Embed Size (px)
Citation preview
Circulatory Disturbances 1: Introduction and Edema
Shannon Martinson, January 2016 http://people.upei.ca/smartinson/ VPM 152 General Pathology
INTRODUCTION – NORMAL CIRCULATORY SYSTEM
Distribution of fluid is carefully controlled (homeostasis)
Deviations from normal can have profound pathological effects
Normal function requires intact blood and lymph vessels
Endothelial cells are important!
Important concepts
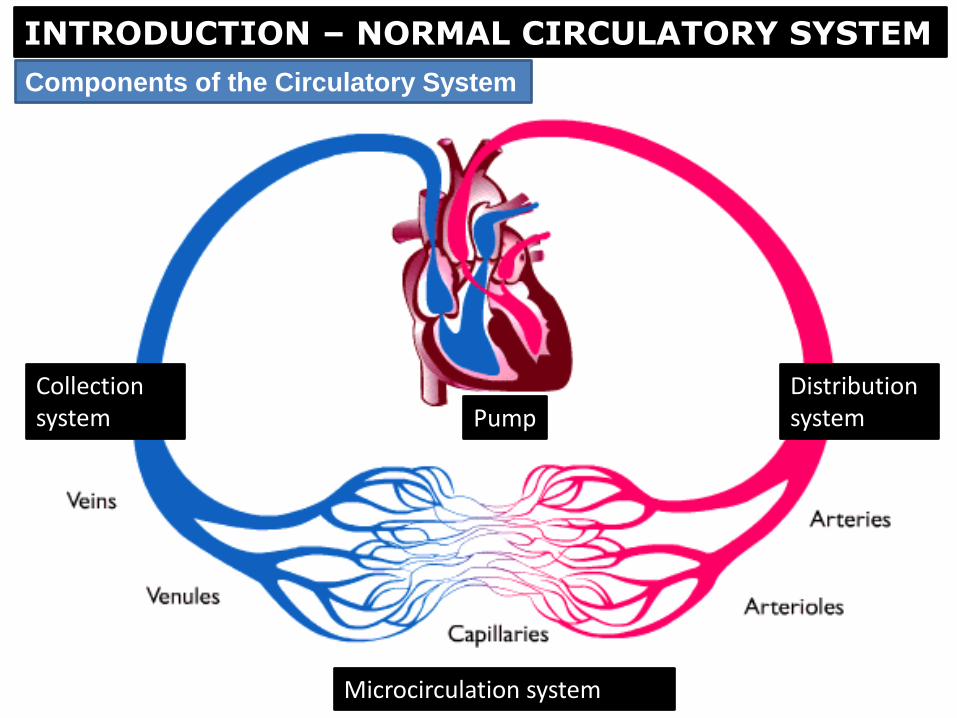
Components of the Circulatory System
INTRODUCTION – NORMAL CIRCULATORY SYSTEM
Pump Distribution system
Collection system
Microcirculation system
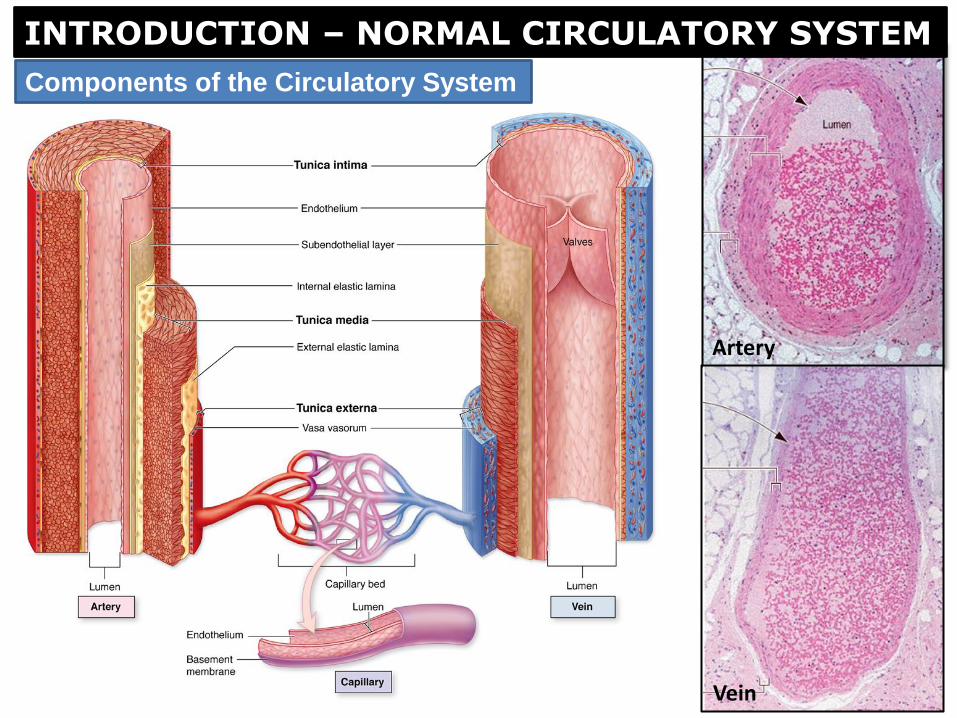
Artery
Vein
Components of the Circulatory System
INTRODUCTION – NORMAL CIRCULATORY SYSTEM
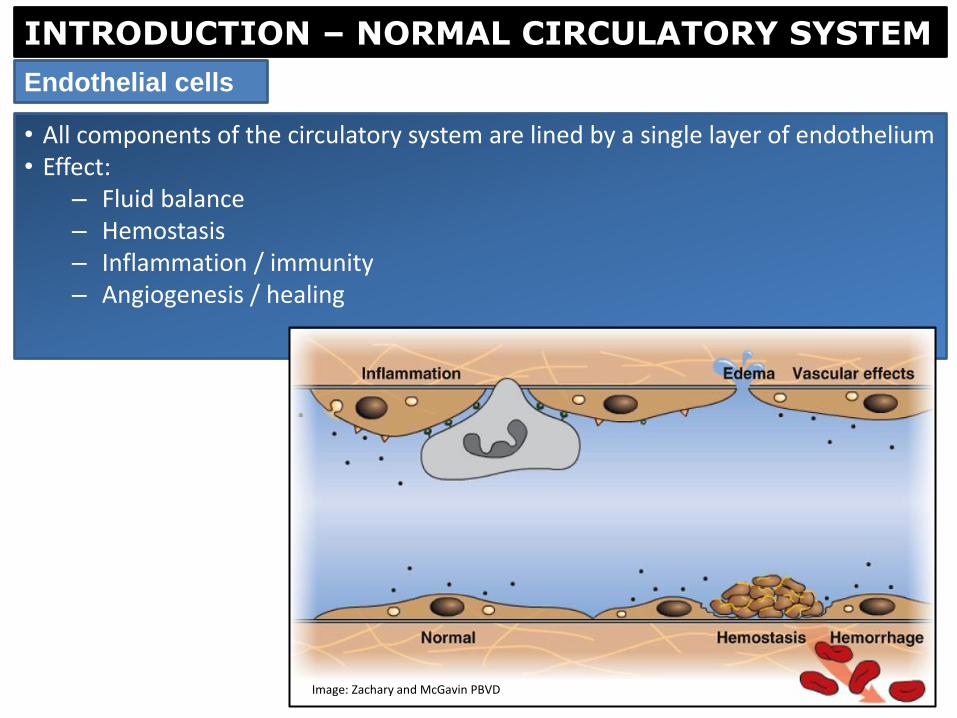
• All components of the circulatory system are lined by a single layer of endothelium • Effect:
– Fluid balance – Hemostasis – Inflammation / immunity – Angiogenesis / healing
INTRODUCTION – NORMAL CIRCULATORY SYSTEM
Endothelial cells
Image: Zachary and McGavin PBVD
INTRODUCTION – NORMAL CIRCULATORY SYSTEM
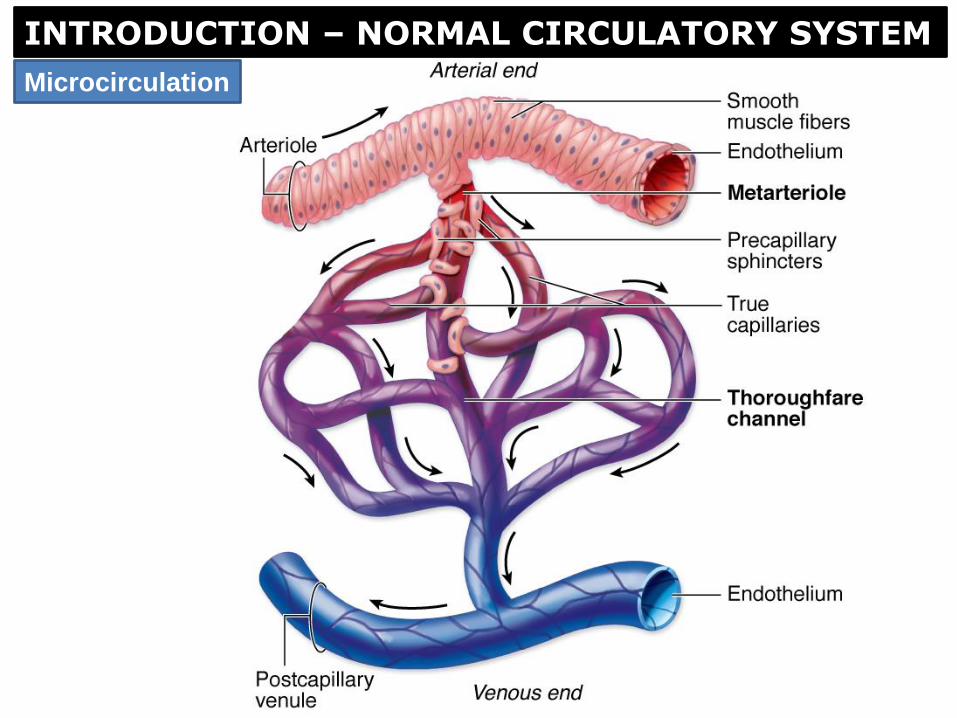
Microcirculation
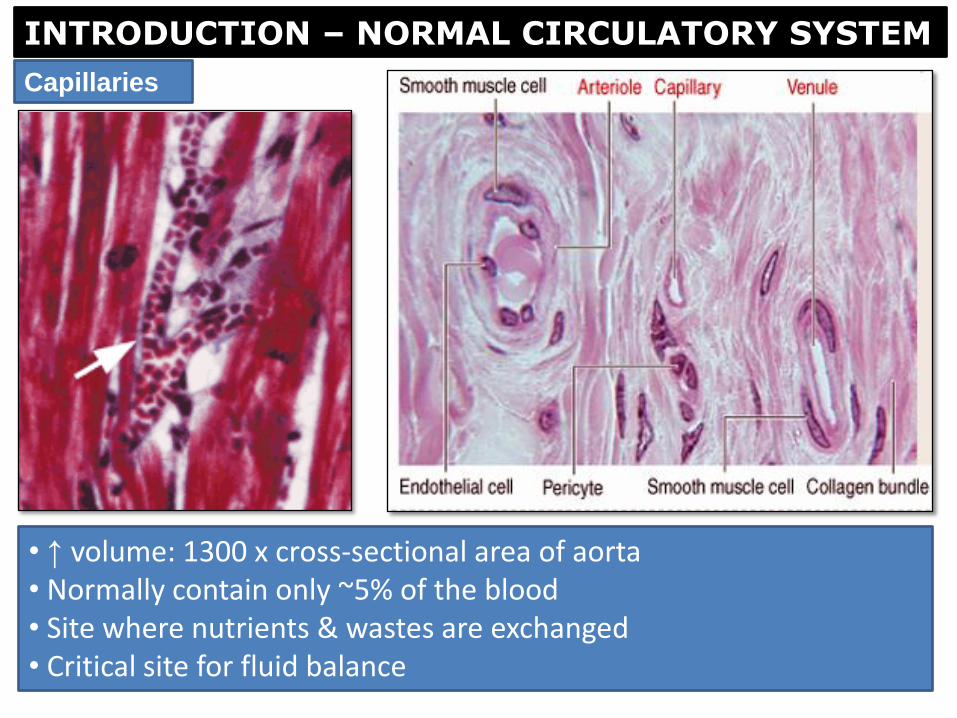
• ↑ volume: 1300 x cross-sectional area of aorta • Normally contain only ~5% of the blood • Site where nutrients & wastes are exchanged • Critical site for fluid balance
INTRODUCTION – NORMAL CIRCULATORY SYSTEM
Capillaries
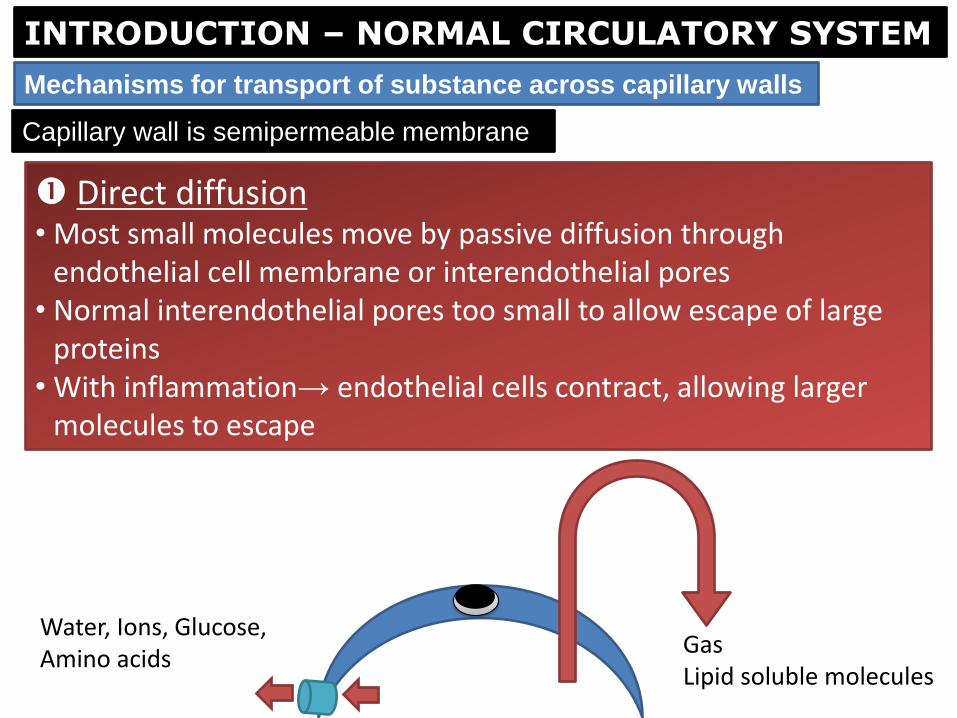
Capillary wall is semipermeable membrane
Direct diffusion • Most small molecules move by passive diffusion through
endothelial cell membrane or interendothelial pores • Normal interendothelial pores too small to allow escape of large
proteins • With inflammation→ endothelial cells contract, allowing larger
molecules to escape
INTRODUCTION – NORMAL CIRCULATORY SYSTEM
Mechanisms for transport of substance across capillary walls
Gas Lipid soluble molecules
Water, Ions, Glucose, Amino acids
Capillary wall is semipermeable membrane
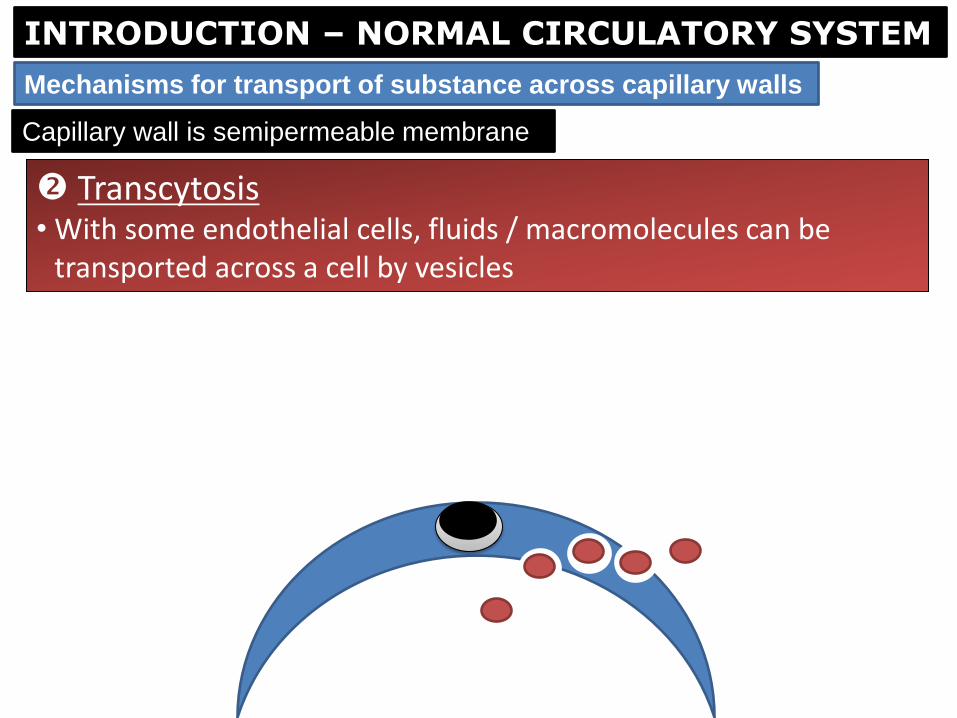
INTRODUCTION – NORMAL CIRCULATORY SYSTEM
Mechanisms for transport of substance across capillary walls
Transcytosis • With some endothelial cells, fluids / macromolecules can be
transported across a cell by vesicles

