Embed Size (px)
Citation preview

Abstract: Clinicians commonly useelectrical stimulation (ES) to controlacute edema. But, exceptfor anecdotalreports, there is little evidence to sup-port that practice. We recently con-ducted a series of controlled, blindedstudies on several nonhuman animalmodels to determine the efficacy ofseveral forms of ES, but high-voltagepulsed current (HVPC) in particular, incontrolling acute posttraumatic edema.We observed that acute posttraumaticedema is curbed by HVPC when certainprotocols are used. Results of thesestudies suggest to us that wave fomn,polarity, treatment schedule, intensityand frequency of pulses all influenceES, and that clinical protocols needrevision.
A thletic trainers and physicaltherapists are among those whofrequently use various forms of
electrical stimulation (ES) to controlacute edema. High-voltage pulsed cur-rent (HVPC) probably has been advo-cated more than any other form of ESfor this application, although to datelittle evidence has been reported fromcontrolled studies of therapeutic effectsfor any form of ES for acute edema.Indeed, evidence to support use of ESfor edema control is remarkably weak.
Historical ReviewLicht'9 attributed to Murat (1783) the
observation that "electrification hadbeen successful in such conditions as... , edema of the limbs, ...." Unfor-tunately, neither Licht nor Muratprovided any support for this statement.More recently, Newton," in describingthe first HVPC unit from 1945, ascribesto the DynaWave NeuromuscularStimulator anecdotal evidence that itwas useful in treating decubiti, bums,sprains, strains, and pain. Crisler,9 how-ever, seems to have been the first to
Frank C. Mendel is an associate professorofanatomy in the Department ofAnatomicalSciences at the State University ofNew Yorkat Buffalo, NY 14214.Dale R. Fish is an associate professor of PT& exercise science at the State University ofNew York at Buffalo.
New Perspectives in
Edema Control via
Electrical Stimulation
Frank C. Mendel, PhDDale R. Fish, PhD, PT
provide any clinical evidence that ESwas useful for treating "sprains, strains,and charley horses." He claimed "com-plete relief," usually after only three orfewer treatments of 5 minutes or less onsuccessive days. Crisler reported"vigorous muscular twitching," whichhe called "deep massage," and at-tributed the relief of signs andsymptoms of sprains and strains to thisactivity. He also mentioned avasomotor effect as being important, aswell as "a direct nervous effect," butexplained neither, nor did he providereferences. Crisler used an ultrafaradicM-4 impulse generator, which wascapable of generating up to 300V, had afrequency rate of 4-30 pps, and pulseduration of only a few microseconds.Crisler did not specify wave shape otherthan faradic, but other parameters aretypical of high-voltage stimulators.
Newton25 suggested that commonuse of HVPC began in 1974 as a resultof a national advertising campaign byElectro-Med Health Industries. It wasnot until 1981, however, that protocolsand rationales for those protocols beganto be published. Newton23 presented apaper on the theoretical physiologicaleffects of HVPC at the Annual Con-ference of the American PhysicalTherapy Association. This paper laterwas expanded into a monograph24 by anHVPC supplier and was provided aspart of the documentation with equip-ment. Alon' also produced a seeminglyinfluential monograph on HVPC thatwas published by a manufacturer ofhigh-voltage stimulators.
Alon' discussed a variety of applica-tions of HVPC, but cited Crisler9 as the
sole reference to support use of HVPCfor edema control. Soon after Newton' sand Alon's works came a series ofpapers that extolled the virtue of incor-porating HVPC into existing regimens.Brown7 claimed that HVPC (and inter-mittent compression) "in conjunctionwith other rehabilitation techniqueshave proved very effective in reducingedema and speeding recovery," butcited only Alon,' who in turn cited onlyCrisler.9 Brown,7 apparently unawarethat he was working with two activeelectrodes of the same polarity, advo-cated reversing polarity for 15 minutesafter an initial 15 minutes of stimulationto tolerance and concomitant intermit-tent pressure (from Jobst boot). He sug-gested that alternating polarity served tospeed healing by moving interstitialfluid, thereby decreasing pooling, ad-hesions, and pain. The editor (Knight)noted that some of the points presentedby Brown were only conjecture and thatthere were no "substantial data to indi-cate the effectiveness of these treat-ments; ...." However, Knight went onto say that many respected cliniciansclaimed success in reducing edema withHVPC. Ross and Segal'9 claimed"remarkable" results treating postopera-tive patients for pain, edema, and woundhealing using HVPC. These authorsconcluded that HVPC is similar to gal-vanic current (ie, direct current) and at-tributed a variety of "polar effects" toHVPC. On the basis of these presumedattributes, Ross and Segal developedprotocols that brought these reputed ef-fects to bear. They provided two casehistories. Finally, Quillen (1981 and1982, cited in Alon and DeDomenico3)
Journal of Athletic Training 63

is stated by Alon to have resolved swell-ing of Grade I and II sprains in an
average of 3 to 4 days using sensory-level stimulation.
Lamboni and Harris18 claimed thatthe effects of ice, elevation, and com-
pression could be made "even more ef-ficient" in reducing effusion with theaddition of HVPC, but cited no refer-ences. They postulated that musclecontractions evoked by HVPC ". .
.'milks' the exudate from the area, in-creasing lymphatic drainage," and thatthe stimulation promotes production of
enkephlins (sic), which is thebody's natural anti-inflammatoryagent." They provided no references tosupport this alleged action forenkephalins.
