Embed Size (px)
DESCRIPTION
Medical Portion for CE Speaker
Citation preview

This program has been sponsored by an educational grant from
Presented by:Name, Credentials
TitlePlace of Employment

The faculty, planners, and manager who are in a position to have control over content of this activity (including their spouse and/or life partner) have disclosed the following financial relationships or relationships to products or devices they or their spouse/life partner have with commercial interests relative to the content of this CE activity.

The Institute for Wellness and Education is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education. This program is approved for 2.0 contact hours (0.2 CEUs) under the ACPE universal program number 0459-0000-11-038-L01-P&T.

Discuss the incidence and pathophysiology of venous disorders
Identify patients at risk for the development of venous disorders
Describe the effects and medical efficacy of medical compression stockings for venous disorders
Evaluate the alternative revenue that graduated compression garments can generate
Assess the role of the pharmacist in maximizing patient compliance and slowing disease progression
Identify strategies to increase routine use of graduated compression garments for venous disease

What percentage of Americans are affected by venous disease?
A.20%
B.30%
C.40%
D.50%
E.60%

60% of American suffer from venous disease and its sequelae
More than 80 million Americans suffer from vein problems, most common are› Varicose veins› Spider veins
Incidence increases with age and is more common in women
More people lose work time from venous disease than from arterial disease
National Heart Lung and Blood Institute (NHLBI). Available at: http://www.nhlbi.nih.gov/ Accessed 01/27/11.American College of Phlebology (ACP). Available at: http://www.phlebology.org/patientinfo/index.html Accessed 01/27/11.Vascular Disease Foundation Newsletter. Spring 2005; Volume 5, N2

Family history Females
› Pregnancy› Medications
Travel (periods ≥8 hours) Lifestyle
› Sedentary› Obese (women)› Smoking (men)› Prolonged standing or sitting
occupation
Bergan JJ. The Vein Book. 2007; p. 42 Geerts WH, et al. CHEST. 2008; 133: 381S-453S.
DVT Injury to vein walls and
venous valves Immobilization post-
surgery Increasing age (changes
elasticity of veins)

Prospective case-control study of 134 families (402 total subjects)› 67 controls and their parents› 67 patients and their parents
Varicose veins in legs 30-40 years old No history of DVT
Risk for development of varicose veins in› BothBoth parents affected: 90% males and females› OneOne parent affected: males 25%, females 62%› NeitherNeither parent affected: 20% males and females

Study Data
Mark PE, et al. Approx. 1.1-1.5 per 100,000 US and EU deliveries result in death from pulmonary embolisms
Thaler E, et al. 33% of primaparas and approx. 50% of multiparas have evidence of varicose veins after pregnancy
Emergent varicose veins occur in approximately 25% if pregnancies
Rodger M. Pregnant women have a 7- to 10-fold increased risk of VTE compared to nonpregnant women
VTE kills 1 in every 20,000 pregnant women annually VTE occurs in up to 12 per 10,000 women from conception
to delivery and up to 7 per 10,000 women after delivery
Dresang LT, et al VTE is the leading cause of maternal death in the US 78-90% of DVTs during pregnancy occur in left leg
Marik PE, et al. NEJM. 2008; 359(19):2025-2033Thaler E, et al. Swiss Med Wkly. 2001; 351:659-662Rodger M. Hematology. 2010: 173-180Dresang M. Hematology. 2010: 173-180

30% first time pregnancy; 55% two or more result in varicose veins› Increased blood volume (40-50%)› Hormonal changes› Pressure of the fetal head
Compression Stockings are beneficial during pregnancy and post partum period
Swiss Medical Weekly 2001; 659-662Physiology 1998; Issue 9: 1-3Br J. Obstec Gynecol. 1999; Jun; 106: 106(6): 563-9

Deep Vein System› High Pressure System› Handles up to 90% of venous blood volume› Include: Anterior and posterior tibial veins, peroneal veins, popliteal
vein, superficial femoral vein, common femoral vein
Superficial Vein System› Low Pressure System› Handles remaining 10% of
venous blood volume› Include: Greater and lesser
saphenous vein
Perforating/Communicator Veins› Communicator veins connect
“like” veins› Perforating veins connect
deep to/from superficial veins

Think of a Roadmap!Think of a Roadmap!
Deep
Superficial
Perforating/
Communicator

