Embed Size (px)
Citation preview

Weak alloantibody anti Jka missed on routine crossmatching: a case report illustrating the importance of “Type & Screen”

Case Report
Weak alloantibody anti Jka missed on routinecrossmatching: a case report illustrating theimportance of “Type & Screen”
Rajnath Makroo a,*, Aakanksha Bhatia b, Rosamma c
aDirector & Senior Consultant, Department of Transfusion Medicine, Indraprastha Apollo Hospitals,
Sarita Vihar, New Delhi, IndiabRegistrar, Department of Transfusion Medicine, Indraprastha Apollo Hospitals, Sarita Vihar, New Delhi, IndiacChief Technical Officer, Department of Transfusion Medicine, Indraprastha Apollo Hospitals, Sarita Vihar,
New Delhi, India
a r t i c l e i n f o
Article history:
Received 7 January 2014
Accepted 17 February 2014
Available online xxx
Keywords:
Clinically significant
Hemolytic transfusion reactions
Dosage effect
Group and screen policy
a b s t r a c t
THE KIDD system of blood groups was discovered in 1951 by Allen, Diamond and Niedziela.
The Kidd antibodies are clinically significant antibodies and a number of hemolytic
transfusions reactions resulting from them have been reported. Kidd antibodies are at
times difficult to detect. They exhibit distinct dosage effect. We present here one such case
of alloantibody anti Jka, that could have easily been missed, if the “Group and Screen
policy” routinely practiced at our hospital was not in place.
Copyright ª 2014, Indraprastha Medical Corporation Ltd. All rights reserved.
1. Introduction
Provision of safe blood for transfusion is the prime re-
sponsibility of every transfusion facility. This does not only
imply thorough testing for infectious markers, but also pro-
tection from hemolytic transfusion reactions resulting from
alloimmunization. Ever increasing efforts at improving blood
safety have led to incorporation of regular screening protocols
for detection of irregular immune antibodies at various
transfusion centers across the globe. The ultimate goal is to
identify the exact specificity of the antibody and provide the
corresponding antigen negative blood to the patients.
In most transfusion centers across India, detailed sero-
logical workup for such irregular antibodies is performed
either in cases where a blood group discrepancy is detected or
in cases of an incompatible/positive crossmatch. Since such a
practice is less time consuming and cost effective, it appears
to be the most practical approach, especially in the Indian
setting. However, there is a definite chance of missing certain
antibodies, some of which may be clinically significant. This
usually happens when the units that are cross matched lack
the particular antigen/s against which the patient has devel-
oped antibodies. Also at times the titer of the irregular anti-
body may be fairly low for causing a positive crossmatch.
Besides this there are several antigens and their
* Corresponding author.E-mail address: [email protected] (R. Makroo).
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.elsevier .com/locate/apme
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e3
Please cite this article in press as: Makroo R, et al., Weak alloantibody anti Jka missed on routine crossmatching: a case reportillustrating the importance of “Type & Screen”, Apollo Medicine (2014), http://dx.doi.org/10.1016/j.apme.2014.02.004
http://dx.doi.org/10.1016/j.apme.2014.02.0040976-0016/Copyright ª 2014, Indraprastha Medical Corporation Ltd. All rights reserved.

corresponding antibodies that display a “Dosage Effect”
resulting in misleading crossmatch findings. Examples of
such antibodies are anti-Jka, anti-Jkb, anti-Fya, anti-Fyb, anti-C,
anti-E, and anti-c.1,2
THE KIDD system of blood groups was discovered in 1951
by Allen, Diamond and Niedziela.3 The Kidd antibodies are
clinically significant antibodies, usually IgG in nature and a
number of hemolytic transfusion reactions (HTRs), espe-
cially delayed HTRs resulting from them have been re-
ported.4 Kidd antibodies are at times difficult to detect. They
may directly agglutinate antigen positive cells; however the
reactions are generally weak. They exhibit distinct dosage
effect. The anti Jka reacts more strongly with Jk (aþb�) cells
than with Jk (aþbþ), while some anti Jka can only be
detected using Jk (aþb�) screening cells and thus all
screening and identification cell panels must contain at
least one such cell.5
We present here one such case of alloantibody anti Jka, that
could have easily beenmissed, had we not had been following
the “Group and Screen policy” routinely at our hospital.
