Embed Size (px)
Citation preview

Metformin ® XRBenefits of continuing
Metformin XR with the use
of Insulin

Page 2
Mohamed Mashahit Fayoum Universit
Page 3
Agenda
Introduction
Diabetes burden 2016 updates
Metformin ® XR, What do the guidelines say?
Metformin e® XR rationale & Clinical benefits
Metformin ® XR Reshaping Metformin efficacy

Page 4
Type 2 DM is an old disease….
….still need to be revised
First Description of Diabetes 1550 BC
This papyrus found in 1862 contains descriptions of various diseases including a polyuric state resembling diabetes mellitus.
Treatment recorded was a 4 day course of a liquid extract of bones, wheat, grain, grit, green lead and earth.

Page 5

Page 6

Page 7

Page 8
Agenda
Diabetes burden 2016 updates
Glucophage® XR, What do the guidelines say?
Glucophage® XR rationale & Clinical benefits
Glucophage® XR Reshaping Metformin efficacy

Page 9
Diabetes: A global emergency
IDF Diabetes Atlas, 7th edition
Estimated number of people with diabetes worldwide and per region in 2015
and 2040 (20-79 years)

Page 10
Diabetes around the world
IDF Diabetes Atlas, 7th edition

Page 11
IDF Diabetes Atlas, 7th edition
One in 7 adults have diabetes in Egypt
Diabetes (20-79 years)2015 2040
Number of people with diabetes
(diagnosed and undiagnosed)
7.8 million
(3.8-9.0 million)
15.1 million
(7.3-17.3 million)
Raw country prevalence14.8%
(7.2-17.1%)
17.8%
(8.6-20.4%)
Mean diabetes-related expenditure per person
with diabetesUSD 219 USD 218
Number of adults with undiagnosed diabetes3.2 million
(1.5-3.7 million )
6.2 million
(3-7.1 million)
Percent of undiagnosed diabetes 41.20%
Number of deaths due to diabetes78,200
(42,000-87,800)
Percent of deaths before age 60 43.60%

Page 12
Top 10 countries
IDF Diabetes Atlas, 7th edition
Top ten countries/territories for number of people with diabetes (20-79 years), 2015 and 2040

Page 13

Page 14
An estimated
average of
1,622 USD per
person with
diabetes was
spent on
diabetes-related
health
expenditures in
2015

Page 15
UKPDS 33. Lancet 1998; 352: 837-53
Risk of disabling complications in T2DM patients
Complications
Heart attacks 27 patients
Stroke 10 patients
Retinopathy 23 patients
Premature Mortality
Diabetes deaths 28 patients
Life expectancy 5-7 years
100 Patients - Age 55
15 Years Follow-up
Patients with type 2 diabetes are at heightened risk of disabling complications versus non-diabetics

Page 16
Agenda
Diabetes burden 2014 updates
Metformin ® XR, What do the guidelines say?
Glucophage® XR rationale & Clinical benefits
Glucophage® XR Reshaping Metformin efficacy

Page 17
Glucophage XR in guidelines:

Page 18
Add basal or
intensify insulin
Lifestyle intervention and metformin
Add sulfonylurea
(least expensive)
Add basal insulin
(most effective)
Add TZD
Add TZDAdd basal
insulin***
Add
sulfonylurea
If HbA1c ≥7%*
If HbA1c ≥7%
If HbA1c ≥7%
Intensive insulin + metformin +/− TZD**
Nathan DM et al. Diabetes Care 2006;29(8):1963-72.
Nathan DM et al. Diabetologia 2008;51(1):8-11.
Intensify
insulin***
ADA/EASD Management Algorithm