26Newton and Karselis examined ef-fects of HVPC on the pH of skin underelectrodes and concluded that no
polarizing effects were detectable atthese sites after 30 minutes of con-
tinuous cathodal HVPC at 100V and80-82 pps. Although not directly re-
lated to use of ES for control of edema,observations made by Newton and Kar-selis seemed to counter the belief thatHVPC produced long-lasting polar ef-fects, ie, produced electrical fieldscapable of inducing unidirectionalmigration of ions.
Santiesteban et a130 compared the ef-ficacy of medium frequency interferen-tial current with cold compression andcontrast baths in reducing pain andswelling and increasing ROM in sub-acute ankle sprains. It is unclear howthis experiment was executed, but itseems that there were only four peoplein each group. Treatment protocols foreach group were unspecified, as were
degree of injury and time elapsed sinceinjury. The authors concluded, how-ever, that medium frequency interferen-tial current was at least as effective as
cold compression and contrast baths.Voight34 noted that use ofHVPC for
post-traumatic edema had been reportedby many, citing Crisler9, Alon', Brown,7and Gieck,'2 but characterized thesereports as "subjective evaluations" andnot based on thorough research. Seem-ingly on the basis of those subjectiveevaluations, however, Voight con-
cluded that clinically, HVPC seemed tochange capillary fluid dynamics, which
resulted in reduction in edema. He thenspeculated that HVPC might retardblood flow into extracellular spaces byenhancing clotting, inducingvasoconstriction by stimulating sym-pathetics, and repelling negativelycharged plasma proteins, therebypreventing them from leaving capil-laries or dispersing them once they hadescaped. Voight further speculated thatpositive polarity might facilitate throm-bus formation, but enhance leakage ofnegatively charged plasma proteins.(Negative polarity might repulse plas-ma proteins, but prolong time for throm-bus formation.) In other words, Voightassumed that HVPC had polarizing ef-fects like direct current. His proposedprotocol was to alternate positive andnegative stimulation (to achievebenefits and minimize disadvantages ofboth) at 60-80 pps at tolerance or atsubmotor level "to ensure that no furtheraggravation of the tissues takes place"for 20 to 30 minutes, but conceded thatthe best time was unknown.
Ralston27 noted that little was pub-lished on the use of HVPC, so he con-
ducted a survey of 19 athletic trainers todetermine how and why HVPC wasbeing applied. Most followed the in-structions provided with theirstimulators. Ralston concluded that,"There is very little, if any, 'state of theart' research published that gives defini-tive uses for high voltage galvanicstimulation." He then, mysteriously,went on to say, "A protocol for the mosteffective use of high voltage galvanicstimulation can, in fact, be synthesizedfrom the knowledge we possess on thesubject today." He proceeded to listvarious protocols.
Mohr et a122 were apparently the firstto conduct controlled experiments todetermine the effect of HVPC on exist-ing edema. Specifically, they attemptedto ascertain whether HVPC could ac-celerate resolution of already resolvingedema. They traumatized one hindlimb of a series of rats, and after 24, 48,and 72 hours, treated half the animalswith cathodal HVPC at 80 pps, 40V for20 minutes. Animals were unrestrainedexcept during treatment so that muscleactivity might have influenced out-comes, but they reported that volumesof treated limbs did not differ sig-
nificantly from those ofuntreated limbs.This led them to conclude that moreresearch was needed and that HVPCwas at least not "contraindicated in thetreatment of traumatic edema."22
Alon and DeDomenico3 providedsome physiological rationale for whyHVPC might be applied to controledema, and then, after noting that thisrationale was as yet unsubstantiated,suggested several provisional protocols.After reviewing the supporting litera-ture (again Crisler9 and Quillen,1981,1982), they concluded that:"Present data concerning the specificvalue of TENS in edema or joint ef-fusion absorption are so limited that onemust wait for future studies to confirmor refute the claims for its effective-ness."
Michlovitz et al2' compared ice andice plus HVPC in the treatment of gradeI and II acute lateral ankle sprains.Ankles of 10 subjects were elevated andreceived ice and wrap for 30 minutes oneach of 3 consecutive days; ankles of 10others were elevated and received iceand HVPC at submotor levels and 28pps; ankles of 10 others received thesame treatment as group II except theirHVPC was administered at 80 pps.Volumes of ankles in each of the threegroups were reported not to be sig-nificantly different after the first andthird treatments. However, changes involume following treatments were fre-quently less than the measurement errordetermined during reliability testing.Conclusions based on volume measure-
ments are, therefore, suspect. Range ofdorsiflexion and decreases in pain didnot differ among groups.
Gieck and Saliba'3 described variousforms of ES and their reputed applica-tions; only HVPC was listed amongthose forms of ES as a viable mode foredema modulation. They endorsed itsuse for this purpose by stating that theyused it in their clinic, but included onlyNewton23,24 and a manufacturer's guidebook'7 in their references.