Primary function of venous system is blood return to the heart
Three mechanisms to achieve venous blood return to heart Multiple muscle pumps Competent valves A pressure gradient
Lohr, J, et al. Curriculum Recommendations from American Venous Forum. 2006. Available at: http://veinforum.org/index.php?page=venous-curriculum Accessed 1/27/11

Which muscle pump(s) is/are referred to as the
“peripheral heart” and is primarily responsible for venous return?
A.Foot/ankle pump
B.Arterial pressure
C.Calf pump
D.A and C only
E.All of the above


The major peripheral pump consists of calf muscle
Calf Muscle Contraction (Systole) Increase in venous blood pressure forces
valves open Blood shunts towards heart to empty veins
Calf Muscle Relaxation (Diastole) Decrease in venous blood pressure allows
valves to close Prevents blood reflux

Additional peripheral pumps include:
Foot
Arterial Pressure
Abdominal Pressure
Ankle


Valve Open Pumps blood against gravity towards heart Valve Closed
Inhibits gravitational reflux of pumped blood

Vein Wall InjuryVein Wall Injury
↑↑
Venous Venous HypertensionHypertension
↑↑
Damaged ValvesDamaged Valves


Dynamic Pressure› Energy imparted by pumping action of the
heart Hydrostatic Pressure
› Pressure generated by the effects of gravity on the lower extremity
› Venous blood is pumped out of the dependent limb against the force of gravity
› Pressure determined by the distance (height) to the right atrium
Lohr, J, et al. Curriculum Recommendations from American Venous Forum. 2006. Available at: http://veinforum.org/index.php?page=venous-curriculum Accessed 1/27/11

PressurePressureDifferenceDifference
30-40mmHg30-40mmHg40-50mmHg40-50mmHg
Pressure at the Ankle in Normal Venous System
Lying Down 10 mmHg
Standing 90 mmHg
Walking 25-35 mmHg
Pressure at the Ankle in Defective Venous System
Lying Down 10 mmHg
Standing ≥100 mmHg
Walking ≤70 mmHg
The effect of the calf, ankle and foot pumps takes place after
only 7 steps!only 7 steps!

Disturbances within the veins which alter venous blood return to the heart
Due to local pathological changes: Venous thrombosis Valvular function Changes in venous wall Endothelial damage
Eklof B, et al. Controversies in the Management of Venous Disorders. London: Butterworths, 1989.

Virchow’s Triad
DVT affects approx. 2 million Americans annually
Pulmonary embolisms kill up to 300,000 Americans annually
The Awareness…74% of adults have little or no awareness of DVT
57% are unable to name any common risk factors or pre-existing conditions that could lead to the development of DVT
95% report that their physician had never discussed this medical condition with them
September 15, 2008 “Call to Action” by acting Surgeon General – Steven Galson, MD, MPH
APHA Deep-Vein Thrombosis Omnibus Survey. Conducted by Wirthlin Worldwide 2002.The Coalition to Prevent Deep-vein Thrombosis Web site. 2010. http://www.preventdvt.org/about/what-is-dvt.aspx. Accessed:
10/27/2010.

Observational study of 7222 subjects residing in Worchester, MA to evaluate VTE diagnosis (determined from ICD-9 codes) post-hospitalization from 1999, 2000, and 2003
Arch Intern Med. 2007; 167(14): 1471-1475
1897 subjects experienced DVT (n=1348), PE (n=285), or both (n=264) within the 3-year period.
Of the 1897 validated VTE cases, 73.7% (n=1399) presented in the outpatient setting with signs and symptoms or confirmed VTE diagnosis within 1 day of hospital admission.

True or False. Venous insufficiency is synonymous with arterial insufficiency.
A.True
B.False

Peripheral Vein Insufficiency (Disease)
Inadequate return of venous blood from the legs to the heart
Clinical Symptoms: tired/heavy, achy cramping in the legs
Clinical Indication: pain worsens when standing and improves with leg elevation and leg activity
Peripheral Arterial Insufficiency (Disease)
Narrowing of the arteries, commonly the pelvis & legs
Clinical Symptoms: cramping, pain, tired legs or hip muscles
Clinical Indication: pain that worsens during walking/activity and subsides with rest
PAD=peripheral arterial disease; PVD=peripheral venous disease

Telangiectasia(spider veins)
Varicose Veins
Deep Vein Thrombosis
Lipodermatosclerosis
Superficial Phlebitis

