Embed Size (px)
Citation preview


Stepwise intensification of insulin in T2DM management—Exploring the concept of the basal-plus approach in clinical practice
LOBNA F ELTOONY Head Of Internal Medicine Department
Faculty Of MedicineAssiut University




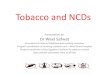
HOMA=homeostasis model assessment
Adapted from Holman RR. Diabetes Res Clin Pract 1998;40(suppl 1):S21–5.
Decreasing -cell function as part of the progression of T2DM
Normal -cell function by HOMA (%)
Time (years)
0
20
40
60
80
100
―10 ―8 ―6 ―4 ―2 0 2 4 6
Time of diagnosis?
Pancreatic function
~ 50% of normal


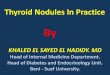
Clinical Inertia: “Failure to Advance Therapy When Recommended”
Mean A
1C
at La
st V
isit*
(%)
8.2 Years
ADA Goal
Diet and Exercise
Years Elapsed Since Initial Diagnosis
Initiation of
insulin therapy
SU or metformin
Combination oral agents8.6%
8.9%
9.6%
7
8
9
10
2.5 Years 2.9 Years 2.8 Years
*Adapted from: Brown JB et al. Diabetes Care. 2004;27:1535-1540.


Insulin
The most powerful agent we
have
to control glucose


Patient J.L., December 15, 1922 February 15, 1923
The Miracle of Insulin

Indications of insulin
Continuous Use* Type 1 Diabetes
* Type 2 Diabetes with OHA failure
- Primary - Secondary
Intermittent Use* Type 2 diabetes during
- major surgery
- pregnancy, labour and delivery
- myocardial infarction
- acute infections
- Hypergycemic emergencies: DKA & HHS
Life-saving in T1DM
Essential in T2DM

Starting dose of insulin
• T1DM: 1 -0.2-1 U/kg / day1
• T2DM: 0.2-0.3 U/kg / day
In split mixed regimen- 2/3 as intermediate acting & 1/3 as
short- acting 2
In basal bolus regimen: ½ basal at bed time and ½ bolus in 3
divided doses.
Dosage is individualized and titrated soon
1Goodman & Gillman’s The pharmacological basis of therapeutics ed. 9th .pg. 15012 Harrison’s Principles of Internal Medicine (15th Edition) pg. 2131


Hb
A1
C(%
)
UKPDS: Long-term follow-up
Bailey CJ & Day C. Br J Diabetes Vasc Dis 2008; 8:242–247.
Holman RR, et al. N Engl J Med 2008; 359:1577–1589.
Differences in mean glycated
hemoglobin levels between the
intensive therapy group and the
conventional-therapy group
were lost by 1 year, with similar
glycated hemoglobin
improvements thereafter in all
groups (p= not significant)
P=0.71
Glucose similar
BUT CV events
now better
Metformin group 21% 33% 27%

A new paradigm
Del Prato S. Diabetologia 2009; 52:1219–1226.
Del Prato S. Diabetologia 2009; 52:1219–1226.

Why Early insulin initiation? Clinical & Pharmacological Reasons(4)
Insulin
Improves beta-cell function
(reduces glucotoxicity &
lipotoxicity)
Reverses insulin resistance Improves Quality of Life
Beneficial effects on
lipids
Insulin provides
4 benefits beyond
glycemic control

LIFESTYLE MEASURESThen at each step, if not to target (generally HbA1c <7.0%)
IDF Treatment algorithm for people with type 2 diabetes
or
oror
MetforminSulfonylurea or
α-Glucosidase inhibitor
Sulfonylureaα-Glucosidase inhibitor
or DPP-4 inhibitoror Thiazolidinedione
Basal insulin orPre-mix insulin
GLP-1 agonist
Basal + meal-time insulin
Metformin(if not first line)
α-Glucosidase inhibitoror DPP-4 inhibitor
or Thiazolidinedione
Basal insulin orPre-mix insulin
(later basal + meal-time)
Alternative approachUsual approach
Considerfirst line
Considersecond line
Considerthird line
Considerfourth line

