Embed Size (px)
Citation preview

Treatment of Breast Cancer in 2012Where are we now?
Dr Janice WalsheConsultant Medical Oncologist
St Vincent’s University Hospital, Dublin

Outline
• Overview of treatment approach• Updates in diagnostics and therapy
– Oncotype Dx– Hormonal therapy advances– Chemotherapy Advances– “Targeted therapy advances”
• Hereditary breast cancer• Follow-up and “what can I do”

0
500
1000
1500
2000
2500
3000
3500
4000
4500
500019
95
2000
2005
2010
2015
2020
new
cas
es p
er y
ear
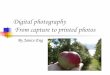
Projected number of Breast Cancers to 2020

0%
1%
2%
3%
4%
19
50
19
54
19
58
19
62
19
66
19
70
19
74
19
78
19
82
19
86
19
90
19
94
19
98
20
02
20
06
20
10
20
14
year of death
risk
of
de
ath
fro
m c
an
cer
be
fore
ag
e 7
5 (
%)
Deaths from Breast Cancer 1950-2014

Why?
• Incidence is increasing– Mammographic screening– Environmental Factors
• Mortality is decreasing– Early Detection– Better Treatment Options

Treatment Approach

Treatment for Breast Cancer
• Local therapy– Lumpectomy + radiation– Mastectomy (+/- radiation in
more advanced disease)– Goal: treat primary site of
disease
• Systemic therapy– Chemotherapy– Hormonal therapy – Targeted therapy

Special Environment
• Specialist Breast Cancer Unit• Multidisciplinary Approach
– Histopathologist– Surgery– Medical Oncology– Radiation Oncology– Genetic Risk Assessment– Nursing Expertise– Support services (Dietician, social worker,
psychologist, OT)

What directs the sequence of the Treatment?
Varies
• Clinical/ pathological stage and subtype of the tumor
• Biological characteristics of the tumor

Staging Breast Cancer

Factors that Influence Treatment Decisions
• Patient Age• Histological Subtype & Grade• Tumour Size • Lymph Node Involvement• Hormone Receptor Status
– Positive or Negative
• Her-2 neu Expression– IHC graded 1+, 2+, 3+– FISH amplified

Staging Breast Cancer
• Early Stage (Stage I & II)
• Locally Advanced (Stage III)
• Metastatic (Stage IV)

Systemic Therapy Setting & Purpose
Early StageLocally Advanced Metastatic
No evidence of diseaseReduce risk of recurrence
Render inoperable operable
Commence systemic therapy
Reduce risk metastatic disease
Disease control

Early Stage Disease
Hormones Herceptin Chemo Clinical Trial
Hormone positive
HER-2 positive
Risk of recurrence
Access to new therapies
Tumour size / Grade / Age / Co-morbidities
60% 20%

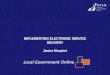
Rationale for Hormone Therapy
• Prevent breast cancer cells from receiving stimulation from endogenous estrogen
Beatson, 1896

Hypothalamus
Gonadotropins(FSH + LH)
Ovary
EstrogensProgesterone
ProlactinGrowth Hormone
Pituitary gland
Premenopausal and Postmenopausal
Adrenal gland
ProgesteroneAndrogensEstrogens
Corticosteroids
Premenopausal
Adrenocorticotropichormone (ACTH)
Estrogen Production in Premenopausal and Postmenopausal Patients
Aromatase inhibitors

Early
Breast Cancer Trialists Group Overview:
Tamoxifen
EBCTCG, Lancet 2005,365: 1687

Side Effects of Tamoxifen
Common side effectsHot flashes
Rare but serious side effectsThromboembolic diseaseEndometrial cancerCataracts
Issues with SSRIs

Hormonal Therapy in Postmenopausal Women

Aromatase Inhibitors- Mechanism of Action
Smith et al., N Engl J Med 348(24):2431-42 2003

