programme Manager
Implementing the Care Act: Policy in
PracticeImplementation challenges and priorities for 1 April 2015
16/17 reform (funding and appeals)
Andrew Burridge, NW Care Act
Programme Manager
Complex legal framework
• 1960s – series of scandals based around large psychiatric institution see a move to community based care
• Local Authority Social Services Act (1970) – establishing social services committees, the formal role of Director, and the need to act under the general direction of the Secretary of State.
• Chronically Sick and Disabled Persons Act (1970) – introduced a duty on the LA to assess the individual needs of adults who met the criteria within the National Assistance Act
• Disabled Persons Act 1986 – enabled individuals and carers to request an assessment.
• Social Security Act 1986 – replaced Supplementary Support with Income Support, with a tighter financial criteria.
• 1988 Independent Living Fund introduced – small direct payments to people with severely disability and low incomes
• NHS and Community Care Act 1990 – established the duty to provide a service if needs are established as eligible. New arrangements for assessment and care management and individuals receiving individual tailored packages of care. As long stay hospitals closed an assumption that people will receive care in their own homes.
• Community Care and Direct Payments Act 1996 – local authorities enabled to provide cash payments to people rather than provide a service.
• Health and Social Care Act 2001 – mandatory to provide direct payments
• Health and Social Care Act 2008
• Health and Social Care Act 2012
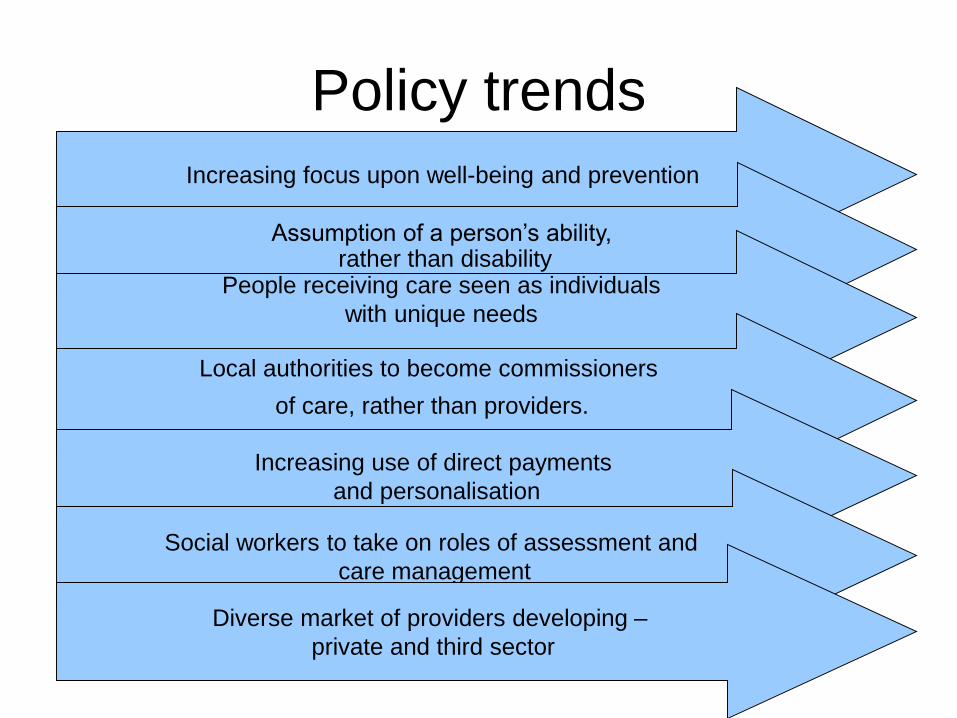
Policy trends
Increasing focus upon well-being and prevention
Assumption of a person’s ability,rather than disability
People receiving care seen as individuals
with unique needs
Local authorities to become commissioners
of care, rather than providers.
