Embed Size (px)
Citation preview

Vitamin K and its clinical applications
Dr. Rohini C Sane

VITAMIN K “K ” is the abbreviation of the German word “Koagulation ”
VITAMIN K are Naphthoquinone derivatives and have long side
Isoprenoid chain.
1929 – Henrick Dam – isolation of Vitamin K1 –(Noble Prize )
1939 – Edward Doisy – isolation of Vitamin K2 –(Noble Prize 1943 )

Properties of Vitamin K
A. Anti hemorrhagic factor = coagulation vitamin K
B. Yellow oil
C. With Low Melting point
D. Optically active
E. Thermostable
F. Labile for light and alkali
G. Absorbs UV light
H. Synthesis by intestinal bacteria
I. Daily dietary requirement nil (dietary factors and synthesis by intestinal
bacteria 70-140 micrograms /day )

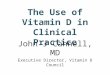
CHEMISTRY OF VITAMIN K
VITAMIN K1 VITAMIN K2 VITAMIN K3
NAME OF SIDE
CHAIN
PHYLOQUINONE
( 20C )
FARNO QUINONE
( 30C )
MENADIONE
SOURCES (ALPHA –ALPHA)
CABBAGE
SOYABEAN
BACTERIA ,FISH ,MEAT SYNTHETIC
-USED IN CLINICAL
PRACTICE
CHEMISTRY 3 PHYTYL
1,4 NAPHTHQUINONE
2 METHYL 3 DIFARNESYL
1,4 NAPHTHQUINONE
2 METHYL
1,4 NAPHTHQUINONE
SOLUBILITY FAT SOLUBLE FAT SOLUBLE WATER SOLUBLE
Comparison of types of vitamin k

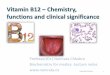
Chemistry of Vitamin K
Isoprenoid chain
Isoprenoid chain
Isoprenoid chain
Naphthoquinone
Naphthoquinone

Dietary sources of vitamin k for vegetarians

Dietary sources of vitamin k for non-vegetarians

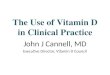
Metabolism : Absorption and transport of Vitamin K
Dietary/ Intestinal Vitamin K
Small intestine
Target Tissue
Bile salts
LDL
1. storage in Liver
2. Transportation in
plasma by
Beta Lipoproteins
1. No excretion in
urine
2. Excretion in feces
in large quantities
(bacterial origin)
Absorption along with Chylomicrons
Transport

MORAWITZ THEORY OF BLOOD COAGULATION
THROMBIN
PROTHROMBIN
FIBRINFIBRINOGEN BLOOD
COAGULATION
INTRENSIC AND EXTRENSIC FACTORS

Factors of blood coagulation dependent on VITAMIN K
Factor II = PROTHROMBIN
Factor VII = SPCA
Factor IX = CHRISMAS FACTOR
Factor X = STUART PROWER FACTOR
All of them are synthesized in the liver as inactive zymogens.
They undergo post translational modification : Gamma carboxylation of Glutamic
acid residue.
Gamma carboxylation of Glutamic acid (GCG ) synthesis needs Vitamin K as a
cofactor.

Vitamin k dependent carboxylation of the precursors of clotting factors
PROTEIN* -----NH--- CH---CO + O2 + CO2
Ι
CH2
Ι
CH2 (PROTEIN * : PRECURSORS OF CLOTTING FACTORS II ,VII,IX,X)
Ι
COOH
DICUMAROL &
WARFARIN CARBOXYLASE and VITAMIN K
PROTEIN -----NH ----CH---CO
Ι
CH2
Ι
CH2
COO⁻ COO ⁻ ( CARBOXYLATED CLOTTING FACTORS II ,VII,IX,X) Ca ²⁺

Osteocalcin and Vitamin K
Osteocalcin is
1. A small protein ( 40-50 amino acids )
2. synthesized by osteoblasts of bone and its synthesis is induced by Vitamin D
3. Structural protein of kidney ,lung and spleen
4. Functional activity dependent on Vitamin K for gamma carboxylation of Glutamic acid residue at active site
5. Binds to hydroxy apatite crystals of bone- dependent on Vitamin K for gamma carboxylation of Glutamic acid residue at active site
6. Contains hydroxyproline - dependent on Vitamin K and C.

Functions of vitamin K
GLUTAMIC ACID OF CALCIUM BINDING PROTEINS (FACTOR II,VII,IX,X OSTEOCALCIN )
GAMMA CARBOXY GLUTAMIC ACID (Glu-Coo- )
CALCIUM BINDING (Ca2+) to PROTEINS
(in Organs dependent on Calcium binding proteins)
VITAMIN K DEPENDENT carboxylase oxygen , CO2 ,NADH and Vitamin K

Organ dependent on calcium binding protein and Vitamin K
Organ dependent on calcium binding protein and Vitamin K are
1. Bone
2. Spleen
3. Placenta
4. Kidney

Vitamin K dependent carboxylase
Vitamin K dependent carboxylase is
1. A microsomal enzyme
2. needs oxygen , CO2 ,NADH and Vitamin K
3. Undergoes cyclic process which is Vitamin K dependent and process is
inhibited by Dicumarol/ Warfarin