Griffin et al'5 seem to have been thefirst to observe a "clinically sig-nificant," albeit not a statistically sig-nificant, treatment effect for HVPC inreducing chronic rather than acuteedema. These investigators only ex-
amined 10 people in each of three test
64 Volume 280* Number 1 * 1993

groups (intermittent pneumatic com-
pression, HVPC, and sham-HVPC) andstill just missed achieving a significanttreatment effect for HVPC, ie, therewere not significant differences be-tween intermittent pneumatic compres-
sion and HVPC or between HVPC andplacebo-HVPC, but differences were
significant between intermittentpneumatic compression and placebo-HVPC. These results were promising,but not yet conclusive.
Finally, Cosgrove et al8 examinedthe effects on trauma-induced edema ofmonophasic pulsed current and sym-
metrical biphasic pulsed current relativeto a control. Like Mohr et al,22 theyexamined the influence ofES on alreadyresolving edema. They administeredsubmotor stimulation or sham treatmentto rat hind paws for one hour at 24, 48,and 72 hours post-trauma. They usedsubmotor stimulation to "isolate effectof electrokinetic influences on proteinmobility," but let animals move aboutfreely between treatments, ie, voluntari-ly induced muscle pump effects. Basedon volume measurements performedbefore each treatment, they concludedthat there were no significant differen-ces between monophasic pulsed current
and control groups or betweenmonophasic pulsed current and sym-
metrical biphasic pulsed current groups
in accelerating diminution of naturallyresolving edema. They went on to
proclaim that ". procedures currentlyused in the clinic do not significantlyreduce existing edema caused bytrauma in rat hind limbs."
Despite a lack of supportingevidence, HVPC continues to bepromulgated in current texts, eg, 2,13,25 as
viable therapies for acute edema, al-though others are more cautious, eg,
3,10,31
In summary, clinicians have beenand continue to use ES, HVPC in par-
ticular, to control edema, although therewere no controlled studies that clearlydemonstrated the efficacy of thismodality. An optimal protocol usingHVPC for any edematous conditionwas, therefore, unknown.
Our ResearchIt was with this background in mind
that we began a series of studies
0
0
ai)
>
.0)
C)
0
05-
100r
* Frog * 120 PPS. Impact - 90% Visible Motor Threshold* High Volt (Pulsed) - Immersion.Continuous - ImmRedite Multiiplre (Fhorusr 3min Rx;
..'........ ....... .''
I.,l.,...,.......
_o-. ".'. '. '.i
I-........ ......................
80
60
40
20
n(I0 4 8 12
Time in Hours
designed to determine if ES, and HVPCin particular, affect edema. Demonstra-tion of clinical efficacy of any form ofES for control of acute edema requirescontrol for such variables as age, sex,
health, severity of injury, time from in-jury to treatment, site of injury, anddifferences in physiology from one in-dividual to the next. Studies of animalspermit much greater control of variablesand, hence, require much smaller
16 20 24
samples and far less time and expense.
Use of these models requires the as-
sumption that the physiology of themodel specified is sufficiently similar tothat of humans, that a therapeutic effectin the model is likely to be manifestedin humans as well. With those caveatswell in mind, we began our investiga-tions. The remainder of this com-
munication is a summary of thoseinvestigations using frogs4-6,11,16,32,33 and
66 Volume 28* Number 1 * 1993
u

rats2o as models. We believe that resultsof these studies are potentially relevantto those who treat acute edema, and, ata minimum, provide a strong rationalefor clinical trials.
Summary of MethodsThe procedure for all studies was the
same. We anesthetized the animals,painted lines on their legs, measuredvolume displacement of their feet andlegs, and traumatized both feet of eachanimal using a uniform method (weightdrop or hyperflexion). We then ran-
domly selected one limb for treatment,usually beginning a series of 30-minutetreatments interspersed with 30-minuteor 60-minute rests. We measured limbvolumes (using water displacement)immediately after trauma and afterevery treatment and rest, sometimes up
to 24 hours postinjury. We statisticallycompared treated and untreated limbvolume changes (mL/kg body weight).We anesthetized frogs by immersion
in aqueous solutions ofMS222 (3 aminobenzoic acid ethyl ester; 3 g/L water),and anesthetized rats with in-traperitoneal injections of Inactin.Anesthesia could be maintained in frogsfor 24 hours by dripping anesthetic overthem. Rats were anesthetized with a
7o 100
0
o) 80
0
> 60
(DEr 40
oV 20
U)
* Rat
* Impact* High Volt (Pulsed)* Continuous
* Cathodal
8
single injection for only 4.5 hours. Wedetermined limb volume displacementby placing the animal in a cloth sling,suspending the sling from a camera
boom, and lowering the boom until thehind limb to be measured was sub-merged in an immersion vessel to a linepreviously painted on the limb. We col-lected the water that subsequentlyspilled from the overflow chamber in a
small beaker and weighed it on a
microbalance. We determined thereliability of this volume measurementsystem by performing 30 repeatedvolume measurements on each of fouruntraumatized frog hind limbs. Thecoefficient of variation ranged from0.79% to 1.01% (mean=0.88%), or an
ANOVA-based intraclass correlationcoefficient of 0.995. Measuring bothlimbs of a rat 20 times produced an
intraclass correlation coefficient of0.99.
Typically, we induced trauma bydropping a steel rod through a verticaltube from a uniform height onto theplantar aspect of a foot just distal tomalleoli. In one study, however, we
induced sprains by hyperflexing anklejoints of frogs with a motor that forcedfeet through a uniform range of motionat a uniform rate.4
* 120 PPS* 90% Visible Motor Threshold* Immersion* Four 30min Rx; 30min Rests
...........