Venous Hypertension
Chronic Venous Insufficiency
Venous Ulcers

Grade Description
C0 No evidence of venous disease
C1 Superficial telangictasias (reticular veins) only (<4mm diameter)
C2 Simple varicose veins only (>4mm diameter)
C3 Ankle edema as a sequel of varicose veins
C4 Skin changes (pigmentation, venous eczema, lipodermatosclerosis)
C5 Skin changes with healed ulceration
C6 Skin changes with active ulceration
Evans CJ, et al. J Vasc Surg. 2004: 40: 1248-1252
C=ClinicalE=Etiology
A=AnatomyP=Pathophysiology

Which medication classes may indicate that a patient has or is at risk for venous insufficiency?
A.Anticoagulants
B.HRT
C.Antineoplastic agents
D.Prenatal vitamins
E.All of the above

Medications that increase
thromboembolism risk: Hormone replacement
therapy Oral contraceptives Raloxifene Tamoifen
Medications indicating additional
thromboembolism risk: Antineoplastic or related
agents, i.e., Etoposide Cyclophosphomide Tyrosine Kinase inhibitors
(i.e., imatinib) Thalidomide/lenalidomide
Anticoagulants


True or False. Venous insufficiency is a condition that goes away with treatment.
A.True
B.False

Treatment Goal: Restore patient to active lifestyle, minimize pain and/or disability
Treatment Methods: Pharmacologics (i.e., anticoagulants) Herbal alternatives Vein procedures Non-Pharmacologics/ Compression Therapy

Reduces symptomatic and asymptomatic VTE by 50-65%
Oral vitamin K antagonist Coumadin (warfarin)
Direct thrombin inhibitor Pradaxa (dabigatran)
Anti-factor Xa inhibitor Heparin Lovenox (enoxaparin) Fragmin (dalteparin) Arixtra (fondaparinux) Xarelto (rivaroxaban)
Oral investigational drugs* Apixaban
*Awaiting market approval.Vascular Disease Foundation Newsletter. Spring 2005; Volume 5, N2

Grape Seed Extract Horse Chestnut Seed Extract
Butcher’s Broom
Main Constituents:ResveretrolQuericiten
BlueberryRed WineElderberry
Sweet CloverPycnogenol

Sclerotherapy Radiofrequency Ablation (RFA) Endovenous Laser Treatments
(EVLT) Phlebectomy Stripping & Ligation
Before After
In practice, it is recommended that graduated compression therapy be worn
pre- and post- vein procedures

Bandages Intermittent Pneumatic Compression Devices Foot Pumps Portable Devices
(continuous enhanced circulation therapy)
Compression Therapy Support stockings, Medical compression stockings, or
Graduated compression stockings Anti-embolism stockings
Ramelet AA. Dermatol Surg. 2002;28:6-10.

Air compressor & inflatable sleeve For ARMS or LEGS
Gradient, segmental,
intermittent compression

SHORT STRETCH

Photos Compliments of Circ AidPhotos Compliments of Circ Aid

Improve blood flow velocity To restore blood flow velocity to
normal To reduce or prevent edema Prevent/treat venous
diseases
44

20 - 40%
50 - 80%
100%
Graduated CompressionIndicated for prevention and management of venous disorders in ambulating patients and wheel-chair bound patients
Picture obtained from http://www.newlook.com.sg/tedantiembolismstockings.asp. Accessed 09/02/10.
Graduated Compression Therapeutic Compression
Ranges: 15-20mmHg6 (class I) up to 50-60mmHg (class IV)
Utilized in the community setting, including assisted living facilities, long-term care facilities, and nursing homes
Commonly available as: Socks and stockings Calf-length, thigh-high, and
pantyhose styles Cotton and/or nylon fabrics and
yarns

Anti-embolism Stockings
“TEDS are for BEDS”
Therapeutic Compression Ranges: 18-8mmHg, 20-10mmHgUtilized in the hospital or nursing home setting For bed-ridden patients
Class A (8-15mmHg) compression reflects the standard in some countries but there is insufficient clinical evidence to support it’s use in practice. (European Prestandard, 2001)TEDS=Thromboembolic Deterrent Stockings
Anti-embolism StockingsIndicated for prevention of
thromboembolisms in recumbent patients

