Embed Size (px)
Citation preview

May-Jun 2015 | vol. 1 | issue 3 www.hysteroscopy.info
INSIDE THIS ISSUE
WELCOME 1
Interview of the month 3
Talking about ... 5
Hysteroscopy Devices 6
Highlights articles 8
Did you know...? 9
What's your diagnosis? 10
Case report 11
Resident's corner 14
Editorial 15
1
One of the biggest challenges of hysteroscopy is the treatment of submucosal fibroids.
For over 30 years the "gold standard" has been resection with monopolar resectoscope, performed in the operating room with the patient under anesthesia and using glycine as a distention media. Within the limitations of the technique is the approach of the deep fibroids. Different proposals as an alternative to monopolar resectoscope have emerged, including vaporization electrodes connected to resectoscope (Brooks, 1995; Vilos and Abu-Rafea, 2005) and vaporization with Nd: YAG (Ubaldi, 1995) among others, but that have been abandoned for various reasons. The most promising innovation technique was the introduction of bipolar resectoscopes that, using saline as a distention media, suppressed the risks associated glycine.
Since the 1990s, when the hysteroscopic procedures appear in query without anesthesia and applying the concept of "see and treat", the treatment of fibroids became our challenge. In recent years we are witnessing the emergence of different devices and surgical techniques for the in office surgical approach of submucosal fibroids, in many cases without using any anesthesia.
We are able through an instrument of 4-5 mm in diameter with a working channel 5 Fr of using different types of energy such as Versapoint with bipolar energy or laser diode and apply different techniques that allow us even today resection of deep submucosal fibroids (Bettocchi Haimovich 2009 and 2013). New technology has become available with the introduction smaller bipolar resectoscopes, aimed at in office hysteroscopy, small morcellators (Truclear and Myosure) and even vaporization systems based laser diode (myofiber).
In the current situation ways to decrease costs of procedures as well as decompress saturated operating rooms are sought. This is the present and the future of hysteroscopy, more and more procedures will be performed in the office, efficiently and safely, without the need of anesthesia, at a much lower cost than performing them in the operating room.
This coming May 15th will be held in Barcelona the 2nd National Fibroid’s Meeting. In this meeting the evolution/revolution of in office hysteroscopy regarding the management of fibroids will be addressed. One aim is to clarify the role of the new devices in terms of indications and limitations especially in dealing with fibroids. (www.miomas.net)
I hope that initiatives such as this magnificent Newsletter and with the support of the gynecological community will give to hysteroscopy the importance that it deserves.
Dr S. Haimovich
HYSTEROSCOPY PICTURES
2

TEAM COODINATORSPAIN
L. Alonso
EDITORIAL COMMITTEE
SPAINE. Cayuela
L. Nieto
ITALYG. Gubbini
USAJ. Carugno
MEXICOJ. Alanis-Fuentes
PORTUGALJ. Metello
ARGENTINAGonzalez A. M.
ITALIAA. Laganà
VENEZUELAJ. Jimenez
SCIENTIFIC COMMITTEE
A. Tinelli (ITA)L. Bradley (USA)A. Úbeda (Spa)A. Arias (Ven)
M. Rodrigo (Spa)A. Di Spiezio (Ita)
E. de la Blanca (Spa)J. Rios (Spa)
M. Bigozzi (Arg)S. Haimovich (Spa)
R. Lasmar (Bra)
All rights reserved. The responsibility of the signed contributions is
primarily of the authors and does not necessarily reflect the views of the editorial or
scientific committees.
HYSTEROSCOPY
PICTURES
May-Jun 2015 | vol. 1 | issue 3www.hysteroscopy.info
2
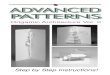
Chronic endometritis is usually presents in a silent way, becoming an incidental finding when performing endometrial biopsy for other reasons.
The use of hysteroscopy with liquid distention media of the uterine cavity has been shown to be an effective method for the diagnosis of chronic endometritis. A common hysteroscopic finding in chronic endometritis is the presence of a thickened endometrial edematous mucosa. Also, a thin hyperemic micropolyps layer (less than 1 mm) that appears to float in the endometrial cavity can be seen.
Using these criteria, the hysteroscopic diagnosis of chronic endometritis has a sensitivity up to 93%.
Appreciate the appearance of the micropolyps.
The presence of edema, hyperemia and
micropolyps suggest the diagnosis of endometritis.
If you are interested in sharing your cases or have a hysteroscopy image that you consider unique and want to share, send it to [email protected]

