Embed Size (px)
DESCRIPTION
Citation preview
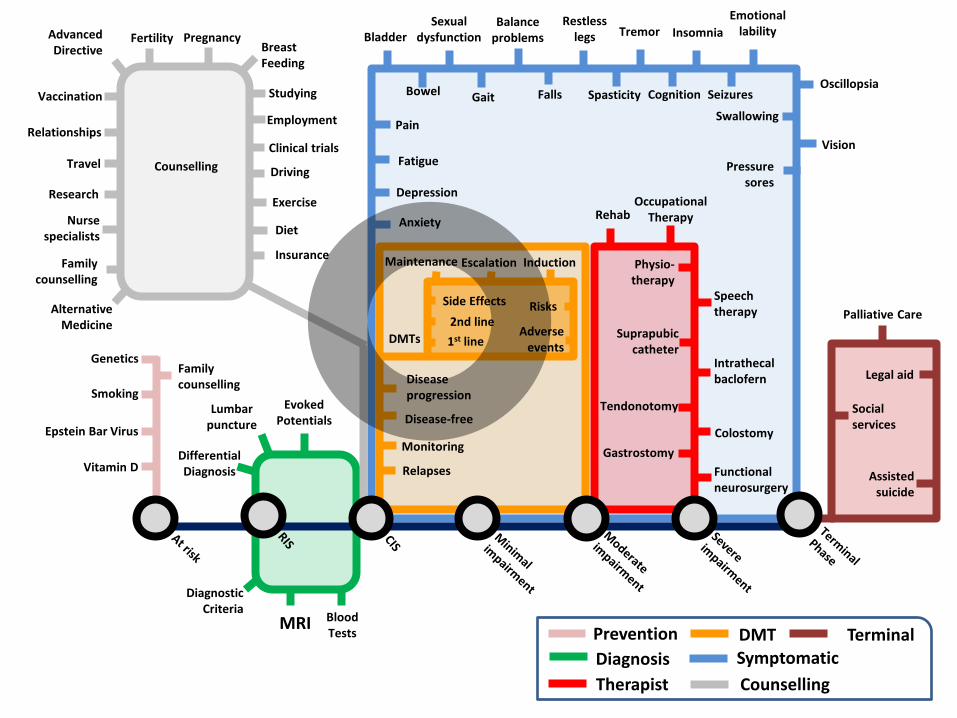
Treatment Highlights
Gavin Giovannoni
Barts and The London School of Medicine and Dentistry
TOWER
The efficacy and safety of teriflunomide in patients with relapsing MS: results from TOWER, a Phase III placebo-controlled study
Ludwig Kappos,1 Giancarlo Comi,2 Christian Confavreux,3 Mark S. Freedman,4 Aaron E. Miller,5 Tomas P. Olsson,6
Jerry S. Wolinsky,7 Teresa Bagulho,8 Jean-Luc Delhay,9 Yan Zheng,8 Philippe Truffinet9 and Paul O’ Connor10
NCT00751881
1University Hospital Basel, Basel, Switzerland; 2University Vita-Salute San Raffaele, Milan, Italy; 3Université Claude Bernard Lyon 1, Lyon, France; 4University of Ottawa, Ottawa, ON, Canada; 5Mount Sinai School of Medicine, New York, NY, USA; 6Karolinska Institute, Stockholm, Sweden; 7University of Texas Health Science Center, Houston, TX, USA; 8Genzyme, a Sanofi company, Bridgewater, NJ, USA; 9Genzyme, a Sanofi company, Chilly Mazarin, France; 10University of Toronto, Toronto, ON, Canada
#1
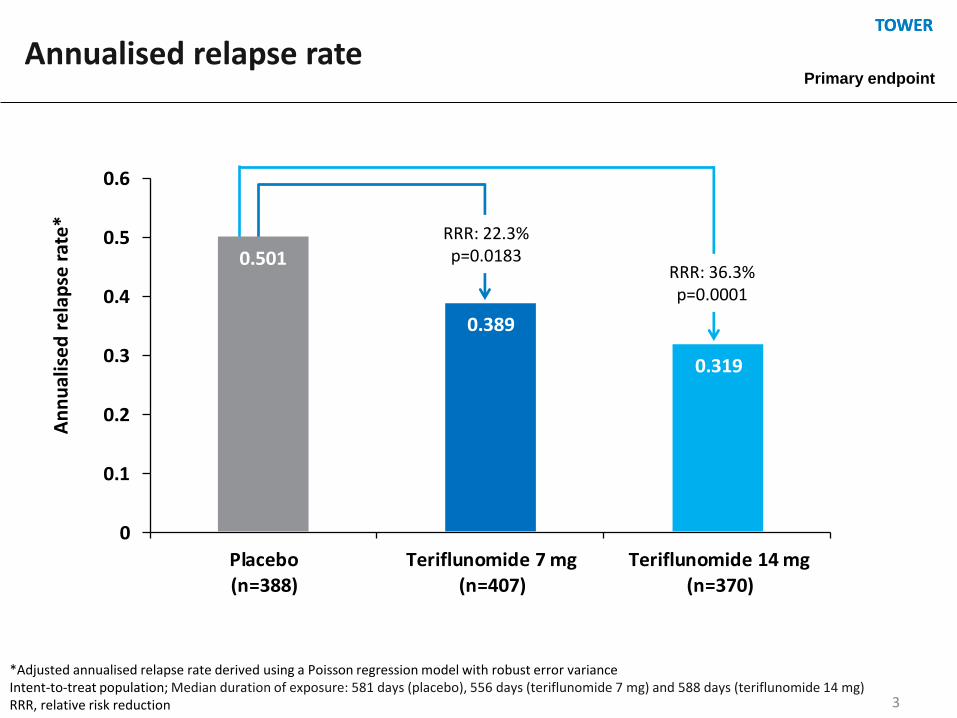
TOWER TOWER
3
0.501
0.389
0.319
0
0.1
0.2
0.3
0.4
0.5
0.6
Placebo(n=388)
Teriflunomide 7 mg(n=407)
Teriflunomide 14 mg(n=370)
RRR: 22.3% p=0.0183
RRR: 36.3% p=0.0001
An
nu
alis
ed
re
lap
se r
ate
*
Annualised relapse rate