Early Insulinization Is Recommended by the ADA/EASD to Avoid Clinical Inertia
●If HbA1c targets are not achieved after ~3 months of initial treatment, alternative
therapy such as basal insulin should be initiated1,2
MonotherapyEfficacy*Hypo riskWeightSide effectsCosts
MetforminHigh
Low riskNeutral / loss
GI / lactic acidosisLow
If HbA1c target not achieved after ̴3 months of monotherapy, proceed to 2-drug combination (order not meant to denote any specificpreference - choice dependent on a variety of patient- and disease-specific factors):
Dual therapy†
EfficacyHypo riskWeightSide effectsCosts
Metformin +
Sulfonylurea Thiazolidinedione DPP-4 inhibitor SGLT 2 inhibitor GLP-1 receptor agonistHigh
Moderate riskGain
HypoglycemiaLow
HighLow risk
GainEdema, HF, fxs
Low
IntermediateLow riskNeutral
RareHigh
If HbA1c target not achieved after ̴3 months of dual therapy, proceed to 3-drug combination (order not meant to denote any specificpreference - choice dependent on a variety of patient- and disease-specific factors):
IntermediateLow risk
LossGU, dehydration
High
HighLow risk
LossGI
High
Insulin (basal)Highest
High riskGain
HypoglycemiaVariable
Healthy eating, weight
control, increased
physical activity,
and diabetes
education
Early insulin therapy has the potential to achieve near-normal glucose control
& prevent progression of glucose intolerance3
1. Inzucchi SE, et al. Diabetologia 2012;55:1577–96
2. Nathan DM, et al. Diabetes Care 2009;32:193–203
3. ORIGIN Trial Investigators. N Engl J Med 2012;367:319–28
ADA=American Diabetes Association; EASD=European Association for the Study of Diabetes

AACE/ACE diabetes algorithm for glycemic control (A1c > 9.0%).

Rationale for initiating insulin therapy with basal insulin

WHAT!?
Did you say
INSULIN?!
Barriers to
the Use of
Insulin

Patient Concerns About Insulin
• Fear of injections
• Worries that insulin
could worsen diabetes
• Concerns about
hypoglycemia
• Complexity of
regimens



Step One: Initiating Insulin
• Start with either…
– Bedtime intermediate-acting insulin or
– Bedtime or morning long-acting insulin
Insulin regimens should be designed taking
lifestyle and meal schedules into account
Nathan DM et al. Diabetes Care 2006;29(8):1963-72.

Basal insulin in type 2 diabetes(e.g. LA 0.1-0.2 U/kg or 10U)
Non-insulin therapies
LA = Long-Acting insulin: Glargine, Detemir
Basal Insulin in Type 2 Diabetes

Basal Insulin Therapy
• Usual first step in beginning insulin therapy
• Continue oral agents and add basal insulin to optimize FPG
• A1C of up to 9.0% usually brought to goal (7%) by addition of basal insulin therapy to oral agents
• Easy and generally safe: patient-directed treatment algorithms with small risk of serious hypoglycemia
ADA=American Diabetes Association; EASD=European Association for the Study of Diabetes.
ADA/EASD Management of hyperglycemia in type 2 diabetes: A patient-centered approach. Diabetologia (2012) 55:1577–1596

Starting With Basal Insulin in DM 2
Advantages
• 1 injection with no mixing
• Insulin pens for increased acceptance
• Slow, safe, and simple titration
• Low dosage
• Effective improvement in glycemic control
• Limited weight gain6-37


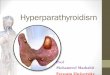
Comparison of 24-hour glucose levels in control subjects vs patients with diabetes (p<0.001).Adapted from Hirsch I, et al. Clin Diabetes 2005;23:78–86. Time of day (hours)
400
300
200
100
006.00 06.0010.00 14.00 18.00 22.00 02.00
Pla
sma
glu
cose
(m
g/d
l)
NormalMeal Meal Meal
20
15
10
5
0
Plasm
a gluco
se (m
mo
l/l)
Why Basal insulin?
Hyperglycaemia due to an increase in fasting glucose
T2DM
Treating fasting hyperglycaemia lowers the entire 24-hour plasma glucose profile

A balanced approach for insulin therapy in T2DM
250
200
150
100
50
0
Pla
sma
glu
cose
(m
g/d
L)
06:00 12:00 18:00 24:00 06:00
Time
T2DM
Normal
Mealtime hyperglycaemiaFasting hyperglycaemia
60
40
20
0
Co
ntr
ibu
tio
n (
%)
80
1(<7.3)
2(7.3-8.4)
3(8.5-9.2)
4(9.3-10.2)
5(>10.2)
HbA1c quintiles
Postmeal hyperglycaemiaFasting hyperglycaemia
Diabetes Care 1990; 16: 676–686 Monnier L. Diabetes Care 2003;26:881