..................
..................
... ...
............................................................................................................................
......................................................................................................................................................................................................
.................................
....
...............
0 4 12 16 20 24
Time in Hours
We randomly assigned limbs totreatment or control. We then im-mersed hind limbs of an animal inwater-filled beakers. We placed carb-on-rubber electrodes in these beakers so
that water in the beakers served as distalelectrodes, ie, immersion technique.This technique circumvented problemsin maintaining contact of surfaceelectrodes on small, irregularly shapedbody parts and difficulties in applyingelectrodes for long periods. Moreover,it allowed us to repeatedly immerse un-
encumbered limbs for measurement oflimb volumes with no manipulation ofthose limbs. In all but one study," waterin the immersion beakers served as thecathode (electrode with abundance ofelectrons and hence a negative charge).
Typically, we began a series of four,30-minute treatments within 10 minutesafter injury. Individual treatments werefollowed by either 30-minute or 60-minute rest periods. In one study,5 wedelayed 4.5 hours post-trauma and thenadministered treatment for 6 continuoushours. In another study,32 we ad-ministered only a single 30-minutetreatment immediately after trauma wasinduced. At commencement of eachtreatment, we immersed hind limbs inseparate beakers and slowly increasedvoltage until we observed minimal limbmovement in both limbs, ie, we deter-mined grossly visible motor threshold.We randomly selected a limb to receivestimulation at 90% of motor thresholdin all but one ofour studies.33 In that oneexception,33 we exceeded motorthreshold to induce twitches. Havingbrought the control limb to motorthreshold, we stimulated it no further.
We generally provided stimulationvia Intelect 500S (Chattanooga Corp;P.O. Box 4287; Chattanooga, TN37405) high-voltage stimulators. Out-put consisted of pulses, each comprisedoftwo fast-rising phases of 5gs and 8gsduration separated by an intrapulse in-terval of 75ks. We delivered these pul-ses at 120 pps except in the study inwhich we exceeded motor threshold; inthat investigation we delivered them at1 pps. In the only instance in which wedid not use HVPC,'6 we used a low-volt-age pulsed current (LVPC) machine(NTRON 8100; Henley International;104 Industrial Blvd; Sugarland, TX
Journal of Athletic Training 67

77478) capable of producing no morethan approximately 100 V. Thismachine was modified by adding an
internal bridge to produce double-peaked monophasic pulses of negativepolarity (deviate in only negative direc-tion from zero current baseline). Here,"effective" pulse duration was 620-630gs because interphase duration wasvirtually zero. We applied dispersiveelectrodes to the skin overlying hips or
we placed them in the bottom of slingsthat supported the animals throughoutdata collection, ie, covered much of thebelly.
As described earlier, we measuredvolumes before and after trauma, aftereach treatment and rest period, and insome cases, for up to 24 hours post-trauma. A person ignorant of limb as-
signment collected all data. Wetypically incised skin at ankles and feetjust before killing the animals to con-
firm that volume changes were at-tributable to edema and not frankbleeding.We always expressed data as chan-
ges from pre-trauma hind limb volumesper kilogram body weight (mL/kg). Weused analysis of variance (ANOVA)with repeated measures to test the nullhypotheses and we selected a 0.05 levelof significance throughout. We alsoemployed various post hoc tests in thedifferent studies.
Summary of ResultsPositively Curbed Edema Formation
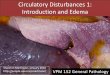
1. Four, 30-minute treatments ofcathodal HVPC, interspersedwith 60-minute rests, applied viaimmersion technique immedi-ately after injury at 120 pps andintensities 10% less than visiblemotor threshold significantly(F[1,5]=12.53, p=.001) curbsedema formation following im-pact injury for up to 17 hours infrogs6 (Fig 1). Note that severalhours after treatments ceased,treated limbs increased slightly involume, whereas untreated limbsdecreased slightly over that time.
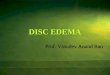
2. Four, 30-minute treatments ofcathodal HVPC, interspersedwith 30-minute rests, applied viaimmersion technique immedi-
intensities 10% less than visiblemotor threshold significantly(F[1,8]=10.41, p=.003) curbsedema formation following im-pact injury in rats20 (Fig 2).
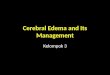
3. Four, 30-minute treatments ofcathodal HVPC, interspersed
o 100
0
a)
> 60
CC40
0)
) 20
C/)
>-
* Frog* Sprain* High Volt (Pulsed)* Continuous* Cathodal
with 60-minute rests, applied viaimmersion technique immedi-ately after injury at 120 pps andintensities 10% less than visiblemotor threshold significantly(F[1,11] =18.83, p=.0001) curbsedema formation following ankle
* 120 PPS* 90% Visible Motor Threshold* Immersion* Immediate Multiple (Four 30min Rx;
1 hr Rests; Monitor 24hrs)
0 4 8 12
Time in Hours16 20 24
ig _.
100
0
o0
> 60
0
40
0_
a)
0)20
CD
* Frog* Impact* High Volt (Pulsed)* Continuous* Cathodal
* 120 PPS* 90% Visible Motor Threshold* Immersion* 30min Rx; Monitor 24hrs
..........
......
-..
.......................................
..... ....
..................................
....
......
0 4 8 12 16 20 24
Time in Hours
ately after injury at 120 pps and
68 Volume 280M Number 1 * 1993
I
I .........
