Embed Size (px)
Citation preview
Onkologie 2014Stefan Kubicka

Vorsorge
Supportive Therapie
Optimierte Systemtherapie
Personalisierte Therapie
Immuntherapie
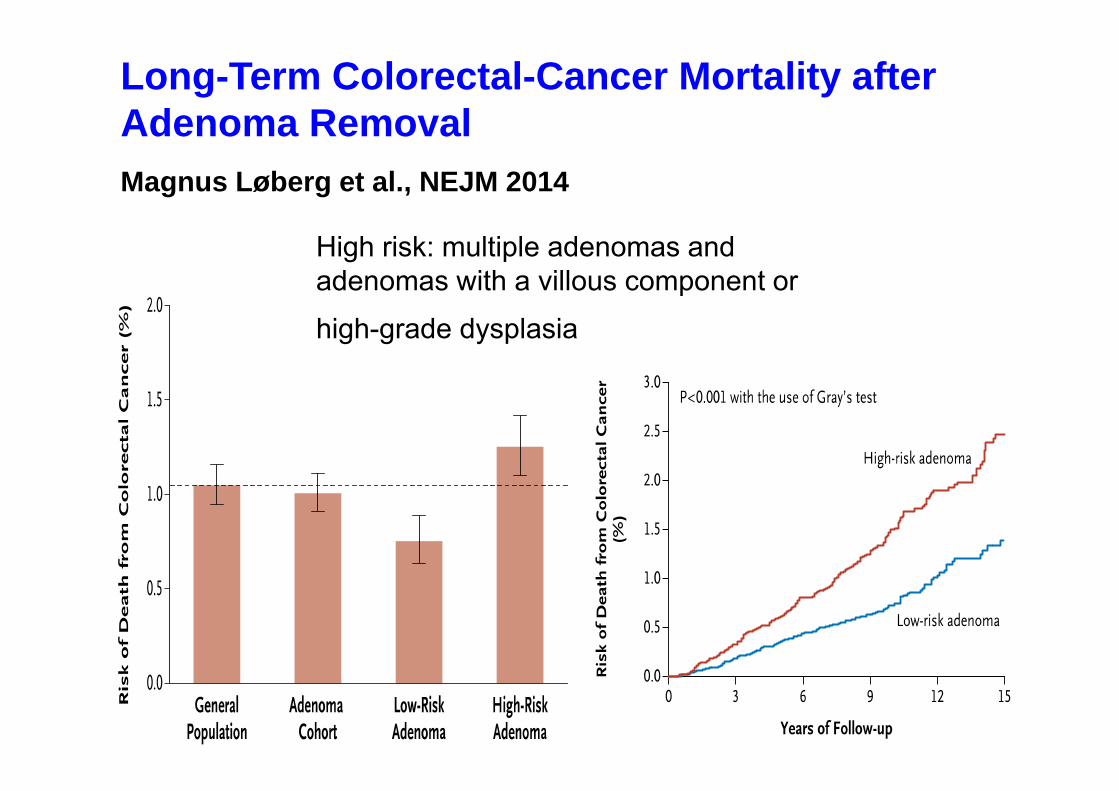
High risk: multiple adenomas andadenomas with a villous component or
high-grade dysplasia
Long-Term Colorectal-Cancer Mortality after Adenoma RemovalMagnus Løberg et al., NEJM 2014
50-74 y; Screening interval 4 years
Measurement of prostate-specific antigen (PSA) in serum, witha cutoff of 3·0 ng/mL or more, was the main screening test andindication for biopsy (an ancillary test was used for men withPSA 3·0–3·9ng/mL).
Sextant biopsies were initially recommended for screen-positive men
Screening and prostate cancer mortality: results of theEuropean Randomised Study of Screening for ProstateCancer (ERSPC) at 13 years of follow-upFritz H Schröder, J et al., Lancet Oncology 2014
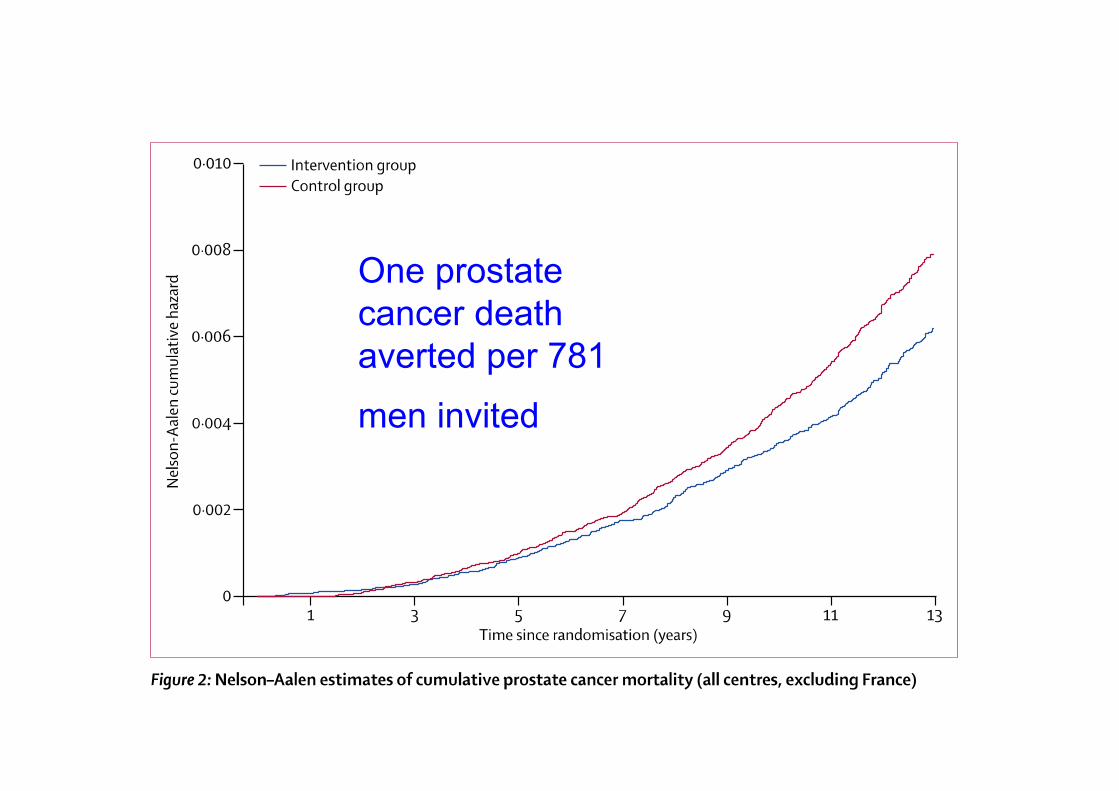
One prostatecancer deathaverted per 781
men invited

Vorsorge
Supportive Therapie
Optimierte Systemtherapie
Personalisierte Therapie
Immuntherapie
Oral rivaroxaban versus enoxaparin with vitamin K antagonist for the treatment of symptomatic venous
thromboembolism in patients with cancer (EINSTEIN-DVT and EINSTEIN-PE): a pooled subgroup analysis of two