3
May-Jun 2015 | vol. 1 | issue 3 www.hysteroscopy.info
INTERVIEW WITH...Dr. Attilio Di Spiezio is a world recognized gynecologist who characterizes by his observations and research without limits.With the publication of his new book “State of the Art Hysteroscopic Approaches to Pathologies of the Genital Tract” he culminates a long journey into the world of hysteroscopy, which has led him to be recognized as a pioneer of modern hysteroscopy with the highest level of international appreciation.
The book "State of the Art Hysteroscopic Approaches to Pathologies of the Genital Tract" offers a wide and renovated vision of the current state of hysteroscopy. Highlighting novel chapters on chronic endometritis, the dysmorphic uteri and cervical pathology. A work published by Karl Storz that clearly and simply, discover the current state os the art in hysteroscopy. A must for both gynecologists in training, as well as for the fully trained gynecologist.
Attilio Di Spiezio Sardo
School of Medicine and SurgeryUniversity of Naples ‘Federico II’
Naples, Italy
At the beginning of the book, you give a tribute to those gynecologists who had accompanied you on your training. In your opinion, how important is the figure of the Mentor? The Mentor by definition is someone who imparts wisdom to and shares knowledge with a less experienced colleague. The Mentor has an invaluable role in medicine and mostly in endoscopic surgery where you need not only to acquire psychomotor skills but also surgical competencies. While psycomotor skills can be acquired on inanimate models, for surgical competencies you need a Mentor who can speed up your learning curve, reducing the unavoidable complications at the beginning of your “endoscopic trip”. I owe much of my career to all my Mentors who have guided my “endoscopic hand” since I was a medical student.
Does the development of assisted reproduction technology have contributed to the advancement of hysteroscopy? I think so. In the last years, the entire gynecological community, including those working in “infertility centers”, had to recognize that the uterine cavity and its inner layer, the endometrium, are fundamental for the implantation of the embryo. However, despite hysteroscopy is generally recognized as the gold standard technique for the evaluation of the uterine cavity and treatment of its relevant pathological disorders, its use as a routine procedure in the infertility work-up is still under debate as there is no consensus on its efficacy and effectiveness in improving the prognosis of infertile couples.
I found really interesting the chapter on Hysteroscopic Outpatient Metroplasty To Expand Dysmorphic Uteri. (HOME-DU technique), could you give us a brief summary? The new classification system of Müllerian anomalies developed by the ESGE/ESHRE CONUTA working group has dedicated a specific interest to those uteri, named “dysmorphic”, characterized by a normal outline but with an abnormal lateral wall’s shape of the uterine cavity ( i.e. T-shaped uterus and tubular-shaped/infantilis uteri). These uteri are associated with infertility and pregnancy loss and in the previous American Fertility Society classification were included in class VII and mainly related to diethylstilbestrol-related (DES) exposure. However clinical experience has shown that these uteri are more common than expected, mostly diagnosed in young infertile patients with no history of DES exposure.