Fix Fasting First
Basal Insulins
Normal Fasting Blood Glucose
Elevated Fasting Hyperglycemia and HGO
Hence need to fix fasting first

Look at all available basal insulins

Types of basal insulin
Intermediate-Acting (e.g. NPH, lente)
Long-Acting (e.g. ultralente)
Long-Acting Analogues (glargine, detemir)
Onset 1-3 hr(s) 3-4 hrs 1.5-3 hrs
Peak 5-8 hrs 8-15 hrsNo peak with glargine, dose-dependent peak with detemir
Duration Up to 18 hrs 22-26 hrs9-24 hrs (detemir); 20-24 hrs (glargine)
Rossetti P, et al. Arch Physiol Biochem2008;114(1): 3 – 10.

37
Profile of Insulin Glargine vs NPH
GlargineNPH

The quest for a better basal insulin… A “qualified A1c” by
hypoglycaemia
Hy
po
gly
caem
ia
NPH
Glargine
A1c
~ 0.4–0.6% ?
The impact of hypoglycaemia on A1c

Addition of Glargine allows most patients with T2DM to reach glycemic targets
1Riddle M, et al. Diabetes Care 2003;26:3080–6; 2Yki-Järvinen H, et al. Diabetologia 2006;49:442–51; 3Bretzel RG, et al. Lancet 2008;371:1073–84; 4Janka H,
et al. Diabetes Care 2005;28:254–9; 5Rosenstock J, et al. Diabetes Care 2006;29:554–9; 6Yki-Jarvinen H, et al. Diabetes 2006;55 Suppl. 1:A30
Hb
A1c (%
)
APOLLO3 LAPTOP4 Triple
Therapy5
LANMET2Treat-To-
Target1
INITIATE6
7.147.156.96
7.146.80
8.718.85 8.80
9.58.80
8.61
6.96
Baseline
Study endpoint
58.0Target HbA1c
≤7% (%)49.4 48.057.0NA NA
7
8
9
10
6
The most studied basal insulin
With established CV safety,
10 million patients,
> 60 million patient-years,
>59,000 participants in clinical trials

Basal Insulin Therapy in T2DM: AACE/ACE Recommendations
• Initiate insulin treatment by adding a long-acting basal formulation to existing noninsulin agents
40
Relatively peaklesstime-action curves
Greater day-to-day consistency
Lower risk of hypoglycemia
• Start with 10 U or 0.1-0.2 U/kg per day at bedtime• Slowly titrate by 1-3 U every 2-3 days until FPG reaches the desired target (<100
mg/dL for most patients)• Decrease dosage if FPG declines below a threshold specified for individual patient
*Under FDA review as of October 2012.Rodbard HW, et al. Endocr Pract. 2009;15:540-559.
Basal insulin analogues (detemir, degludec,* or glargine) are strongly preferred over human NPH insulin

Schreiber SA, et al. Diabetes Technol Ther 2008; 10:121–7.
Insulin glargine + OADs provides sustained glycaemic control
Extension of an original 9-month, open-label, uncontrolled,
multi-centre, observational study (n = 12,216)
Months of treatment
6.5
7.0
7.5
8.0
8.5
9.0
3 9 32
8.6
7.27.0 7.0
Mea
n H
bA
1c
(%)
n = 1,915 (extension)
Sustained Glycaemic Control with Basal Insulin in T2DM: ‘Real-life’ Data

8.5
9.0
8.0
7.5
7.0
6.5
0 4 8 12 16 20 24
HbA
1c(%
)
NPH + OADInsulin glargine + OAD
Weeks
0
2
4
6
8
10
12
14
16 21% risk reduction
p <0.02
42% risk
reduction p <0.01
Overall Nocturnal Hypoglycemia
Events
per
patient
per
year
Insulin Glargine vs. NPH in Treat-to-Target Trial: HbA1c and Hypoglycemia
Riddle et al. Diabetes Care 2003;26:3080-6.
Randomized to NPH or Glargine +
OAD with target HbA1c <7%