Increasing use of direct payments
and personalisation
Social workers to take on roles of assessment and
care management
Diverse market of providers developing –
private and third sector
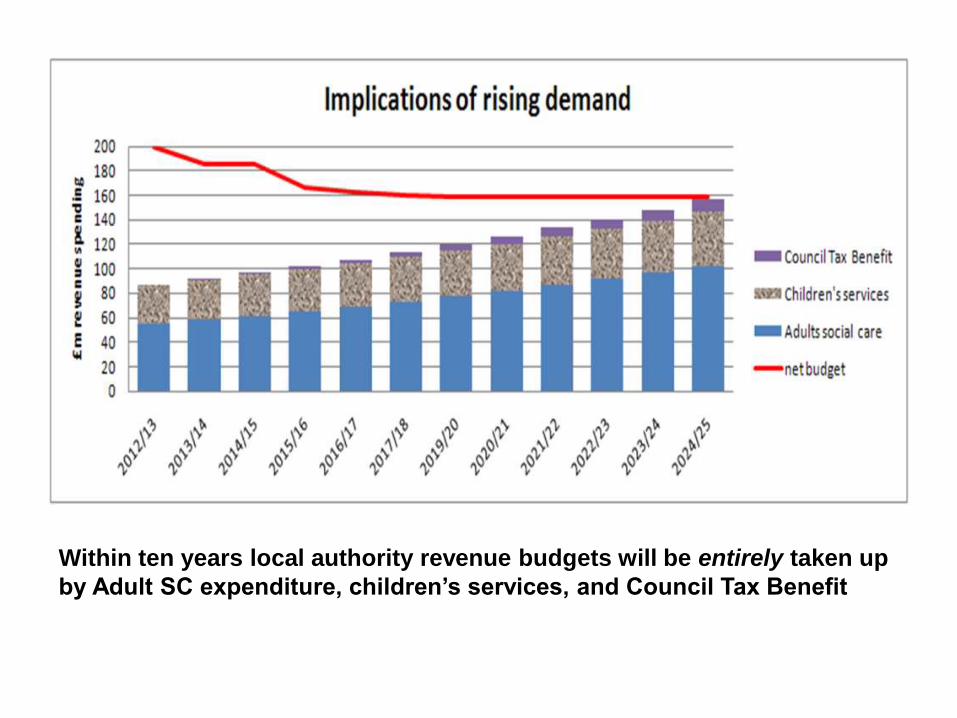
Within ten years local authority revenue budgets will be entirely taken up
by Adult SC expenditure, children’s services, and Council Tax Benefit
• Places well-being, and outcomes, is at the centre of every decision
• Focus on prevention and delaying needs, and integration and partnership working is reinforced
• Provides a single framework for social care addressing:– Assessment (extending rights to self-funders)
– Carers
– Charging and financial assessment
– Advocacy
– Person centred care and support planning
– Adult safeguarding
– Integration and partnership working
– Moving between areas (portability) and transitions
– Delegating functions (third party assessments)
– Prisons
– Sight registers (visual impairment)
– Managing provider failure
Care Act 2014: Single framework for social care
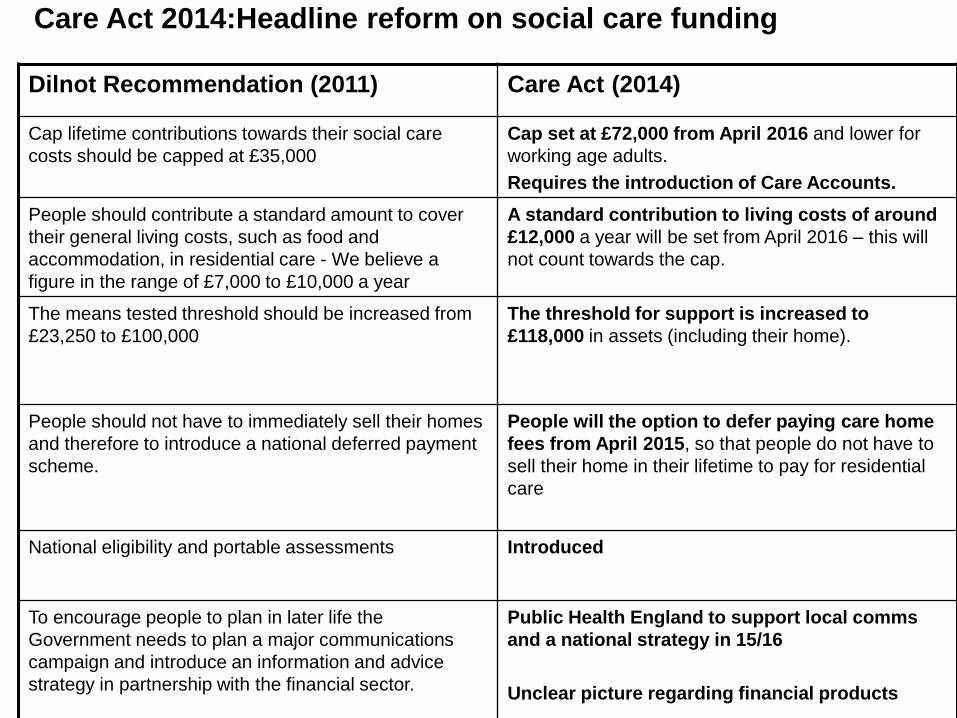
Dilnot Recommendation (2011) Care Act (2014)
Cap lifetime contributions towards their social care
costs should be capped at £35,000
Cap set at £72,000 from April 2016 and lower for
working age adults.
Requires the introduction of Care Accounts.
People should contribute a standard amount to cover
their general living costs, such as food and
accommodation, in residential care - We believe a
figure in the range of £7,000 to £10,000 a year
A standard contribution to living costs of around
£12,000 a year will be set from April 2016 – this will
not count towards the cap.
The means tested threshold should be increased from
£23,250 to £100,000
The threshold for support is increased to
£118,000 in assets (including their home).
People should not have to immediately sell their homes
and therefore to introduce a national deferred payment
scheme.
People will the option to defer paying care home