There is insufficient clinical evidence to support the clinical efficacy of compression pressures <15mmHg to support ambulatory patients. (European Prestandard, 2001)
“OTC” Medical Therapy (Prescription Recommended)
15-20mmHg 18-25mmHg 20-30mmHg 30-40mmHg 40+mmHg
• Tired, achy legs• Occupational or
evening edema• Leg discomfort
from prolonged standing/sitting
• Preventing pregnancy varicosities &swelling
• Predisposed risk• Reduce travel
swelling• Prevention of
traveler’s thrombosis
• Lower extremity edema in diabetic patients without contraindications and ABI >0.6
• Heavy, fatigued, aching legs
• Mild edema in lower extremities
• Mild varicosities w/ minimal edema
• Mild varicosities & pregnancy edema
• Post-procedure of small veins
• DVT prevention or management
• Moderate varicosities w/ mild-moderate edema ± pregnancy
• Post-procedure of larger veins
• CEAP C3, C4, C5, C6
• Recurrent or active venous ulceration
• DVT prevention or management
• DVT or PTS treatment
• Severe varicosities
• Severe edema• CEAP C4, C5,
C6• Recurrent
venous ulceration
• Severe post traumatic, fracture edema
• Severe PTS
A simple change of socks!!!A simple change of socks!!!

“OTC” Medical Therapy (Prescription Recommended)
15-20mmHg 18-25mmHg 20-30mmHg 30-40mmHg 40+mmHg
• Tired, achy legs• Occupational or
evening edema• Leg discomfort
from prolonged standing/sitting
• Preventing pregnancy varicosities &swelling
• Predisposed risk• Reduce travel
swelling• Prevention of
traveler’s thrombosis
• Lower extremity edema in diabetic patients without contraindications and ABI >0.6
• Heavy, fatigued, aching legs
• Mild edema in lower extremities
• Mild varicosities w/ minimal edema
• Mild varicosities & pregnancy edema
• Post-procedure of small veins
• DVT prevention or management
• Moderate varicosities w/ mild-moderate edema ± pregnancy
• Post-procedure of larger veins
• CEAP C3, C4, C5, C6
• Recurrent or active venous ulceration
• DVT prevention or management
• DVT or PTS treatment
• Severe varicosities
• Severe edema• CEAP C4, C5,
C6• Recurrent
venous ulceration
• Severe post traumatic, fracture edema
• Severe PTS
A simple change of socks!!!A simple change of socks!!!

Progressive arterial insufficiency Uncontrolled congestive heart failure Acute dermatitis, weeping dermatosis, cutaneous sepsis
Signs of infectionExtensive venous ulcerationSkin sensitivities or allergiesNeuropathyHistory of diabetesConfinement to bed or non-ambulatory use unless otherwise prescribed by the physician

True or False. Diabetic patients should not wear graduated compression socks.
A.True
B.False

Lower extremity edema is a common clinical finding in diabetic patients
Lack of reliable measures to objectively quantify edema makes it difficult to assess it’s prevalence in diabetic patients
Edema in diabetics is difficult to isolate and may have multiple etiologies
Brodovicz KG, et al. Clin Med Res. 2009;7(1-2):21-31.Fries R. MMW Fortschr Med. 2004;146(16):39-41.Powell AA, et al. Am Fam Physician. 1997;55(5):1721-6.

What features should a diabetic compression sock include?
A.At least 18-25mmHg
B.Is graduated in pressure above the calf
C.Flat-toe seam
D.Cushioned sole
E.Only C and E
F.All of the above

4-week pilot study N=18
Diabetes Lower extremity edema of the leg, foot, and ankle Ankle-brachial index (ABI) >0.6
Assess whether diabetic compression socks* can reduce LE edema in diabetic patients without compromising vascularity
Fitted for 4-7 pair of diabetic compression socks which were white, padded foot, and flat toe seam
LE=lower extremityDiabetic compression socks provided 18-25mmHg

Mean Foot Circumference
27.98
27.4227.6027.58 27.41

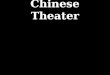
Mean Ankle Circumference
25.2824.32
24.14
24.3624.42
Statistically significant

Mean Calf Circumference
41.5940.32
41.1241.10 41.08
Statistically significant

31.20
29.50 29.3030.05
28.58
Cutaneous Edema

1.10
1.05
1.16
1.26
1.18
Safety and Efficacy of Mild Safety and Efficacy of Mild Compression (18-25mmHg) Therapy in Compression (18-25mmHg) Therapy in
Patients with Diabetes and Lower Patients with Diabetes and Lower Extremity EdemaExtremity Edema
Wu SC, Crews RT, Najafi B, et al. J Diabetes Sci Technol 2012 Vol 6 Issue 3
ABI