Initiate & Titrate basal insulin
FPG, fasting plasma glucose
Nathan DM, et al. Diabetes Care 2009;32:193-203.
Initiate insulin with a single injection of a basal insulin (Glargine)
CheckFPGdaily
In the event of hypoglycemia or FPG level <3.89 mmol/L(<70 mg/dL)
Reduce bedtime insulin dose by 4 units, or by 10% if >60 units
• Bedtime or morning long-acting insulin OR
• Bedtime intermediate-acting insulin
Daily dose: 10 units or 0.2 units/kg
INITIATE
• Increase dose by 2 units every 3 days until FPG (70–130 mg/dL)
• If FPG is >180 mg/dL, increase dose by 4 units every 3 days
TITRATE
Continue regimen and check HbA1c every 3 monthsMONITOR
• Continue regimen and check HbA1c every 3
months

• If HbA1c is <7%...
– Continue regimen and check HbA1c every 3 months
• If HbA1c is ≥7%...
– Move to Step Two…
After 2-3 Months…
Nathan DM et al. Diabetes Care 2006;29(8):1963-72.

Step-by-step approach
Even with optimal use of basal insulin, it is estimated that, using current treatment paradigms, ~40% of people will not meet HbA1c recommendations of < 7%.
A well-considered step-by-step approach to the intensification of insulin therapy, adding one, two or three prandial insulin injections to basal insulin according to each individual’s prandial requirements, seems a logical way forward.
The current evidence underlying this concept of meal-driven insulin intensification for the treatment of T2D, as well as the implications of adopting such an approach in clinical practice.
D. R. Owens Diabet. Med. 30, 276–288 (2013

In spite of titrating basal insulin, the inability to achieve
glycemic control despite normal or near-normal
fasting glucose usually means that excessive glycemic
excursions may be occurring during postprandial
period

Step Two: Intensifying InsulinIf fasting blood glucose levels are in target range but HbA1c ≥7%, check blood glucose before lunch, dinner, and bed and add a second injection:
• If pre-lunch blood glucose is out of range,
add rapid-acting insulin at breakfast
• If pre-dinner blood glucose is out of range,
add NPH insulin at breakfast or rapid-acting insulin at lunch
• If pre-bed blood glucose is out of range,
add rapid-acting insulin at dinner
Nathan DM et al. Diabetes Care 2006;29(8):1963-72.

Insu
lin
Eff
ect
B DL HS
Bolus insulinBasal insulin
Basal-Plus Insulin Therapy
Endogenous insulin
Adapted with permission from McCall A. In: Insulin Therapy. Leahy J, Cefalu W, eds. New York, NY:
Marcel Dekker, Inc; 2002:193
Tuesday, February 16,
2016
48

Making Adjustments
• Can usually begin with ~4 units and
adjust by 2 units every 3 days until blood
glucose is in range
Nathan DM et al. Diabetes Care 2006;29(8):1963-72.
•When number of insulin Injections increase from 1-
2………..Stop or taper of insulin secretagogues (sulfonylureas).

Insulin Initiation & Intensification – AACE 2015
START BASAL
A1c <8% A1c >8%
TDD: 0.1-0.2U/Kg TDD: 0.2-0.3U/Kg
Insulin titrationevery 2-3 days
to reachglycaemic goal
Fixed regimen: Increase TDD by 2U
Adjustable regimen FBG > 180 mg/dL: add 20% of TDD FBG 140-180 mg/dL: add 10% of TDD FBG 110-139 mg/dL: add 1 unit
If hypoglycemia, reduce TDD by BG < 70 mg/dL: 10% - 20% BG < 40 mg/dL: 20% - 40%
Glycemic control not at goal*
Intensify: Add prandial insulin
TDD:0.3-0.5 U/Kg
50% Basal Analog
50% Prandial Analog
Less desirable : NPH & regular/premixed insulin
Insulin titrationevery 2-3 days
to reachglycemic goals
Increase prandial dose by 10% for any meal if the 2-hr PP or next premeal glucose is > 180 mg/dl
Premixed: Increase TDD by 10% if fasting/premeal BG > 180 mg/dL
If fasting AM hypoglycemia, reduce basal insulin
If nighttime hypoglycemia, reduce basal and/or pre-supper or pre-evening snack short/rapid-acting insulin
If between-meal daytime hypoglycemia, reduce previous premealshort/rapid-acting insulin
* <7% for most patients with T2DM; fasting & premeal BG < 110 mg/dL; absence of hypoglycemia; ENDOCRINE PRACTICE Vol 21 No. 4 April 2015 e1