INTRODUCTION – NORMAL CIRCULATORY SYSTEM
Regional differences in capillary lining
Continuous capillary
• Muscle • Brain • Skin • Bone • Lung
Image: Zachary and McGavin PBVD
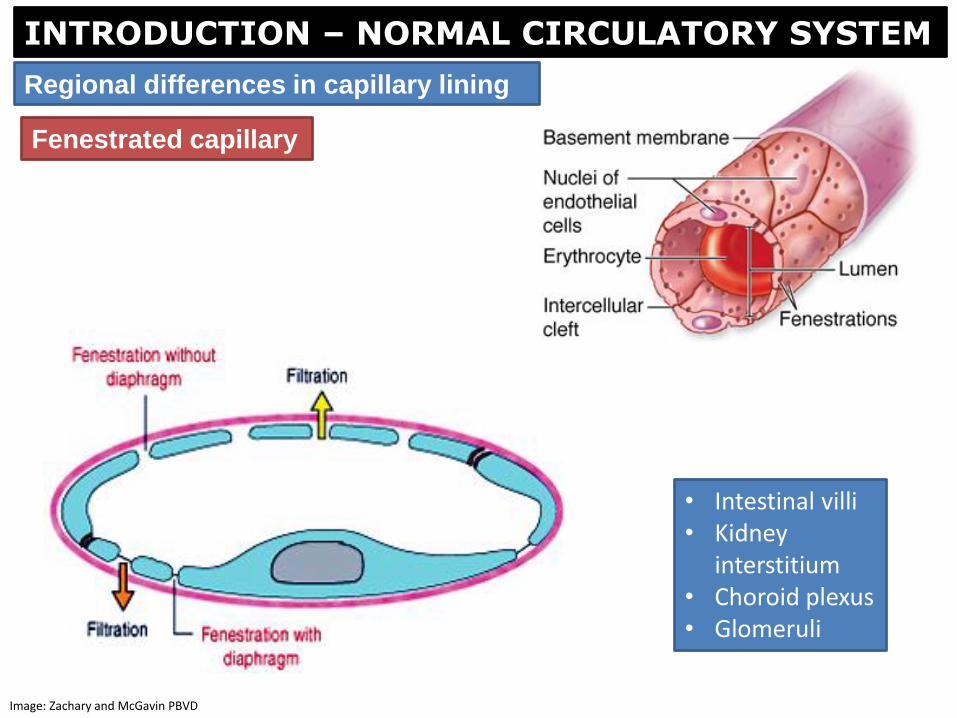
INTRODUCTION – NORMAL CIRCULATORY SYSTEM
Regional differences in capillary lining
Fenestrated capillary
• Intestinal villi • Kidney
interstitium • Choroid plexus • Glomeruli
Image: Zachary and McGavin PBVD
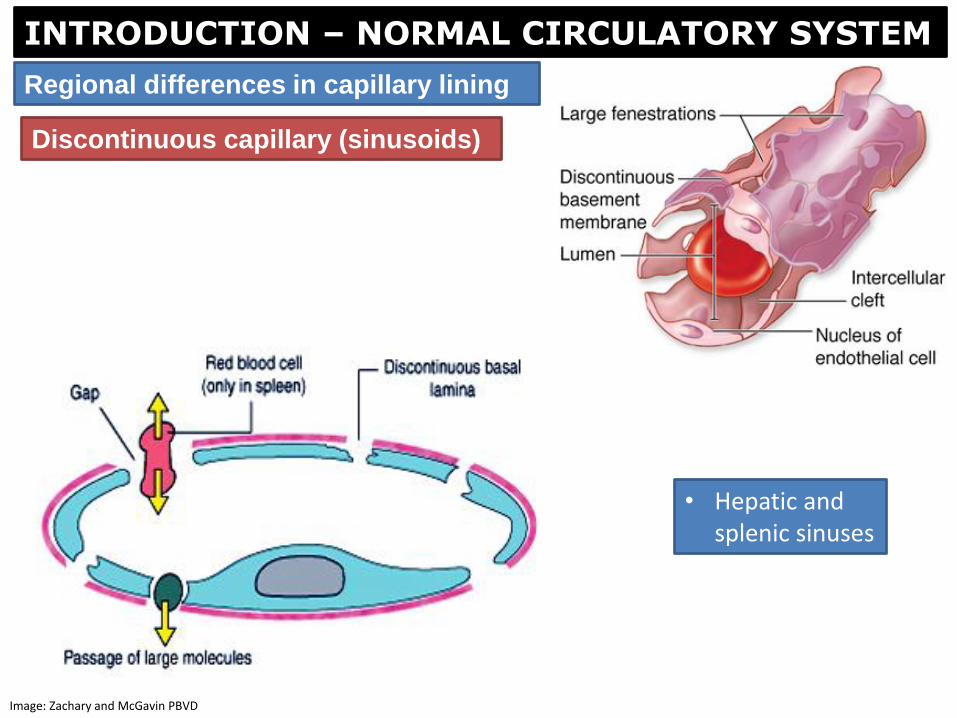
INTRODUCTION – NORMAL CIRCULATORY SYSTEM
Regional differences in capillary lining
Discontinuous capillary (sinusoids)
• Hepatic and splenic sinuses
Image: Zachary and McGavin PBVD
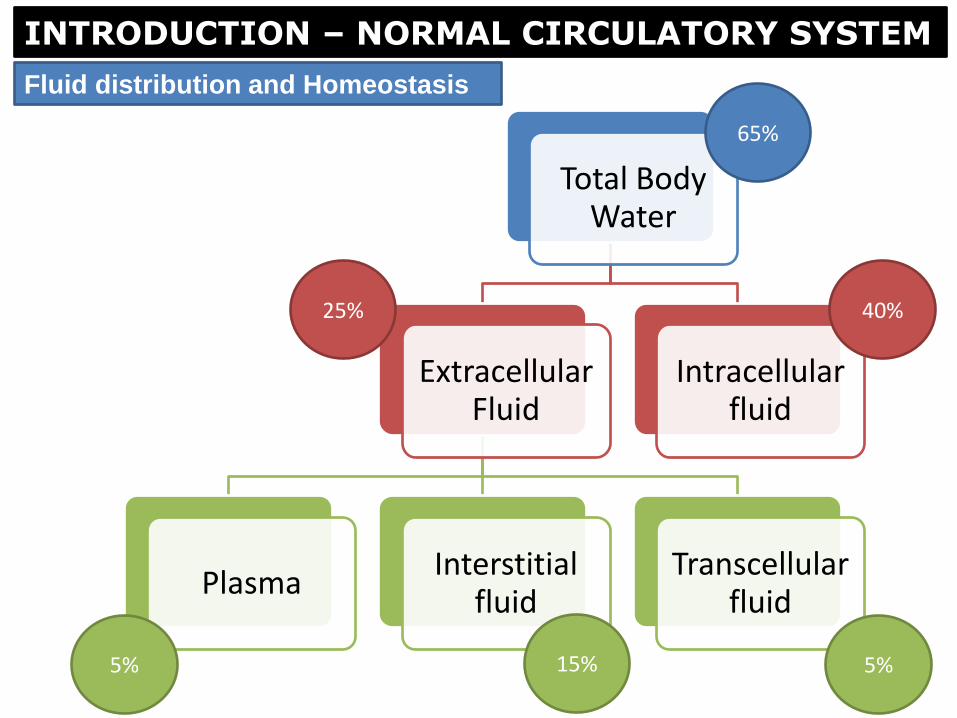
INTRODUCTION – NORMAL CIRCULATORY SYSTEM
Fluid distribution and Homeostasis
Total Body Water
Extracellular Fluid
Plasma Interstitial
fluid Transcellular
fluid
Intracellular fluid
5% 15% 5%
40% 25%
65%