4
www.hysteroscopy.info May-Jun 2015 | vol. 1 | issue 3
When faced with a tubular uterine cavity or an increased smooth muscle component on the walls of a ‘T’ shaped uterus, the literature reports success with a resectoscopic technique designed to improve the volume and the morphology of the uterine cavity. The technique involves the use of a hooked loop which is meticulously guided by the surgeon placing parallel longitudinal incisions along the main axis of the uterine cavity. The aim is to decrease the centripetal force of muscle fibers and of any fibro-muscular rings that have contributed to the stenosis, and to promote a consecutive increase in the volume of the uterine cavity. Recently, our group has developed a new outpatient technique yielding an increase in volume and an improved morphology of both T-shaped and tubular uterine cavities (Hysteroscopic Outpatient Metroplasty To Expand Dysmorphic Uteri: the HOME-DU technique). The novelty relies in the fact that such a technique combines the surgical principles of traditional resectoscopic surgery with the latest innovations of minimally invasive operative hysteroscopy and bipolar technology. The technique involves two incisions of 3–4 mm in depth made with a 5-Fr bipolar electrode along the lateral walls of the uterine cavity in the isthmic region, followed by additional incisions placed on the anterior and posterior walls of the fundal region up to the isthmus . The operation ends with the application of an anti-adhesive gel. Preliminary data on a cohort of 30 patients showed a significant increase in the volume of the uterine cavity, with a substantial improvement in uterine morphology. This resulted in an improvement of the reproductive outcomes with a clinical pregnancy rate of 57% and a live birth rate of 71% at mean follow-up of 15 months.
As Prof Nappi coded, hysteroscopy has sometime become the "Cinderella" of gynecology. Has the prime time of hysteroscopy arrived yet? I think so! The number of gynecologist performing diagnostic and operative hysteroscopy is rapidly increasing all over the world and many technical and technological innovations continue to be reported in the hysteroscopy field. “Hysteroscopy Newsletter” is an example of the need to “give voice” to such a growing number of endoscopic surgeons, who are specifically focused on hysteroscopy.
Has hysteroscopy reached its limits? What do you foresee as the future of hysteroscopy? Absolutely not! The limits of hysteroscopy are still far! Indeed there are many aspects of the uterine cavity which still need to be completely elucidated. I am thinking about endometrial receptivity, embryo implantation, uterine congenital anomalies, the progression from hyperplasia to carcinoma, the endocervical canal…. All the technological improvements which could help us to investigate and treat these and other unknown aspects/conditions of the uterine cavity will represent the “future” of hysteroscopy!
Do you have any advice for the young physician who is starting out in the world of surgery? Yes, I have! Follow your talent, achieve an excellent training and continually update during you career. But above all, keep in mind that the endoscopic training consists of 4 phases [didactic (i.e. theoretical knowledge), laboratory (i.e. training on inanimate models to simulate real procedures), observational (i.e. observation of real-time procedures) and preceptorship (i.e. performing a surgical procedure under direct supervision)] each of which is equally important. In other words, don’t be anxious to go straightaway to the operating room, but wait for the proper time to do it!
“ The limits of hysteroscopy are still far away!”

May-Jun 2015 | vol. 1 | issue 3 www.hysteroscopy.info
5
TALKING ABOUT
The role of diagnostic hysteroscopy in infertility is still debated today. Despite the growing literature demonstrating that treatment of adhesions, submucosal fibroids and uterine septa improve pregnancy rates, managing dysfunctional or inflammatory disorders remains doubtful. As mentor of young laparoscopists, I was surprised that the first objective of apprentices is the diagnosis of structural and functional abnormalities such as endometrial polyps and fibroids. However, experience shows that often these conditions are absent, while other images, such as congestion or endometrial hypertrophy, are present.
What is the real significance of these findings in infertility? We analyzed two groups of couples whom underwent diagnostic hysteroscopy before or after the first cycle of in vitro fertilization (IVF) and showed (ESGE, 2012) that pregnancy rates are doubled if the findings of endometritis were treated (and therefore diagnosed) before the first IVF cycle. How was the diagnosis made? Simply through images of suspected hysteroscopic endometritis, since microbiology or endometrial biopsy are often inconclusive and show low diagnostic sensitivity.
Moreover, there is still a high number of reproduction units that do not perform diagnostic hysterocopy before the first IVF cycle, but who diagnose "endometrial normal" after a "normal endometrium" apparent after ultrasound study, hysterosalpingogram, saline infusion or sonohysterography. Elaborating on the issue of treatment of infertility, a recent Cochrane (Cochrane Database Review, 2013) demonstrated that the findings on the treatment of endometrial polyps are not possible given the diversity of imaging and medical decisions on which it is based. Obviously, endometrial hypertrophy is the result of hyperestrogenism and creates an unfavorable environment on which an embryo should be implanted. If the focal hypertrophy create futures polyps, why should we treat focal endometrial growths, but not widespread growths?
There is a need for randomized control trials. However, if the diagnostic techniques are not homogeneous, the results will not be. Therefore, while we diagnose polypoid endometrium, will be resected without the use of energy before an IVF cycle.
Endometrial polyps and pre endometrium polypoid in vitro fertilization: Deal or no deal.
Úbeda. A. Hospital Universitari Quirón Dexeus. Spain