*Adjusted annualised relapse rate derived using a Poisson regression model with robust error variance Intent-to-treat population; Median duration of exposure: 581 days (placebo), 556 days (teriflunomide 7 mg) and 588 days (teriflunomide 14 mg) RRR, relative risk reduction
Primary endpoint


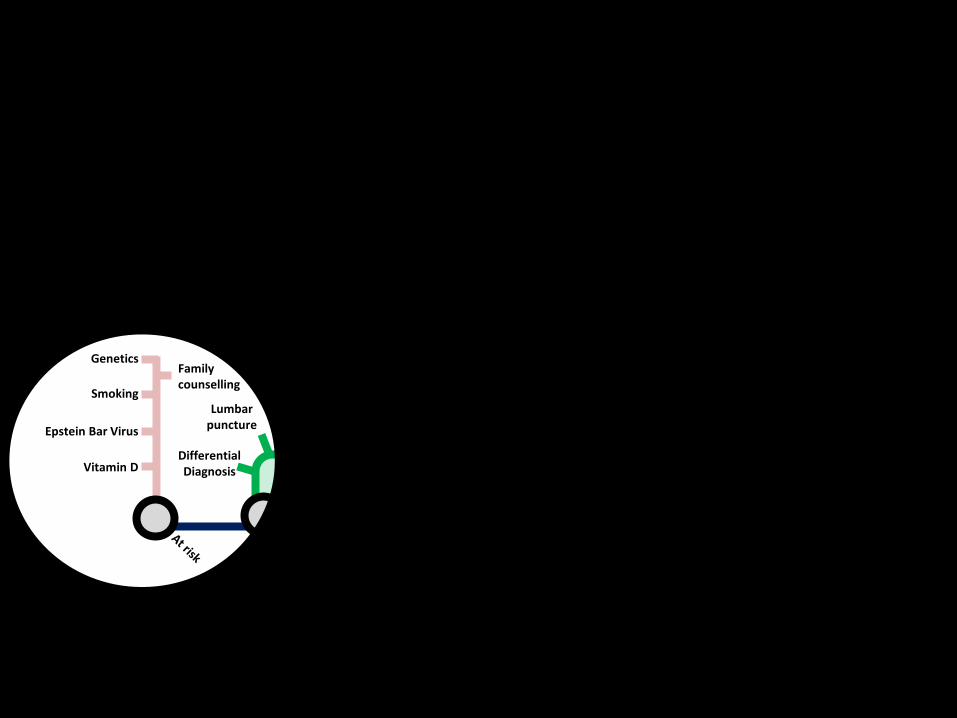
Epstein Bar Virus
Genetics
Vitamin D
Smoking
Risks
Adverse events
Differential Diagnosis
MRI
Evoked Potentials
Lumbar puncture
Blood Tests
Diagnostic Criteria
Cognition
Depression
Fatigue
Bladder
Bowel
Sexual dysfunction Tremor
Pain Swallowing
Spasticity Falls
Balance problems Insomnia
Restless legs Fertility
Clinical trials
Gait
Pressure sores
Oscillopsia
Emotional lability
Seizures
Gastrostomy
Rehab
Suprapubic catheter
Intrathecal baclofern
Physio- therapy
Speech therapy
Occupational Therapy
Functional neurosurgery
Colostomy
Tendonotomy
Studying
Employment Relationships
Travel
Vaccination
Anxiety
Driving
Nurse specialists
Counselling
Family counselling
Relapses
1st line
2nd line
Maintenance Escalation Induction
Monitoring
Disease-free
Disease progression
DMTs
Side Effects
Advanced Directive
Exercise
Diet
Alternative Medicine
Pregnancy Breast Feeding
Research
Insurance
Vision
Palliative Care
Assisted suicide
Social services
Legal aid Family counselling
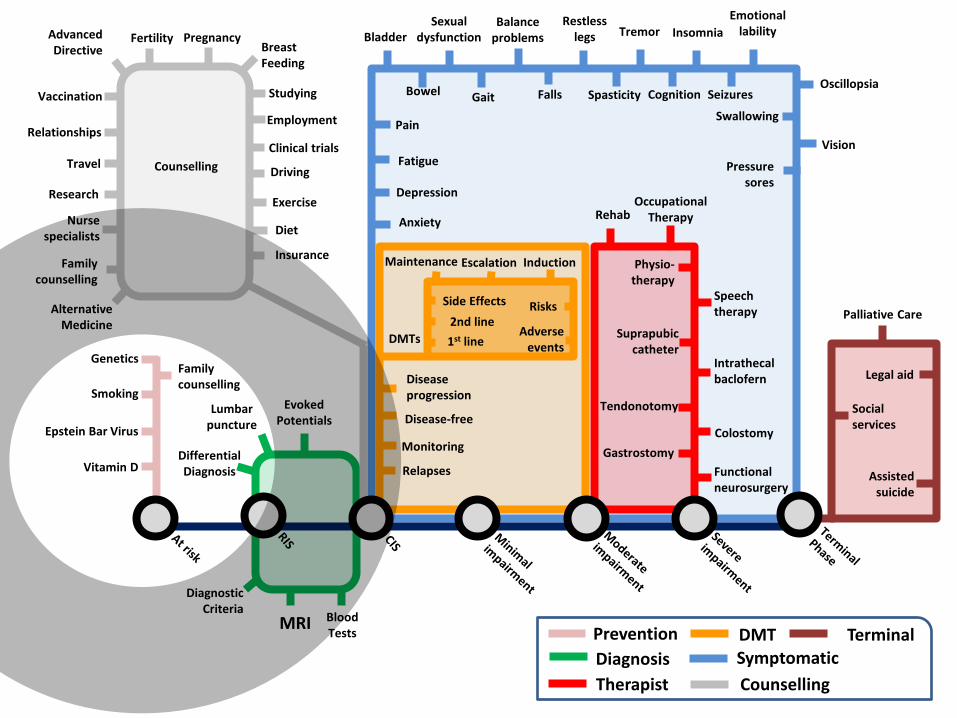