INTRODUCTION – NORMAL CIRCULATORY SYSTEM
• is the space between microcirculation and the cells Interstitium
Function
• Binds cell/structural elements into discrete tissue and organs
• Medium through which metabolic products pass between circulation and cells
Structure
• Composed of extracellular matrix (ECM) and supporting cells
• ECM provides structural support and has adhesive absorptive properties
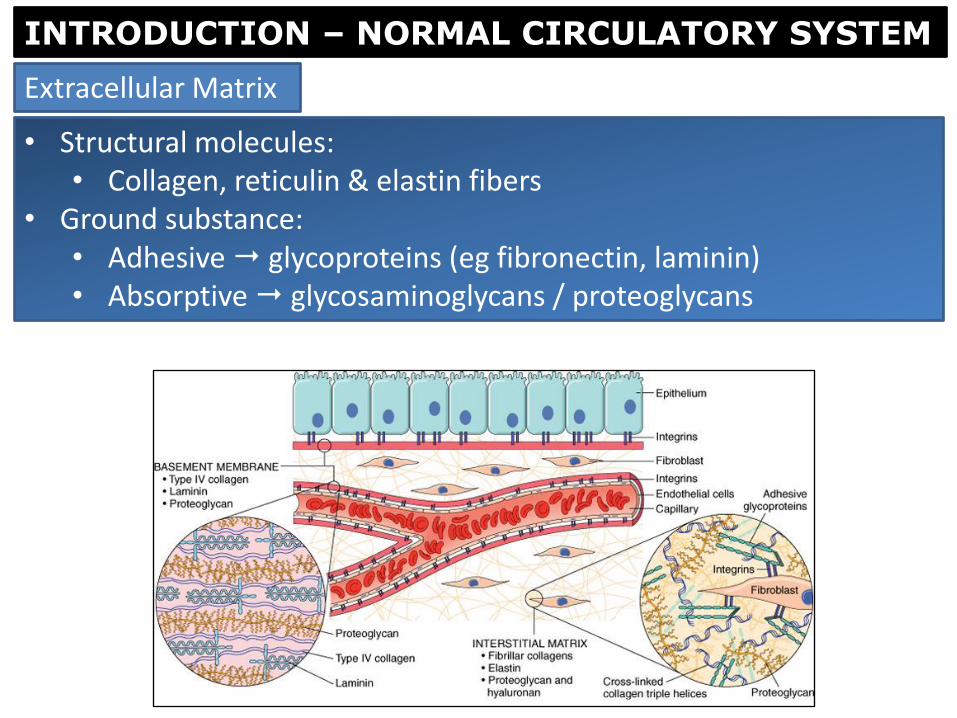
• Structural molecules: • Collagen, reticulin & elastin fibers
• Ground substance: • Adhesive glycoproteins (eg fibronectin, laminin) • Absorptive glycosaminoglycans / proteoglycans
Extracellular Matrix
INTRODUCTION – NORMAL CIRCULATORY SYSTEM
INTRODUCTION – NORMAL CIRCULATORY SYSTEM
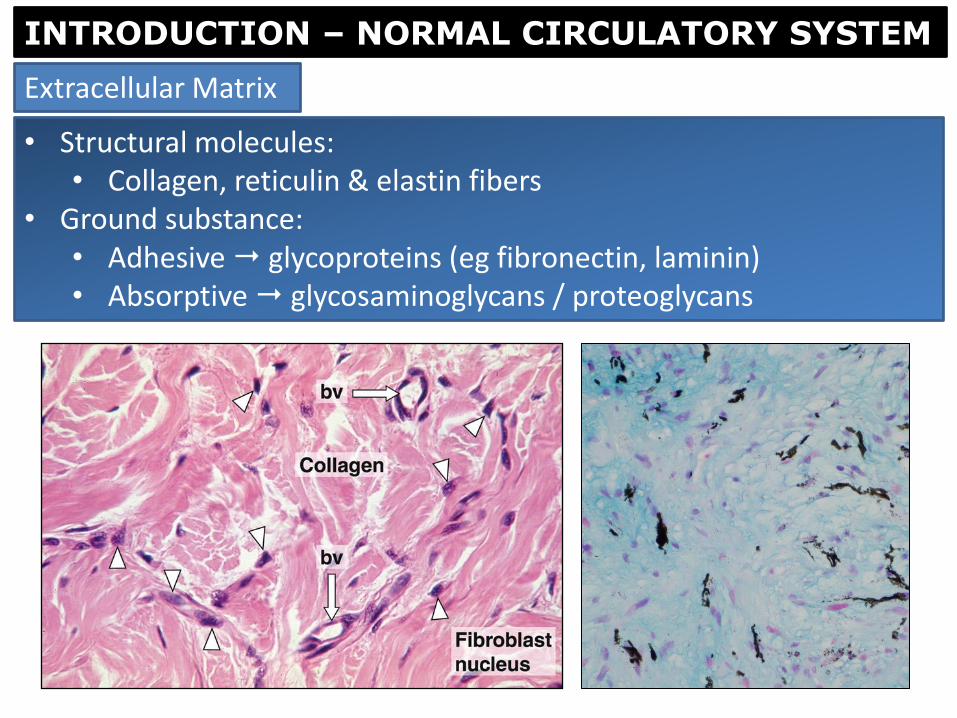
• Structural molecules: • Collagen, reticulin & elastin fibers
• Ground substance: • Adhesive glycoproteins (eg fibronectin, laminin) • Absorptive glycosaminoglycans / proteoglycans
Extracellular Matrix
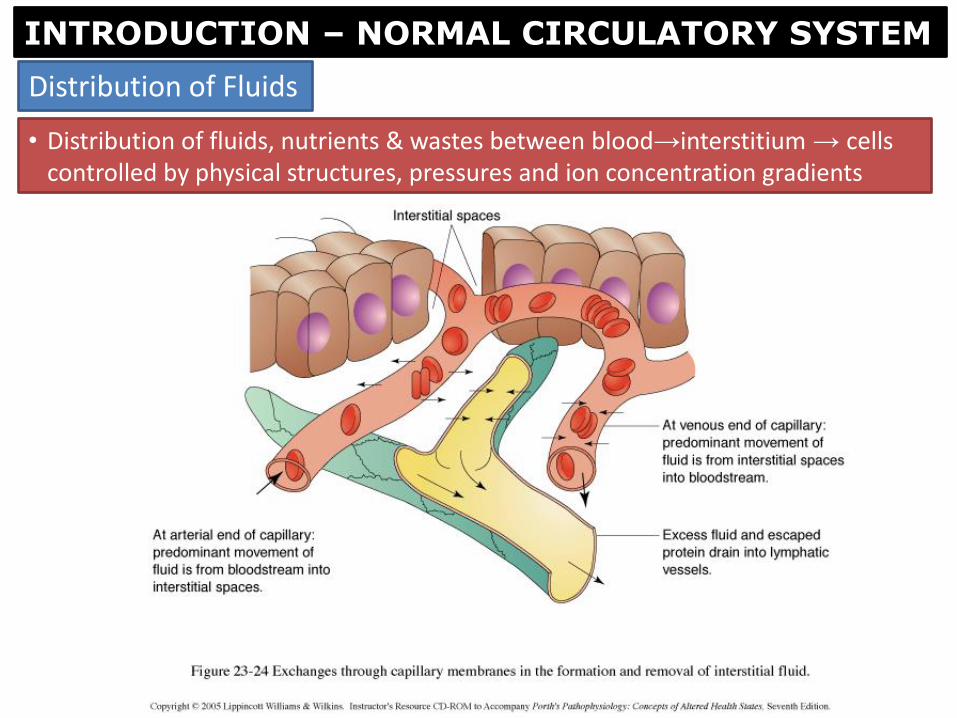
• Distribution of fluids, nutrients & wastes between blood→interstitium → cells controlled by physical structures, pressures and ion concentration gradients
INTRODUCTION – NORMAL CIRCULATORY SYSTEM
Distribution of Fluids
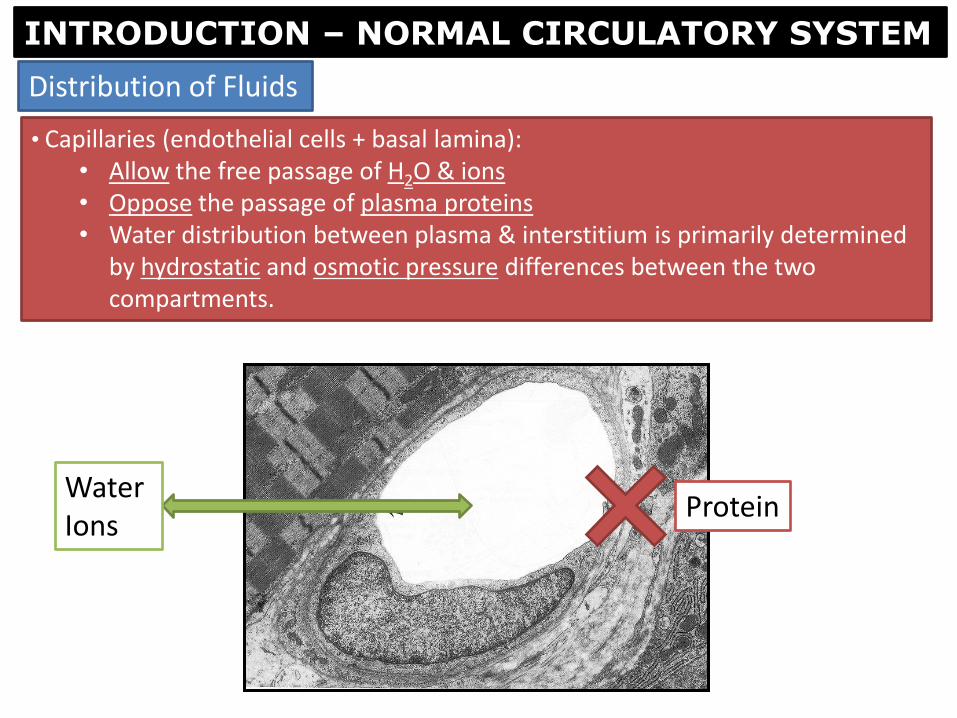
• Capillaries (endothelial cells + basal lamina): • Allow the free passage of H2O & ions • Oppose the passage of plasma proteins • Water distribution between plasma & interstitium is primarily determined
by hydrostatic and osmotic pressure differences between the two compartments.
INTRODUCTION – NORMAL CIRCULATORY SYSTEM
Distribution of Fluids
Water Ions
Protein