DFS includes all deaths as a first event
At risk:A 2618 2540 2448 2355 2268 2014 830T 2598 2516 2398 2304 2189 1932 774
Follow-up time (years)
0
5
10
15
20
25
0 1 2 3 4 5 6
Absolute difference: 1.7% 2.4% 2.8% 3.7%
Pat
ien
ts (
%)
Anastrozole (A)
Tamoxifen (T)
HR
0.83
0.87
HR+
95% CI
(0.73–0.94)
(0.78-0.97)
P-value
0.005
0.01ITT
A
424
575
T
497
651
Howell A, et al. Lancet 2005
Recurrence Rate for HR+ Patients

Aromatase Inhibitors• Anastrazole (Arimidex), Femara (Letrozole), Aromasin (Exemestane)
• Improve outcome in postmenopausal women
• Side Effects– Osteopenia, Osteoporosis, Increased risk of fractures– Possible increase in cholesterol– Arthralgias

Adjuvant Chemotherapy

Progress in Chemotherapy for
Early Stage Breast Cancer Combination chemotherapy (CMF)
Use of anthracyclines
Addition of taxanes
Superior taxane containing regimens
Addition of trastuzumab
1970s
2000s
BUT: ALL chemotherapy is associated with toxicities and risks… need better ways to identify which patients will benefit from treatment

Adjuvant Chemotherapy
• Degree of benefit varies according to nodal status and patient age
• Degree of benefit varies according to sensitivity of tumor to hormones (ER+ vs. ER-)

Side effects
• Cardiac toxicity– Anthracyclines increase risk of congestive heart failure– Arrhythmias increased with taxanes– Radiation
• Neuropathy– Taxanes
• Hypersensitivity– Taxanes, require steroids
• Ovarian ablation– Premature menopause
» Infertility, Impaired quality of life, bone effects• Second malignancies

SO…How can we do better?
• Better selection of patients for treatment with chemotherapy
• Treat only those patients who are most likely to recur AND who will therefore benefit most from the addition of chemotherapy
• Take advantage of genomics

RS = + 0.47 x HER2 Group Score
- 0.34 x ER Group Score + 1.04 x Proliferation Group Score + 0.10 x Invasion Group Score + 0.05 x CD68 - 0.08 x GSTM1 - 0.07 x BAG1
Oncotype DX or Recurrence Score (RS) Assay for patients with ER + LN- disease
PROLIFERATIONKi-67
STK15Survivin
Cyclin B1MYBL2
ESTROGENERPR
Bcl2SCUBE2
INVASIONStromelysin 3Cathepsin L2
HER2GRB7HER2
BAG1GSTM1
REFERENCEBeta-actinGAPDHRPLPO
GUSTFRC
CD68
16 Cancer and 5 Reference Genes From 3 Studies
Category RS (0 – 100)Low risk RS < 18Int risk RS ≥ 18 and < 31
High risk RS ≥ 31

0%
5%
10%
15%
20%
25%
30%
35%
40%
0 5 10 15 20 25 30 35 40 45 50
Recurrence Score
Dis
tan
t R
ec
urr
en
ce
at
10
Ye
ars
Low Risk Group High Risk Group Intermediate Risk Group
Recurrence Score as a Continuous Predictor
My RS is 30, What is the chance of recurrence within 10 yrs?
My RS is 30, What is the chance of recurrence within 10 yrs?
95% CI

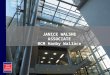
Oncotype DX™ Clinical Validation: B-14 Results – DRFS
DRFS for the three distinct cohorts identified
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 2 4 6 8 10 12 14 16
Years
DR
FS
P <0.00001
Low Risk (RS <18) n = 338
Intermediate Risk (RS 18-30) n = 149
High Risk (RS 31) n = 181
Paik et al. N Engl J Med. 2004;351:2817-2826.