When to stop titrating basal insulin and add prandial insulin? Current opinions
1 Skyler JS. In: Lebovitz HE, ed. Therapy for diabetes Mellitus and related disorders. Alexandria, VA: American Diabetes Association, Inc.; 2004:207-223.
2 American Diabetes Association. Practical Insulin: A Handbook of Prescribing Providers. 3rd ed. 2011:1-683 Inzucchi S, et al. Diabetes Care. 2012;35:1364-1379 ; 4 Davidson MB, et al. Endocr Pract. 2011;17:395-403
The individual is not meeting glycemic targets on basal insulin1-4 and:
A1C still not at goal with 0.5 U/kg/day
of daily basal insulin3
Elevated A1C despite normal FPG with basal insulin2,3
FPG with basal insulin is within
targeted range, but PPG is persistently
above goal3,4
Further increases in basal insulin resultin hypoglycemia3

Stepwise Intensification of Treatment for Continuity of Control
Progressive deterioration of -cell function
Lifestyle changes
Oral agents
BasalAdd basal insulin and titrate
Basal plusAdd prandial insulin at main meal
Basal bolusAdditional prandial doses as
neededFBG above target
HbA1c above target
HbA1c above target
FBG at target
HbA1c above target
Adapted from Raccah D et al. Diabetes Obes Metab 2008;10(2):76-82.
When glycaemic targets are not met:
– Treatment should be changed to the next ‘step’
– Currently, therapy change is often too late
– Earlier treatment modification is necessary

• If HbA1c is <7%...
– Continue regimen and check HbA1c every 3 months
• If HbA1c is ≥7%...
– Move to Step Three…
After 2-3 Months…
Nathan DM et al. Diabetes Care 2006;29(8):1963-72.

Advancing Basal/Bolus Insulin
Indicated when FBG acceptable but
– A1C > 7% or > 6.5%
and/or
– SMBG before dinner > 140 mg/dL
Insulin options
– To glargine or NPH, add mealtime aspart / lispro
– To suppertime 70/30, add morning 70/30
– Consider insulin pump therapy
Oral agent options
– Usually stop sulfonylurea
– Continue metformin for weight control
– Continue glitazone for glycemic stability?


Isoglycemic clamp study
Inadequate prandial insulin : Postprandial Hyperglycemia Excess inter-prandial supply: Increased risk of Hypoglycemia
Insulin Profiles: Premixed 30/70 Aspart
0
100
200
300
400
0 4 8 12 16 20 24 hrs
Pla
sma
Insu
lin (p
M) HYPER HYPER HYPER
Luzio S et al, Diabetologia 49:1163-8, 2006
riskHYPO
riskHYPO
The pre-mixes are NOT suitable to Treat-to-target A1C <7.0%

Insulin Glargine is more suited for initiating insulin therapy than premixed insulin analogues
Basal insulin
e.g. insulin Glargine
Premixed insulin
e.g. premixed insulinaspart 30/70
Initial number of injections daily 1 21
Daily initial dose Insulin glargine: 10 U 6 U + 6 U1
Timing of injections Morning or eveningBreakfast
and dinner1
Monitoring fortitration targets
FPG(once daily)
FBG and preprandial BG(twice daily)1
LifestyleFlexible mealtimesand meal content
Scheduled mealtimesand set meal plans
IntensificationAddition of once-daily prandial insulin
(basal-plus) to basal bolusIncrease to 3 times daily
1. Summary of product characteristics for NovoMix 30, 50 and 70. Available at www.emea.europa.eu/humandocs/Humans/EPAR/novomix/novomix.htm (last accessed 2 July 2008).

Clinical evidence for the‘basal-plus’ / basal-bolus’ approach

Glulisine added to glargine further improves glycemic control
*For difference in change in HbA1c
Randomization
Proof of concept (POC) study: Basal Plus+1 therapy versus basal insulin glargine alone
Control
group
Glargine
+ glulisine
p = 0.0499
0
10
20
30
40
% a
ch
iev
ing
Hb
A1c
<7
.0%
8.8
22.4
p = 0.029*
Control
groupGlargine
+ glulisine
6
7
8
9
Hb
A1c (%
)
8.07.87.8
7.5
Endpoint
8.07.8 7.8
7.5
8.8
Owens DR, et al. Diabetes Obes and Metab 2011.