randomised controlled trialsMartin H Prins, et al., Lancet Hematology 2014
Rivaroxaban (15 mg twice daily for 21 days, followed by 20 mg once daily)
Standard therapy (enoxaparin 1·0 mg/kg twicedaily and warfarin or acenocoumarol)
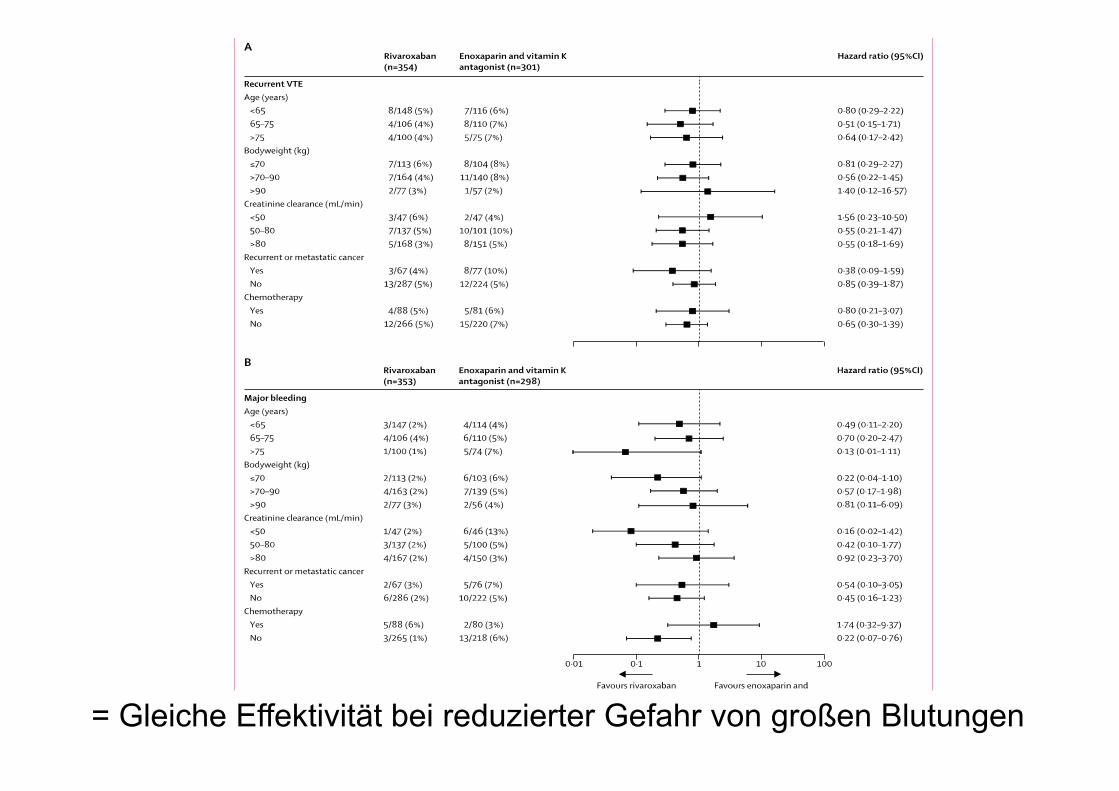
= Gleiche Effektivität bei reduzierter Gefahr von großen Blutungen
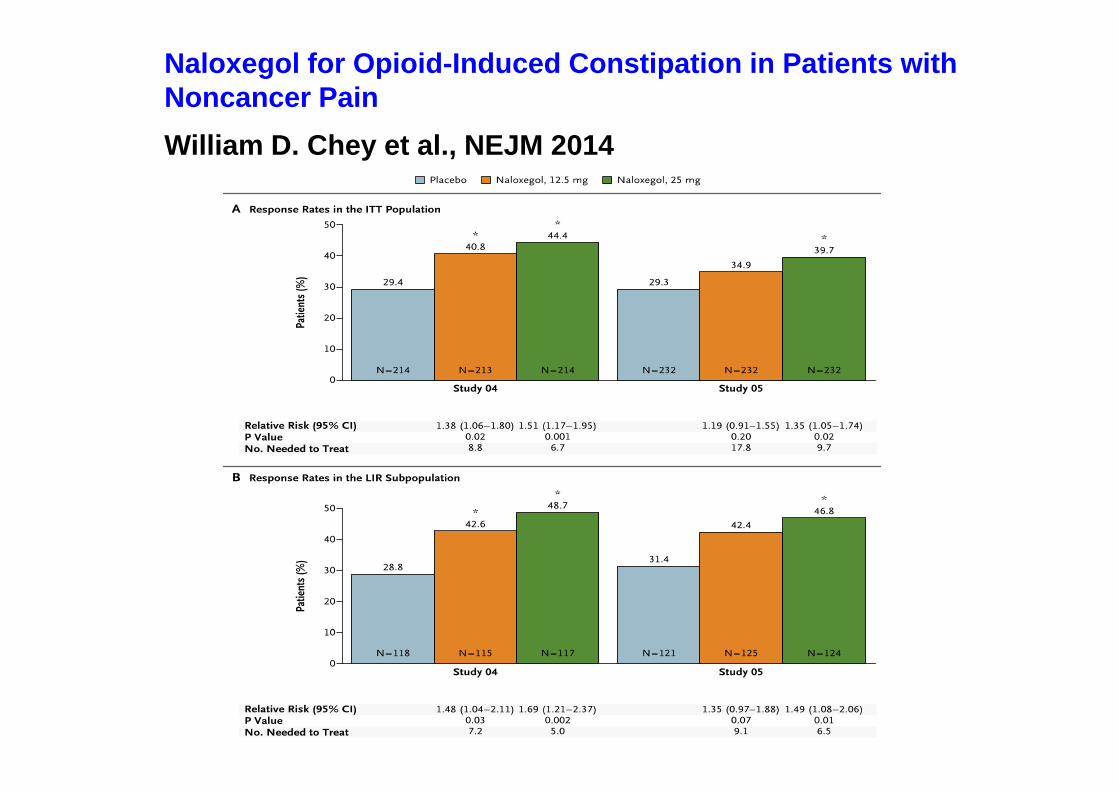
Naloxegol for Opioid-Induced Constipation in Patients withNoncancer PainWilliam D. Chey et al., NEJM 2014
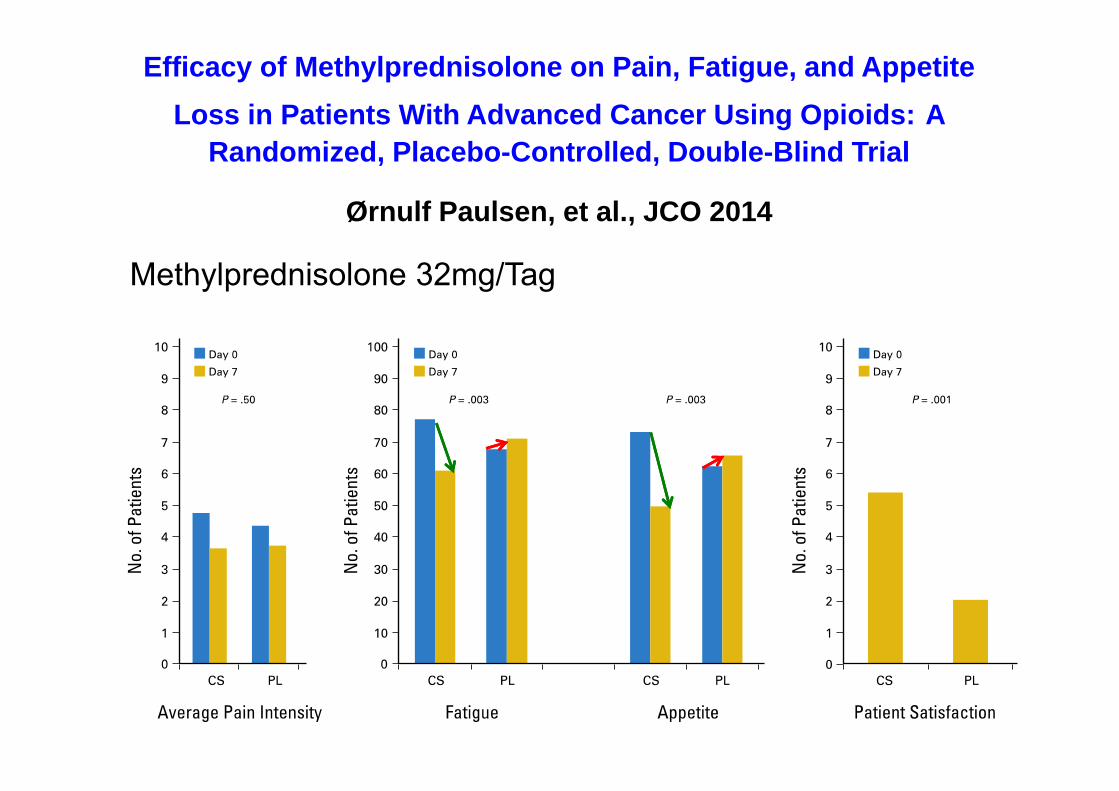
Efficacy of Methylprednisolone on Pain, Fatigue, and Appetite Loss in Patients With Advanced Cancer Using Opioids: A
Randomized, Placebo-Controlled, Double-Blind Trial
Ørnulf Paulsen, et al., JCO 2014
Methylprednisolone 32mg/Tag
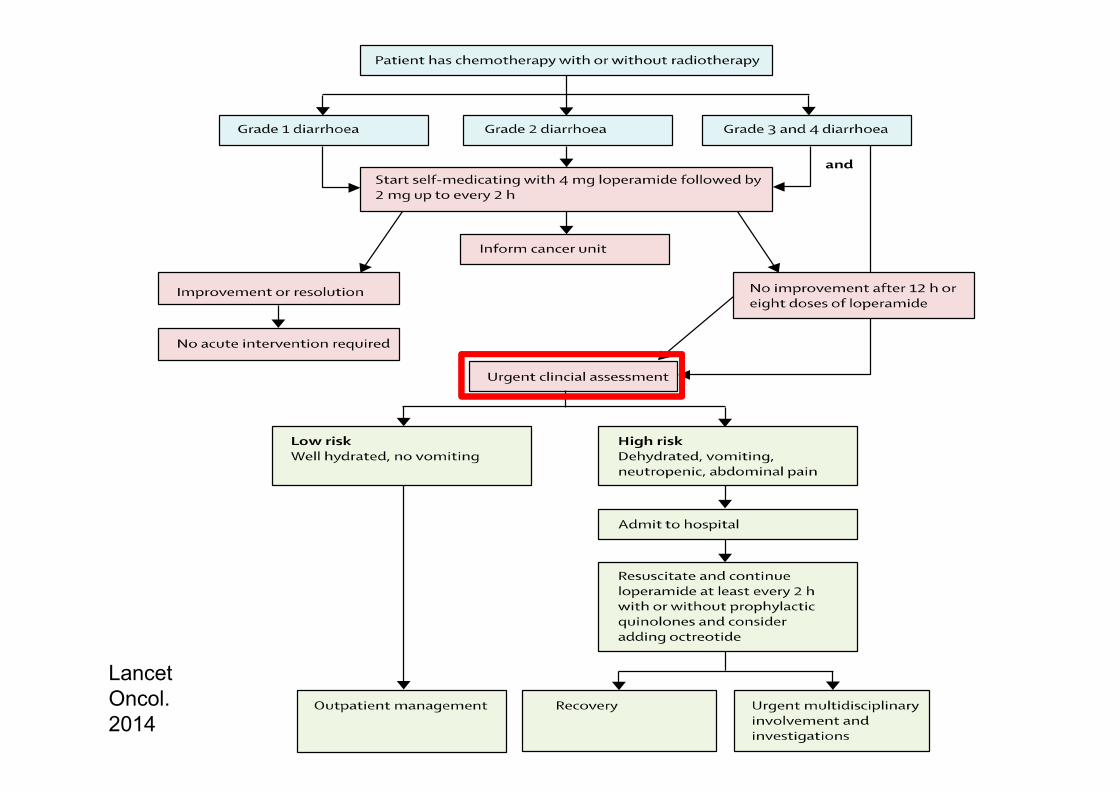
LancetOncol.2014

Vorsorge
Supportive Therapie
Optimierte Systemtherapie
Personalisierte Therapie
Immuntherapie
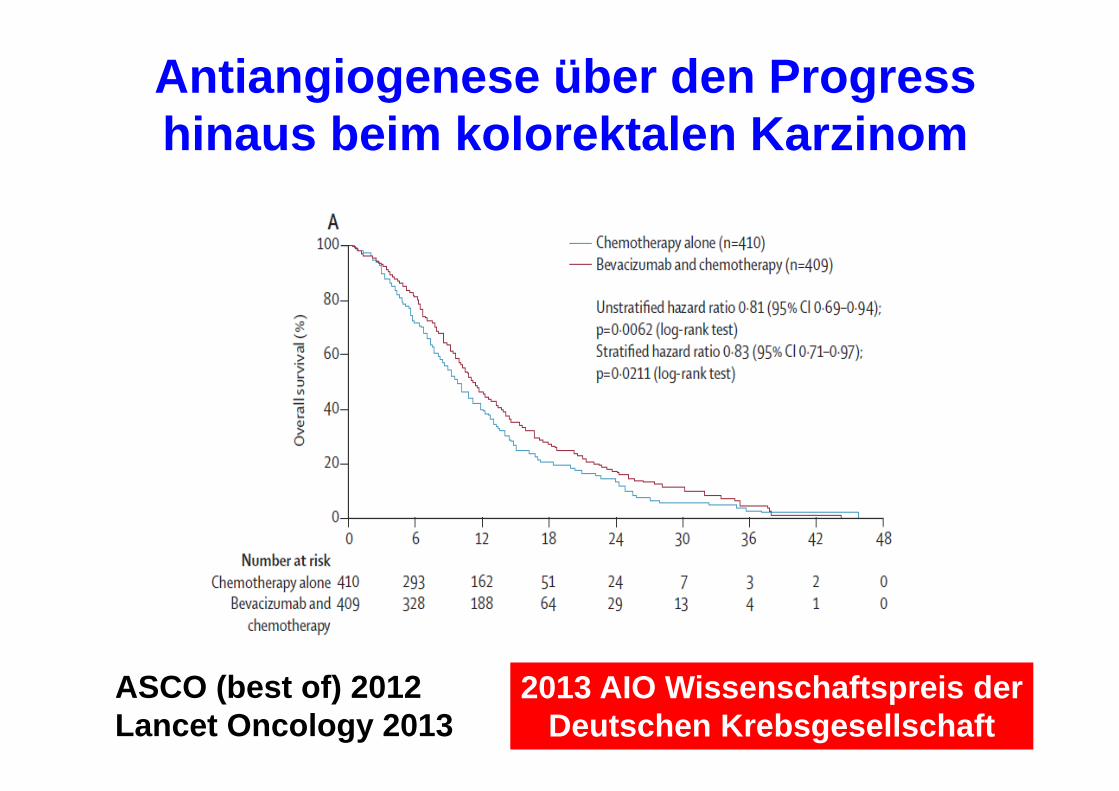
ASCO (best of) 2012Lancet Oncology 2013
2013 AIO Wissenschaftspreis der Deutschen Krebsgesellschaft
Antiangiogenese über den Progress hinaus beim kolorektalen Karzinom
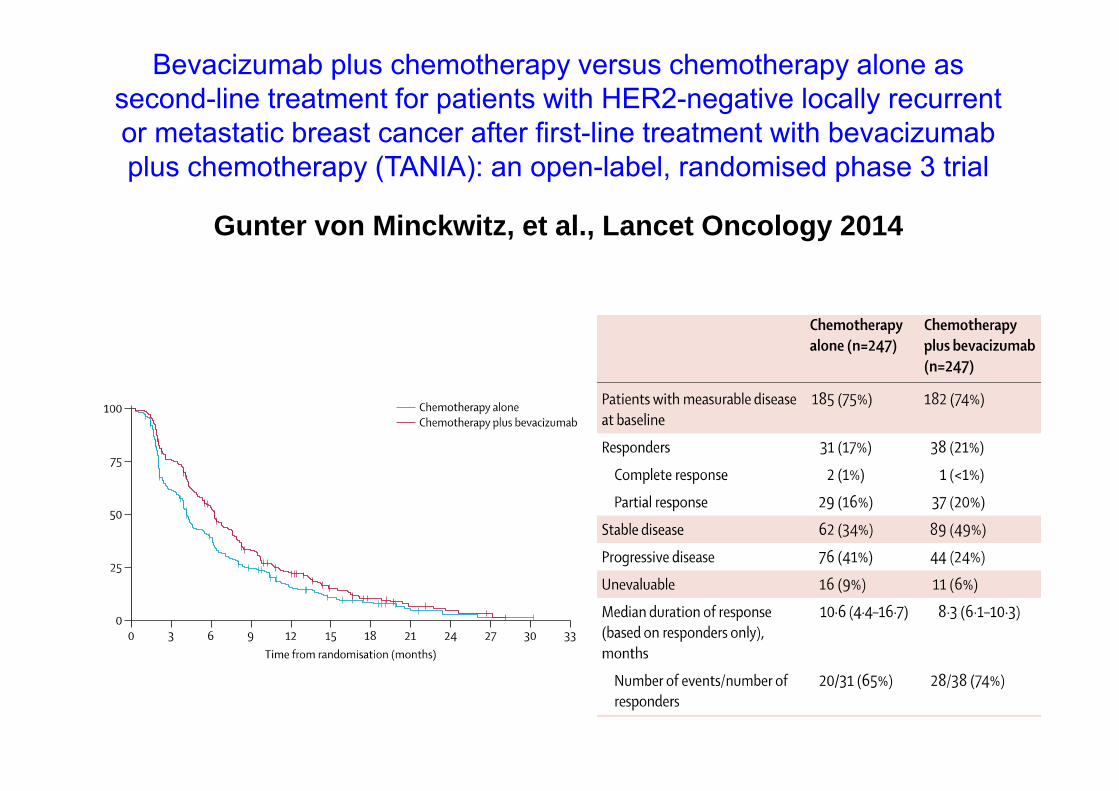