.... .....................
.............................
..............................................
................

sprain for up to 24 hours in frogs4(Fig 3).
4. A single 30-minute treatment ofcathodal HVPC applied via im-mersion technique immediately
after injury at 120 pps and inten-sities 10% less than visible motorthreshold significantly (F[1,81=11.32, p=.003) curbs edema for-mation following impact injury
for more than four hours in frogs32(Fig 4).
5. Cathodal HVPC initiated 4.5hours after injury and applied viaimmersion technique for six con-
tinuous hours at 120 pps and in-tensities 10% less than visiblemotor threshold significantly(F[1,10]=4.146, p=.05) curbsedema formation following im-
pact injury in frogs5 (Fig 5).
No Effect on Edema Formation6. Four, 30-minute treatments of
cathodal low voltage pulsed cur-
rent (LVPC), interspersed with30-minute rests, applied via im-mersion technique immediatelyafter injury at 100 pps and inten-sities 10% less than visible motorthreshold do not significantly(F[1,11]=0.14, p=.71) curbedema formation following im-
pact injury in frogs'6 (Fig 6).7. Four, 30-minute treatments of
cathodal HVPC, interspersedwith 30-minute rests, applied viaimmersion technique immedi-ately after impact injury at one
pps and intensity sufficient to in-duce muscle twitches do not sig-nificantly (F[1,11]=.04, p=.85)curb edema formation in frogs33(Fig 7).
8. Four, 30-minute treatments ofanodal HVPC interspersed with30-minute rests, applied via im-mersion technique immediatelyafter injury at 120 pps and inten-sities 10% less than visible motorthreshold fail (F[ 1,8]=.02, p=.90)to curb edema formation follow-
ing impact injury in frogs" (Fig8).
DiscussionBefore comparing our results with
those of others and hypothesizing the
physiologic mechanisms that might un-
derlie our observations, we wish to dis-
cuss similarities and differences amongour own studies that might be germaneto interpreting information in our
figures. In our figures, we plot results
of individual studies on the compositeresults of all our studies. The legendscontain a more comprehensive explana-tion. In our first three studieS46 (Figs 1,
Journal of Athletic Training 69
. Frog - 120 PPS
. Impact - 90% Visible Motor Threshold
. High Volt (Pulsed) - Immersion
. Continuous - Delayed Single (Delay 4.5 hrs; 6 hrs Rx;
. Cathodal Monitor 24hrs)oo ...............................
...........
---
.... ...... .............
--
... .. ......
.................................... ..............
80.......... ...................................................
4-0 ........................
CD .........................
..
...........................................
.... .................
.....................
......................
20
0- 00 4 8 1 2 1 6 20 24
Time in Hours
- Frog - 100 PPS- Impact - 90% Visible Motor Threshold- Low Volt (Pulsed) - Immersion- Continuous - Immediate Multiple (Four 30min Rx;- Cathodal 30 min Rests; Monitor 24 hrs)
.. ................................................ ..... .......
............... ..........
...............t.. .. .. .. .. .. .. .. .. .. .. .. .. ... .. ... ......
..
..................... ].
...
4-a ..............
(D ......
...........
..
Y)
C/)--O0- 0
0 4 8 12 16 20 24
Time in Hours

3, and 5), we suspended frogs in slingsduring treatment and measurementswith limbs in dependent position, butwe placed them prone during restperiods between and after treatments.Prone positioning might be expected toinfluence total amount or rate of swell-ing. Indeed, in our third study,5 we
placed frogs in prone position during the4.5 hours between trauma and the treat-ment and again after treatment ceased.The values during the first 4.5 hours fortreated and untreated limbs were nearlyidentical, and both sets of limbs were
within the range of treated limbs in allstudies in which a treatment effect wasevident (Fig 5). This suggests that, atleast under certain circumstances,HVPC is as effective in curbing edemaas maintaining an edematous part at thelevel of the heart. Only after treatmentbegan did rates of swelling betweentreated and untreated limbs begin todiverge. Because of the apparent treat-ment effect of prone positioning, we
maintained animals in their slings withlimbs in dependent position throughoutall subsequent experiments, ie,1116,20,32,33 Also, unacceptable numbers
of hematomas forced us to reduce theweight and height from which theweight was dropped in our last fivestudies. 1,16,20,32,33 Amount and durationof edema among studies are, therefore,not strictly comparable.
In all but one20 (Fig 2) of our studiesin which a treatment effect was evi-dent,4632 both treated and untreatedlimbs swelled. That is, only in rats20 didwe observe an absolute reduction ofedema in treated limbs. In the otherstudies, swelling was significantly lessin treated limbs than in untreated limbs,but swelling was only curbed, notprohibited or reduced, in treated limbs.This curbing lasted varying amounts oftime; a single 30-minute treatment sig-nificantly curbed edema in treated limbsfor at least four hours.32 This residualeffect seemed to be extended when mul-tiple treatments were administered.46Treatment effect was clearly finite. Atvarying times after treatments ceased,volumes of treated and untreated limbsconverged.We believe that clear evidence of a
treatment effect in both frogs and ratsreflects a common physiologic response
to trauma and hence to treatment inthese distantly related forms. Frogs andrats have long been studied and used as
models for inflammatory response andwound healing in humans. This is notto say that the physiology of frogs andrats does not differ in significant waysfrom that of humans; thus, results ofstudies of frogs and rats cannot be ap-plied directly to humans (see tl for a
-5 100l-.