fees from April 2015, so that people do not have to
sell their home in their lifetime to pay for residential
care
National eligibility and portable assessments Introduced
To encourage people to plan in later life the
Government needs to plan a major communications
campaign and introduce an information and advice
strategy in partnership with the financial sector.
Public Health England to support local comms
and a national strategy in 15/16
Unclear picture regarding financial products
Care Act 2014:Headline reform on social care funding
What should be in place for 1 April
2015?• The third national stocktake is our best evidence
regarding progress
• Overall a positive picture for changes from April 201599% of councils say that they are very or fairly confident that they will be able to deliver the Care Act Reforms from April 2015, compared to 97% in stocktake 2 and 90% in stocktake 1.
• Concerns relate to– demand and cost
– Market sustainability
– Finance and IT
– Market sustainability
• Local authorities should be compliant with the legal framework…
Cornerstones Legal Manuals
Cornerstones Legal Manuals
• All local authority Care Act leads and council
solicitors should have access to these
• No fundamental overhaul
• Inevitably much will be established via case law
although Cornerstones have shared some useful
precedents
• Likelihood is some organisations will have their
challenges ready from 1 April – consultation was
raised as a potential area…
Wellbeing
Section 1 of the Act creates a new statutory duty to promote the wellbeing of individuals. The ‘wellbeing principle’ is a guiding principle for the way in which local authorities should perform their care and support functions.
It involves “actively seeking improvements”
• Applies to people whose needs are not eligible
• A list of ‘factors’ are included, far reaching ranging from personal dignity, protection from abuse, participation in work and education, and domestic and personal relationship.