Page 19
ADA/EASD Consensus Algorithm for
Management of DiabetesDiabetes Care. 2009, 32:193-203
At diagnosis:
Lifestyle
+
Metformin
Lifestyle+Metformin
+
Pioglitazone(No hypoglycemia, edema, CHF, bone loss)
Lifestyle+Metformin
+
Sulfonylurea
Lifestyle+Metformin
+
Intensive insulin
Lifestyle+Metformin
+
Basal Insulin
Lifestyle+Metformin
+
GLP1 (No hypoglycemia, wt loss, Nausea/vomiting)
Lifestyle+Metformin
+
Pioglitazone
+
Sulfonylurea
Lifestyle+Metformin
+
Basal Insulin
Tier 2: less well-validated
therapies
Tier 1: Well-validated core therapies
Step 1 Step 2 Step 3
Amylin agonists, Glinides
DPP-4 inhibitors may be
appropriate in selected
patients
*Useful when
hypoglycemia is to be
avoided

Page 20

Page 21
IDF guidelines as of December 2011

Page 22 IDF Treatment algorithm 2011
www.idf.org/treatment-algorithm-people-type-2-diabetes
IDF treatment algorithm for people with type 2 diabetes developed 2011

Page 23
HbA1c > 7%
HbA1c > 7%
ADA-EASD Position Statement (2012)
Antihyperglycaemic therapy for T2DM
Inzucchi SE et al . Diabetes Care 2012; April 19th online e-pub DOI:10.2337/dc12-0413
Metformin

Page 24 Davidson JA Chan JCN. Scientific Handbook, Metformin :the Gold Standard John Wiley & Sons
SEMDSA guidelines. JEMDSA 2012;17:S1-S94
Country or
Region
UK (NICE)
Australia
Asia-Pacific
Fra (AFSSAPS)
Lat Am (ALAD)
USA (ADA)
Europe (EASD)
IDF (global)
South Africa
(SEMDSA)
Year
2005/8/9
2004
2005
2009
2007
2006/8/9/12
2006/8/9/12
2005/12
2012
BMI definition
of overweight
(kg/m2)
>25
None
>23
>28
>27
>25
>25
>25
>25
Overweight
Metformin
Metformin
Metformin
Metformin
Metformin
Metformin
Metformin
Metformin
Metformin
Non-overweight
Metformin
Metformin
Metformin, SU,TZD,AGI
Metformin, SU or AGI
Metformin
Metformin
Metformin
Metformin , SU
Metformin
Recommendations for initiating pharmacologic
therapy after failure of diet and exercise
Glucophage® XR is the optimal 1st line therapy in all Guidelines
Glucophage XR in guidelines:

Page 25
Heart Attack Stroke
39%
Reduction
41%
Reduction
UKPDS 34. Lancet 1998; 352: 854-65
* versus lifestyle therapy
Improved Clinical Outcomes with
metformin - fewer life threatening
complications*

Page 26
The legacy effect of Metformin on Macrovascular complications from UKPDS 10 years Trial follow up.

Page 27
Cardiovascular benefits of Metformin:

Page 28
Cardiovascular benefits of Metformin:

Treatment algorithms of T2DM
Page 30
ADA/EASD 2015 update:

Page 31
ADA/EASD 2015 update:

Page 32
Glucophage® XR in the Guidelines

Page 33
Glucophage® XR in the Guidelines

Page 34
Benefits of continuing Metformin with Insulin in T2DM:
“Metformin is often continued when basal insulin is added,
with studies demonstrating less weight gain...“

Page 35
“Insulin plus metformin is a particularly effective means of
lowering glycaemia while limiting weight gain...“
Benefits of continuing Metformin with Insulin in T2DM:

Page 36
Benefits of continuing Metformin with Insulin in T2DM:
Metabolic
Benefits
Cardiovascular
Benefits
Glycaemic
Benefits
Insulin requirements

Page 37
Agenda
Diabetes burden 2014 updates
Glucophage® XR, What do the guidelines say?
Metformin® XR rationale & Clinical benefits
Glucophage® XR Reshaping Metformin efficacy

Page 38
Benefits of continuing Metformin with Insulin in T2DM: (Cardiovascular)
“...Metformin, reduce the risk of Macrovascular
disease after a follow-up period of 4.3 years by
39%”