VITAMIN K CYCLE IN CARBOXYLATION REACTIONS
PROTEIN-GLUTAMIC ACID CARBOXYLASE PROTEIN- CARBOXY GLUTAMIC ACID
VITAMIN K 2,3 EPI OXIDE FORM
(HYDRO QUINONE FORM)
REDUCTASE REDUCTASE
DICUMAROL/ WARFARIN
QUINONE FORM
Fetal Warfarin syndrome :
Treatment of pregnant women with Warfarin leads to fetal bone malformation

Role OF Vitamin K and Warfarin
warfarin as an anti- Coagulant

Mechanism of action of Vitamin K and Warfarin in coagulation

Deficiency of vitamin K
RDA of vitamin K = 70 -140 Micrograms /day( This is available in a normal diet )
Intestinal bacterial synthesis of vitamin K is sufficient to meet needs of the
body.
Deficiency of vitamin K is very RARE and occurs when intestinal flora of
microorganism is disturbed and vitamin K synthesis is inhibited .

Causes of Deficiency of vitamin K
1. Prolonged antibiotic therapy(killing intestinal bacteria)
2 . Malabsorption of lipids due to
A. Sprue
B. Steatorrhea
C. Coeliac diseases
D. Obstructive jaundice ( unavailability of bile salts –when fat and fat soluble vitamins not absorbed)
E. Chronic pancreatitis
3. Short circulation bowel as a result of surgery
4. Consumption of Spoilt Clover Hay ( contains Dicumurol = Vitamin K Antagonist )
5. HEMORRHAGIC DISEASE OF NEWBORNS (intestinal flora not formed after placental detachment)

Causes and consequences of Deficiency of vitamin K :1. ( Prolonged antibiotic therapy(killing intestinal bacteria)
Prolonged antibiotic therapy(killing intestinal bacteria)
Lack of active prothrombin
Prolonged prothrombin time
Delayed coagulation/clotting time
Spontaneous hemorrhages
Profuse bleeding with minor injuries

Hemorrhagic disease of newborns and Deficiency of vitamin K
Hemorrhagic disease of newborns is attributed by Deficiency of
vitamin K.
Causes of Hemorrhagic disease of newborns leading to Deficiency of
vitamin K are
1. Lack of hepatic stores of vitamin K
2. Absence of Intestinal flora ( synthesis of vitamin K inhibited )
3. Limited oral intake ( if breast milk has low levels of vitamin K : less
than 15 mg /liter )
Management of Hemorrhagic disease of newborns : Premature/preterm
infants –prophylactic doses of 1mg Menadione ( synthetic vitamin K )

Clinical manifestation of Deficiency of vitamin K
In adult and children ,deficiency of vitamin K is manifested as
1. Bruising tendency
2. Enchymotic patches
3. Mucous membrane hemorrhage
4. Post traumatic/ internal bleeding
5. Hemorrhagic disease of newborns
Prolonged prothrombin time
Delayed coagulation/clotting time

Management of Deficiency of vitamin K
Management of Deficiency of vitamin K includes
1. Water Soluble Vitamin K3 Injection 1mg Menadione
( synthetic vitamin K )
Oral Doses Of Vitamin K Not Effective

Function of Vitamin K in Oxidative Phosphorylation :
Function of Vitamin K in Oxidative Phosphorylation is demonstrated as follows :
MITOCHONDRIA
UV RAYS
OXIDATIVE PHOSPHORYLATION INHIBITED
UV EXPOSED MITOCHONDRIA + VITAMIN K OXIDATIVE PHOSPHORYLATION RESTORED
DICUMUROL = UNCOUPLER OF OXIDATIVE PHOSPHORYLATION

Antagonists of Vitamin K1.Heparin : used in treatment of heart diseases as it prevents clotting
Prothrombin time (PT) increases after administration of VITAMIN K
(Normal Prothrombin time : 11 seconds)
Heparin administration needs close monitoring
2. Dicumarol / Warfarin : Structural similarity with vitamin K - inhibits
conversion of prothrombin to thrombin
3.Salicylates

DICUMAROL/ WARFARIN
Dicumarol/ Warfarin are
1. Structural analogs of vitamin K
2. Competitive inhibitors of Vitamin K dependent carboxylase therefore
inhibit gamma carboxylation of Glutamic acid residue at active site of
coagulation factors (FACTOR II,VII,IX,X, OSTEOCALCIN)
3. Wildly used as an anticoagulant for therapeutic purpose

Hypervitaminosis K
Hypervitaminosis K leads to
1. Hemolytic anemia
2. Jaundice ( hyperbilirubinemia and kernicterus-leading to brain damage)

Prothrombin time and vitamin K
Prothrombin time is index of liver function is and
prolonged in cases of abnormalities liver functions .
Criteria Defective liver
functions
Vitamin K deficiency
Prothrombin time (PT) * Prolonged Prolonged
Cause of prolongation of
prothrombin time
Lack of synthesis of
coagulation factors
/Unavailability of bile
salts
Unavailability of vitamin K for
activation of prothrombin
After administration of
vitamin K ( Menadione )
Failure to restore PT restore PT
Measurement of (PT) * before and after surgery is essential.

FAT SOLBLE VITAMIN AND THEIR FUNCTIONS