Embed Size (px)
DESCRIPTION
Citation preview

Immunological aspect of tuberculosis
Ph.D student. Muslim Dhaher Musa Veterinary medicine college/ Microbiology Dept .

Introduction Tuberculosis (TB) remains a major global health problem. It causes ill health among
millions of people each year and ranks as the second leading cause of death from an
infectious disease worldwide, after the human immunodeficiency virus (HIV). The latest
estimates included in WHO report are that there were 8.6 million new TB cases in 2012
and 1.3 million TB deaths [1] . Each year around 3000 people in Iraq die from this
respiratory disease primarily spread by coughing and sneezing. Based on 2009 estimates
in Iraq, the incidence of TB was 56 per 100 000 population per year for all forms of TB
cases with 25 out of 56 being infectious cases. As a result of deteriorating socioeconomic
conditions during the last decade, the incidence of TB has been on the rise. With gradual
improvements in security and support from the Global Fund, WHO and the Global Drug
Facility, the national TB programme has been revitalized. Notifications of smear-positive
cases increased from 37% in 2007 to 46% in 2009[2].

Although tuberculosis was believed to be eliminated as a public health problem in the United States, the disease re-emerged in the early 1990s, particularly in areas where HIV-infection levels are high. The is disease is still the leading killer of individuals with AIDS (kuby 2013)

Sites of TB DiseaseTB disease can occur in pulmonary and extrapulmonary sites.
Pulmonary
TB disease most commonly affects the lungs; this is referred to as pulmonary TB. In
2011, 67% of TB cases in the United States were exclusively pulmonary. Patients with
pulmonary TB usually have a cough and an abnormal chest radiograph, and may be
infectious. Although the majority of TB cases are pulmonary, TB can occur in almost any
anatomical site or as disseminated disease
Extrapulmonary
Extrapulmonary TB disease occurs in places other than the lungs, including the larynx,
the lymph nodes, the pleura, the brain, the kidneys, or the bones and joints.

Miliary TB Occurs when tubercle bacilli enter the bloodstream and disseminate to all parts of the
body, where they grow and cause disease in multiple sites. This condition is rare but
serious. “Miliary” refers to the radiograph appearance of millet seeds scattered
throughout the lung. It is most common in infants and children younger than 5 years of
age, and in severely immunocompromised persons. Miliary TB may be detected in an
individual organ, including the brain.

Pathogensis Rout and site of infection: Mycobacterium tuberculosis is an obligatory aerobic, intracellular
pathogen, which has a predilection for the lung tissue rich in oxygen supply. The tubercle bacilli enter the
body via the respiratory route. The bacilli spread from the site of initial infection in the lung through the
lymphatics or blood to other parts of the body ,the apex of the lung and the regional lymph node being
favored sites. Extrapulmonary TB of the pleura, lymphatics, bone, genito-urinary system ,meninges,
peritoneum, or skin occurs in about 15 percent of TB patients. Events following entry of bacilli, Phagocytosis
of M. tuberculosis by alveolar macrophages is the first event in the host-pathogen relationship that decides
outcome of infection. Within 2 to 6 weeks of infection ,cell-mediated immunity (CMI) develops, and thereis an
influx of lymphocytes and activated macrophages into the lesion resulting in granuloma formation. The bacilli
may remain forever within the granuloma, get re-activated later or may get discharged into the airways after
enormous increase in number, necrosis of bronchi and cavitation.Fibrosis represents the last-ditch defense
mechanism of the host, where it occurs surrounding a central area of necrosis to wall off the infection when all
other mechanisms failed. Pathogenicity of mycobacterium tuberculosis depend on their ability to escape
phagocytic killing , by presence of Mycolic acid are unique alpha branch lipid found in cell wall of the
bacterium . Mycolic acid are hydrophobic molecule that form a lipid shell around the bacteria and effect on
the premability of the cell surface wherby prevent attack of mycobacterium by by cationic protein , lysozyme