• Hydrostatic pressure in the vascular system + interstitial osmotic pressure moves fluid out of the vascular system.
INTRODUCTION – NORMAL CIRCULATORY SYSTEM
Distribution of Fluids
Plasma hydrostatic pressure
Tissue colloidal osmotic pressure
Starlings Equation
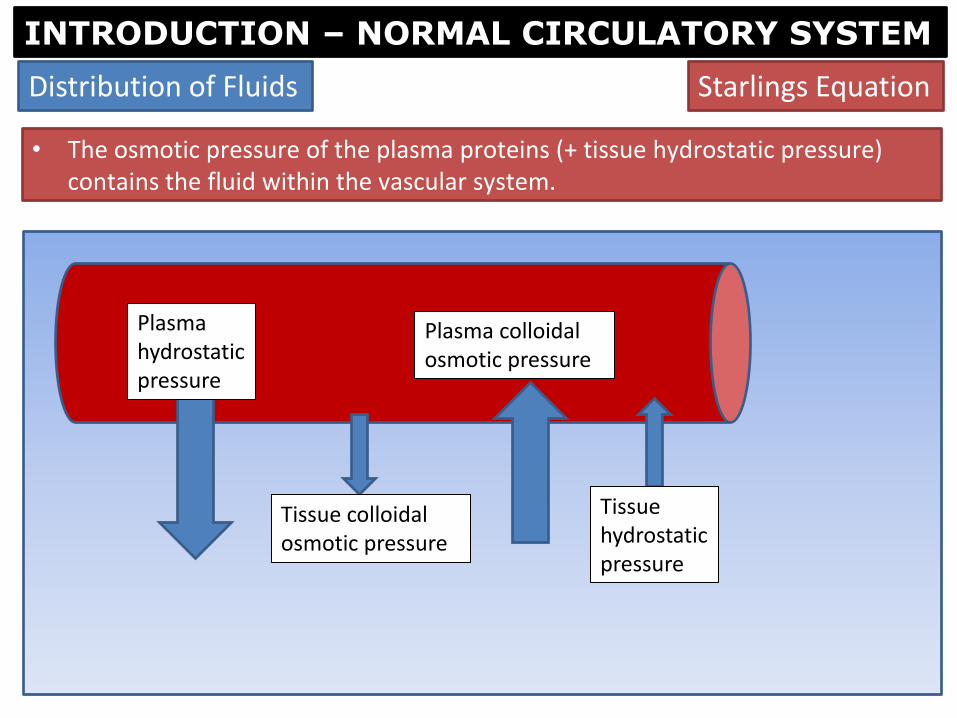
• The osmotic pressure of the plasma proteins (+ tissue hydrostatic pressure) contains the fluid within the vascular system.
INTRODUCTION – NORMAL CIRCULATORY SYSTEM
Distribution of Fluids
Plasma hydrostatic pressure
Tissue colloidal osmotic pressure
Plasma colloidal osmotic pressure
Tissue hydrostatic pressure
Starlings Equation
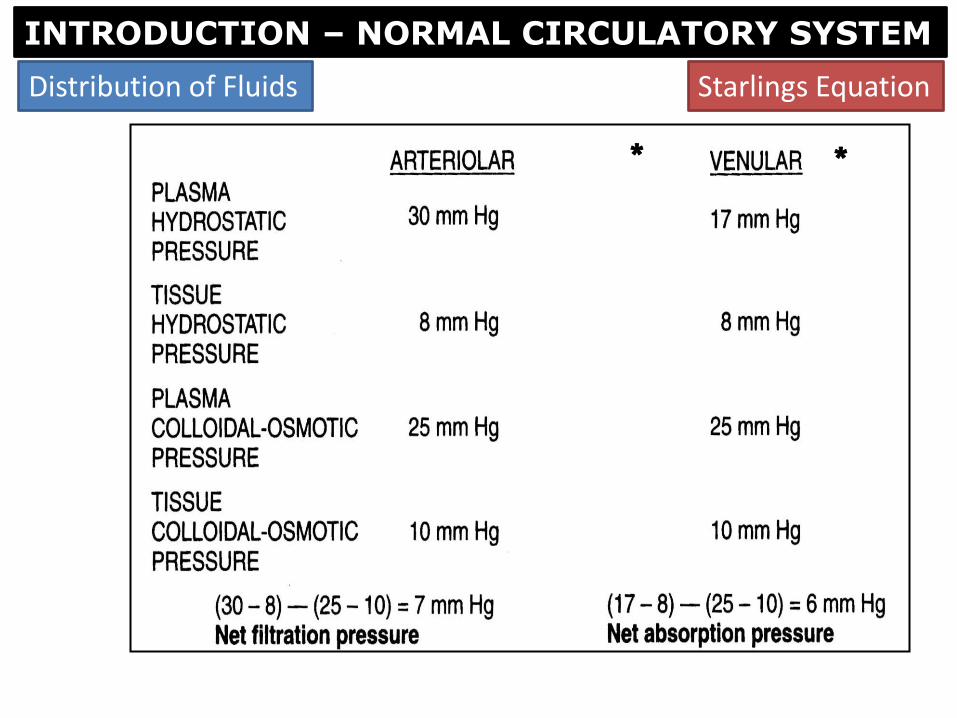
INTRODUCTION – NORMAL CIRCULATORY SYSTEM
Distribution of Fluids
* *
Starlings Equation

INTRODUCTION – NORMAL CIRCULATORY SYSTEM
Distribution of Fluids
Plasma hydrostatic pressure
Tissue colloidal osmotic pressure
Plasma colloidal osmotic pressure
Tissue hydrostatic pressure
Excess fluid Lymphatic drainage
Starlings Equation → Net movement of fluid out of the capillaries
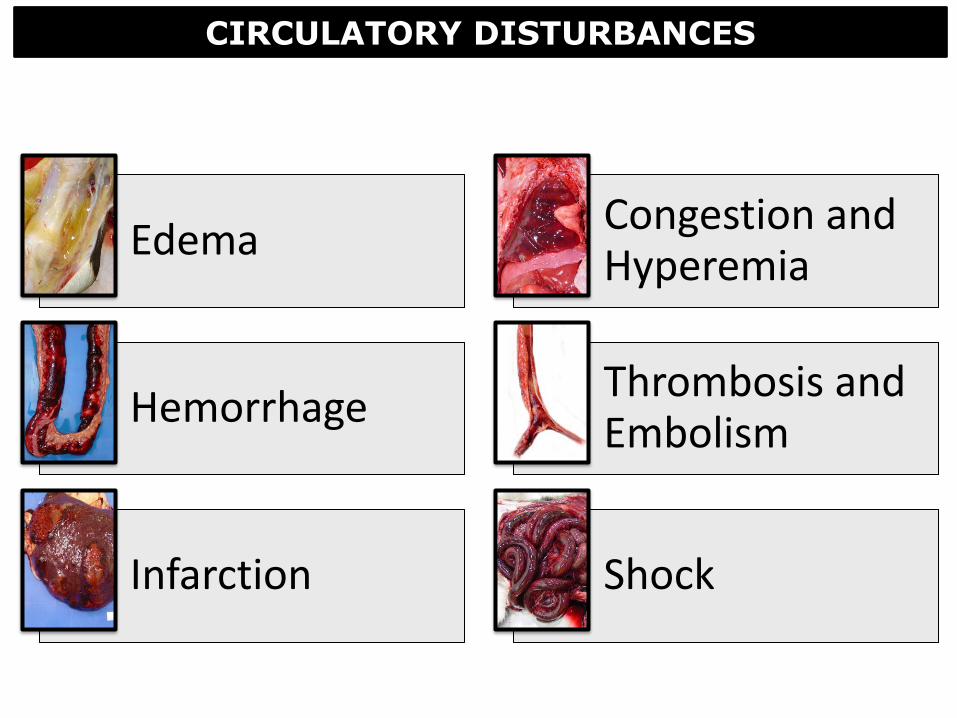
CIRCULATORY DISTURBANCES
Edema Congestion and Hyperemia
Hemorrhage Thrombosis and Embolism
Infarction Shock

EDEMA
Learning Objectives
• Define edema
• Recognize and be able to describe the gross and microscopic appearance of edema
• Know the four mechanisms by which edema develops
• Understand the different mechanisms under which generalized and localized edema develop
• Know the terminology for edema/fluid accumulation in different tissues / regions of the body
• Understand the clinical significance and pathogenesis of edema at important sites (eg lung and brain)
• Understand the clinical significance, gross appearance, and pathogenesis of dehydration