www.hysteroscopy.info May-Jun 2015 | vol. 1 | issue 3
6
DEVICESHYSTEROSCOPY
The Intrauterine Bigatti Shaver (IBS®)The IBS® consist of an angulated 6º telescope with a sheath and an extra working channel wherein a rigid shaver system is
introduced. The inflow of the sheath is connected to a peristaltic pump in order to maintain distention and visualization inside the uterine cavity. The outflow of the system is not connected and only used for passive outflow.
The outer sheath diameter is 24 Fr. (8 mm). The rigid shaver system consists of two hollow reusable metal tubes fitting to each other. The inner tube oscillates within the outer tube and is connected to a hand-piece (Drillcut-X ), a motor unit (Unidrive SIII) and to a roller pump (Endomat), controlled by one foot pedal. The foot pedal activates the movements of the shaver tip and the
roller pump's aspiration at the same time, in order to maintain a continuous suction power of solution and tissue axial through the hollow blade during procedure.
Presently, the double-flow bipolar resectoscope is considered the gold standard technique to perform hysteroscopic operations . Since June 2009 we have proposed an alternative approach to operative hysteroscopy called Intrauterine Bigatti Shaver (IBS®) that, by removing the tissue chips at the same time as their resection, improves visualization during the procedure, reducing several problems of conventional resectoscopy such as fluid overload, water intoxication, uterine perforation, and long surgeon’s learning curve. In cooperation with Karl Storz GmbH & Co., we have created a new shaving system that, when introduced through the straight operative channel of a panoramic 90° optic, allows performance of all major hysteroscopic operations. From June 2009 until March 2015 at our University teaching Hospital: “Ospedale San Giuseppe of Milan - Italy”, we have performed with the IBS® : n.119 myomectomies, n.429 polypectomies, n.32 mixed pathologies (myomectomies + polypectomies + sinechiolysis), n.4 sinechiolysis, n.4 placental remnants removal, n.13 endometrial ablations, n.7 septum resections and n.2 combined myomectomies and septum resection, for a total of 610 operations. We have reported the following complications: n.1 (0.2%) perforation, n.2 (0.4%) fluid overload, n.9 (1.7%) intra -operative bleeding, n.5 (0.9%) cervical lacerations and n.1 (0.2%) via falsa. None of these complications had severe consequences for the patients
Greece and Italy. Since 1992 He has been Tutor of Laparoscopy at the University of Milan. Since 2009 he has dedicated himself to the development of a new device for operative Hysteroscopy
called IBS® “Intrauterine Bigatti Shaver”. This new instrument has shown to be a valid alternative to the Bipolar Resectoscope. At present he is Medical Assistant at the Department of Obstetric and Gynaecology in the University Teaching Hospital of Milan: “Ospedale San Giuseppe”.
Dr. Giuseppe Bigatti was born in Milan and took his Medical degree on at the University of Pavia. Since 1992 He has been Tutor of Hysteroscopy, with the Rollerball Team supervised by Dr. R. Campo, during several workshops organised in Austria,Belgiu, Slovak Republic

May-Jun 2015 | vol. 1 | issue 3 www.hysteroscopy.info
7
Although the latest Cochrane review concluded that there was no evidence to support the usefulness of paracervical block, it is the most common modality used to manage pain at
during in office hysteroscopy. Several papers have shown that the paracervical anesthesia produces an improvement in the perception of pain due to manipulation of the uterine cervix
during hysteroscopy. However, it does not seem to reduce the pain associated with the manipulation of the body / uterine fundus or fallopian tubes. The most commonly anesthetic used is lidocaine 1% with epinephrine, added vasoconstrictor decreases the absorption and
increases the duration of action of the anesthetic, being effective as an anesthetic at 2 minutes after injection and lasting effect about 2-6 hours. Infiltration is usually done at the
height of the uterosacral ligaments, about 3 mm deep and about 5 ml of anesthetic is injected.
A randomised prospective study published by Bigatti et al on Gynaecological Surgery in February 2012 showed that especially for the treatment of large polyps and myomas up to 2 cm it has several well-described advantages. All types of submucosal myomas, including G2 myomas that were excluded from similar studies with morcellators, were included in this study. The main advantage of the IBS® was that the myomas were effectively enucleated from their fovea and the intramural site of insertion of the myoma was removed. The surrounding healthy endometrium was avoided without any thermal injury occurring compared with the less precise behaviour of conventional resectoscopy. Despite the well-described advantages of the shaver technique, myomas larger than 3 cm, which present a higher consistency, often underwent a second step procedure or a conversion to conventional bipolar resectoscopy. In order to improve on the result of the IBS® there are two possibilities . The first is to increase the cutting power of the blades by means of disposable blades or newly designed blades, which show to be more aggressive on the myomatous tissue. The second possibility is the myomas consistency reduction by means of a medical treatment. Regarding this option, we believe that one possible answer could be the use of progesterone in the preoperative treatment of patients with submucosal myomas. At present the IBS® can be considered a valid alternative to the conventional bipolar resectoscope.
TIPS and TRICKS... 4U
Some things just can’t be learned from books. Some things can only be learned through experience. In this section the best hysteroscopists will share their tricks with you.