Mild graduated compression socks decreased swelling in diabetic patients with LE edema without compromising vascularity

Promotes circulation Fiber blend of cotton, acrylic, nylon, and elastic
Regular 100% wool or cotton socks are too tight on the foot, reduce circulation, and are not cool and do not keep the foot dry
Cushioned Regular socks do not provide comfort and protection
Flat seams Coarse seams on regular socks rub the foot and .
cause blisters and calluses to emerge
Feldman CB, et al. Diabetes Spectrum.14(2), 59-613Herring KM, et al. J Amer Pod Med Assn. 80, 63-70.

Pre-diabetic Newly diagnosed Edema Gestational diabetes No neuropathy ABI >0.6 without claudication
Diabetic patients a more likely to exercise when their legs feel good!

Key Benefits: • Designed for oversized legs •Made with Nano Bamboo Charcoal Fiber which is a natural deodorizer that absorbs odor causing agents and reduces microbial growth• Helps regulate skin temperature •Releases Infrared Rays that may promote blood circulation. • Padded heel and forefoot for extra comfort. • Ventilated airflow mesh on top of forefoot and instep.
Compression Level: 10-15mmHg up to 20-30mmHgStyle(s): Ankle, Crew, Merry Jane, Over the Calf Color(s): Black, Navy, Sand, White (Not all styles in all colors) Sizing based on shoe size, availability varies by productPrice: $9.95-$12.95

Key Benefits: •Clinically proven to reduce swelling and improve circulation•American Podiatric Medical Association (APMA) Seal of Approval•Non-binding calf band•Flat toe seam•Extra padding on foot•DriRelease fiber blend for moisture wicking, odor control, and softness•Latex free•True graduated compression
Compression Level: 18-25mmHgStyle(s): Over the Calf Color(s): White Sizing ankle & calf measurementsPrice: $30-40

Silver Sole Key Benefits:
• Unisex. Sized by shoe size.• Silver knitted for antimicrobial benefits• Pillowed sole adds cushion to reduce blistering and callous buildup• Mid-foot compression to prevent sock bunching
Compression Level: 12-16mmHgSize(s): S, M, L, XL Style(s): Anklet, Low Cut, Crew Length, Knee-HighColor(s): Black, White, Pink Price: $16-$17

Key Benefits: •Non-irritating, smooth toe seam•Extra padding in the foot, heel and toe•Moisture-wicking acrylic multi-fiber yarns•Antibacterial, antifungal finish
Compression Level: 8-15mmHgStyle(s): Knee Length, Crew Length, Mini-Crew LengthColor(s): White, Black, Navy, Brown/ Mini-Crew white only Price: $9-$12.99 or 3/$34.50

“Your labs show you have diabetes. I know your legs hurt
but you need to exercise to improve your circulation,
and start these medications!”




Average Prescription Margins in 2009 for an Independent Pharmacy were 6-12%
(margins vary based upon brand vs. generic medication and cash vs. insurance reimbursement)
How is the average independent pharmacy combating tight margins when
93% of their revenue is from Prescription Drugs?
In addition to offering retail items on the front-end…
SOME dramatically increase # of prescriptions filled/day!MINIMAL PROFIT INCREASE…PHARMACY CLOSES
OTHERS find a Niche Service with wide margins!HUGE PROFIT INCREASE…PHARMACY SURVIVAL
Gude S. Drug Topics. 2007 Oct 22. 70

71
School Supplies Pens Pencils Paper Book Bags
Toys Greeting Cards Magazines Candy Hairbows Household Items
Paper Towels Toilet Tissue Laundry Detergent All Purpose Cleaner Trash Bags

Premium Brands Jobst SIGVARIS Mediven Juzo
Economy Brands Futuro Activa Bellhorn Bauerfeind Loving Comfort Therafirm Truform Many private label
brands

How Many Pregnant Women Per Month? 10 6 # pairs per year purchased $30 Retail Per Pair (Avg)
Margin 50%
120 Per Year
720 pairs per year
$21,600 in Sales
$10,800 in GP $$$