Bevacizumab plus chemotherapy versus chemotherapy alone assecond-line treatment for patients with HER2-negative locally recurrentor metastatic breast cancer after first-line treatment with bevacizumabplus chemotherapy (TANIA): an open-label, randomised phase 3 trial
Gunter von Minckwitz, et al., Lancet Oncology 2014

Vorsorge
Supportive Therapie
Optimierte Systemtherapie
Personalisierte Therapie
Immuntherapie
• Koronare 3-Gefäßerkrankung mit mittelgradig reduziertersystolischer linksventrikulärer Pumpfunktion (EF 45 %)- Z.n. BMS-Implantation Ramus marginalis 1 2006- Z.n. BMS-Implantation RPLS 08/2007- Z.n. PTCA und DES-Implantation der proximalen
RIVA am 06.09.2013• Persistierendes Vorhofflimmern
- CHA2DS2-VASc-Score 6 Punkte- Antikoagulation mit ASS und Clopidogrel, früher
Marcumar®-Therapie• Z.n. selbstlimitierende ventrikuläre Tachykardie• Arterielle Hypertonie• Insulinpflichtiger Diabetes mellitus Typ 2 (ICT, HbA1c-Wert
aktuell 6,2%Hb)- Diabetische Nephro- und Polyneuropathie
• Diabetisches Fußsyndrom- Ulcus D3 rechts dorsal (1C) - Ulcus D1 und D2 links apikal, abgeheilt- Z.n. Amputation D4 und D5 rechts, abgeheilt- Mediasklerose
• CVRF: Ex-Nikotinabusus• pAVK Stadium IV
- Z.n. PTA A. fibularis rechts 07/2012• Chronische Niereninsuffizienz Stadium 2• Morbus Parkinson