B-14 Benefit of TamoxifenBy Recurrence Score Risk Category
Low Risk (RS<18)N
171142
Int Risk (RS 18-30)N8569
High Risk (RS≥31)1
N9979
Interaction P = 0.06
0 2 4 6 8 14 16
Years
0.0
0.2
0.4
0.6
0.8
1.0
DR
FS
PlaceboTamoxifen
1210
0 2 4 6 8 14 16
Years
0.0
0.2
0.4
0.6
0.8
1.0
DR
FS
PlaceboTamoxifen
1210 0 2 4 6 8 14 16
Years
0.0
0.2
0.4
0.6
0.8
1.0
DR
FS
PlaceboTamoxifen
1210
Paik et al. ASCO 2004. Abstract #510.
1 The results should not be used to indicate that tamoxifen should not be given to the high-risk group

Oncotype Dx: Chemotherapy benefit
• Patients with tumors that have high Recurrence Scores have a large absolute benefit of chemotherapy (similar results with CMF and MF)
• Patients with tumors that have low Recurrence Scores derive minimal, if any, benefit from chemotherapy
RS < 18 RS 18-30 RS ≥ 31
0 2 4 6 8 10 12
Years
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
DR
FS
Low R isk Patients (R S < 18) T am + C hemo T am
0 2 4 6 8 10 12
Years
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
DR
FS
Int Risk (RS 18 - 30) Tam + C hemo Tam
0 2 4 6 8 10 12
Years
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
DR
FS
H igh R isk Patients (R S 31) T am + C hemo T am
Paik et al, J Clin Oncol. 2006

Early Stage Breast Cancer –Overtreatment & Inadequate Treatment
Clinical features are not sufficiently predictive of relapse after primary therapy, resulting in…– Overtreatment, because…
– most patients with early stage disease will not have a future recurrence
– Inadequate treatment, because either…• treatment is not given because of favorable clinical features,
or • relapse occurs despite treatment

Biological or Targeted Therapy

Targeted therapies for Early Stage Breast
Cancer
• Treatments that ‘target’ specific proteins or receptors expressed by tumor– Hormonal therapy was the first targeted therapy for breast cancer
• Monoclonal antibodies– Trastuzumab (Herceptin)

HER2-normal (HER2-) breast epithelium cell (~20,000 receptors)
HER2-positive breast cancer cell (up to 1-2 million receptors)
HER-2 Positivity in Breast Cancer
• OVEREXPRESSION: marked increase in number of HER2 receptors on the cell surface
• AMPLIFICATION: increase in number of HER2/neu gene copies in the nucleus
Courtesy of Jeffrey Ross, Albany Medical College, Albany, NY.

Anti-
HER2
Antibodies: Mechanism of
ActionBaselga and Albanell. Ann Oncol. 2001;12(suppl 1):S35.
Noonberg and Benz. Drugs. 2000;59:753.
P
Excessive cell proliferation, survival, and angiogenesis
Potentiation of chemotherapy
Inhibition of tumor cell proliferation
Facilitation of immune function
PP
P PP P P

NSABP B-31/N9831 Joint Analysis: Impact of Adding Trastuzumab to AC Paclitaxel
on Disease-Free Survival*
*N9831 arm B (sequential trastuzumab after ACP) not included in joint analysis.
No. at risk 3351 2379 1455 801 133 0Control 1679 1162 689 374 59 0Trastuzumab 1672 1217 766 427 74 0
0
% S
urv
ivin
g d
isea
se-
free
1 2 3 4 50
50
60
70
80
90
100
Years after randomization
Trastuzumab(133 events)
P<0.0001HR=0.48
Control(261 events)
87.1%85.3%
67.1%
75.4%
Median FU 2.0 y
Romond et al. N Engl J Med., 2005;353:1673.