Prevention
Diagnosis
DMT Symptomatic
Therapist
Terminal
Counselling
Epstein Bar Virus
Genetics
Vitamin D
Smoking
Risks
Adverse events
Differential Diagnosis
MRI
Evoked Potentials
Lumbar puncture
Blood Tests
Diagnostic Criteria
Cognition
Depression
Fatigue
Bladder
Bowel
Sexual dysfunction Tremor
Pain Swallowing
Spasticity Falls
Balance problems Insomnia
Restless legs Fertility
Clinical trials
Gait
Pressure sores
Oscillopsia
Emotional lability
Seizures
Gastrostomy
Rehab
Suprapubic catheter
Intrathecal baclofern
Physio- therapy
Speech therapy
Occupational Therapy
Functional neurosurgery
Colostomy
Tendonotomy
Studying
Employment Relationships
Travel
Vaccination
Anxiety
Driving
Nurse specialists
Counselling
Family counselling
Relapses
1st line
2nd line
Maintenance Escalation Induction
Monitoring
Disease-free
Disease progression
DMTs
Side Effects
Advanced Directive
Exercise
Diet
Alternative Medicine
Pregnancy Breast Feeding
Research
Insurance
Vision
Palliative Care
Assisted suicide
Social services
Legal aid Family counselling
Prevention
Diagnosis
DMT Symptomatic
Therapist
Terminal
Counselling
www.ms-res.org

MS-STAT trial
High dose oral Simvastatin
in Secondary Progressive Multiple Sclerosis
Jeremy Chataway
for the MS-STAT Collaborators
CTN:NCT00647348
EUDRACT NUMBER 2006-006347-31
#2
Slides deleted
Where to next?