How many pregnant patients enter your pharmacy monthly? 20
If, half purchased
two pair every six months 480 pairs sold per year
50% margin
$7,200 in GROSS PROFIT $14,400 in SALES

How many pregnant patients enter your pharmacy monthly? 40
If, half purchased
two pair every six months 960 pairs sold per year
50% margin
$19,200 in GROSS PROFIT $38,400 in SALES

What type of products and services would you want from a graduated compression manufacturer?
A.Business support
B.Quality product
C.Affordability
D.Precise sizing to fit patients
E.All of the above

Business partnership with company and sales representative Doctor detailing Marketing support and literature Health and wellness fairs Education and training
Clinically studied products, medically efficacious Product quality Safe and properly fit garments

Parent company to many subsidiaries supplying durable medical equipment items
Manufacturer of orthopedic soft goods & bracing products including: casting, bracing, wound care, and compression stockings
Premium Line
Economy Line
Premium Line
Economy Line

Manufacture products ranging from medical hosiery to bandages.
#1 physician recommended brand in the United States
Specialize in custom made garments

World’s largest, physician founded, Ready to Wear graduated compression stocking company
Global leader & “Compression Specialists” Precise fit sizing system (PFS2) accommodates
patients with an average or full sized calf with a short or long leg

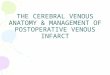
All medical hosiery is manufacturered with double-covered yarns NOT bare spandex
Only company with an in-house pharmacist to manage the Pharmacy Relations Department to address pharmacy business support needs.
Covered Spandex/Lycra
2nd covering(S-twist)
1st covering(Z-twist)

A subsidiary of 3M Widely recognized manufacturer of economical
braces, supports, and compression stockings Available in most national & regional
chain/franchise locations

How can pharmacists help their patients to prevent and/or manage chronic venous disease?
A.Offer clinically-based recommendations to patients regarding graduated compression therapyB.Measure patients and fit them into a graduated compression garment that precisely fitsC.Monitor patients compliance and comfortability in wearing graduated compression therapyD.All of the above

Webb JA. Drug Topics. June 2010; Vol 154(6): 25-28

Ask your patients about their medical history Ask your patients about their compression history Recommend compression therapy to your patients Counsel patients and physicians about the medical
benefits of compression therapy Educate your patient Discuss and emphasize the need for compliance


1.4.3.1: Recommend that mechanical methods of thromboprophylaxis be used primarily in patients at high risk for bleeding, or possibly as an adjunct to anticoagulant-based thromboprophylaxis
Geerts WH CHEST 2008;133: 381S-453SKearon C, et al. CHEST 2008; 133;454S-545S
2.1.4: For general surgery patients with multiple risk factors for VTE, a pharmacological method should be combined with a mechanical method
2.1.5: For general surgery patients with a high risk of bleeding, we recommend the optimal use of mechanical thromboprophylaxis with properly fitted GCS or IPC. When the high bleeding risk decreases, we recommend that pharmacologic thromboprophylaxis be substituted for or added to the mechanical thromboprophylaxis.

3.1.1: Patient with symptomatic
proximal DVT, we recommend use of an elastic compression stocking with an ankle pressure gradient of 30-40 mmHg. Compression therapy, should be started after starting anticoagulant therapy and should be continued for a minimum of 2 years, and longer if patients have symptoms of PTS.
7.2.8: For all pregnant women with previous DVT, we suggest the use of GCS both antepartum and postpartum.
Geerts WH CHEST 2008;133: 381S-453SKearon C, et al. CHEST 2008; 133;454S-545S

9.1: If there is a perceived high risk of VTE in long distance travelers (> 8 hours), we suggest the use of a properly fitted, below knee GCS, providing 15-30 mm Hg of pressure at the ankle, or a single dose of LMWH injected prior to departure
Geerts WH CHEST 2008;133: 381S-453S

93 male workers with CVI from 14 meat factories randomized to the intervention (n=43; 20-30mmHg compression stockings or floor mats) or control (n=50) to assess the effect of compression stockings vs. floor mats on leg edema and pain
Leg pain was measured via subjects subjective complaints of tired legs and leg pain
Leg edema (volume) by Doppler ultrasound (standing) and light reflection rheography (sitting)
Krijen R, et al. J Occu Environ Med. 1997;39(9):889-894
Control Group Compression Rubber Mat
Tired Legs No Difference P<0.005 P<0.01
Leg Pain No Difference P<0.05 No Difference
Volume Change No Difference P<0.05 No Difference