www.hysteroscopy.info May-Jun 2015 | vol. 1 | issue 3
8
OBJECTIVE: To investigate the recurrence potential of intrauterine adhesions after hysteroscopic adhesiolysis.DESIGN: Retrospective observational study.POPULATION: This study included 115 women who had intrauterine adhesions completely separated during hysteroscopic surgery. The treated adhesions were classified into four groups according to their location and extent: Group 1, central type (i.e. intervening space between the adhesions and both lateral uterine sidewalls) at the middle area of uterine cavity; Group 2, central type at uterine cornua; Group 3, cervico-isthmic; and Group 4, extensive if the adhesions were dense with occlusion of part of the uterine cavity other than cervico-isthmic region.METHODS: Postoperative outpatient hysteroscopic adhesiolysis was scheduled 10-14 days after the initial hysteroscopic surgery and procedures were repeated every 10-14 days until no reformed adhesions were detected. Multivariate logistic regression models were built to examine initial adhesion characteristics and other factors associated with adhesion reformation and need for subsequent outpatient adhesiolysis. Categorical data were compared using Fisher's exact test.MAIN OUTCOME MEASURES: Number of postoperative outpatient hysteroscopic adhesiolysis procedures.RESULTS: The location and extent of adhesions according to the allocated group was the only parameter independently related to the number of postoperative outpatient adhesiolysis procedures (P = 0.0004). Women with Group 1 adhesions underwent a lower number of postoperative interventions compared with those with Group 2, 3 and 4 adhesions (P = 0.0355, P = 0.0004 and P = 0.0087, respectively).CONCLUSIONS: There is an increased likelihood of intrauterine adhesion recurrence when successfully divided adhesions were originally located at the uterine cornua, the cervico-isthmic region or involved a large portion of the uterine cavity.
The influence of the location and extent of intrauterine adhesions on recurrence after hysteroscopic adhesiolysis
Yang JH, Chen CD, Chen SU, Yang YS, Chen MJ.BJOG. 2015 Mar 6. doi: 10.1111/1471-0528.13353. [Epub ahead of print]
Is cold loop hysteroscopic myomectomy a safe and effective technique for the treatment of submucous myomas with intramural development? A series of 1434 surgical procedures.
Mazzon I, Favilli A, Grasso M, Horvath S, di Renzo GC, Gerli S.J Minim Invasive Gynecol. 2015 Mar 18. doi: 10.1016/j.jmig.2015.03.004. [Epub ahead of print]
OBJECTIVE: To assess the safety and efficacy of cold loop hysteroscopic myomectomy in a large series of cases.DESIGN: Retrospective study.DESIGN: Classification: Canadian Task Force Classification III.SETTING: "Arbor Vitae" Centre for Endoscopic Gynaecology in Rome, Italy.PATIENTS: A total of 1215 patients with one or more G1-G2 submucous myomas.INTERVENTIONS: Cold loop hysteroscopic myomectomy.MEASUREMENT: A total of 1690 myomas were removed. A minimum of one to a maximum of five fibroids for each surgical procedure were totally removed. Out of 1215 patients, 1017 (83.7%) were treated with a single surgical procedure. Twelve intraoperative complications occurred (0.84%). No cases of uterine perforation with the thermal loop or clinical intravasation syndrome were reported.CONCLUSION: Cold loop hysteroscopic myomectomy seems to represent a safe and effective procedure for the removal of submucous myomas with intramural development, while at the same time respecting the anatomical and functional integrity of the myometrium. The use of a cold loop in resectoscopic myomectomy is associated with a low rate of minor intraoperative complications and an absence of major complications. This could be of primary relevance with a view to fertility and future pregnancies.
HIGHLIGHT ARTICLESPublished on different medias

May-Jun 2015 | vol. 1 | issue 3 www.hysteroscopy.info
9
DID YOU KNOW...?
The “isthmocele” represents a possible consequence of one or more cesarean deliveries and may be symptomatic
in some women. It is a defect that can be easily diagnosed by hysteroscopy and successfully treated by resectoscopic technique.
The mesenchymal metaplasia involves the endometrial stroma and this stroma can be replaced by cartilaginous and bone tissue, glial,
adipose, smooth muscle tissue and foci of extramedullary hematopoiesis.