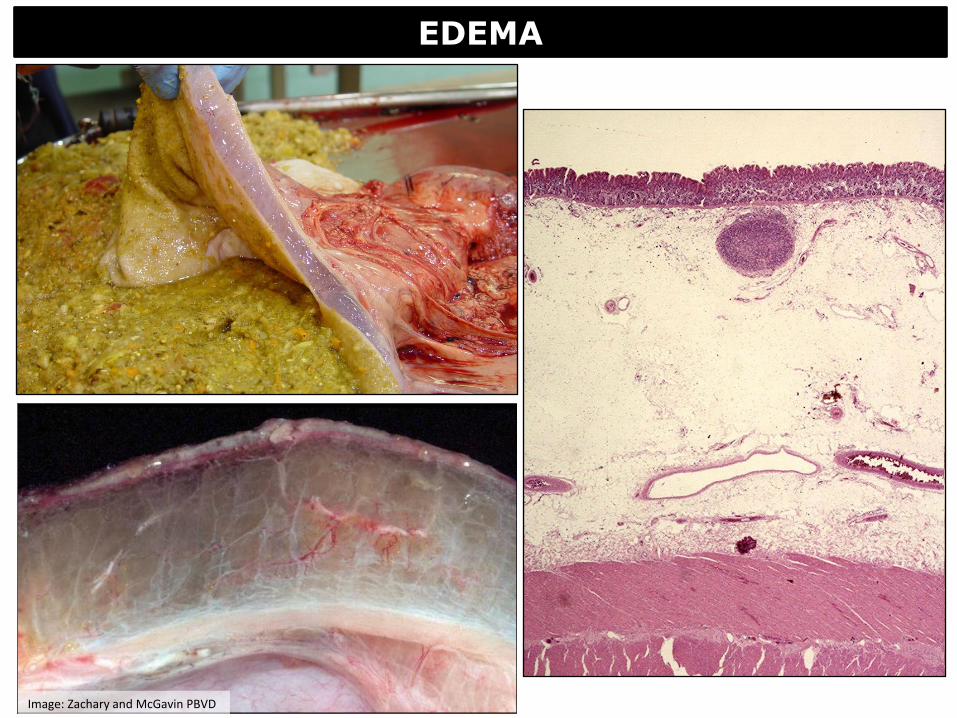
Gross Appearance of Edema • Organs wet (± gelatinous) and heavy
• Organs swollen and fluid may weep from cut surface
• May be yellow
EDEMA
• Abnormal (excess) accumulation of fluid in interstitial tissue spaces or body cavities
EDEMA
Image: Zachary and McGavin PBVD

Histologic Appearance of Edema
• Lightly staining eosinophilic fluid (if some protein content)
• Clear / no staining (if protein content low)
• Lymphatics usually dilated
EDEMA
Image: Zachary and McGavin PBVD
EDEMA
Image: Zachary and McGavin PBVD

hronic local passive hyperemia
1) ↑Intravascular hydrostatic pressure
2) ↓Plasma colloidal osmotic pressure
3) ↓ Lymphatic drainage
4) ↑Vascular permeability
Edema – 4 Pathophysiological Mechanisms of Development
EDEMA

Due to impaired venous blood flow
• Generalized edema– eg heart failure
• Localized edema – eg tight bandage causing local obstruction of venous return
NORMAL
1. Increased intravascular hydrostatic pressure
EDEMA - Pathophysiological Mechanisms of Development

Due to hypoproteinemia
• Proteins not absorbed
• Starvation
• Malabsorption
• Proteins not produced
• Liver disease
• Proteins lost**
• Kidney (glomerular) disease
• Intestinal damage
• Causes generalized edema
NORMAL
2. Decreased plasma colloidal osmotic pressure
EDEMA - Pathophysiological Mechanisms of Development
Plasma colloidal osmotic pressure is exerted mostly by plasma protein
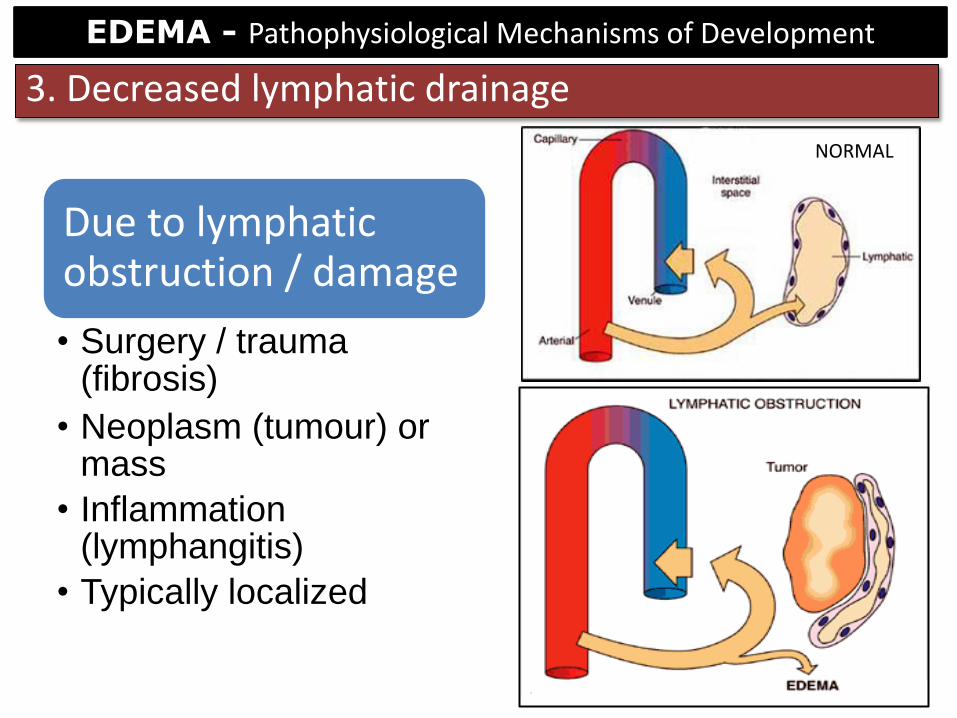
Due to lymphatic obstruction / damage
• Surgery / trauma (fibrosis)
• Neoplasm (tumour) or mass
• Inflammation (lymphangitis)
• Typically localized
NORMAL
3. Decreased lymphatic drainage
EDEMA - Pathophysiological Mechanisms of Development
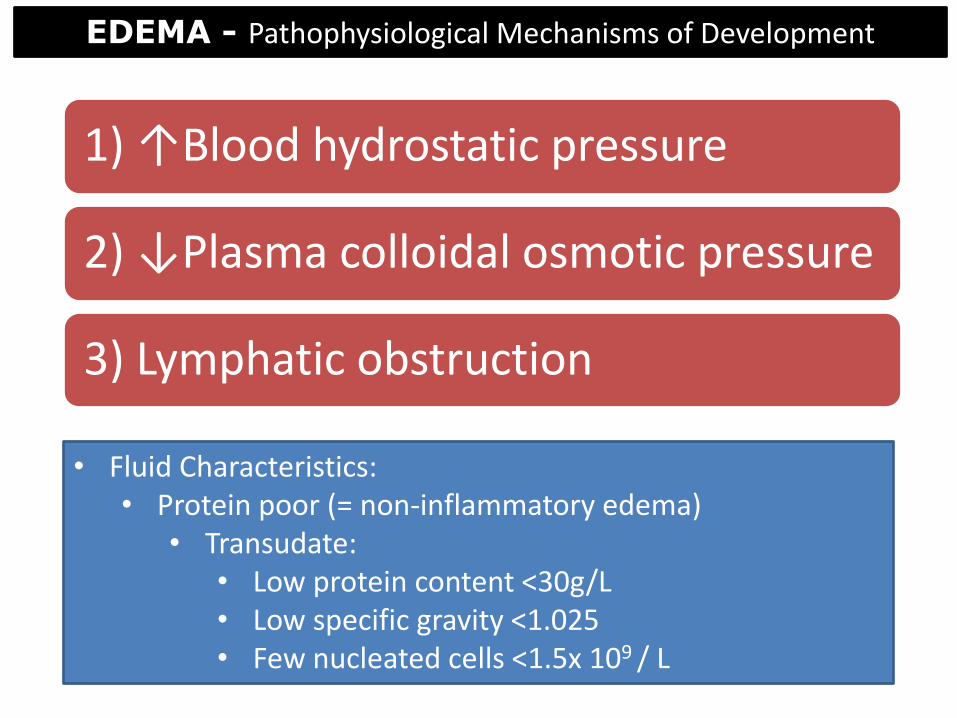
1) ↑Blood hydrostatic pressure
2) ↓Plasma colloidal osmotic pressure
3) Lymphatic obstruction
• Fluid Characteristics: • Protein poor (= non-inflammatory edema)
• Transudate: • Low protein content <30g/L • Low specific gravity <1.025 • Few nucleated cells <1.5x 109 / L
EDEMA - Pathophysiological Mechanisms of Development

Increased permeability
• Mostly due to inflammatory / immune reactions release of inflammatory mediators
• “inflammatory edema”
• Endothelium can be directly damaged by specific agents (eg viruses, toxins)
NORMAL
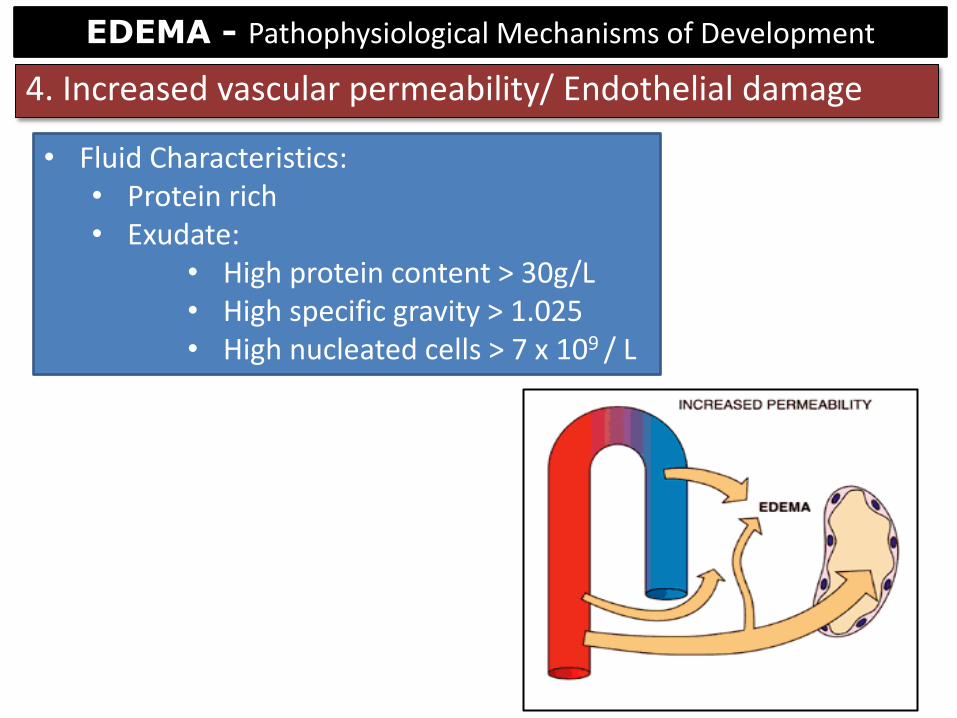
4. Increased vascular permeability/ Endothelial damage
EDEMA - Pathophysiological Mechanisms of Development
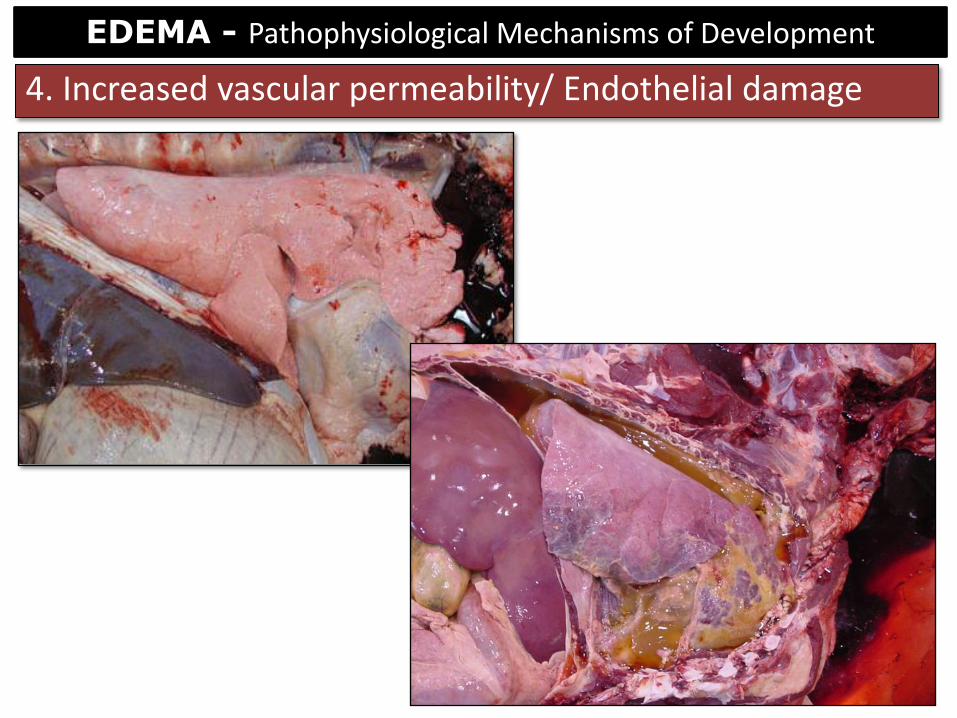
4. Increased vascular permeability/ Endothelial damage
EDEMA - Pathophysiological Mechanisms of Development
• Fluid Characteristics: • Protein rich • Exudate:
• High protein content > 30g/L • High specific gravity > 1.025 • High nucleated cells > 7 x 109 / L
4. Increased vascular permeability/ Endothelial damage
EDEMA - Pathophysiological Mechanisms of Development