Control
group
Glargine
+ glulisine
p = ns
0.0
0.2
0.4
0.6
Me
an
bo
dy
we
igh
t c
ha
ng
e
fro
m b
ase
lin
e (
kg
)
0.5
0.2
Proof of concept (POC) study: Basal Plus+1 therapy versus basal insulin glargine alone
Glargine
+ glulisine
Control
group
0
2
4
6
8 7.688.19
10p = ns
Sy
mp
tom
ati
c h
yp
o
(eve
nt/
pa
tien
t-y
ea
r)
Glargine
+ glulisine
0.0
Control
group
0.0
0.1
0.2
0.3
Se
ve
re s
ym
pto
ma
tic h
yp
o
(eve
nt/
pa
tien
t-y
ea
r)
0.2
p = ns
Basal plus approach is safe with only minor weight gain
Randomization Endpoint
Owens DR, et al. Diabetes Obes and Metab 2011.

1.2.3 study: Insulin glargine with addition of 1, 2 or 3 daily doses of glulisine
• Subjects:
– Insulin naïve (785 entered study, 343 randomized) with type 2 diabetes(HbA1c ≥8.0%)
– Receiving 2 or 3 OHAs for ≥3 months (OHAs continued except sulfonylurea)
Randomization (subjects with HbA1c >7.0%, n=434)
24 weeks
Insulin glargine
(n=785)
14 weeks
Additional insulin glulisine once daily (n=115)
Additional insulin glulisine twice daily (n=113)
Additional insulin glulisine three times daily (n=115)
(1.2.3 study)
Mean study entry values:
• HbA1c (%): 9.8
• BMI (kg/m2): 35.0
Davidson M, et al. Endocr Pract 2011;17:395–403.

Glargine plus glulisine
(patients with HbA1c >7%)
Responders (whole population; n=785)
0
20
40
60
80
% a
ch
ievin
g H
bA
1c
<7.0
%
Additional
subjects
achieved
HbA1c <7.0%
with glulisine added to
glargine
23%
Run in Randomization Wk 8 Wk 16 Wk 24
7.40
7.0
10.1910.19
10.16
7.44
7.29
8.0
9.0
10.0Glulisine 1x
Glulisine 2x
Glulisine 3x
HbA1c (randomized population; n=343)
Glargine
(alone)
Subjects achieved
HbA1c <7.0% with
glargine during run
in
37%
Davidson M, et al. Endocr Pract 2011;17:395–403.
Hb
A1c (%
)
Intensification with glulisine improves glycemic control
1.2.3 study: Insulin glargine with addition of one, two or three daily doses of glulisine

p = NS for all other pairwise comparisons
Hypoglycemia (event/patient-year)
0
0.25
0.50
0.75
1.0
Seve
re o
r se
rio
us ‘h
yp
os’
x1 x2 x3
Glulisine
0.28
0.89
p = 0.044
0.64
0
5
10
15
20
x1 x2 x3
Glulisine
Confirm
ed s
ym
pto
matic ‘h
yp
os’
12.310.6
15.9
x1 x2 x30
1
2
3
4
5
Mea
n c
han
ge fro
m b
ase
line (
kg)
3.8 3.94.1
Glulisine
Body weight
Davidson M, et al. Endocr Pract 2011;17:395–403.
1.2.3 study: Insulin glargine with addition of one, two or three daily doses of glulisine

Randomization if A1c >7.0%Glimepiride stoppedGlargine / PremixOther OADs maintained
All-To-Target: Study Design
Randomized Comparison of Premixed Insulin vs Either Basal-Plus or Basal-Bolus
Premix (70/30) 2 x daily + 2-3 OADsN = 192
G+1: Glargine + upto 1 Glulisine + 2-3 OADsN = 189
G+3: Glargine + upto 3 x Glulisine + 2-3 OADsN = 191
Screening * ** ** Treatment in G+1 and G+3 groups intensified at weeks 12, 24, 36 or 48 if A1c>7%
Riddle, MC et al. Diabetes, Obesity and Metabolism 2014. 16: 396–402,
Inclusion Criteria
T2DM≥2 years BMI<45kg/m2
HbA1c>7.5% Use of 2-3 OADS
Run-in
Run-in (4 week) Randomized (60 weeks)
R