And oxygen radicle in the phagocytic granule .
Host immune mechanisms in TB
Innate immune response: The phagocytosis and the subsequent secretion of IL-12 are processes initiated in the
absence of prior exposure to the antigen and hence form a component of innate immunity. The other components of
innate immunity are natural resistance associated macrophage protein (Nramp),neutrophils, natural killer cells (NK).
Nramp: Nramp is crucial in transporting nitrite from intracellular compartments such as the cytosol to more acidic
environments like phagolysosome,where it can be converted to NO.
Neutrophils : At the site of multiplication of bacilli, neutrophils are the first cells to arrive followed by NK cells, γ/δ
cells and α/β cells. There is evidence to show that granulocyte-macrophage-colony stimulating factor (GM-
CSF)enhances phagocytosis of bacteria by neutrophils[4].
Natural killer (NK) cells: NK cells are also the effecter cells of innate immunity. These cells may directly lyse the
pathogens or can lyse infected monocytes. During early infection, NK cells are capable of activating phagocytic cells
at the site of infection. A significant reduction in NK activity is associated with multidrug-resistant TB (MDR-TB).

IL-2 activated NK cells can bring about mycobactericidal activity in macrophages infected withM.
avium complex (MAC) as a non specific response. Apoptosis is a likely mechanism of NK cytotoxicity.
NK cells produce IFN-γ and can lyse mycobacterium pulsed target cells [5]. Apoptosis Another
potential mechanism involved in macrophage defense against M. tuberculosis , it is association with
TB is mediated through a down regulation of bcl-2, an inhibitor of apoptosis [6]
The interactions between M. tuberculosis and TLRs are complex and it appears that distinct
mycobacterial components may interact with different members of the TLR family. M. tuberculosis
can immunologically activate cells via either TLR2 orTLR4 in a CD 14-independent, ligand-specific
manner[7]. TLR (2 ,4, 9) are expressed on immue cells ( macrophage , B-cell, dendritic cell , mast
cell , specific type of T- cell ) and also on non immune cells ( epithelial cell and fibroblast ). Both TLR
2,9 and NOD receptor signaling induce transcription of gene that encode for cytokines which
include IL-1 beta ,TNF alpha and IL-6 for the recurtiment of immue cells to sit of infection . Also IL-2
signaling by ligation with lipoprotein of mycobacterium tuberculosis inhibit the MHC expression and
processing of Anitgen by macrophage

Acquired immune response Humoral immune response: Since M. tuberculosis is an
intracellular pathogen, the serum components may not get access and may not play
any protective role . Although many researchers have dismissed a role for B cells or
antibody in protection against TB, recent studies suggest that these may contribute
to the response to TB[8].
Cellular immune response T-cell
CD4 T cells:M. tuberculosis resides primarily in avacuole within the macrophage, and
thus, major histocompatibility complex (MHC) class II presentation of mycobacterial
antigens to CD4+ T-cells is an obvious outcome of infection. These cells are most
important in the protective response against M. Tuberculosis, In humans, the
pathogenesis of HIV infection has demonstrated that the loss of CD4+ T cells greatly
increases susceptibility to both acute and re-activation TB. The primary effector
function ofCD4+ T cells is the production of IFN-γ and possibly other cytokines,

NOS2 expression by macrophages was also delayed in the CD4+ T cell
deficient mice, but returned to wild type levels in conjunction with IFNγ
expression [9].
CD8 T cells: CD8+ cells are also capable of secreting cytokines such as IFN-γ
and IL-4 and thus may playa role in regulating the balance of Th1 and Th2 cells
in the lungs of patients with pulmonary TB. The mechanism by which
mycobacterial proteins gain access to the MHC class I molecules is not fully
understood. Bacilli in macrophages have been found outside the phagosome 4-
5 days after infection, but presentation of mycobacterial antigen by infected
macrophages to CD8 T cells can occur as early as 12h after infection[12] .
Reports provide evidence for a mycobacteria-induced pore or break in the
vesicular membrane surrounding the bacilli that might allow mycobacterial
antigen to enter the cytoplasm of the infected cell