• The individual will have the best view which of these factors are important
Assessment and EligibilityThe LA will need to:
• carry out an assessment of anyone who appears to require care and support, regardless of their likely eligibility for state-funded care
• focus on how needs and impact on their wellbeing, and the outcomes they want to achieve
• involve the person or other people in the assessment
• provide access to an independent advocate if required
• consider other things besides care services that can contribute to the desired outcomes (e.g. preventive services, community support)
• use the new national minimum threshold to judge eligibility for publicly funded care and support
Assessment and Eligibility
• Concern regarding widening of eligibility threshold and definition of ‘significant’
– To be eligible someone must1) Have needs arising from physical or mental impairment or
illness
2) Be unable to achieve two or more of the specified outcomes
3) As a result there be a significant impact on the person’s wellbeing
– Ultimately rests upon consideration of evidence, and the assessors’ professional judgement (SCIE & Cornerstones)
Assessments and Eligibility
• Review policy and procedure
• Understand at what point the LA can take
into account local resources
• Ensure IT systems are up to date (or find
an interim fix)
• Understand the requirement to give a
written record of the eligibility decision
• Review people currently receiving care
Charging and Deferred Payments
• The Government’s intention was to not substantially change the existing law on charging.– LAs retain discretion, and may wish to review
charging policies in light of the Care Act.
– Can charge arrangement fees to self-funders.
– Consultation in this area appears particularly important.
– Discretion to offer DPA has turned into a duty.
– A framework for tops ups, although the LA must ensure that at least one option is available and within the person’s Personal Budget.
Deferred Payments
• DH has provided a model deferred
payment agreement.
• Have shared information on fees
• One of our LAs has led on a training
package that we are delivering across the
region
• Local authorities are unclear if they need
to consult on the arrangements.
Carers
Carers put on equal footing
• An equal right to an assessment, where a carer appears to have needs
• Carers should receive a personal budget setting out the cost of meeting their needs and the amount the local authority will pay
Local authorities are having to:
• Understand eligibility for the carer – the concept of ‘necessary care’ and what significant impact means for carers.
• Understand what services will be available for carers who are ineligible – all should receive a statement setting out whether they have eligible needs and how their needs will be met; and all carers should be offered information and signposting to services aimed at improving their wellbeing and preventing need.
Challenges include:
• Identifying the numbers of carers and anticipate the assessments required – census suggests very high numbers
• Understanding how indicative budgets are put together and shared
The NW Carers Network has developed an assessment framework providing some tools for understanding carers needs:
• Carers Assessment Framework
• Determining ‘Necessary Care’
• Measuring the effect of the caring role on the carer
• Assessing significant impact on the carers’ wellbeing
• Resource Allocation System for Carers
NW Carers Assessment
Framework
Market shaping
• A duty to support a market for adult social care that delivers a wide range of care and support services.
• Duties on local authority to manage provider failure. Local authorities would ultimately already by likely to step in and should have contingency plans.
• Risk of upward pressure on market fees in residential and nursing care – particularly the ‘top-up’ subsidy issue.– Postponed to April 2016 – the right of a self funder to request LA
support in arranging for needs to be met is likely to see transfer of private payers to lower local authority fee levels.
• Regional or sub-regional strategic partnerships with providers?