0
o) 800
> 60
40C)
20
o
* Frog* Impact* High Volt (Pulsed)* Continuous* Cathodal
more complete rationale for nonhumanmodels and limitations of thosemodels). At a minimum, however,evidence of a treatment effect in bothfrogs and rats is likely to be predictiveof similar effects in humans and, we
believe, provide adequate justificationfor clinical trials.We believe that our studies are im-
portant because, as far as we know, they
1 PPS* Twitches* Immersion* Immediate Multiple (Four 30min Rx;30 min Rests; Monitor 24 hrs), ~~~~~~~~., , ,
.. .. ... ... ... ...................
...........
............................
..........................................
.............................................
.............................................................................................................................................................
................ ...
.........
...............
0 4 8 12 16 20 24
Time in Hours
5 100
c:0
C) 800
> 60
a)
0)20
o O0
* Frog* Impact* High Volt (Pulsed)* Continuous* Anodal
I.. ......
* 120 PPS* 90% Visible Motor Threshold* Immersion* Immediate Multiple (Four 30min Rx;30min Rests)
-.-.-.-.-.......--------..... ...,,A y .b.e ........,,,,,,,,................ .................
1 ............ ~ ~~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
.... ... ..._J^.l.
4 8 12 16 20 24
Time in Hours
70 Volume 28* Number 1 * 1993
-1-1 IJ

are the first to show, under controlledconditions, a clear treatment effect forsensory-level (ie, below visible motorthreshold) HVPC, or any other form ofES, on acute edema, at least during andfor a short time after treatment(s).Others3'7'9'8,27 29,34 have only providedtestimonials to the efficacy of HVPC incontrolling edema. Newton24 observedincreased ROM, but no reduction inedema after HVPC in an uncontrolledstudy. Mohr et a122 observed no treat-ment effect, and Michlovitz et a12'reported none beyond that of ice.Cosgrove et a18 observed that neithermonophasic pulsed current nor sym-metrical biphasic pulsed currentreduced existing edema relative to con-trols. Only Griffin et al'5 observed a
"clinically significant" reduction inchronic edema using HVPC at inten-sities sufficient to induce muscle con-
tractions.As noted, our studies provide, per-
haps for the first time, somejustificationfor using HVPC for treating acuteedema. But others, namely Mohr et a122and Cosgrove et al,8 conducted control-led studies and observed no treatmenteffect for HVPC. We speculate thattime of intervention is critical. If Reed28is correct in suggesting that HVPCreduces permeability of microvessels,then it might be necessary to reduce thatpermeability at a time when proteins(with attendant fluids) are escaping thevascular system. That is, HVPC mightneed to be applied during the acutestage, while proteins and fluids are stillbeing lost from vascular to extravas-cular spaces. Reducing permeabilityafter proteins and fluids have escapedvascular spaces (ie, in subacute stage)might even slow resolution ofedema byretarding movement of escaped fluidinto blood vessels. We typically in-itiated treatment within minutes, but nomore than 4.5 hours, after trauma,whereas Mohr et a122 and Cosgrove et a18waited 24 hours to begin. By this time,edema had reached its peak and mighteven have been resolving. Unfortunate-ly, Mohr et a122 and Cosgrove et a18measured limb volumes at 24-hour in-tervals, immediately before treatments.Consequently, we do not know if the ESthey administered altered limb volumesduring or shortly after treatments. They
observed only that no treatment effectwas discernible nearly 24 hours aftertreatment. It is noteworthy thatCosgrove et a18 reported that mean limbvolumes for control rats were less thanthose for symmetrical biphasic pulsedcurrent-treated rats, significantly so at96 hours post-trauma. The authors notethat symmetrical biphasic pulsed cur-
rent might have had an "adverse effecton edema reduction" and suggest thatthis effect might result from a lack ofresidual net charge. In our view, it isalso possible that either or both forms ofES administered by Cosgrove et almight have reduced vascular per-meability during and for some time aftertreatments and thereby retarded uptakeof fluids back into the vasculature.Hence, limb volumes of treated ratsmight be expected to exceed those ofuntreated animals when such treatmentsare applied in the subacute stage.
Results of some of our studies callinto question the protocols commonlyused in clinics. None of those protocolshave been derived from well-controlled,blinded studies. Several of our studiesstrongly suggest efficacy, but onlybegin to suggest guidelines forprotocols. However, contrary to recom-mendations from some sources,3"13polarity seems to be an important vari-able in the context of using "sensory-level" HVPC for controlling acuteedema." Seemingly, not all forms ofES are capable of curbing acuteedema,'6 although only one HVPC gen-erator and one non-high voltage ap-plication have been examined thus far.If responses of frogs and rats are at allindicative of human responses, thentreatment once a day for 30 minutes toan hour is probably not adequate toachieve meaningful benefits.8'32
Tentative ProtocolResults from our series of experi-
ments lead us to suggest the followingtentative protocol for management ofacute edema: Cathodal HVPC at 120pps at 90% of visible motor thresholddelivered via immersion technique. Wesuggest that 30-minute treatments beapplied every 4 hours beginning as soon
after injury as possible, or as long as
edema is still likely to be forming. Wefurther suggest that treatments continue
only as long as edema is likely to beforming. We are just beginning to testthis suggested protocol in clinics. Itsefficacy in treating humans is, therefore,unknown. Its efficacy relative to othermodalities is equally unknown, as is itsapplicability to chronic edema.