www.hysteroscopy.info May-Jun 2015 | vol. 1 | issue 3
10
Palshetkar Nandita, Pai Rishma Dhillon, Pai Hrishikesh D
Jaypee 2013, 294 Pages
The Textbook of Hysteroscopy provides clear understanding of techniques, outlines potential complications, and highlights circumstances for which procedures are contraindicated. This book provides excellent resources that aims to meticulously cover the role of hysteroscopy, both diagnostic and therapeutic in clinical gynecology and infertility practice. Chapters are relevant, complete, and easy-to-understand procedures are described in detail and fully illustrated with color photographs. Cover step-by-step descriptions of common operative surgical techniques and practical hints on hysteroscopic procedures. This book provides solid grounding in the art and science of hysteroscopy. It is strongly recommended to all gynecologists in training and to those already in practice.
Sometimes, when performing hysteroscopy, it is important to pay attention to every corner of the uterus, as Vasari stated «cerca trova», «he who
seeks finds»
WHAT'S YOUR DIAGNOSIS?
Answer to the previous issue: The image is a picture of intrauterine adhesions

May-Jun 2015 | vol. 1 | issue 3 www.hysteroscopy.info
11
CASE REPORT
Endometrial smooth muscle metaplasia Garcia Mourin B. Alonso Pacheco L. Spain
The term metaplasia is defined as the transformation of a well-differentiated tissue into another well differentiated type. Little is known about endometrial metaplasia. These can be of two types, epithelial metaplasia and mesenchymal metaplasia affecting the endometrial stroma. In the latter type of metaplasia, it may occur within the islets of endometrial stromal smooth muscle, cartilage and bone, glial tissue, fat and foci of extramedullary hematopoiesis. We describe a case of smooth muscle metaplasia and review the scarce literature, trying to correlate this diagnosis with endometrial leiomyomata.
CASE
A 34 years old patient presented to our office for hysteroscopic assessment of the endometrial cavity after ultrasound findings suspicious of submucosal fibroid that fills the entire cavity. Hysteroscopy demonstrates the existence of multiple submucosal fibroids type 0, of less than 1 cm in diameter. After hysteroscopy, an ultrasound revealed a 7.2 x 4.9 cm uterine cavity with the presence of multiple fibroids.
A hysteroscopic myomectomy was performed, the fibroids were enucleated from its bed and were extracted with cutting loop as a curette, using electrosurgery only to remove the larger two fibroids.
After the intervention, the patient received estrogen treatment to prevent adhesion formation. Neither the hysteroscopy performed one-month later nor the one performed at 6 months, revealed any remnants of the fibroids previously described.
Pathology revealed multiple smooth muscle proliferation without atypia, in transition with endometrial stroma, establishing the diagnosis of nodular stromal metaplasia with leiomyoma differentiation.

www.hysteroscopy.info May-Jun 2015 | vol. 1 | issue 3
12
DISCUSSION
The finding of endometrial metaplasia is rare with only a few published cases, being perhaps most common type bone metaplasia. Smooth muscle metaplasia is included within endometrial mesenchymal metaplasia, and although rare, is probably the most common mesenchymal metaplasia. Probably in most cases go unnoticed classified as diffuse fibroids.
It seems that there is presence of endometrial cells with multipotential capacity to differentiate into endometrial stromal as well as smooth muscle fibers. In fact, it is not uncommon to find small pockets of smooth muscle within the endometrial stroma, sometimes being classified as endometrial foci leiomyomas.
The pathology of our case suggests of multiple formations with myomatous appearance, with diameters ranging from 0.3 to 1 cm that occupies a total volume of 3.5 cc. Countless microscopically smooth muscle proliferation without atypia is seen swirling in transition with endometrial stroma and the diagnosis of stromal nodular metaplasia with leiomyoma differentiation is established. There appears to be similarities between the cases of endometrial leiomyoma and endometrial smooth muscle metaplasia that could be considered as the same entity and is the pathology and the existence of smooth muscle proliferation in endometrial stromal transition, that gives the key aspects for the diagnosis smooth muscle metaplasia.
This is a very rare condition with only a few well-documented cases. To our knowledge this is the first hysteroscopic image of this condition. We have found another similar picture, but it was a subendometrial leiomyomata.