2. Case report
A 17-year-old girl with epilepsy was admitted to our hospital.
CT showed a subdural hematoma, which required evacuation.
As a routine protocol her “Group and Screen” sample was
received at the department of Transfusion Medicine. Her
blood groupwas B Positive, and antibody screening performed
using the Solid Phase RedCell Adherence technology (Capture,
Immucor Inc. Norcross, GA) was negative. Two units of
crossmatch compatible packed red cells were issued for the
patient.
Two weeks later another request for two units of packed
red cells was received for this patient. As it had been over 72
hours since the previous transfusion episode, as per the
transfusion policy followed at our center, antibody screening
was repeated. To our dismay this time the antibody screen
performed using a four cell panel of Capture (Immucor Inc.
Norcross, GA.) was positive in one of the cells. The results are
shown in Table 1.
In the meanwhile, at the crossmatching counter two
random B positive units had already been cross matched for
the patient, both of which were compatible. Resisting the
tendency to issue crossmatch compatible blood looking at the
low hemoglobin levels of the patient and rising pressure from
the clinical side, we went ahead with antibody identification.
Appropriate samples were requested to be sent to the blood
bank for testing. The serological investigations performed
were as follows:
Direct Coomb’s Test e Positive (1þ).
Auto control e Positive (most likely due to positive DAT).
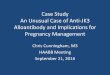
Antibody identificationwas run on the automated analyzer
Galileo (Immucor Inc. Norcross, GA). The results obtained are
shown in Table 2.
The reaction pattern clearly points towards an anti Jka.
Since the reaction strengths were only weak to 1þ, we
concluded that this patient had a weak alloantibody anti Jka.
Extended antigen typing of the patient could not be performed
since she was recently transfused.
Table
1e
Antibodysc
reenin
gch
art
e4ce
llpanel(Im
muco
rIn
c.Norcro
ss,GA).
Rh-H
rKell
Duffy
Kidd
Lewis
PMNSs
Luth
-eren
Xg
DC
cE
eF
VCw
KKpa
Kpb
Jsa
Jsb
Fya
Fyb
Jka
Jkb
Lea
Leb
P1
MN
Ss
Lua
Lub
Xga
1þ
þ0
0þ
00
þþ
þ0
þ0
þþ
þþ
þþ
0þ
þþ
0þ
0þ
01þ
2þ
0þ
þ0
00
00
þþ
þ0
þþ
00
þ0
þ0
þþ
00
0þ
þ0
30
0þ
0þ
þ0
00
þ0
þ0
þþ
0þ
00
þþ
þ0
þþ
0þ
01þ
40
0þ
0þ
þ0
00
þ0
þ0
þ0
þ0
þ0
þþ
0þ
0þ
0þ
þ0
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e32
Please cite this article in press as: Makroo R, et al., Weak alloantibody anti Jka missed on routine crossmatching: a case reportillustrating the importance of “Type & Screen”, Apollo Medicine (2014), http://dx.doi.org/10.1016/j.apme.2014.02.004
Further, this case clearly exemplifies the dosage effect
shown by this antibody. In the cells where the Jka antigen is
present in a homozygous state (double dose), the reaction
strength is higher, while in the cells where the antigen is
present in heterozygous state (single dose), the reaction is
weak.
With these results in hand, we went back to the units that
had been crossmatched for the patient and typed them for the
Kidd antigens. The results of the antigen typing are shown in
Table 3.
The first unit was typed as Jka�Jkbþ and was thus
compatible. It was the second unit that was Jka þ Jkb þ but still
compatible that raised a question on issuing blood merely
based on crossmatch compatibilities. In the second unit the
Jka antigen was in heterozygous state and hence the results of
crossmatch were misleading.