Adjuvant Trastuzumab: Room to Improve
• Generally well tolerated• Some patients will still recur• Intravenous infusion q1-3 wks for one year• Serious side effect: cardiotoxicity
Study Regimen Symptomatic CHF
B31/NCCTG AC TH 3.5 – 4.1%NCCTG AC T H 2.5%HERA Chemo H 0.6%BCIRG 006 TCH 0.4%FinHER H chemo 0%
Piccart-Gephardt, ASCO 2006

Early Stage Disease
Hormones Herceptin Chemo
Premenopausal Postmenopausal
Tamoxifen Tamoxifen
Aromatase Inhibitors
IV
3wkly for 1 year
Cardiac monitoring
Multiple regimens
4-6 months
Alopecia / Mucositis / Sepsis

Locally Advanced Breast Cancer• Same Treatment but Different Sequence
• Systemic therapy first (CT/HT)
• Definitive surgery later

Metastatic disease: Principles of Treatment
• Hormonal therapy for indolent disease
• Single agent chemotherapy for aggressive/symptomatic disease or disease not responding to hormonal therapy
• Polyagent chemotherapy for visceral crisis or disease requiring rapid response
• Iv bisphosphonates for bone secondaries

Trastuzumab emtansine (T-DM1): A unique ADC- KADLYCA
• The mAb, trastuzumab, is conjugated by a thioether linker to the highly potent antimicrotubule agent DM1
– Targets HER2-positive tumor cells
Junttila et al. Br Cancer Res 2011
Trastuzumab
DM1
Thioetherlinker

T-DM1 MoA: Binding of T-DM1
• The trastuzumab component of T-DM1 binds to HER2 receptors on the tumor cell surface
– Leads to downstream signaling inhibition/blockade
Lewis Phillips et al. Cancer Res 2008

T-DM1 MoA: Endocytosis
• HER2 receptor–T-DM1 complex is internalized into the tumor cell via endocytosis
Erickson et al. Cancer Res 2006

T-DM1 MoA: Lysosomal degradation
• Once endocytosis is complete, trastuzumab and the HER2 receptor are degraded and a cytotoxic metabolite* is released
Erickson et al. Cancer Res 2006Lewis Phillips et al. Cancer Res 2008
*Lysine-bound emtansine plus linker

47
How Much Breast and Ovarian Cancer Is Hereditary?
Sporadic
Family clusters
Hereditary
Ovarian CancerBreast Cancer
5%–10% ~10%
15%-20%

48
Features Consistent with Hereditary Breast/Ovarian Cancer
Multiple cases of early onset breast cancer Ovarian cancer (with family history of breast or
ovarian cancer) Breast and ovarian cancer in the same woman Bilateral breast cancer Ashkenazi Jewish heritage Male breast cancer

Treatment is finished- what now?
• Purpose of follow up:– Deal with complications of therapy– Detect recurrence / metastatic disease– Encourage adherence to anti-hormonal therapy
• How?– History, Examination & Annual Mammogram– In asymptomatic women:
» Tumour markers / routine scanning are not associated with a survival benefit and are not recommended

Metastatic Disease is slightly different…
• Tumour markers may be helpful in making clinical decisions
• Restaging studies every 3-6 months to determine progression, sooner if symptomatic, clinically warranted

Lifestyle Modifications• Obesity increases risk of postmenopausal breast
cancer-Maintain a normal Body mass index
• Evidence suggests that physical activity decreases risk of breast cancer and risk of recurrence- Get Active
• Low fat diet decreases risk of breast cancer recurrence – Balanced Healthy Diet
• Moderate alcohol intake-

Breast Cancer Treatment: Progress and Promise
• Chemotherapy– Better treatments– Progress toward targeting only those who will benefit
• Hormonal therapy– AIs improve outcome in postmenopausal women– Premenopausal women – optimal hormonal treatment still
unknown
• Targeted therapy– Trastuzumab decreases risk of recurrence and improves survival– Promising new agents being studied
• Access and participation in well designed clinical trials holds the key to further improvements











![Nicole Marie Walshe [McCann]](https://img.pdfslide.us/doc/110x75/55cf9754550346d033910855/nicole-marie-walshe-mccann.jpg)