83 Jahre AEG Tumor T4, N1, M1 (Lunge)
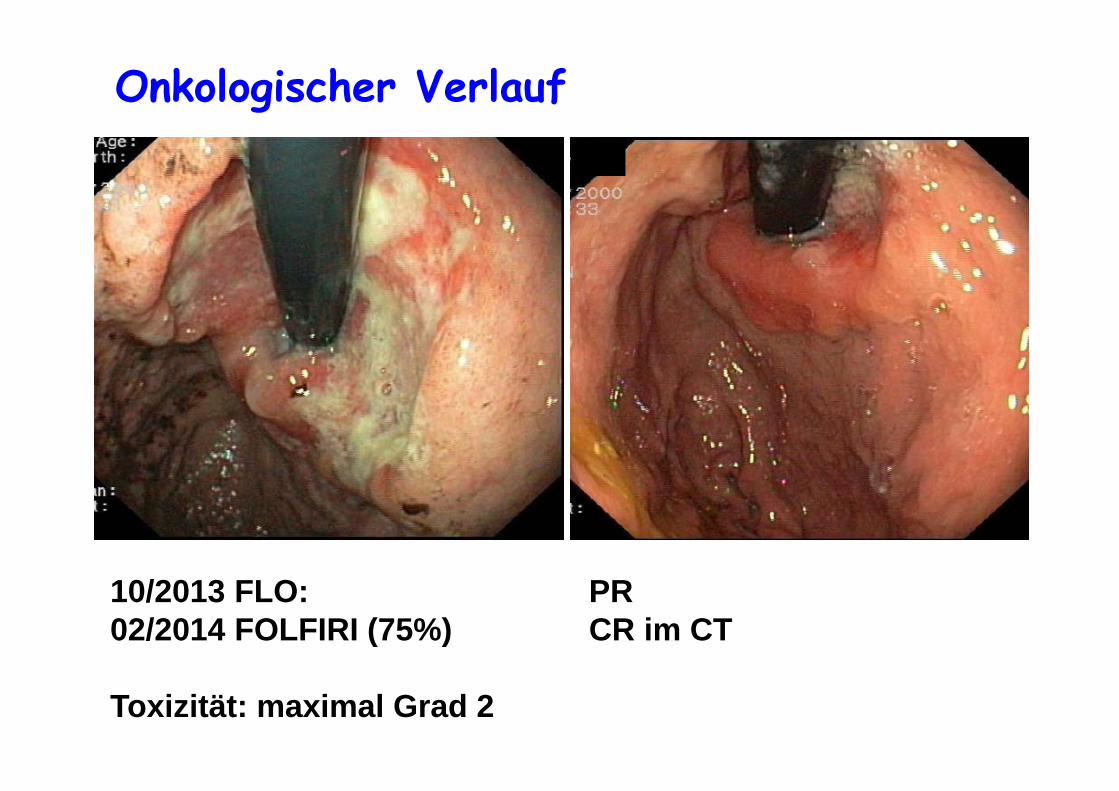
Onkologischer Verlauf
10/2013 FLO: PR02/2014 FOLFIRI (75%) CR im CT
Toxizität: maximal Grad 2


Bestes Ansprechen auf Crizotinib nach Patient
80
60
40
20
0
–20
–40
–60
–80
–100Verä
nder
ung
der T
umor
größ
e vs
. Aus
gang
swer
t (%
)
PD PRSD CR
–30%
10 20 30 40 50 60 70 79Patient Nr.
Kwak et al. New Engl J Med. 2010;363:1693−03
RR: 57 %Tumorkontrolle: 87%
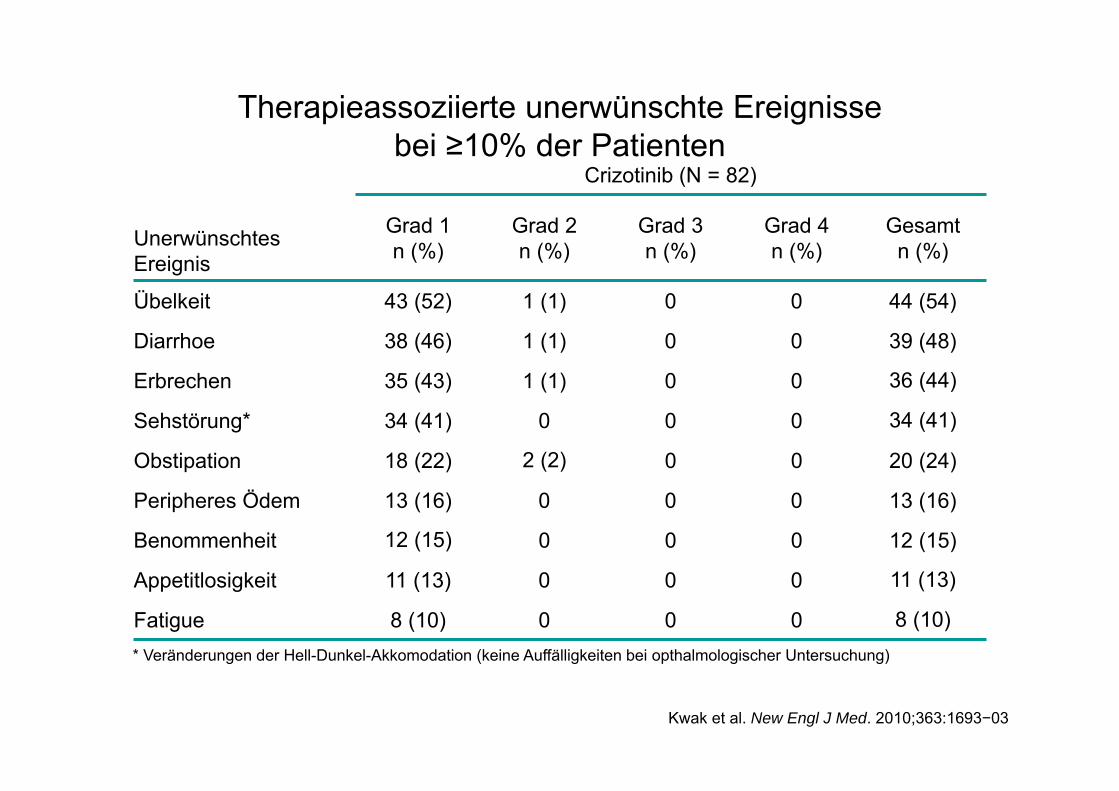
Crizotinib (N = 82)
Unerwünschtes Ereignis
Grad 1n (%)
Grad 2n (%)
Grad 3n (%)
Grad 4n (%)
Gesamtn (%)
Übelkeit 43 (52) 1 (1) 0 0 44 (54)
Diarrhoe 38 (46) 1 (1) 0 0 39 (48)
Erbrechen 35 (43) 1 (1) 0 0 36 (44)
Sehstörung* 34 (41) 0 0 0 34 (41)
Obstipation 18 (22) 2 (2) 0 0 20 (24)
Peripheres Ödem 13 (16) 0 0 0 13 (16)
Benommenheit 12 (15) 0 0 0 12 (15)
Appetitlosigkeit 11 (13) 0 0 0 11 (13)
Fatigue 8 (10) 0 0 0 8 (10)* Veränderungen der Hell-Dunkel-Akkomodation (keine Auffälligkeiten bei opthalmologischer Untersuchung)
Therapieassoziierte unerwünschte Ereignisse bei ≥10% der Patienten
Kwak et al. New Engl J Med. 2010;363:1693−03
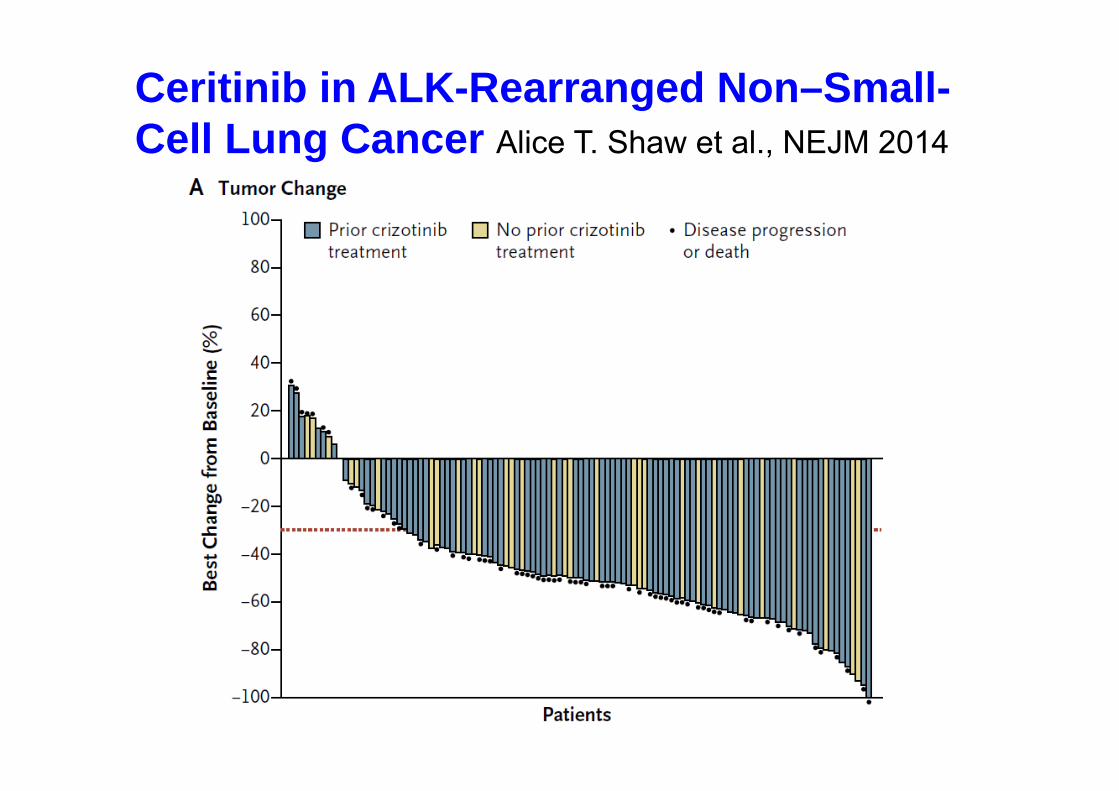
Ceritinib in ALK-Rearranged Non–Small-Cell Lung Cancer Alice T. Shaw et al., NEJM 2014