Page 39
Benefits of continuing Metformin with Insulin in T2DM: (Glycemic benefits)

Page 40
Benefits of continuing Metformin with Insulin in T2DM: (HbA1c reduction)

Page 41
Benefits of continuing Metformin with Insulin in T2DM: (Lipid profile)

Page 42
Benefits of continuing Metformin with Insulin in T2DM: (Weight reduction)
Page 43
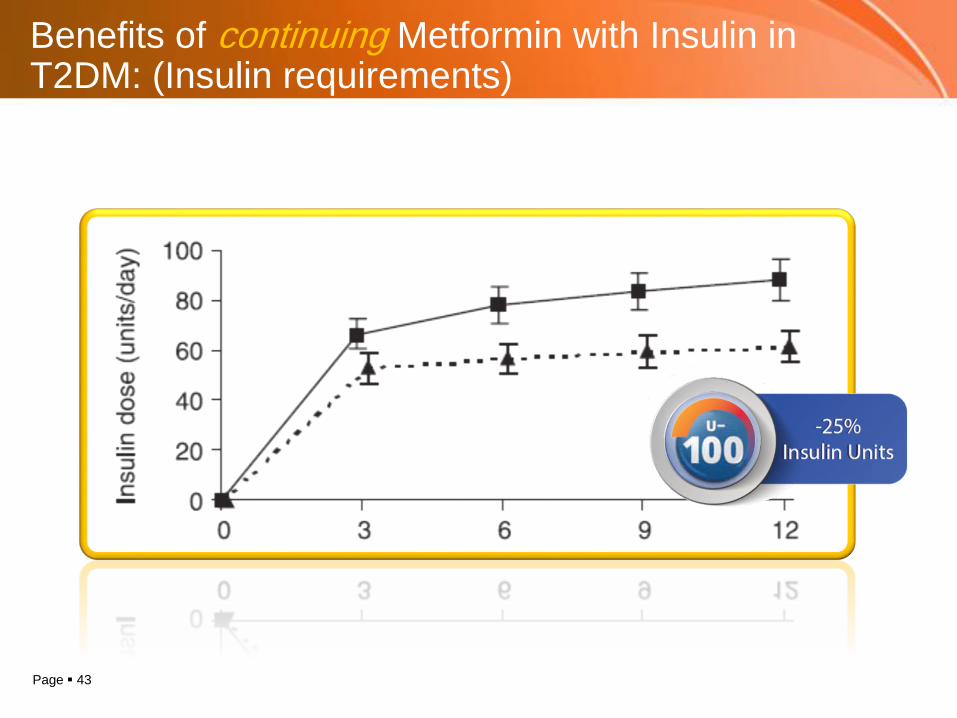
Benefits of continuing Metformin with Insulin in T2DM: (Insulin requirements)

Page 44 Kooy A. Arch Intern Med 2009; 169: 616-25
Metformin plus insulin
Placebo plus insulin
Metformin plus Insulin – health
outcome benefits in type 2 diabetes
over 4.3 years
39%

Page 45
GI disturbance
ConvenienceDose
2 gm/day
Metformin XR rationale:

Page 46
Metformin XR rationale:

Page 47
Metformin XR rationale: (GI side effects)

Page 48

Page 49
Glucophage XR rationale: (optimal dose)

Page 50
Metformin XR rationale: (optimal dose)
The optimal dose of
metformin for the control of
glycaemia is in the
region of 2000 mg/dayand
the average daily dosage of
metformin
achieved in routine clinical
practice lies between 1000
mg and 2000 mg
in most European
countries.
2000 mg is the optimum dose of Metformin
reducing A1c by 2%

Page 51
Glycemic benefits of 2gm/day:

Page 52
G Metformin XR rationale: (Compliance)
Page 53
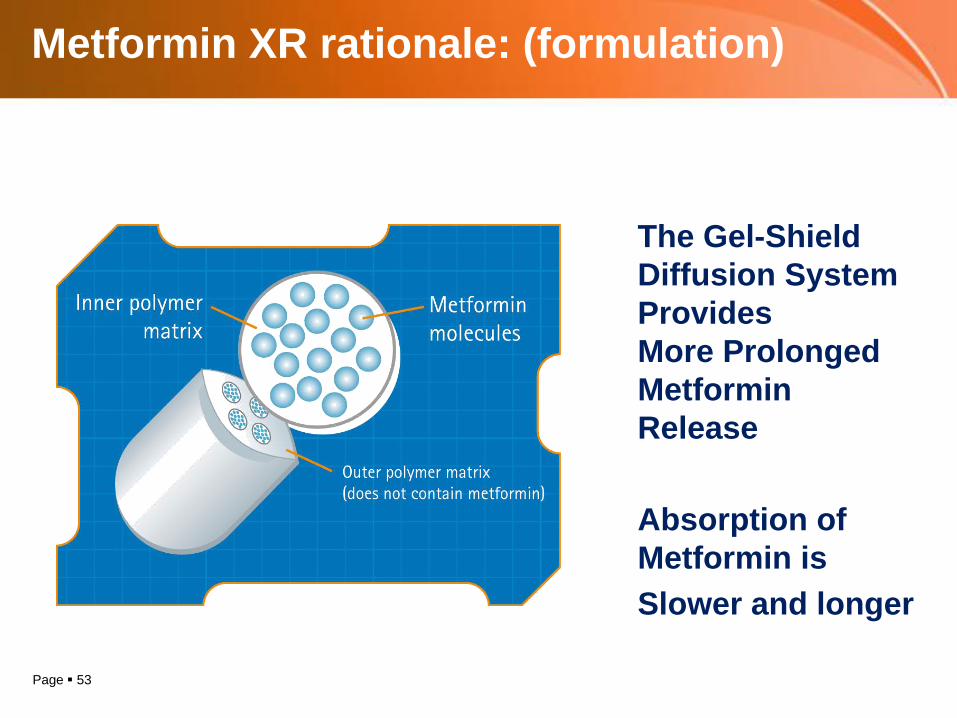
Metformin XR rationale: (formulation)
The Gel-Shield
Diffusion System
Provides
More Prolonged
Metformin
Release
Absorption of
Metformin is
Slower and longer

Page 54
Agenda
Diabetes burden 2014 updates
Glucophage® XR, What do the guidelines say?
Glucophage® XR rationale & Clinical benefits
Metformin ® XR Reshaping Metformin efficacy

Page 55
Patients Started on Metformin ® XR at Diagnosis –Tolerance Over 12 Months

Page 56
Switchover to Metformin ® XR Improves Adherence in Routine General Practice

Page 57
Metformin XR dosing schedule:
Divided Dose Once Daily

Page 58
Contra-indicationsBenefits
Holstein A Diabetologia 2005; 48: 2454-9
Metformin: Contra-indications

Page 59
• Severe renal dysfunction.
• Severe liver disease.
• Use of IV contrast media.
• Major surgical procedures.
• Congestive heart failure.
• History of alcohol abuse.
Metformin: Contra-indications

Page 60
eGFR level
(ml/min per 1.73 m2)Action
> 60No renal contraindication to metformin
Monitor renal function annually
< 60 and > 45
Continue use
Increase monitoring of renal function
(every 3-6 months)
< 45 and > 30
Prescribe metformin with caution
Use lower dose (e.g., 50%, or half-maximal dose)
Closely monitor renal function (every 3 months)
< 30 Stop metformin
Lipska KJ et al. Diabetes Care 2011;34:1431-1437
Metformin: Renal Function

Page 61
Take home message:
Insulin partner- More glyceamic control
- Decreases insulin requirements
- Benefits on lipid profile
- Benefits in weight reduction
2% reduction in HbA1c
Least GI upset
Once daily dosing

Page 62