Hypoglycemia (event rate per patient-year)
*p < 0.01 vs premix ; **p < 0.001 vs premix
12.2
7.1* 7.2*
1.90.8** 0.9**
0.2 0.1* 0.2
Premix BID Basal Plus Basal Bolus
Δ HbA1c from baseline (%)
All-to-Target: Stepwise intensification with glargine and glulisine vs premix
<70 mg/dL + symptoms
<50 mg/dL + symptoms
<36 mg/dL
*p =0.06 vs premix ; **p <0.01 vs premixMean baseline HbA1c = 9.4%
-1.8-2.1* -2.2**
Premix BID Basal Plus Basal Bolus
Riddle, MC et al. Diabetes, Obesity and Metabolism 2014. 16: 396–402,

All-to-Target: A comparison of premixed, basal-plus and stepwise basal-bolus regimens
• More patients achieve A1c < 7% using glargine and glulisine in basal-plus and stepwise basal-bolus regimens compared with twice daily premixed insulin
Riddle M, et al. Diabetes 2011;60(Suppl.1):PP-0409.
HbA1c<7% at week 60
HbA1c<7% at week 60
without hypoglycemia
* vs premix
39%
49%45%
14%
24% 24%
0%
10%
20%
30%
40%
50%
60%
% o
f p
ati
en
ts (
at
week 6
0)
Premix BIDn=192
Glargine+glulisinebasal-plus
n=189
Glargine+glulisinestepwise basal-bolus
n=191
p<0.025*p<0.05*
p<0.05* p<0.01*
Riddle, MC et al. Diabetes, Obesity and Metabolism 2014. 16: 396–402,


69

Proposed progressive insulin strategies in type 2 diabetes.
*Log = rapid-acting insulin analogues (lispro, aspart, glulisine
)

Initiating & Adjusting Insulin
Continue regimen; check
HbA1c every 3 months
If FBG in target range, check BG before lunch, dinner, & bed; depending
on BG results, add second injection (can usually begin with ~4 units and adjust by 2 units every 3 days until BG in range)
Recheck pre-meal BG levels and if out of range, may need to add another
injection; if HbA1c continues to be out of range, check 2-hr postprandial levels
and adjust preprandial rapid-acting insulin
If HbA1c ≤7%...
Bedtime intermediate-acting insulin, or
bedtime or morning long-acting insulin (initiate with 10 units or 0.2 units per kg)
Check FG and increase dose until in
target range
If HbA1c 7%...
Hypoglycemia or FG >3.9 mmol/L (70 mg/dL):
Reduce bedtime dose by ≥4 units(or 10% if dose >60 units)
Pre-lunch BG out of range: add
rapid-acting insulin at breakfast
Pre-dinner BG out of range: add NPH insulin at
breakfast or rapid-acting insulin at lunch
Pre-bed BG out of range: add
rapid-acting insulin at dinner
Continue regimen; check
HbA1c every 3 months
Target range:3.9-7.2 mmol/L (70-130 mg/dL)
If HbA1c ≤7%... If HbA1c 7%...
Nathan DM et al. Diabetes Care 2009;32(1):193-203.

Conclusions
In the early stages of insulin therapy, most individuals seem to achieve favorable glycaemic control with
basal insulin alone, or in combination with a single prandial
insulin injection.
The addition of a single prandial insulin injection at the largest meal is
well tolerated and associated with significant improvements in (HbA1c), low rates of hypoglycaemia & limited
weight gain.
More people achieve recommended HbA1c targets with a basal-plus
strategy, compared with twice-daily premixed insulin therapy, with lower
rates of hypoglycaemia.
Step-by-step approach with the basal-plus strategy is a promising
alternative method of insulin intensification that allows for
individualization of treatment and may delay progression to a full
basal–bolus insulin replacement therapy for many individuals.
Owens D. Diabet Med. 2013 Mar; 30(3): 276–288.

Stepwise Intensification of Treatment for Continuity of Control
Progressive deterioration of -cell function
Lifestyle changes
Oral agents
BasalAdd basal insulin and titrate
Basal plusAdd prandial insulin at main meal
Basal bolusAdditional prandial doses as
neededFBG above target
HbA1c above target
HbA1c above target
FBG at target
HbA1c above target
Adapted from Raccah D et al. Diabetes Obes Metab 2008;10(2):76-82.
When glycaemic targets are not met:
– Treatment should be changed to the next ‘step’
– Currently, therapy change is often too late
– Earlier treatment modification is necessary

THANK YOU
Thank you