Kompetenz in Medizin und Pflege
KLINIKUM AM STEINENBERG
REUTLINGEN
ERMSTALKLINIK
BAD URACH
ALBKLINIK
MÜNSINGEN
ABL1(4,5,6,7)
ERBB4(3,4,6,7,8,9,15,23)
IDH1(4)
NRAS(2,3,4)
TP53(2,4,5,6,7,8,10)
AKT1(3,6)
EZH2(16)
IDH2(4)
PDGFRA(12,14,15,18)
VHL(1,2,3)
ALK(23,25)
FBXW7(5,8,9,10,11)
JAK2(14)
PIK3CA(2,5,7,8,10,14,19,21)
APC(16)
FGFR1(4,7)
JAK3(4,13,16)
PTEN(1,3,5,6,7,8)
ATM(8,9,12,17,26,34,35,36,39,50,54,55,56,59,61,63)
FGFR2(7,9,12)
KDR(6,7,11,19,21,26,27,30)
PTPN11(3,13)
BRAF(11,15)
FGFR3(7,9,14,16,18)
KIT(2,9,10,11,13,14,15,17,18)
RB1(4,6,10,11,14,17,18,20,21,22)
CDH1(3,8,9)
FLT3(11,14,16,20)
KRAS(2,3,4)
RET(10,11,13,15,16)
CDKN2A(2)
GNA11(5)
MET(2,11,14,16,19)
SMAD4(3,4,5,6,8,9,10,11,12)
CSF1R(7,22)
GNAQ(5)
MLH1(12)
SMARCB1(2,4,5,9)
CTNNB1(3)
GNAS(8,9)
MPL(10)
SMO(3,5,6,9,11)
EGFR(3,7,15,18,19,20,21)
HNF1A(3,4)
NOTCH1(26,27,34)
SRC(14)
ERBB2(19,20,21)
HRAS(2,3)
NPM1(11)
STK11(1,4,4/5,6,8)
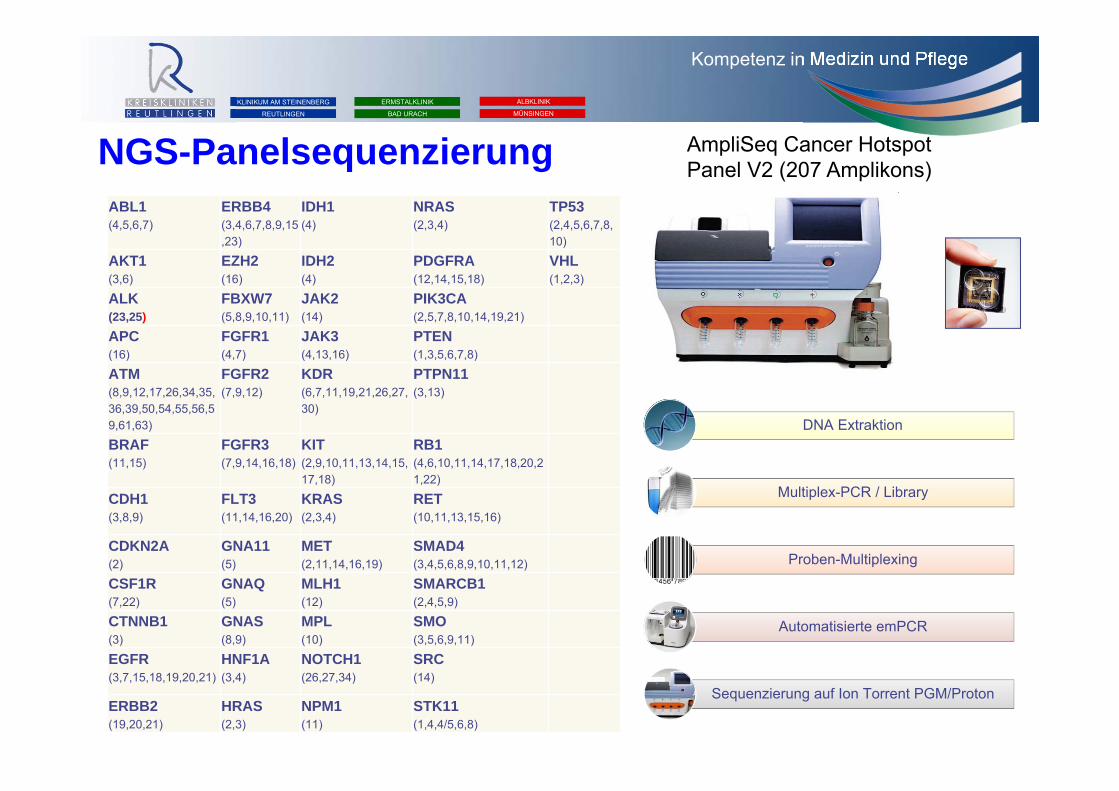
AmpliSeq Cancer Hotspot Panel V2 (207 Amplikons)
DNA Extraktion
Multiplex-PCR / Library
Proben-Multiplexing
Automatisierte emPCR
Sequenzierung auf Ion Torrent PGM/Proton
NGS-Panelsequenzierung
Kompetenz in Medizin und Pflege
KLINIKUM AM STEINENBERG
REUTLINGEN