1) ↑Blood hydrostatic pressure
• Generalized edema
• Localized edema
2) ↓Plasma colloidal osmotic pressure
• Generalized edema
3) ↓Lymphatic drainage
• Localized edema
4) ↑Vascular permeability
• Localized edema
LOCALIZED VS GENERALIZED EDEMA
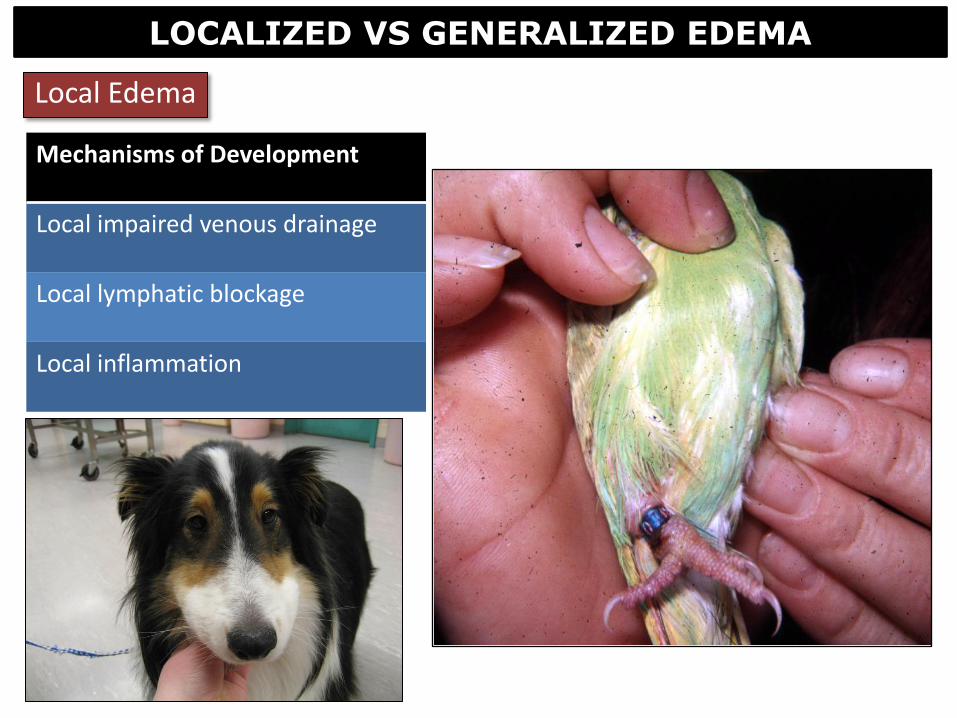
Mechanisms of Development
Local impaired venous drainage
Local lymphatic blockage
Local inflammation
Local Edema
LOCALIZED VS GENERALIZED EDEMA
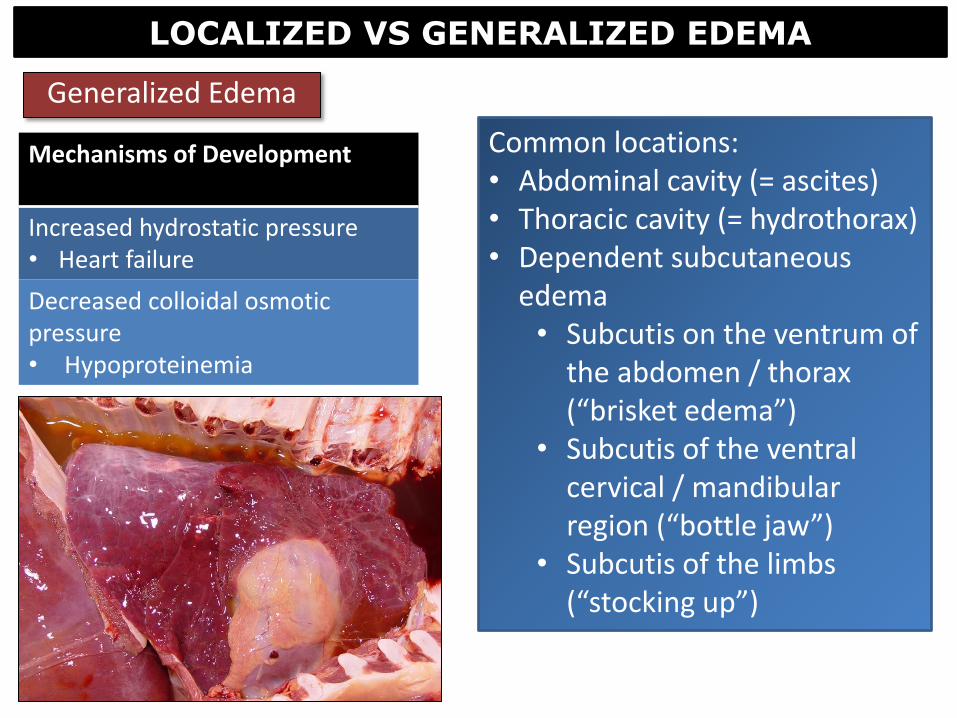
Generalized Edema
Common locations: • Abdominal cavity (= ascites) • Thoracic cavity (= hydrothorax) • Dependent subcutaneous
edema • Subcutis on the ventrum of
the abdomen / thorax (“brisket edema”)
• Subcutis of the ventral cervical / mandibular region (“bottle jaw”)
• Subcutis of the limbs (“stocking up”)
Mechanisms of Development
Increased hydrostatic pressure • Heart failure
Decreased colloidal osmotic pressure • Hypoproteinemia
LOCALIZED VS GENERALIZED EDEMA

Generalized Edema
LOCALIZED VS GENERALIZED EDEMA

TERMINOLOGY OF EDEMA
• When pressure is applied to an area of edema and a depression or dent results Pitting edema

• Severe and generalized edema with profound subcutaneous tissue swelling Anasarca
TERMINOLOGY OF EDEMA

• Non-inflammatory fluid (transudate) in the thoracic cavity Hydrothorax
TERMINOLOGY OF EDEMA
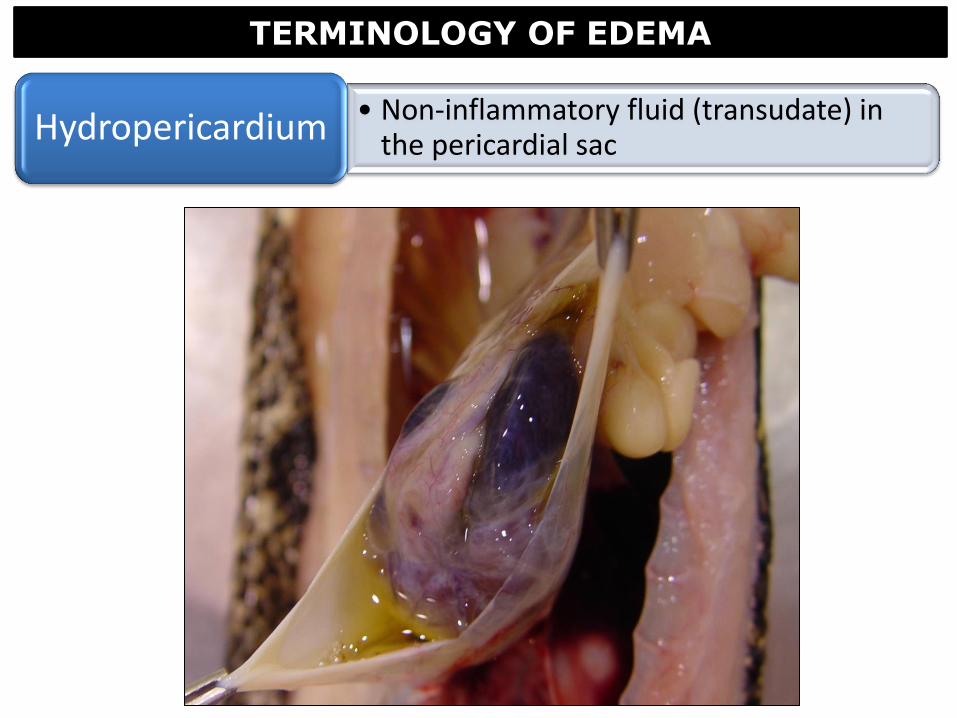
• Non-inflammatory fluid (transudate) in the pericardial sac Hydropericardium
TERMINOLOGY OF EDEMA
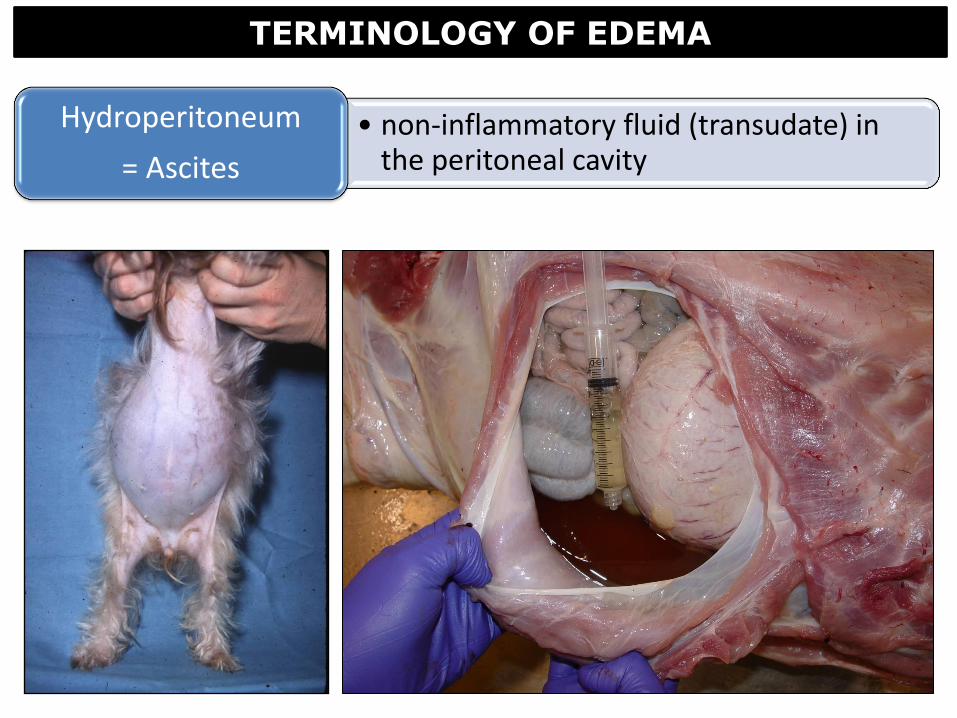
• non-inflammatory fluid (transudate) in the peritoneal cavity
Hydroperitoneum
= Ascites
TERMINOLOGY OF EDEMA