3. Conclusion
The initial negative antibody screen in this case suggests
either absence of alloantibodies or the presence of very
weak existing alloantibodies before transfusion. The
detection of anti-Jka in post transfusion sample indicates
immunization due to transfused units. Had we relied on
crossmatch alone we could have transfused antigen positive
blood to this alloimmunized young lady, thereby adding fuel
to the fire. This case clearly illustrates the need of the “Type
and Screen” policy being incorporated in routine trans-
fusion practice.
Conflicts of interest
All authors have none to declare.
r e f e r e n c e s
1. Makroo RN. Practice of Safe Blood Transfusion: Compendium ofTransfusion Medicine. 2nd ed. New Delhi, India: KongPoshPublications Pvt. Ltd.; 2009.
2. Reid ME, Lomas-Francis C. The Blood Group Antigen Facts Book.2nd ed. New York: Elsevier Academic Press; 2004.
3. Allen F, Diamond L, Niedziela B. A new blood group antigen.Nature. 1951;167:482.
4. Pineda AA, Vamvakes EC, Gorden LD, Winters JL, Moore SB.Trends in the incidence of delayed haemolytic and delayedserologic transfusion reactions. Transfusion.1999;39:1097e1103.
5. Daniels G. Human Blood Groups. 2nd ed. Blackwell Science Ltd;2002.
Table
2e
AntibodyIdentifica
tionch
art-14ce
llpanel(Im
muco
rIn
c.Norcro
ss,GA).
Rh-h
rKell
Duffy
Kidd
Lewis
PMNSs
Luth
-eren
Xg
DC
cE
ef
VCw
Kk
Kpa
Kpb
Jsa
Jsb
Fya
Fyb
Jka
Jkb
Lea
Leb
P1
MN
Ss
Lua
Lub
Xga
1þ
þ0
þþ
00
00
þ0
þ0
þþ
þþ
00
þþ
0þ
0þ
0þ
01þ
2þ
þ0
0þ
00
þ0
þ0
þ0
þþ
00
þ0
þþ
0þ
0þ
0þ
þ0
3þ
0þ
þ0
00
0þ
þ0
þ0
þþ
þ0
þ0
þþ
þ0
0þ
0þ
þ0
4þ
0þ
0þ
þþ
00
þ0
þ0
þ0
þþ
00
þþ
þþ
00
0þ
01þ
50
þþ
0þ
þ0
00
þ0
þþ
00
þþ
þ0
þ0
þþ
þþ
0þ
0w
60
0þ
þþ
þ0
00
þ0
þ0
þþ
00
þ0
þþ
þþ
0þ
0þ
þ0
70
0þ
0þ
þ0
00
þ0
þ0
þ0
þþ
þ0
0þ
þþ
0þ
0þ
þw
80
0þ
0þ
þ0
0þ
þ0
þ0
þ0
þþ
þ0
þ0
0þ
0þ
þþ
0w
90
0þ
0þ
þ0
00
þ0
þ0
þþ
00
þþ
0þ
þþ
0þ
0þ
00
10
00
þ0
þþ
00
0þ
0þ
0þ
00
þ0
þ0
þþ
þ0
þ0
þþ
1þ
11
00
þ0
þþ
00
0þ
0þ
0þ
þ0
þþ
þ0
00
þþ
þ0
þþ
w
12
00
þ0
þþ
00
0þ
þþ
0þ
þW
þ0
0þ
0þ
þþ
00
þ0
1þ
13
00
þ0
þþ
00
0þ
0þ
0þ
0þ
þ0
0þ
þþ
00
þþ
þ0
1þ
14
þþ
00
þ0
0þ
þ0
0þ
0þ
þþ
þþ
þ0
0þ
0þ
þ0
þ0
w Table 3 e Kidd antigen typing of the cross matched donorunits.
X match Donors Result Kidd typing
Patient Donor 1 Compatible Jka�JkbþDonor 2 Compatible Jka D JkbD
Donor 2 red cells are indicated in bold since they were compatible
inspite of being positive for Jka antigen.
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e3 3
Please cite this article in press as: Makroo R, et al., Weak alloantibody anti Jka missed on routine crossmatching: a case reportillustrating the importance of “Type & Screen”, Apollo Medicine (2014), http://dx.doi.org/10.1016/j.apme.2014.02.004

Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/