ERMSTALKLINIK
BAD URACH
ALBKLINIK
MÜNSINGEN
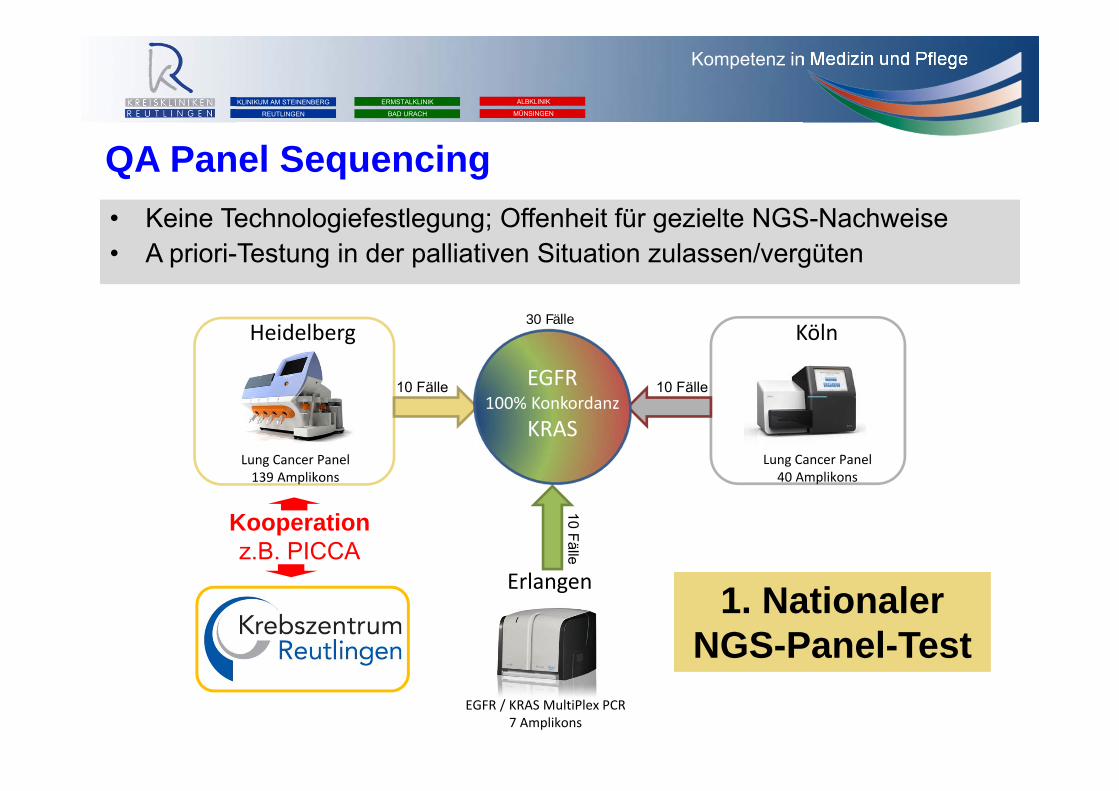
Heidelberg
Lung Cancer Panel139 Amplikons
Köln
Lung Cancer Panel40 Amplikons
Erlangen
EGFR / KRAS MultiPlex PCR7 Amplikons
EGFR100% Konkordanz
KRAS
10 Fälle 10 Fälle
10 Fälle
30 Fälle
QA Panel Sequencing• Keine Technologiefestlegung; Offenheit für gezielte NGS-Nachweise• A priori-Testung in der palliativen Situation zulassen/vergüten
1. Nationaler NGS-Panel-Test
Kooperationz.B. PICCA

Vorsorge
Supportive Therapie
Optimierte Systemtherapie
Personalisierte Therapie
Immuntherapie
Zeit
Anzahl der Übe
rlebe
nden
100%
50%
Zeit
Anzahl der Übe
rlebe
nden
100%
50%

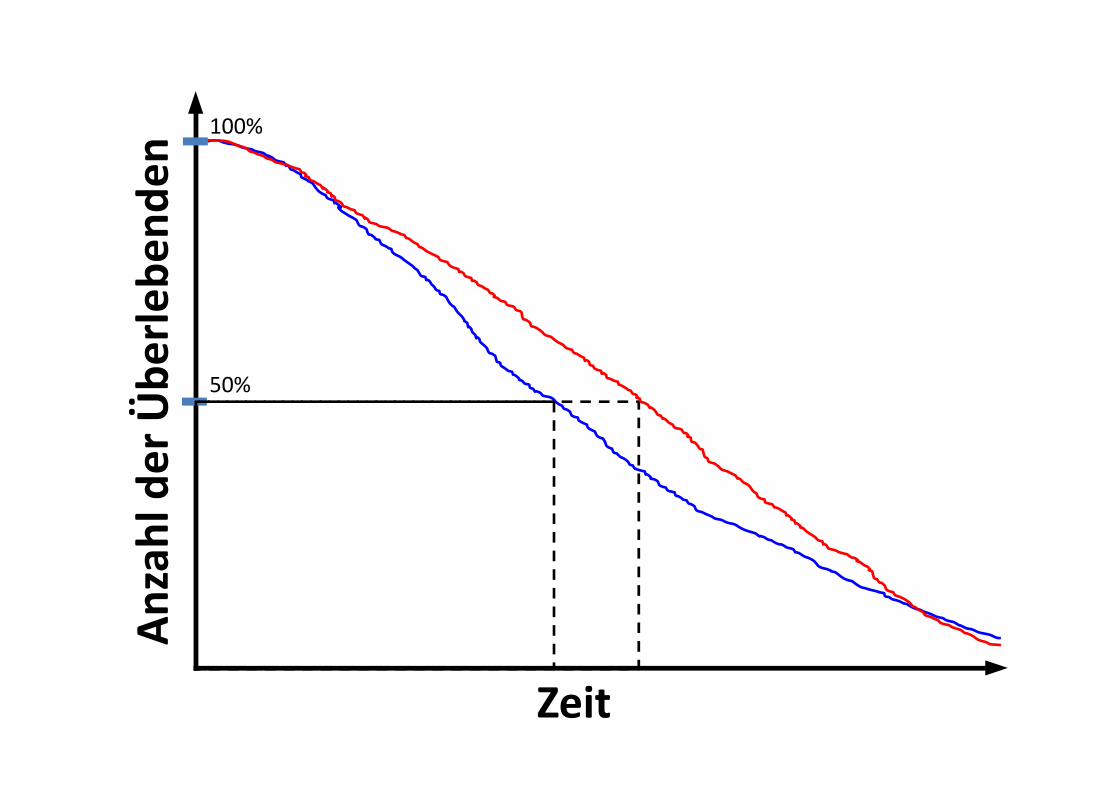
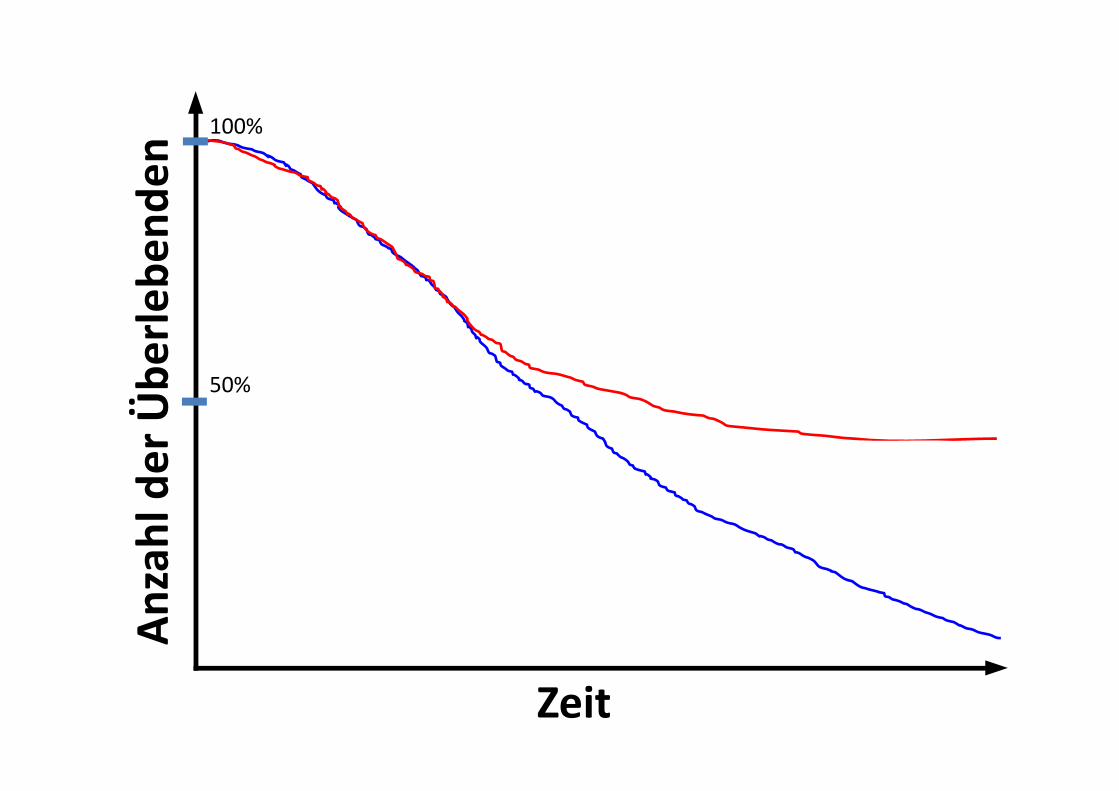
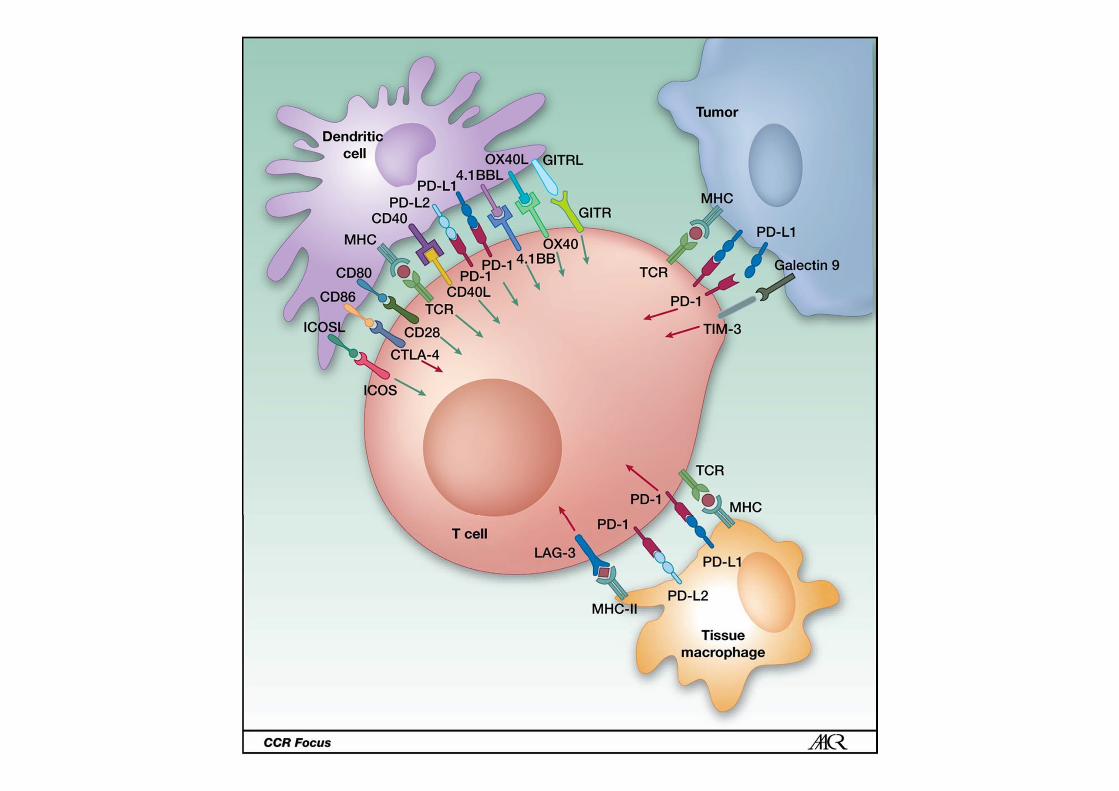
CTLA4 und PD1
Checkpoint Blockade
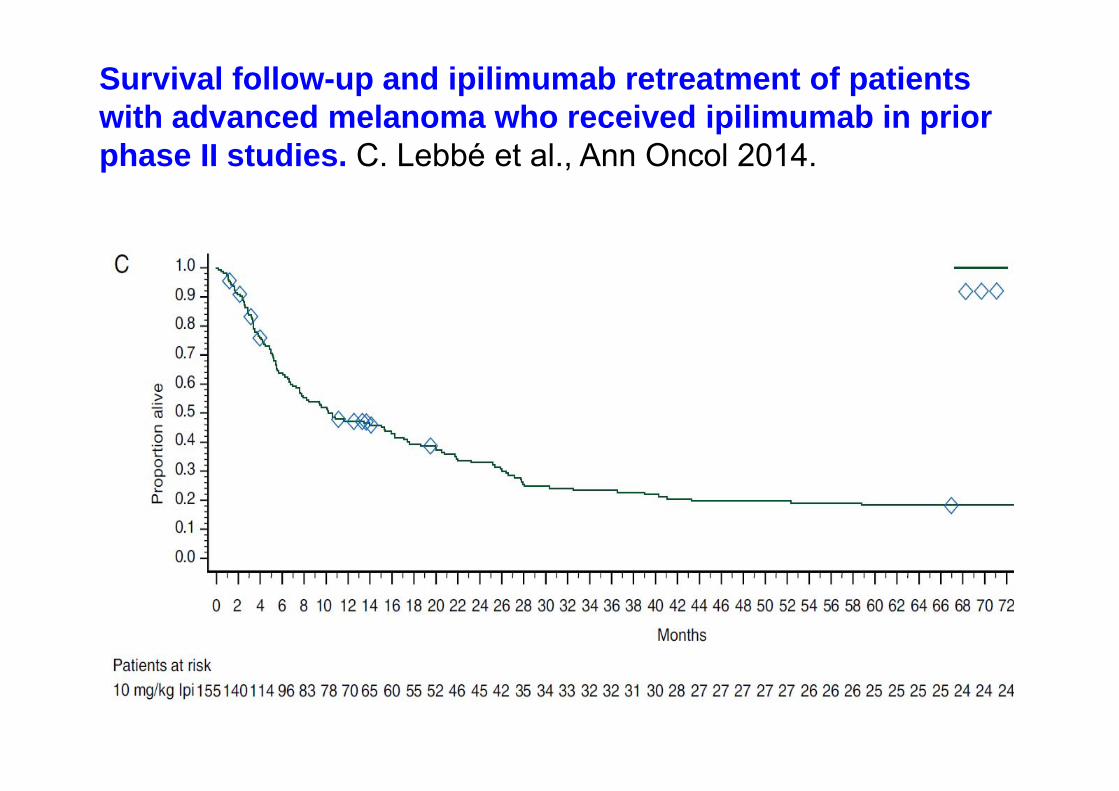
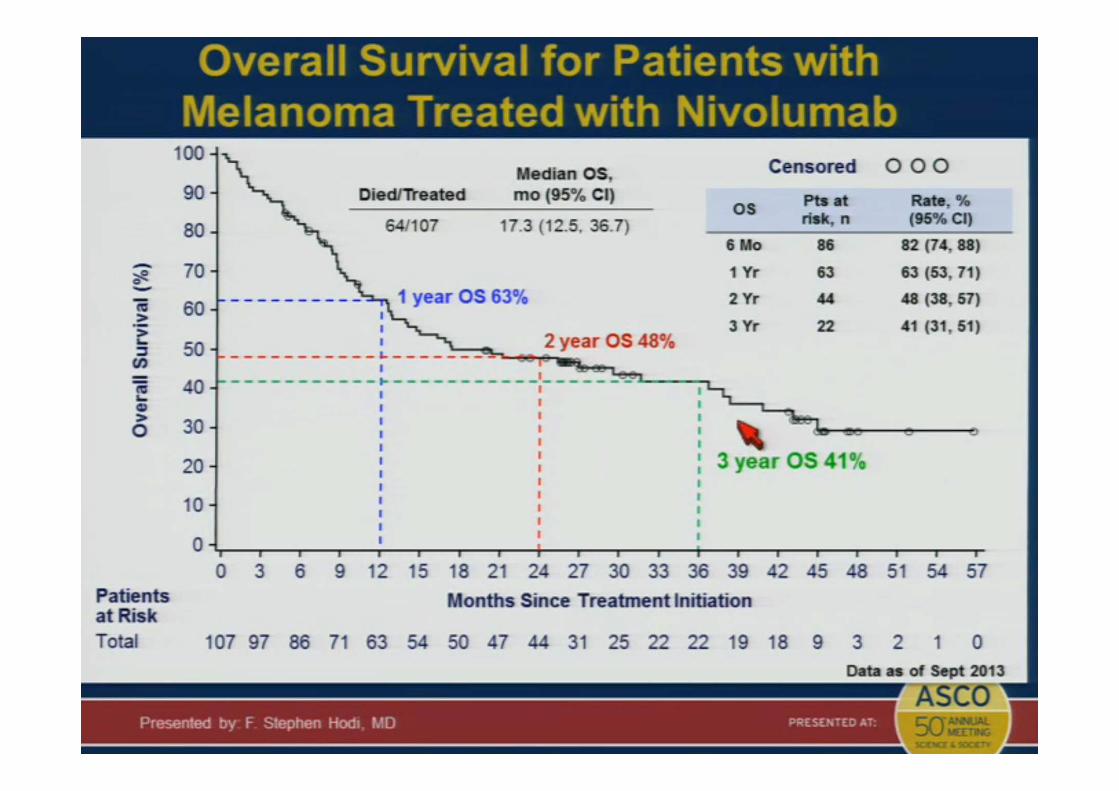
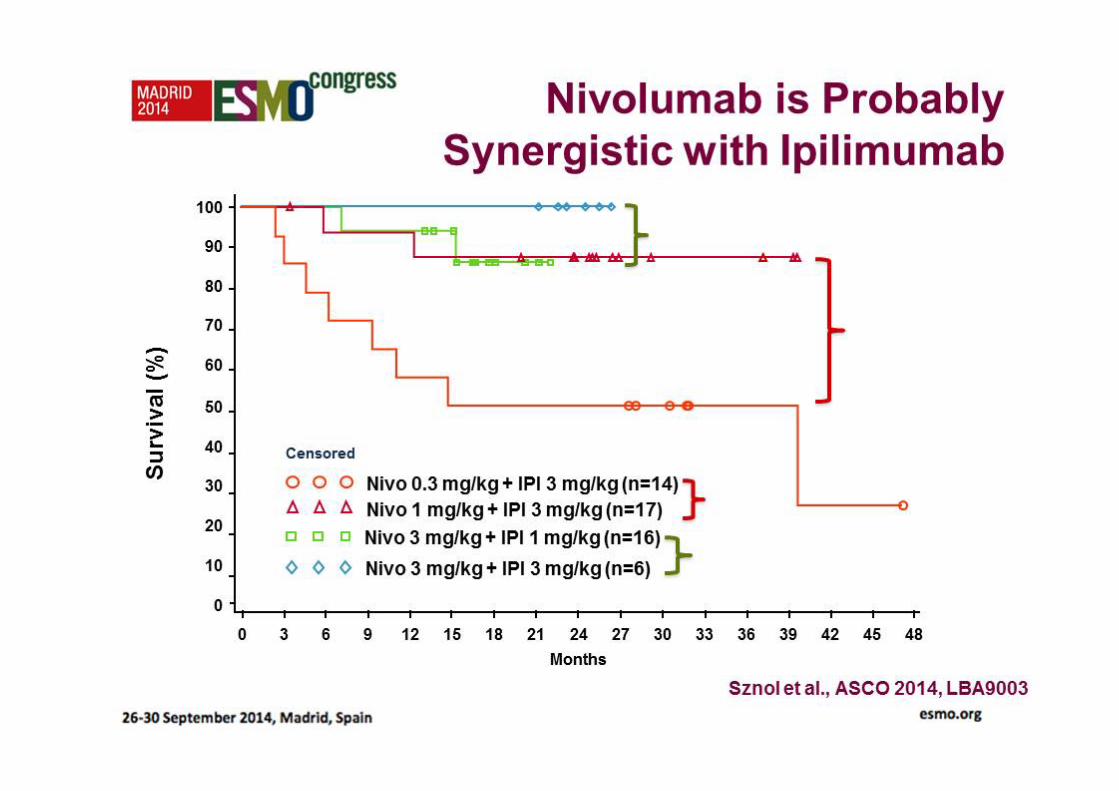
Survival follow-up and ipilimumab retreatment of patients with advanced melanoma who received ipilimumab in prior phase II studies. C. Lebbé et al., Ann Oncol 2014.
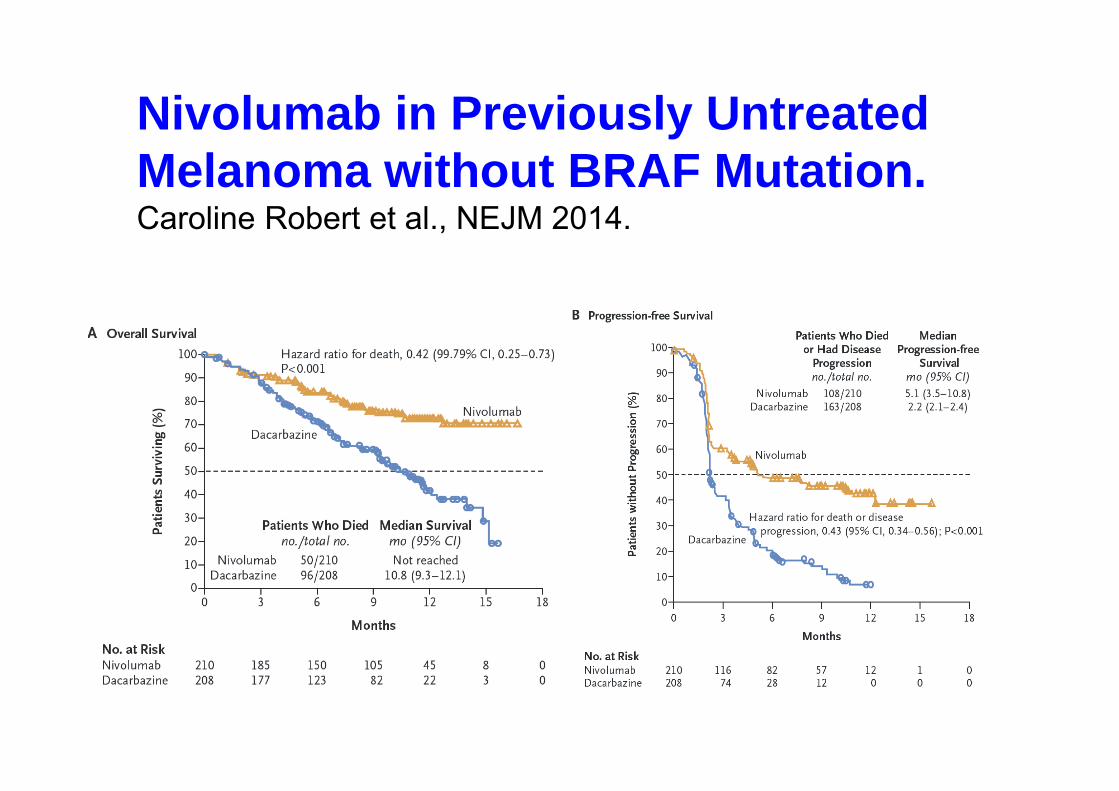
Nivolumab in Previously Untreated Melanoma without BRAF Mutation.Caroline Robert et al., NEJM 2014.