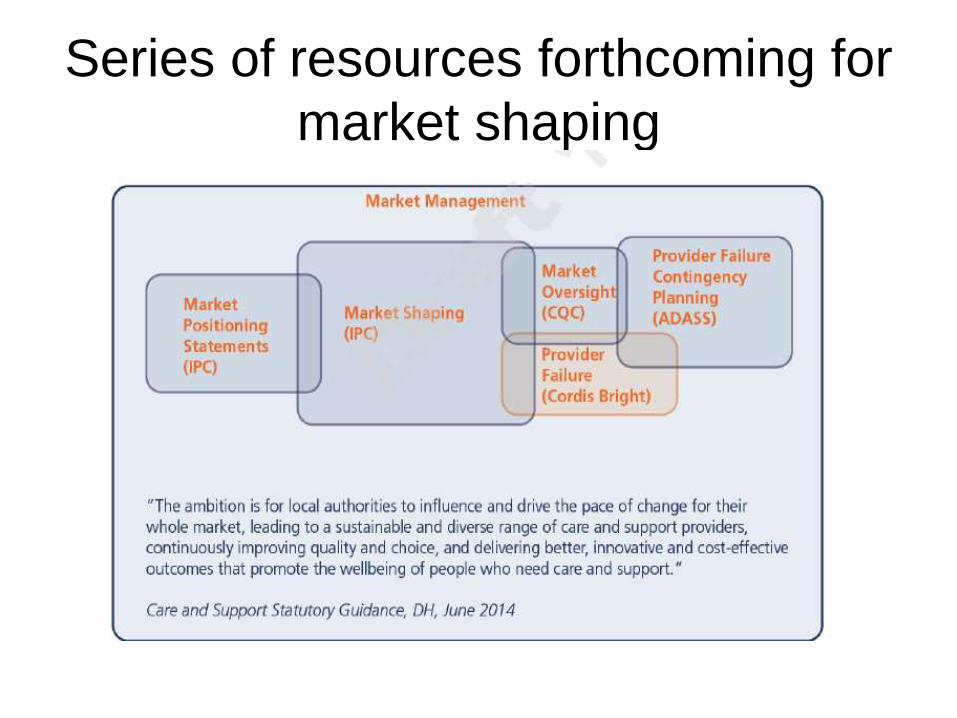
Series of resources forthcoming for
market shaping
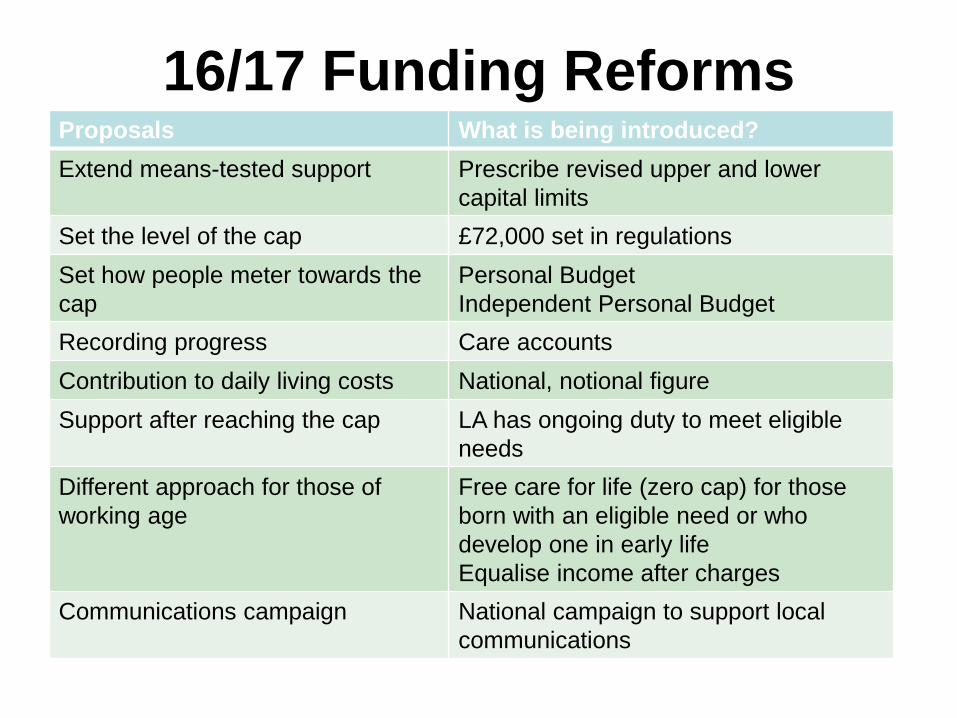
16/17 Funding ReformsProposals What is being introduced?
Extend means-tested support Prescribe revised upper and lower
capital limits
Set the level of the cap £72,000 set in regulations
Set how people meter towards the
cap
Personal Budget
Independent Personal Budget
Recording progress Care accounts
Contribution to daily living costs National, notional figure
Support after reaching the cap LA has ongoing duty to meet eligible
needs
Different approach for those of
working age
Free care for life (zero cap) for those
born with an eligible need or who
develop one in early life
Equalise income after charges
Communications campaign National campaign to support local
communications
What else?