CLINICAL SIGNIFICANCE OF EDEMA
Dependent upon: 1. Extent: mild < moderate < marked / severe 2. Location: skin < lung < brain 3. Duration: acute vs chronic
• Increase in fibrous connective tissue after prolonged edema

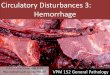
PULMONARY EDEMA
• Accumulation of fluid in interstitium and alveoli of the lungs
• Common cause of death in many disease processes
Pulmonary edema
Normal lung Pulmonary edema
PULMONARY EDEMA
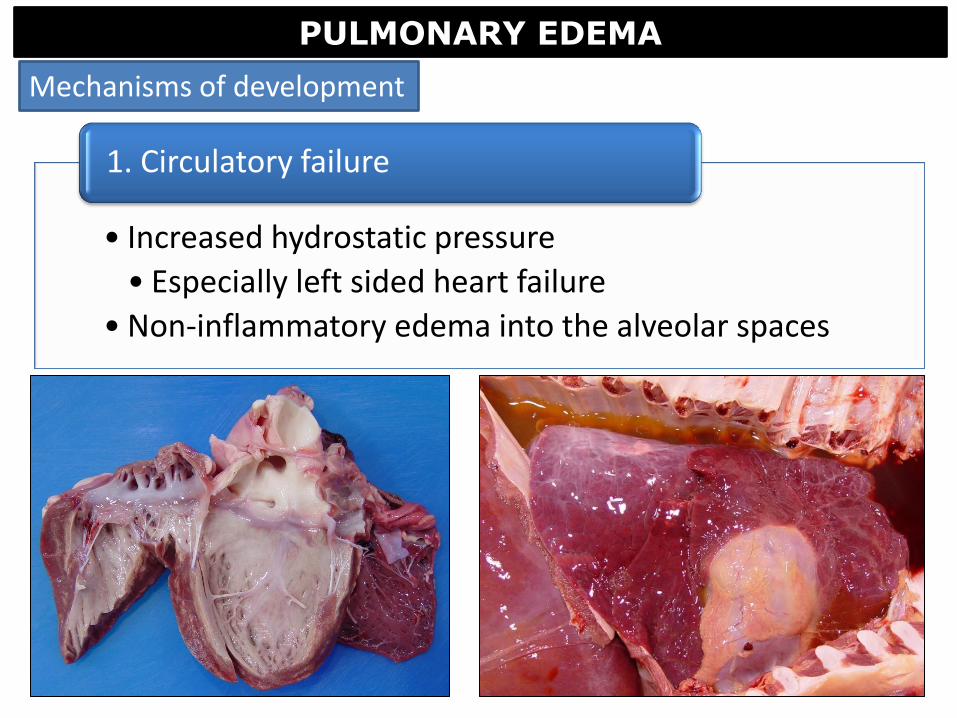
• Increased hydrostatic pressure
• Especially left sided heart failure
• Non-inflammatory edema into the alveolar spaces
1. Circulatory failure
Mechanisms of development
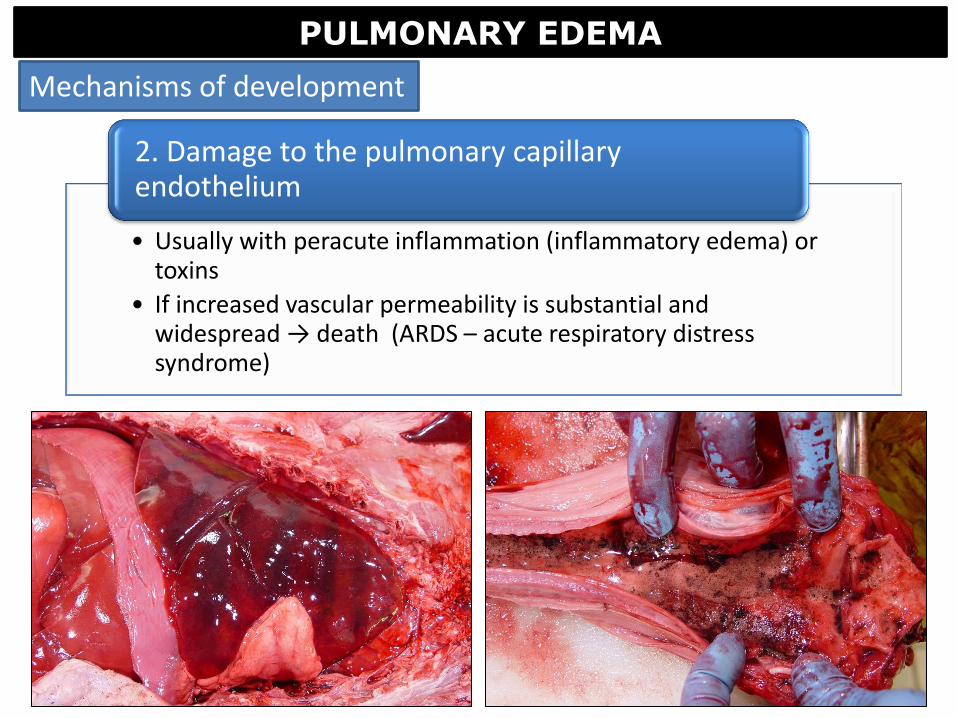
PULMONARY EDEMA
• Usually with peracute inflammation (inflammatory edema) or toxins
• If increased vascular permeability is substantial and widespread → death (ARDS – acute respiratory distress syndrome)
2. Damage to the pulmonary capillary endothelium
Mechanisms of development

1. • Fluid accumulates in the
interstitium
2. • Fluid moves through the basement
membranes into the alveoli
3. • Fluid drains via lymphatics
4. • +/- pleural fibrosis if chronic
Alveolar space
PULMONARY EDEMA
Dynamics of pulmonary edema
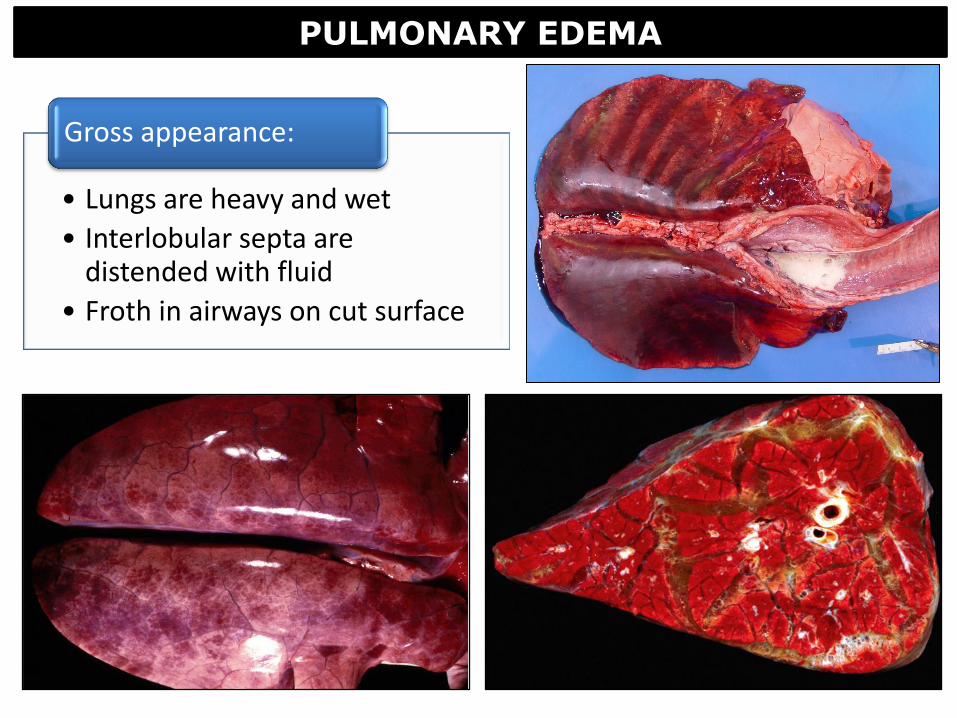
PULMONARY EDEMA
• Lungs are heavy and wet
• Interlobular septa are distended with fluid
• Froth in airways on cut surface
Gross appearance:
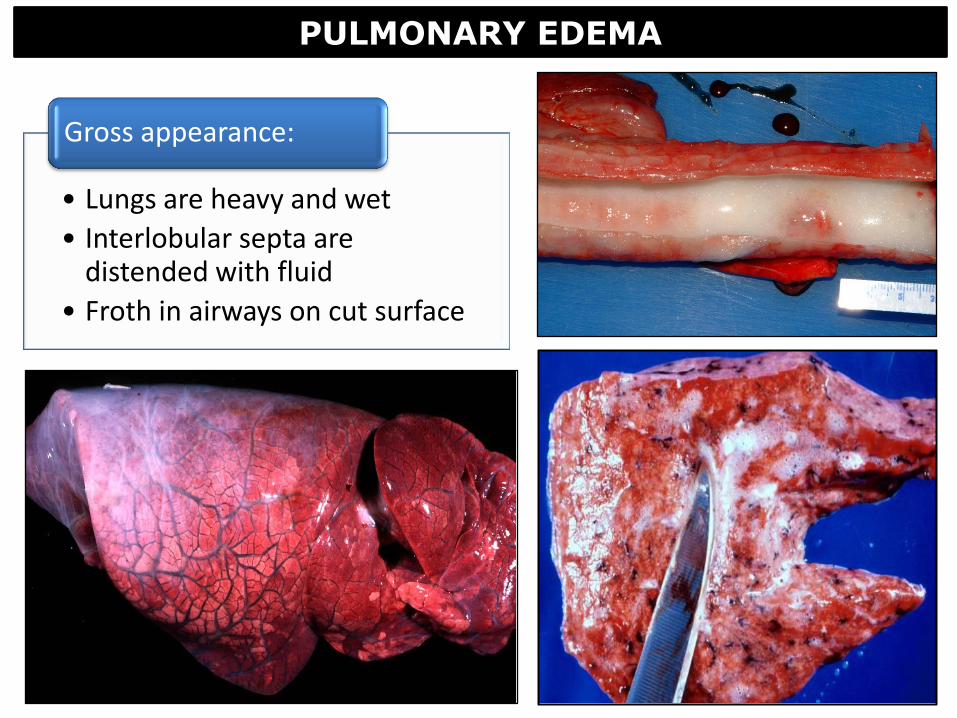
PULMONARY EDEMA
• Lungs are heavy and wet
• Interlobular septa are distended with fluid
• Froth in airways on cut surface
Gross appearance:

Normal lung
PULMONARY EDEMA
• Fluid in interstitium / alveolar spaces
• Dilated pleural / septal lymphatics
• Often pink
Histologic appearance:

• Chronicity → fibrosis of pleura & alveolar septa
• Most commonly seen with cardiac failure and accompanying pulmonary congestion
Chronic pulmonary edema
PULMONARY EDEMA
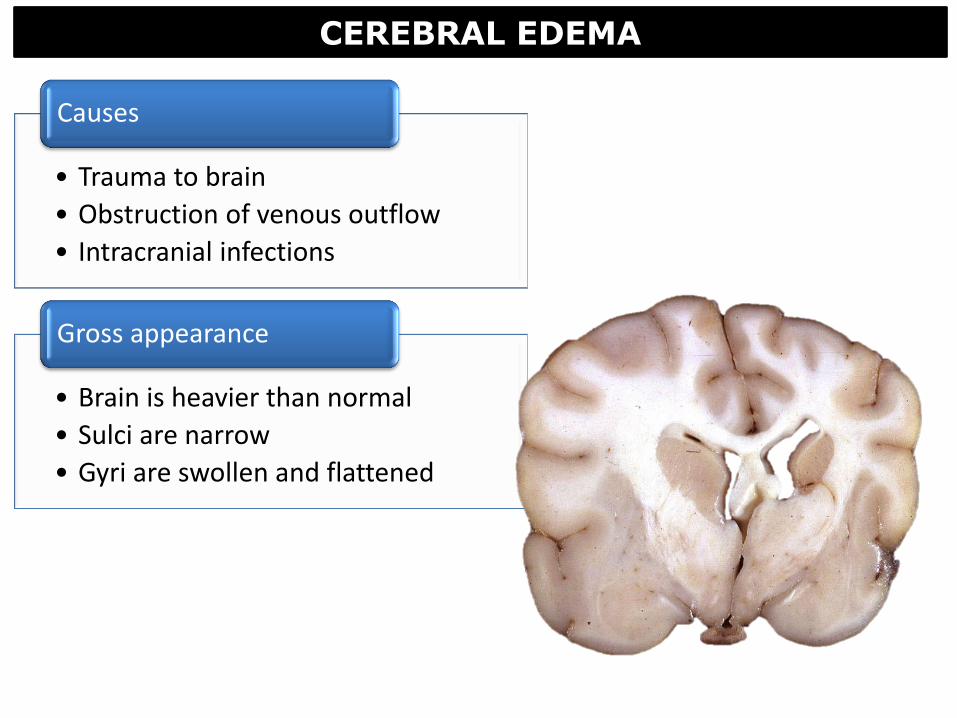
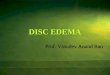
CEREBRAL EDEMA
• Trauma to brain
• Obstruction of venous outflow
• Intracranial infections
Causes
• Brain is heavier than normal
• Sulci are narrow
• Gyri are swollen and flattened
Gross appearance

• Herniation of the cerebellum through the foramen magnum
Cerebellar coning
CEREBRAL EDEMA

• Herniation of caudal cerebral cortex beneath the tentorium cerebelli
Cerebral herniation
Normal
Normal
CEREBRAL EDEMA
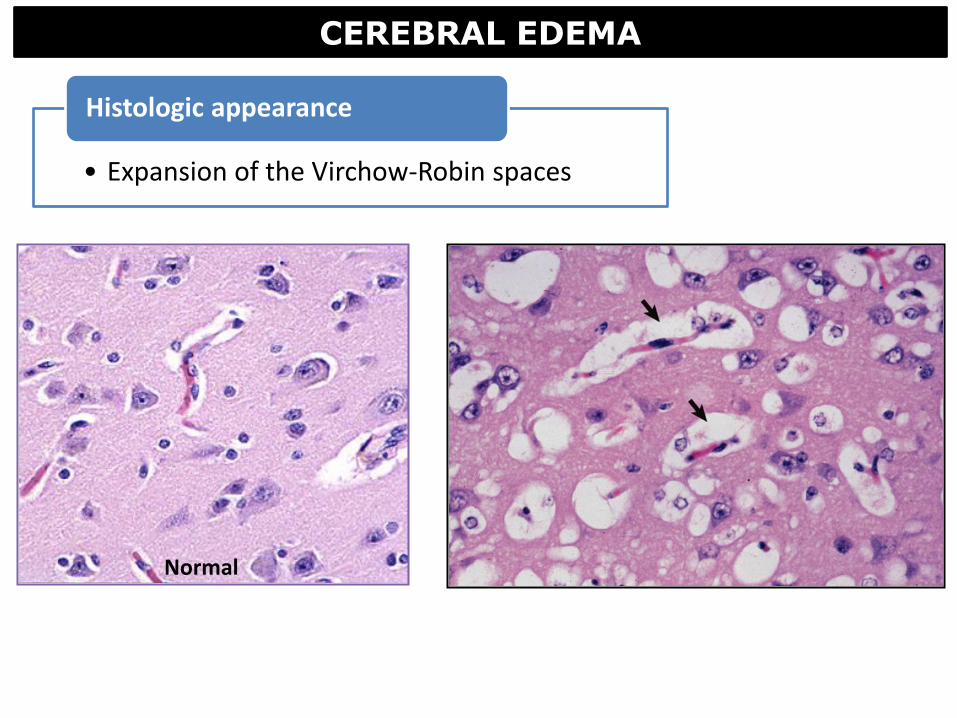
Normal
CEREBRAL EDEMA
• Expansion of the Virchow-Robin spaces
Histologic appearance
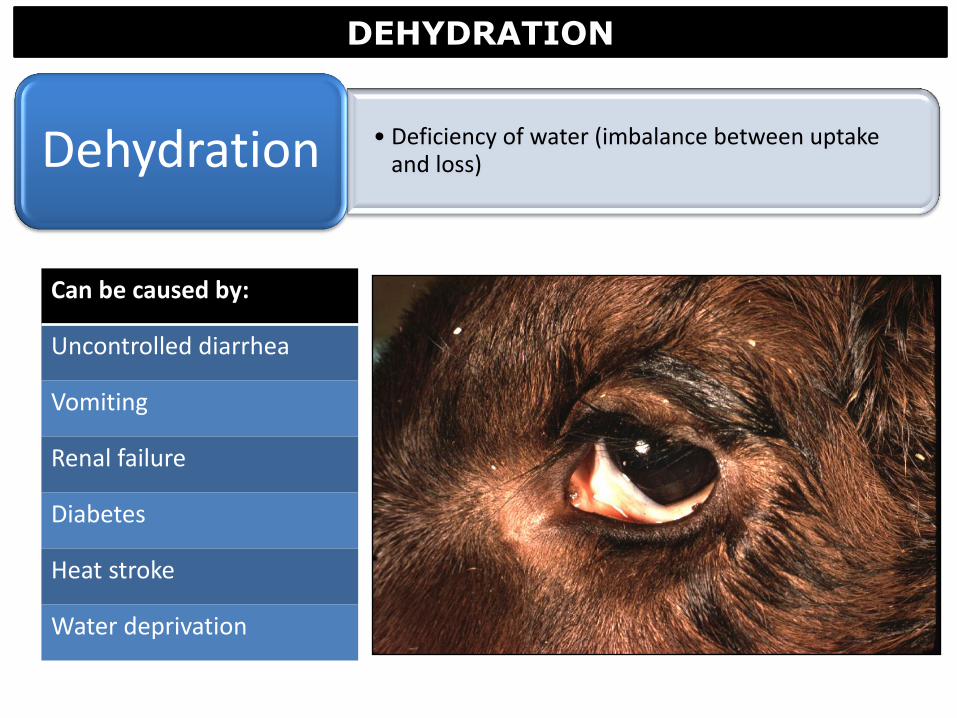
DEHYDRATION
• Deficiency of water (imbalance between uptake and loss) Dehydration
Can be caused by:
Uncontrolled diarrhea
Vomiting
Renal failure
Diabetes
Heat stroke
Water deprivation
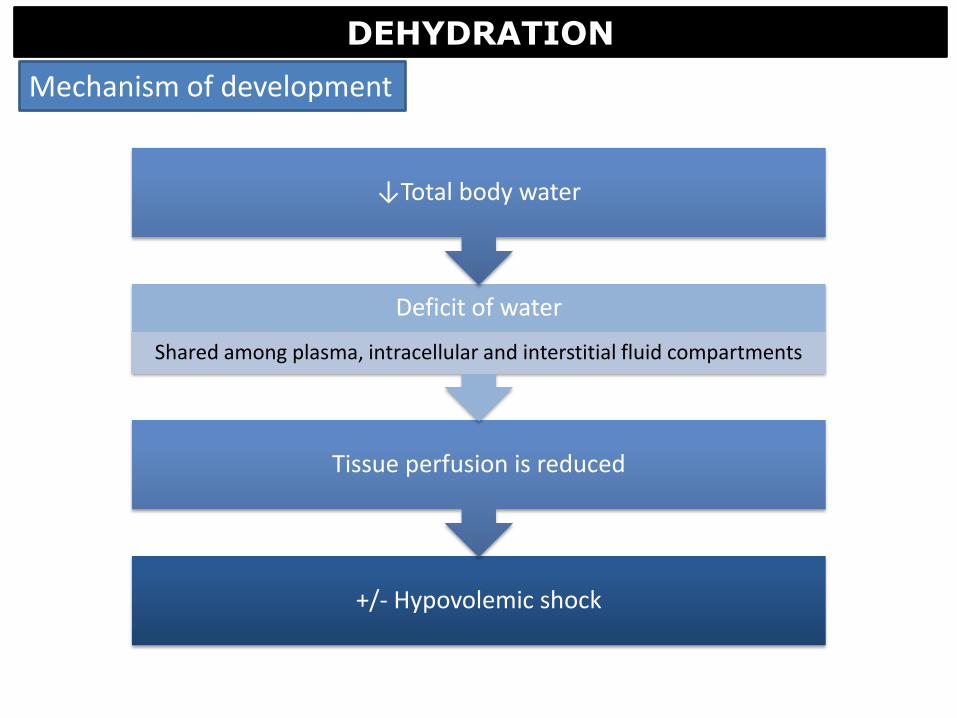
DEHYDRATION
+/- Hypovolemic shock
Tissue perfusion is reduced
Deficit of water
Shared among plasma, intracellular and interstitial fluid compartments
↓Total body water
Mechanism of development

• Skin pulled away from body “tents”
• Eyes are shrunken
• Mucous membranes and subcutaneous tissue are dry/sticky (at necropsy)
Gross Findings
DEHYDRATION

Questions?
A big thanks to Dr Hanna for providing me with material for these lectures!





![Uveitic macular edema: a stepladder treatment paradigm€¦ · of macular edema [1,3–4], this review will focus on uveitic macular edema specifically. Uveitic macular edema Macular](https://img.pdfslide.us/doc/110x75/5ed770e44d676a3f4a7efe51/uveitic-macular-edema-a-stepladder-treatment-paradigm-of-macular-edema-13a4.jpg)