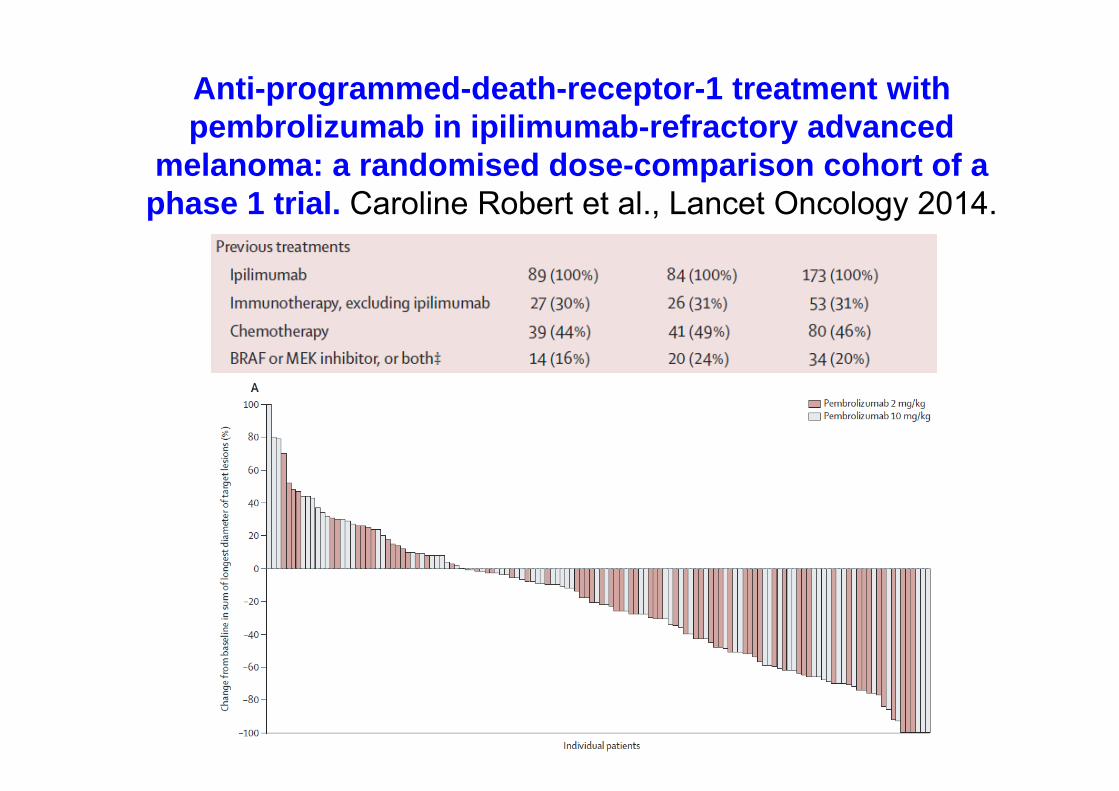
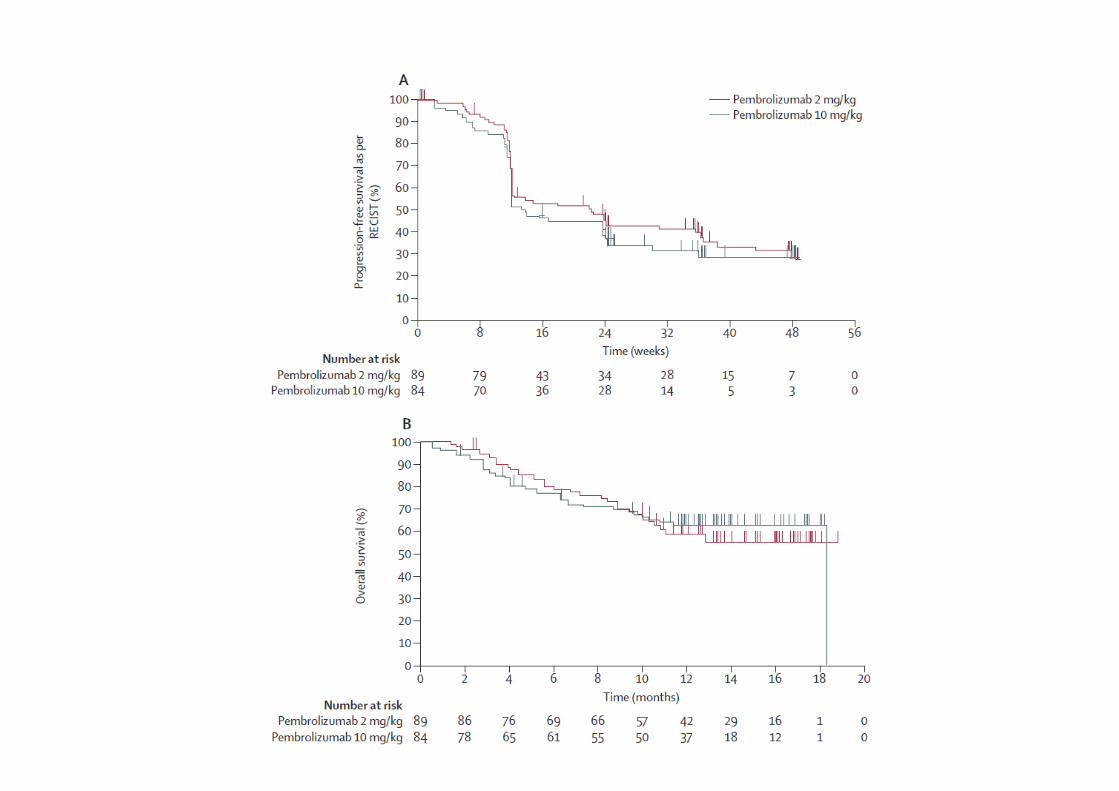
Anti-programmed-death-receptor-1 treatment withpembrolizumab in ipilimumab-refractory advanced
melanoma: a randomised dose-comparison cohort of aphase 1 trial. Caroline Robert et al., Lancet Oncology 2014.
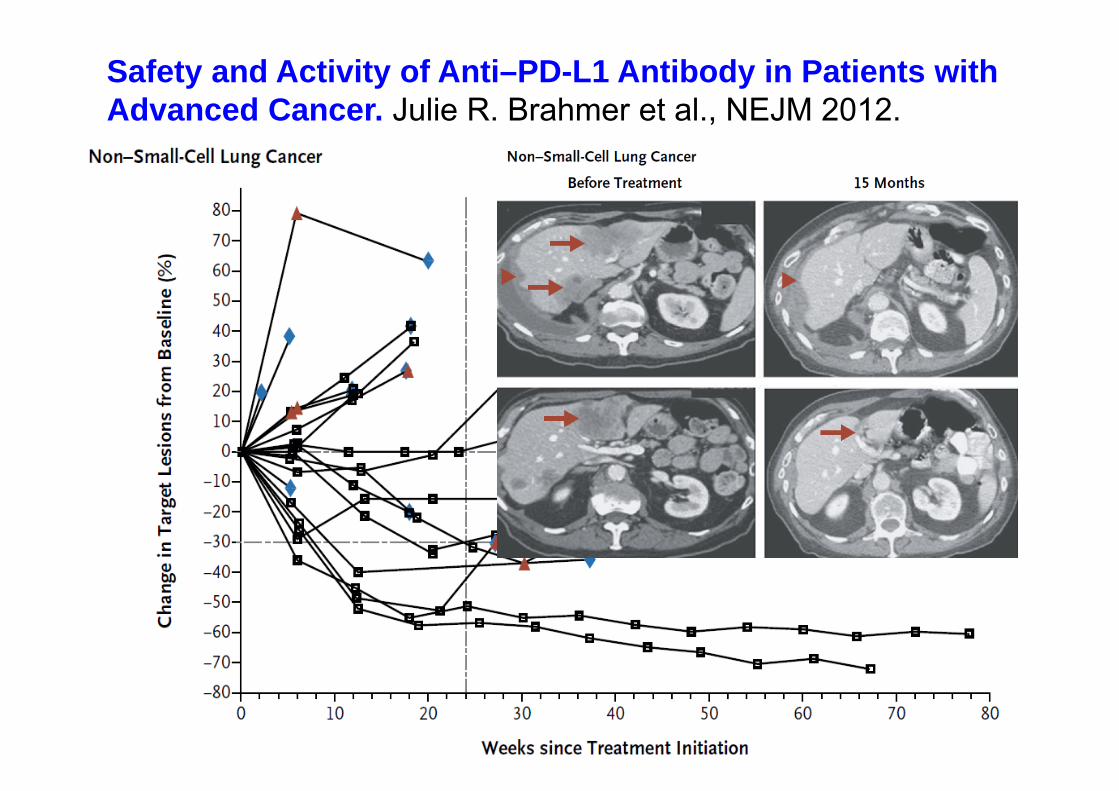
Safety and Activity of Anti–PD-L1 Antibody in Patients with Advanced Cancer. Julie R. Brahmer et al., NEJM 2012.
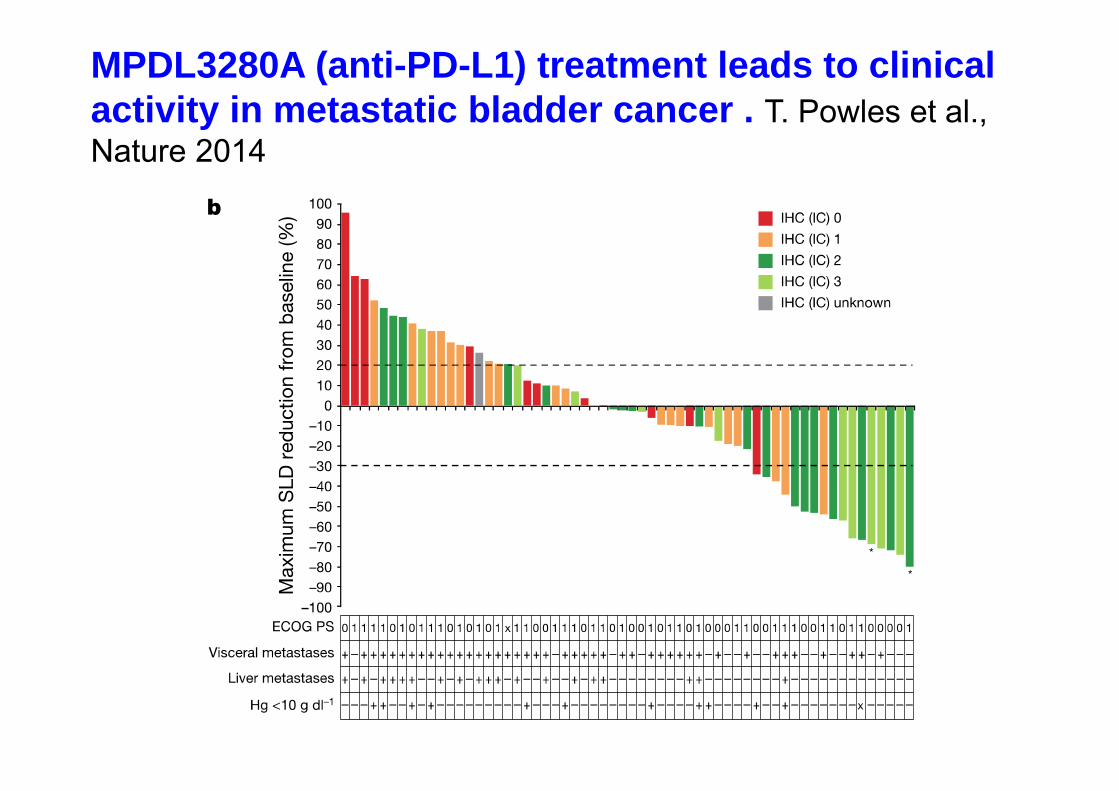
MPDL3280A (anti-PD-L1) treatment leads to clinicalactivity in metastatic bladder cancer . T. Powles et al., Nature 2014

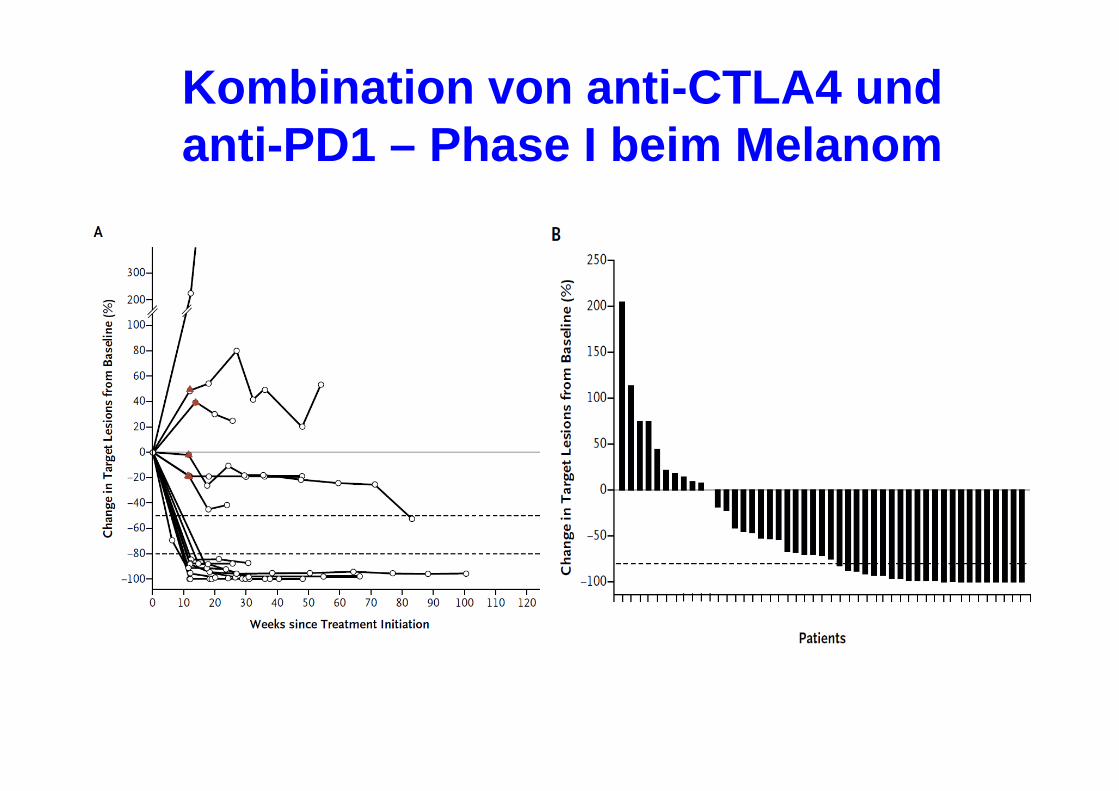
Kombination von anti-CTLA4 und anti-PD1 – Phase I beim Melanom
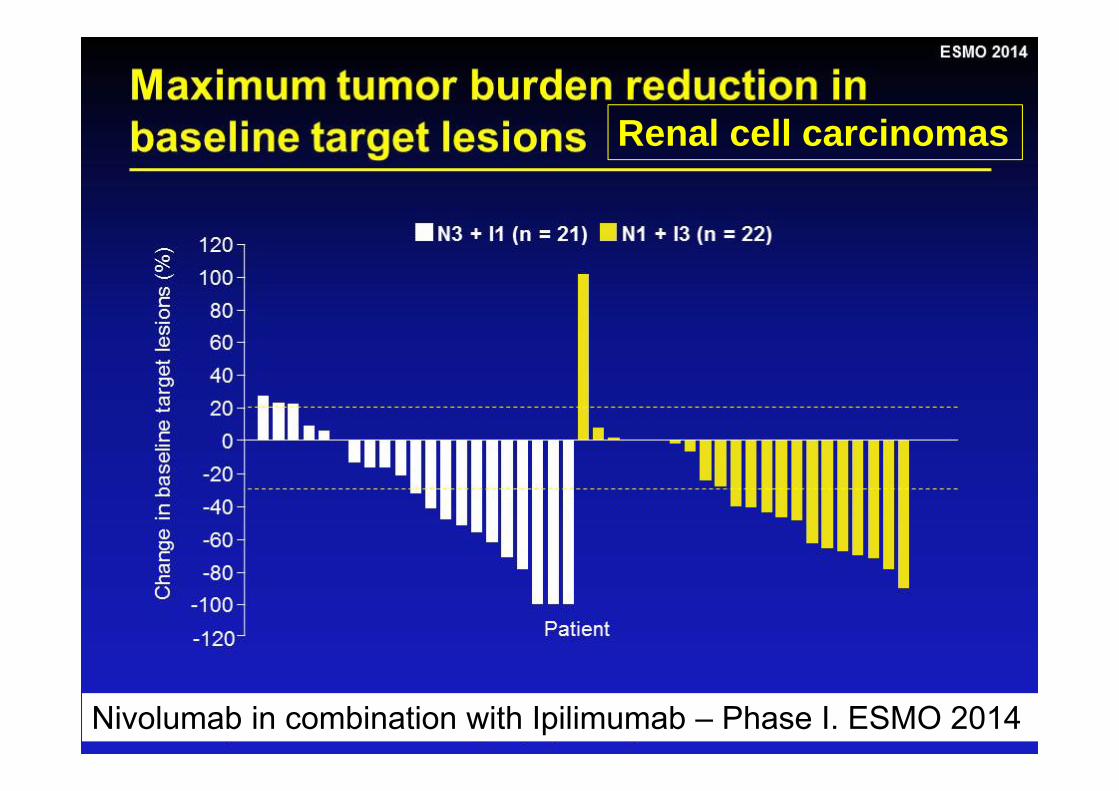
Renal cell carcinomas
Nivolumab in combination with Ipilimumab – Phase I. ESMO 2014
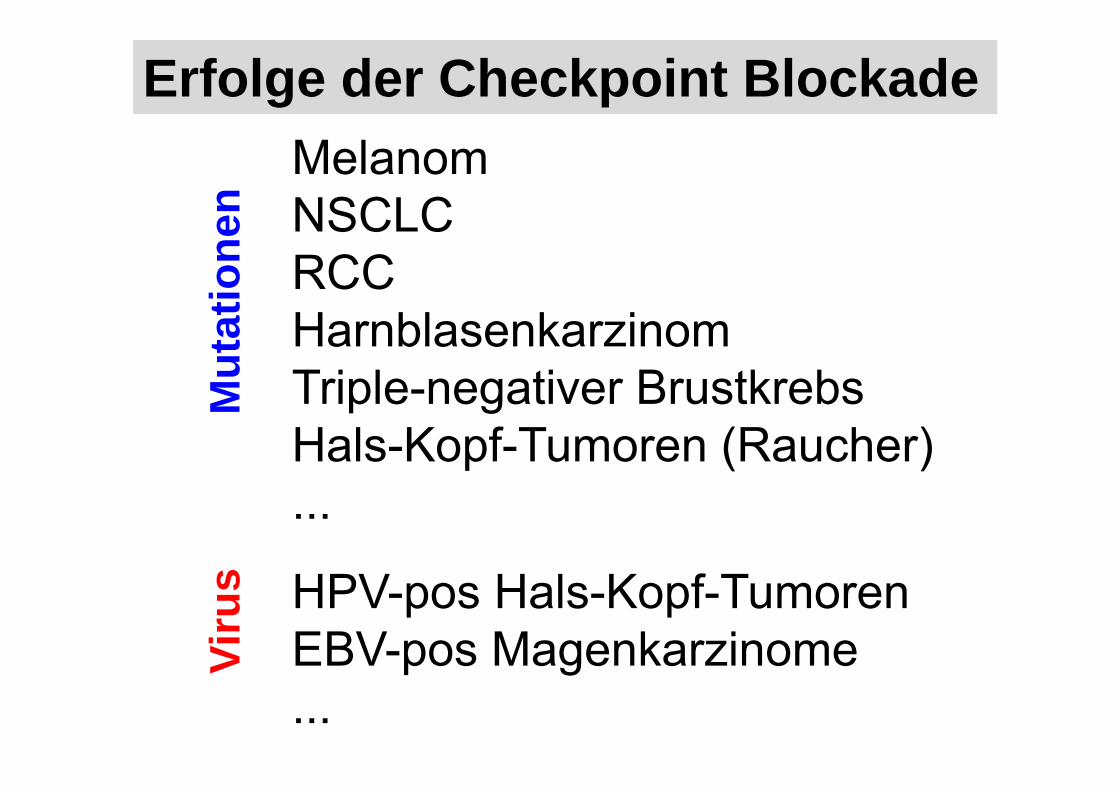
MelanomNSCLCRCCHarnblasenkarzinomTriple-negativer BrustkrebsHals-Kopf-Tumoren (Raucher)...