γ/δ T-cells in TB: The role of γ/δ T cells in the host response in TB
has been incompletely worked out. These cells are large granular
lymphocytes that can develop a dendritic morphology in lymphoid
tissues; some γ/δ T cells may be CD8+. In general ,γ/δ T cells are
felt to be non-MHC restricted and they function largely as cytotoxic
T cells. γ/δ T cells can be found in the peripheral blood of
tuberculin positive healthy subjects and these cells are cytotoxic
for monocytes pulsed with mycobacterial antigens and secrete
cytokines that may be involved in granulomaformation[10]

Cytokines Interleukin-12: IL-12 is induced following phagocytosis of M. tuberculosis bacilli by macrophages and dendritic cells, which leads to development of a Th1 response with production of IFN-γ.
Interferon-γ: IFN-γ, a key cytokine in control of M.tuberculosis infection is produced by both CD4+ andCD8+ T cells, as well as by NK cells. IFN-γ might augment antigen presentation, leading to recruitment of CD4+ T-lymphocytes and/or cytotoxic T-lymphocytes, which might participate in mycobacterial killing. Although IFN-γ production alone is insufficient to control M. tuberculosis infection, it is required for the protective response to this pathogen. IFN-γ is the major activator of macrophages

Tumor necrosis factor (TNF-α): TNF-α is believed to play multiple roles in
immune and pathologic responses in TB. M. tuberculosis induces TNF-α
secretion by macrophages, dendritic cells and T cells.
Interleukin-6: IL-6 has also been implicated in the host response to M.
tuberculosis. This cytokine has multiple roles in the immune response,
including inflammation, hematopoiesis and differentiation of T cells
Interleukin-10: IL-10 is considered to be an anti-inflammatory cytokine.
This cytokine, produced by macrophages and T cells during M. tuberculosis
infection, possesses macrophage-deactivating properties, including down
regulation of IL-12production, which in turn decreases IFN-γ production by
T cells. IL-10 directly inhibits CD4+ T cell responses, as well as by
inhibiting APC function of cells infected with mycobacteria[11]

Tubercle formation Mycobacterium tuberculosis is resistant to intracelluare destruction until M
macrophage activated by Th1cells and dead organism are very slowly removed
because they contain large amount of poorly metabolized material ( wax). As result
the reaction prolonged and the activated macrophages continue to accumulate
many of these cells ingest the bacteria but fail to kill it so they die other
macrophage fuse togather in attempt to kill bacteria they form multinucleated cell
called giant cell due to replacement of normal lung cell by these giant cells and aslo
due to release large amount of lytic enzymes from these activated macrophage lead
to damage of blood vessels in the site of infection causing necrosis and formation of
tubercle . As these lesions heal, they become calcified and are readily visible on x-
rays of the lungs as a defined shadow. Much of the tissue damage seen with M.
tuberculosis is thus actually due to pathology associated with the cell-mediated
immune response.

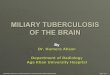
Tuberculs
CD4 T cells are activated within 2
to 6 weeks after infection and
secrete cytokines that induce the
infi ltration of large numbers of
activated macrophages . These
cells wall off the organism inside
a granuloma called a tubercle ,
a cluster of small lymphocytes
surrounding infected
macrophages
.



At present, the only vaccine for M. tuberculosis is an attenuated
strain of M. bovis called
B acille C almette- G uérin (BCG). This vaccine is fairly effective against
extrapulmonary tuberculosis but less so against the more common
pulmonary tuberculosis; in some cases, BCG vaccination has even
increased the risk of infection. Moreover, after BCG vaccination the
tuberculin skin test cannot be used as an effective monitor of exposure
to wild-type M. tuberculosis Because of these drawbacks, this vaccine
is not used in the United States but is used in several other countries.
However the alarming increase in multidrug-resistant strains has
stimulated renewed efforts to develop a more effective tuberculosis
vaccine.