May-Jun 2015 | vol. 1 | issue 3 www.hysteroscopy.info
13
ESGE 24rd anual congress Your Key to endoscopyBudapest, Hungary |October 7-10|2015
6th International IVI CongressReproductive Medicine and BeyondAlicante, Spain |April 23-25|2015
Gineco-endoscopy ClubLaparoscopy and Hysteroscopy Procedures in Gynecology and InfertilityPrague, Czech Republic |May 20-22|2015
Miomas BCN 2015Jornada nacional de miomas 2015Barcelona, Spain |May 15|2015
11th AAGL International Congress on minimally Invasive gynecological surgeryJerusalem, Israel |jun 16-19|201530
XVII Congreso federacion Mexicana de endoscopia ginecológicaMexico, Mexico | April 30-May 3|2015
3rd ISGE African Conference Kenia Society Endoscopic SpecialitiesNairobi, Kenia | August 23-26|2015
3rd Annual MESGE & 6th Congress Of TSGEAntalya, Turkey |April 8-11|2015
22nd World Congress onControversies in Obstetrics, Gynecology & Infertility Budapest, Hungary |Sept. 17-20|2015
CongresSINTERNATIONAL
44th AAGL Global Congress of Minimally Invasive Gynecology Las Vegas, Nevada |nov 15-19|2015
52 Congreso Mexicano de medicina de la reproducción Mérida, Mexico |jul 15-18|2015
44th AAGL Global Congress of Minimally Invasive Gynecology Las Vegas, Nevada |nov 15-19|2015
16th APAGE Annual Congress Beijing, China |nov 5-8|2015

14
May-Jun 2015 | vol. 1 | issue 3www.hysteroscopy.info
Resident'sCORNER
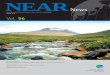
Use of hysteroscopy in relation to intrauterine devices.Barbany, N; Coco, A. Hospital Universitario Quirón-Dexeus. Spain
The use of the IUD as a method of reversible contraception is the most widely long active reversible contraception method (LARC) used worldwide. We present a series of cases in which hysteroscopy was useful for the management of disorders and complications related to these devices.
The main indication for hysteroscopy in women with IUD removal:
1-Failed of in office blind removal 2- Unable to visualize the thread3- Ultrasound diagnosis of malposition or perforation 4- IUD fracture during attempted in office removal5- Diagnosis abnormal bleeding with IUD in situ
Intracavitary IUD threadsIUD with horizontal malposition Decidualized endometrium due to hormonal effect of the IUD
Embedded IUD in patients with endometrial polyp
Round shaped IUD (Not available in the US) without thread and subsequent extraction using hysteroscopic forceps.

15
Dear reader,
With the overwhelming speed in which medical technology is advancing, where robotic surgery and telemedicine are things of the present; this Newsletter was born as a result of the effort of a group of gynecologists who share the passion for hysteroscopy, and have a common goal, the continuous progress in the gynecological care of women.
In the first two volumes of Hysteroscopy Newsletter, world leaders, well recognized pioneers of modern hysteroscopy, have generously shared not only their knowledge, but also valuable practical tips that only true experts can offer. Phrases like "The hysteroscope is my stethoscope" expressed by Dr Linda Bradley reflects the important role that hysteroscopy plays in modern gynecology.
The Hysteroscopy Newsletter team of editors is firmly committed to maintaining the highest level of quality. At the same time, we are pleasantly grateful for the great reception given to our Newsletter, which being available at no cost on the internet in both English and Spanish (for now, with plans to translate it into other languages in the near future) has transcended geographical boundaries and has been downloaded from the web in many countries.
I would like to take this opportunity to encourage young residents, and those who have recently initiated into the wonderful world of hysteroscopy, not only to read our publication, but to actively participate by sending your hysteroscopic images of interesting cases for publication.
Lets continue with this strong enthusiasm... I will see you in the next volume.
Jose Carugno MD FACOG Assistant Professor OB/GYNUniversity of Miami - Miller School of Medicine
Hysteroscopy newsletter
HYSTEROscopy group
Hysteroscopy newsletter
www.twitter.com/hysteronews
www.facebook.com/hysteronews
Hysteroscopy Newsletter is an opened forum to all professionals who
want to contribute with their knowledge and
even share their doubts with a word-wide
gynecological community
FIND US ON
HYSTEROSCOPY
Editorial teaM
www.hysteroscopy.infoMay-Jun 2015 | vol. 1 | issue 3