HPV-pos Hals-Kopf-TumorenEBV-pos Magenkarzinome...
Viru
sM
utat
ione
n
Erfolge der Checkpoint Blockade

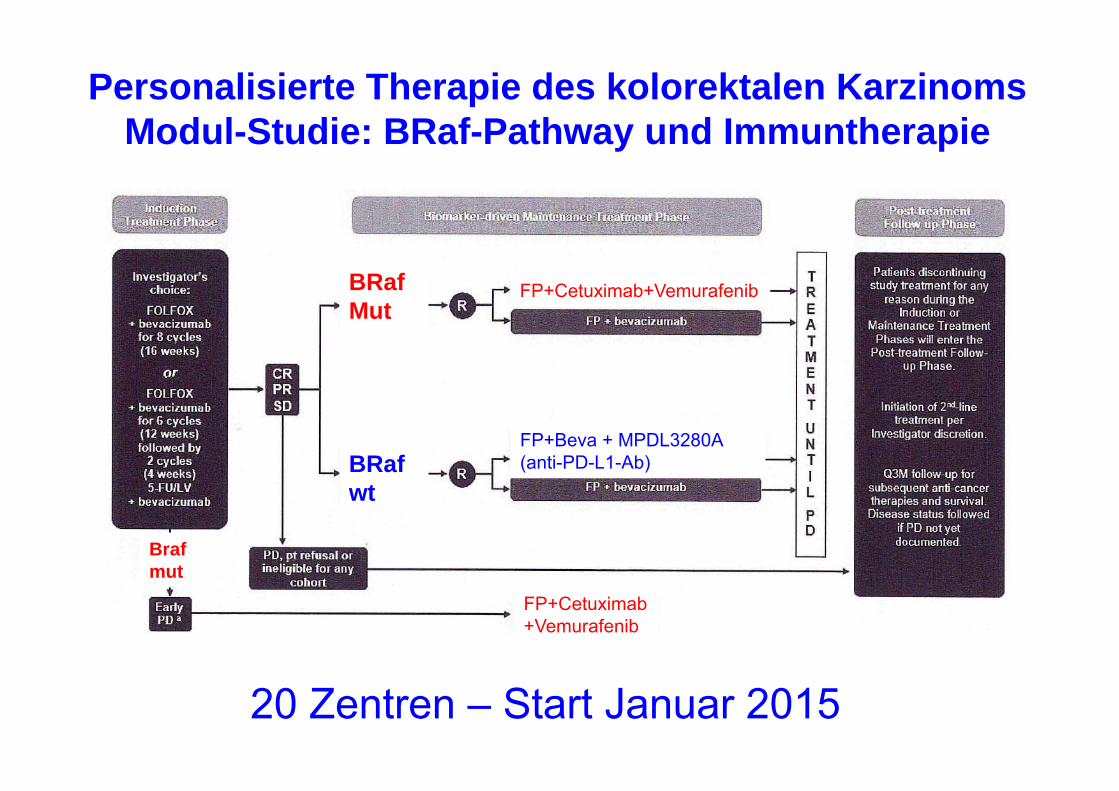
Personalisierte Therapie des kolorektalen KarzinomsModul-Studie: BRaf-Pathway und Immuntherapie
BRafMut
BRafwt
FP+Cetuximab+Vemurafenib
FP+Cetuximab+Vemurafenib
Brafmut
FP+Beva + MPDL3280A (anti-PD-L1-Ab)
20 Zentren – Start Januar 2015
Preis 2013
Entwicklung des Krebszentrum Reutlingen
OSPReutlingen
GemeinsameStudienambulanz
UKT Strahlentherapiein Reutlingen
Ermächtigung amb. Onko
Brustzentrum
Darmzentrum
ProstatakarzinomzentrumGynäkologisches Tumorzentrum
Pankreaskarzinomzentrum
2003 2005 2008 2010 2011 2013 2014
Palliativstation

Palliativstation
Telefon07121 / 200-46 10Fax07121 / 200-43 47
http://www.kreiskliniken-reutlingen.de/klinik-klinikum-am-steinenberg-reutlingen/kliniken-und-institute/palliativstation/artikel-palliativstation.html

Vielen Dank





