• Appeals
– Locally commissioned service
– Duplicating existing complaints
– Will be explained in the January consultation
• Introduction of the delayed right for self
funders to ask the local authority to
arrange residential care
Key messages from DH Charging
Policy Lead• Local authorities should start thinking about this activity now
– Should be mapping the self funders, including engaging providers
• May feel slightly simpler that 15/16 but remember 15/16 implementation will still be being carried out.
• DH are aware that the General Election presents some planning risk for local authorities. However, this is very much Plan A and they urge against a ‘wait and see’ approach.
• Want to encourage proportionate, light touch financial assessment to establish Care Accounts.
• They want to encourage ambitious use of statements for Care Accounts, particularly online methods and methods that put this point of contact in the context of the local prevention, information and advice, and communications strategies.
• Stressing that progress towards the cap starts from the time the person requests the assessment.
• Unresolved questions about:– Daily Living Costs of £230 a week
– Tiered caps for working age adults (seen as less important now)
– How local authorities agree the ‘rate the LA would pay’ in order to calculate personal budgets.
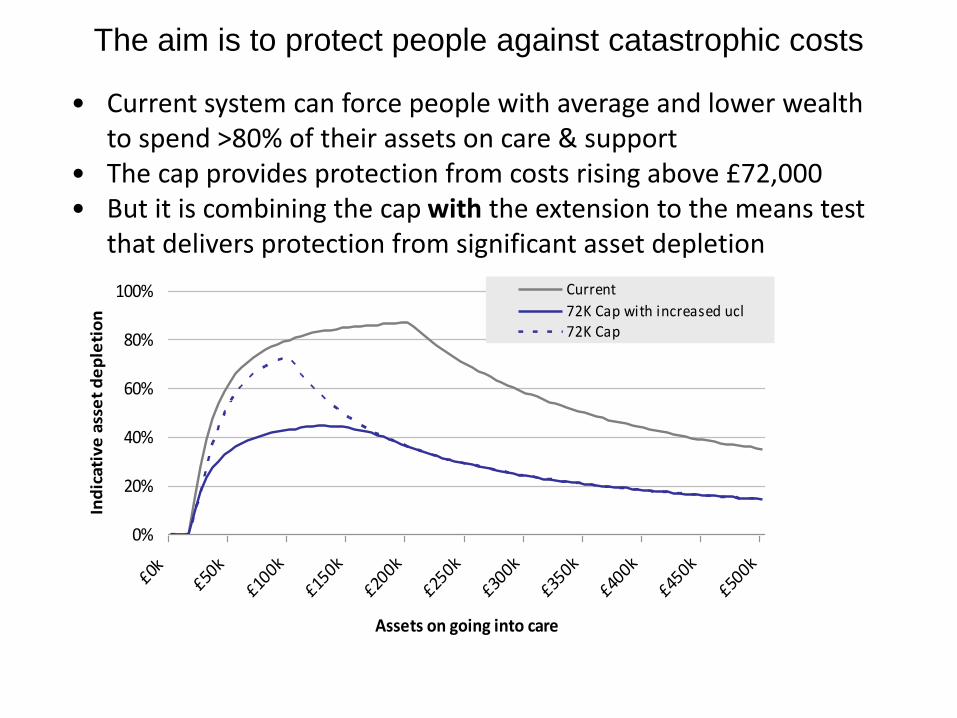
The aim is to protect people against catastrophic costs
0%
20%
40%
60%
80%
100%
£0k£50
k
£100k
£150k
£200k
£250k
£300k
£350k
£400k
£450k
£500k
Assets on going into care
Ind
icat
ive
ass
et
de
ple
tio
n
Current
72K Cap with increased ucl72K Cap
• Current system can force people with average and lower wealth to spend >80% of their assets on care & support
• The cap provides protection from costs rising above £72,000• But it is combining the cap with the extension to the means test
that delivers protection from significant asset depletion