None of our studies provide solidclues to how HVPC might work. Be-cause of the exceedingly short dutycycle of HVPC (less than 1%) and/orbecause anodal HVPC did not exacer-
bate edema formation," we doubt thatthe "electrical field effect" postulated byothers3'8'25 is a significant factor inedema control. Further, strong sensorystimulation (10% less than visible motorthreshold) does not by itself seem toproduce a treatment effect because thislevel of stimulation produced by a low-voltage stimulator'6 and anodal HVPC"failed to curb edema formation. Evenstronger stimulation, producing low-level muscle activity (one twitch persecond), did not produce a treatmenteffect.: When we increased intensity toevoke low-level muscle activity, it wasstill unlikely that we depolarized small-diameter myelinated or unmyelinatedfibers; therefore, we probably did notdirectly activate sympathetics or C-afferents. Thus, we speculate thatwhatever HVPC is doing to curb edemais induced by non-neurological factors.We further speculate, following Reed,28that HVPC might be affectingmicrovessel permeability, which couldin turn, affect both fluid and protein lossto interstitial spaces. Recent, and yetunpublished, work from our lab-oratories shows that anodal HVPCdecreases diameters of histamine-di-lated arterioles, whereas cathodalHVPC has no significant effect. One ofour studies found no treatment effect onedema when using anodal HVPC."These observations suggest that bloodflow to capillaries can be altered byHVPC, but is not critical to edema con-
trol. Another study by others also sug-
gests that edema is not affected bydimensions of arterioles. 14
ConclusionsClinicians have long used forms of
ES, HVPC in particular, to regulateedema. This practice has some theoreti-cal bases, but little objective evidence
72 Volume 28 * Number 1 * 1993

of efficacy. Anecdotal reports and un-supported claims of manufacturersseemingly have been cobbled togetherto form a pseudo rationale for using thismodality for this clinical problem. Be-cause current clinical protocols are notbased on sound empirical evidence,published protocols are of little value.Acute edema typically is treated withice, elevation, and compression; some-times ES is added to those interventions.But, to date, no evidence is availablethat indicates that ES enhances thetherapeutic effects of these othermodalities.
Recent controlled, blinded studies onnonhuman animal models provideevidence, perhaps for the first time, thatsome forms of ES are effective in curb-ing edema formation. Cathodal HVPCdelivered via immersion technique at120 pps and voltages 10% less thanthose needed to evoke visible musclecontraction significantly retards edemaformation if applied early after impactor hyperflexion injuries in frogs andrats. A single 30-minute treatment
olIm4/
checks edema for more than 4 hours,and a series of four, 30-minute treat-ments interspersed with hour rests curbsedema formation up to 24 hours postin-jury in frogs. HVPC administered atlevels sufficient to evoke low-levelmuscle activity (one pps) and LVPC at10% less than visible motor thresholdfail to curb edema formation. Polarityof stimulation seemingly is critical;cathodal stimulation produces a treat-ment effect, whereas anodal does not.Demonstration of treatment effects infrogs and rats suggests that themechanism(s) of edema formation ef-fected by HVPC are probably the samein a wide variety of vertebrates, includ-ing humans, and provide compelling ra-tionale for clinical trials.
AcknowledgementsWe thank Robert Hard, PhD, and
Barbara Evans for assistance withgraphics; Kenneth J. Ottenbacher, PhD,OTR, for statistical consultation; JamesR. Brown, for technical assistance; JohnNyquist, for illustrations; ChattanoogaCorporation and Ntron Inc. for com-plimentary loan of current generators.
References1. Alon G. High Voltage Galvaniic Stintiulation. Chat-
tanooga, Tenn: Chattanooga Corp; 1981:1-5.2. Alon G. Principles of electrical stimulation. In: Nel-
son RM, Currier DP, eds. Clinical Electrotherapy.2nd ed. Norwalk, Conn: Appleton & Lange;1991:35-103.
3. Alon G, De Domenico G. High Voltage Stimultion.AnIntegrated Approach to Clinical Electrotherapy.Chattanooga, Tenn: Chattanooga Corp: 1987:129-146.
4. Bettany JA, Fish DR, Mendel FC. High voltagepulsed direct current: effect on edema formationfollowing hyperflexion injury. Arch Phvs MedRehabil. 1990;71:677-681.
5. Bettany JA, Fish DR, Mendel FC. Influence ofcathodal high voltage pulsed current on acute edema.J Clin Electrophysiol. 1990;2:5-8.
6. BettanyJA, Fish DR, Mendel FC. Influence of highvoltage pulsed direct current on edema formationfollowing impact injury. Phys Ther. 1990;70:219-224.
7. Brown S. Ankle edema and galvanic muscle stimula-tion. PhysSportsmed. November 1981;9:37.
8. Cosgrove K, Alon G, Bell SF, et al. The electricaleffect of two commonly used clinical stimulators ontraumatic edema in rats. Phys Ther. 1992;72:227-233.