Tuberculin test Because the positive tuberculin occur only in animal
that have or had tuberclosis , skin test may be used to identify animal infected by these disease . Skine test of the animal may be preformed in several ways :
1- single intradermal 2- comparative 3- short thermal 4- stormont

The simplest is single dermal test , in this test 0.05 ml of ppd tuberculin derived from M. tuberculosis or M . Bovis is injected into the anal fold and the injection site is examined after 72-96 hours comparison is easily made between injected and uninjected site and positive reaction consist of firm lump .
Advantage is Simplicity. Disadvantage is that because the cross-reaction it canot
distinguish between M .avium and M. avium paratuberculosisOr nocardia , also some animal show positive reaction but at
necropsy there is no lesion (tubercuels). Or it may occur with animals in advanced infection . The lack of the reaction can be seen in animals infected with John disease appear to be due to presence of blocking factor.

Comparative test
Involve intradermal inoculation of both avian and bovine tuberculin . Echa injected at side of the neck at seperat site and these sites are examined after 72 hours if the side of M.avium become enlarged mean animal infected with mycobacterium avium or mycobacterium avium paratubeculosis while if the side of the mycobacterium bovis enlarged greatly mean animal infected with mycobacterium tuberculosis.

Short thermal Large volume of tuberculin is injected
subcutaneously and animal examined for raise in temperature between 4-8 hours later. Explanation : T-cell activated by tuberculin and secret IL-1 that considered as endogenous pyrogen .

Tuberculin reaction



References 1- Global Tuberculosis report WHO 2013
4- Fleischmann J, Golde DW, Weisbart RH, Gasson JC.Granulocyte-macrophage colony-stimulating factorenhances phagocytosis of bacteria by human neutrophils.Blood 1986; 68: 708-115- Molloy A, Meyn PA, Smith KD, Kaplan G. Recognitionand destruction of bacillus Calmette-Guerin-infectedhuman monocytes. J Exp Med 1993; 177: 1691-8.6- Klingler K, Tchou-Wong KM, Brandli O, Aston C,Kim R, Chi C, et al. Effects of mycobacteria on regulationof apoptosis in mononuclear phagocytes.Infect Immun1997;65: 5272-87- Means TK, Wang S, Lien E, Yoshimura A, GolenbockDT, Fenton MJ. Human toll-like receptors mediate cellularactivation by Mycobacterium tuberculosis.J Immunol 1999;163: 3920-7

8- Bosio CM, Gardner D, Elkins KL. Infection of B cell-deficient mice with CDC1551, a clinical isolate ofMycobacterium tuberculosis: delay in dissemination anddevelopment of lung pathology. J Immunol 2000; 164 :6417-25
9- Caruso AM, Serbina N, Klein E, Triebold K, Bloom BR,Flynn JL. Mice deficient in CD4 T cells have onlytransiently diminished levels of IFN-γ, yet succumb totuberculosis.J Immunol 1999; 162: 5407-16
10 -Munk ME, Gatrill AJ, Kaufmann SH. Target cell lysisand IL-2 secretion by gamma/delta T lymphocytes afteractivation with bacteria. J Immunol 1990; 145 : 2434-9.
11- Rojas M, Olivier M, Gros P, Barrera LF, Garcia LF. TNF-a and IL-10 modulate the induction of apoptosis byvirulentMycobacterium tuberculosis in murinemacrophages.J Immunol 1999;162: 6122-3112- McDonough KA, Kress Y, Bloom BR. Pathogenesis oftuberculosis: interaction of Mycobacterium tuberculosiswith macrophages. Infect Immun 1993;61: 2763-73.79