Mr. Little John is a 34 y.o. male and regular patient at your pharmacy. Today he presents with a new prescription for Coumadin 3mg daily. During his ‘pick up’ consultation you learn that he recently had a DVT and spent the past two weeks in the local hospital and wore TEDS during his hospital stay. You notice that he is still wearing his TED hose and he tells you that he has never had to wear compression therapy but his doctor told him that he will need to wear them daily while on Coumadin therapy. He is ambulating, intends to resume his normal daily routine and daily exercise schedule. Per CHEST guidelines and compression indications, do you agree with the Mr. Little John’s physician’s recommendations?

Per CHEST guidelines and compression indications, what compression level would you recommend for Mr. Little John?
A.8-15mmHg
B.15-20mmHg
C.20-30mmHg
D.30-40mmHg
E.Nothing, consult physician first

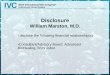
Following an in-depth dialogue with Mr. Little John, you both decide to switch his compression therapy from TEDs to graduated compression therapy. You now measure Mr. Little John and determine his measurements to be:
Shoe Size: 9.5
Ankle Circumference: 9 inches
Calf Circumference: 16 inches
Calf Length: 16.5 inches

1
2
3
Ankle Circumference
Calf Circumference
Calf Length

4
Thigh Circumference
Leg Length
5

You have three brands of graduated compression garments in stock – Futuro, Juzo, and SIGVARIS. Utilize Mr. Little John’s measurements to determine which size of each brand you would place him into.


1. Ankle circumference 2. Calf circumference 3. Calf length

9”9”9”9”
16.5”16.5”16.5”16.5”
16”16”16”16”

How old is the patient? What co-morbid conditions does the patient have? How compliant will this patient be with the recommended level of
compression? What type of lifestyle does the patient live? What type of work does the patient perform on a daily basis? What type of shoe is commonly worn? What type of venous disorder(s) does the patient have? What area of the leg requires compression? Do the toes need to be monitored during treatment?

For sure your patient will say – or be thinking…” I HATE U”!
STOCKINGS ARE:
Too Hot Too hard to Apply and remove Too Tight Too Expensive Too Ugly
HOW WILL YOU RESPOND?
101

Too Hot Recommend cool and comfortable cotton or other breathable fabrics (i.e., microfibers)
Too Hard to Apply & Remove
Show patient how to use donning tools such as gloves, foot sleeves, and extensors
Too Tight Explain how compression works and that their legs will adjustDouble compression garments
Too Expensive Prove the value On average they cost <$0.60 per day “Medicine you Wear” No drug interactions Last 6-months or longer Non compliance ± medications can cost thousands per year!Some raw materials provide easier donning, more durability, less shininess, and stay on better!
Too Ugly Show the patient “NEW” fashion forward productsSuggest camouflaging the sock or stocking under their everyday socks and stockings

Cost is dependent on the severity of venous disease, with indirect cost rising sharply as disease severity increases
Estimated venous ulcer cost per-episode can exceed $40,000
Estimated 2 million workdays per calendar year are lost due to chronic venous ulcers
Rudolph DM, et al. J Wound Ostomy Continence Nurs 1998; 25: 248-55.

Seifert R. JMCP. 2008 Jul;14(6 S-a):S24-S27.

Medication Class
Intervention Opportunity
Medications
Anticoagulants DVT, PE, or PTS
Coumadin (warfarin), Lovenox (enoxaparin), Arixtra (fondaparinux)
Antiemetics Travelers-related thrombosis
Bonine or Antivert (meclizine), Phenergan (promethazine), Zofran (ondansetron), Transderm Scop (scopalamine), Dramamine (dimenhydrinate)
Prenatal Vitamins
Pregnancy-related leg edemaPregnancy-related varicose veins
Prenatal DHA, Prenate Advance, NataChew, Prenate Elite, Nestabs FA
ANY PRENATAL VITAMIN

Identify candidates for prophylactic graduated compression socks and stockings
Consult patients on graduated compression socks and stockings
Encourage appropriate use and compliance of graduated compression socks and stockings
Implement safe and effective monitoring of venous disease patients

Dick Bradley, QS/1 Consulting Services

Name, TitlePractice Site AddressCity, State Zip Code
Phone NumberEmail Address