9. Crisler GR. Sprains and strains treated with theultrafaradic M-4 impulse generator. J Fla MedAssoc. 1953;1 1:32-34.
10. Cummings JP. Additional therapeutic uses ofelectricity. In: Gersh MR, ed. Electrotherapy inRehabilitation. Philadelphia, Pa: FA Davis Co;1992:328-342.
11. Fish DR, Mendel FC, Schultz AM, Gottstein YerkeLM. Effect of anodal high voltage pulsed current onedema formation in frog hind limbs. Phys Ther.1991;71:724-733.
12. Gieck JH. The athletic trainer and rehabilitation. In:Kuland DN, ed. The linjured Athlete. Philadelphia,Pa: JB Lippincott Co; 1982:177-205.
13. Gieck JH, Saliba EN. The athletic trainer andrehabilitation. In: Kuland DN, ed. The Injured Ath-lete. 2nd ed. Philadelphia, Pa: JB Lippincott Co;1988:165-240.
14. Grega GJ, Adamski SW, Dobbins DE. Physiologicaland pharmacological evidence of the regulation ofpermeability. Federation Proc. 1986;45:96- 100.
15. Griffin JW, Newsome LS, Stralka SW, Wright PE.Reduction of chronic post-traumatic hand edema: acomparison of high voltage pulsed current, intermit-tent pneumatic compression, and placebo treatments.Phys Ther. 1990;70:279-286.
16. Kames JL, Mendel FC, Fish DR. Effects of lowvoltage pulsed current on edema formation in froghind limbs following impact injury. Phys Tlier.1992;72:273-278.
17. Killian C, Malone T, Carroll B. High Frequency anidHigh Voltage Protocols. Minneapolis, Minn:Medtronic; 1984:1-6.
18. Lamboni P, Harris B. The use of ice, airsplints, andhigh voltage galvanic stimulation in effusion reduc-tion. Athletic Training. 1983;18:23.
19. Licht S. History of electrotherapy. In: Licht S, ed.Therapeutic Electricity and Ultraviolet Radiation.2nd ed. New Haven, Conn: Elizabeth Licht; 1967:1-70.
20. Mendel FC, Wylegala J, Fish DR. Influence of highvoltage pulsed current on edema formation followingimpact injury in rats. Phys Ther. 1992;72:668-673.
21. Michlovitz S, Smith W, Watkins M. Ice and highvoltage pulsed stimulation in treatment of acutelateral ankle sprains. J Orthop Sports Phys Ther.1988;9:301 -304.
22. Mohr TM, Akers TK, Landry RG. Effect of highvoltage stimulation on edema reduction in the rathind limb. Phys Ther. 1987;67: 1703-1707.
23. Newton RA. Theoretical physiological effects ofhigh voltage galvanic stimulation. Phys Ther.1981;61:706.
24. Newton RA. Electrotherapeutic Treatonenit. Select-itng Appropriate Wave Form Characteristics. Clif-ton, NJ: Preston; 1984:23-24.
25. Newton RA. High-voltage pulsed current. Theoreti-cal bases and clinical applications. In: Nelson RM,Currier DP, eds. Clinical Electrotherapy. 2nd ed.Norwalk, Conn: Appleton & Lange; 1991:201-220.
26. Newton RA, Karselis TC. Skin pH following highvoltage pulsed galvanic stimulation. Phys Ther.1983;63: 1593-1596.
27. Ralston DJ. High voltage galvanic stimulation. Canthere be a "state of the art"? Athletic Trainiing.1985;20:291-293.
28. Reed BV. Effect of high voltage pulsed electricalstimulation on microvascular permeability to plasmaproteins: a possible mechanism in minimizingedema. Phys Ther. 1988;68:491-495.
29. Ross CR, Segal D. High voltage galvanic stimula-tion-an aid to post-operative healing. CurrPodiatr.1981;30:19-25.
30. Santiesteban AJ, Eggart J, Vergamini G. ICT, coldcompression and contrast baths in subacute ankleinjuries. Newsletter Wisc Chapter Am Phys TherAssoc. 1984;14:7-8.
31. Snyder-Mackler L. Electrical stimulation for tissuerepair. In: Snyder-Mackler L, Robinson AJ, eds.Clinical Electrophysiology. Electrothercap andElectrophvsiologic Testing. Baltimore, Md: Wil-liams & Wilkins; 1989:229-244.
32. Taylor K, Fish DR, Mendel FC, Burton HW. Effectof a single 30-minute treatment of high voltagepulsed current on edema formation in frog hindlimbs. Phys Ther. 1992;72:63-68.
33. Taylor K, Fish DR, Mendel FC, Burton HW. Effectof electrically induced muscle contractions on post-traumatic edema formation in frog hind limbs. PhysTher. 1992;72: 127-132.
34. Voight ML. Reduction of post-traumatic ankleedema with high voltage pulsedgalvanic stimulation.Athletic Training. 1984;19:278-279,31 1.
74 Volume 28 * Number 1 * 1993
SURGICRUSPORTS TRPE REMOVER"odorless and nontoxic"
STR is Friendly to you,your potients, and Lhe
environmentEasy to use -- apply over tapeEconomical and rapid acting
* FDA Cleared
Used by: McConnell Sem., Therex PTand Fla. Ctr. Fitness & SM WorkshopsAvailable from Call 800-Elantec info line 444-2547Henry Schein 851-0400Apothecary Products 328-2742IDE Interstate 666-8100Vienna Therapy Prod. 703-938-8781
'4%