Slides deleted
It is time to change the way we measure change:
demonstration, explanation, recommendation
Jeremy Hobart, Stefan Cano, Alan Thompson, David Andrich
Plymouth, London, Perth AU
ECTRIMS Lyon 12 October 2012
#4
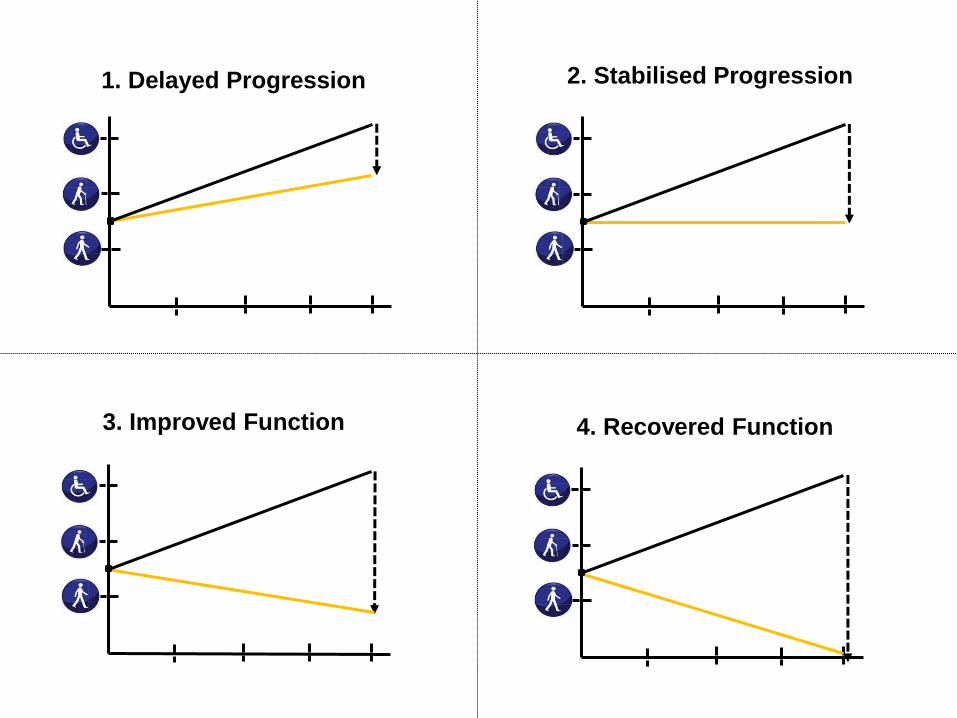
1. Delayed Progression 2. Stabilised Progression
3. Improved Function 4. Recovered Function
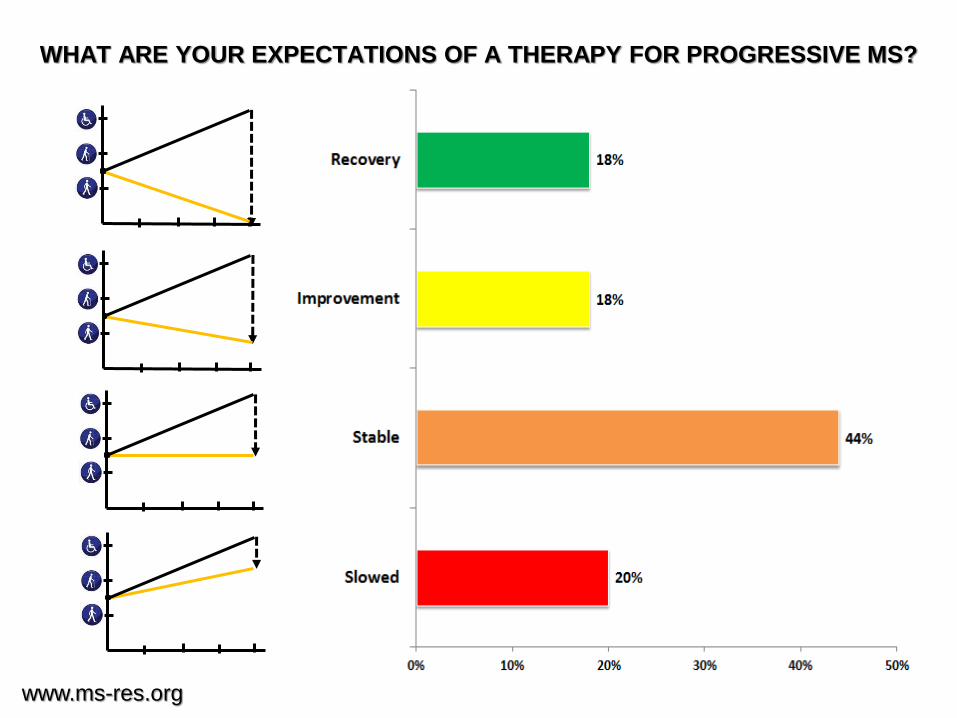
WHAT ARE YOUR EXPECTATIONS OF A THERAPY FOR PROGRESSIVE MS?
16
1
2
3
www.ms-res.org
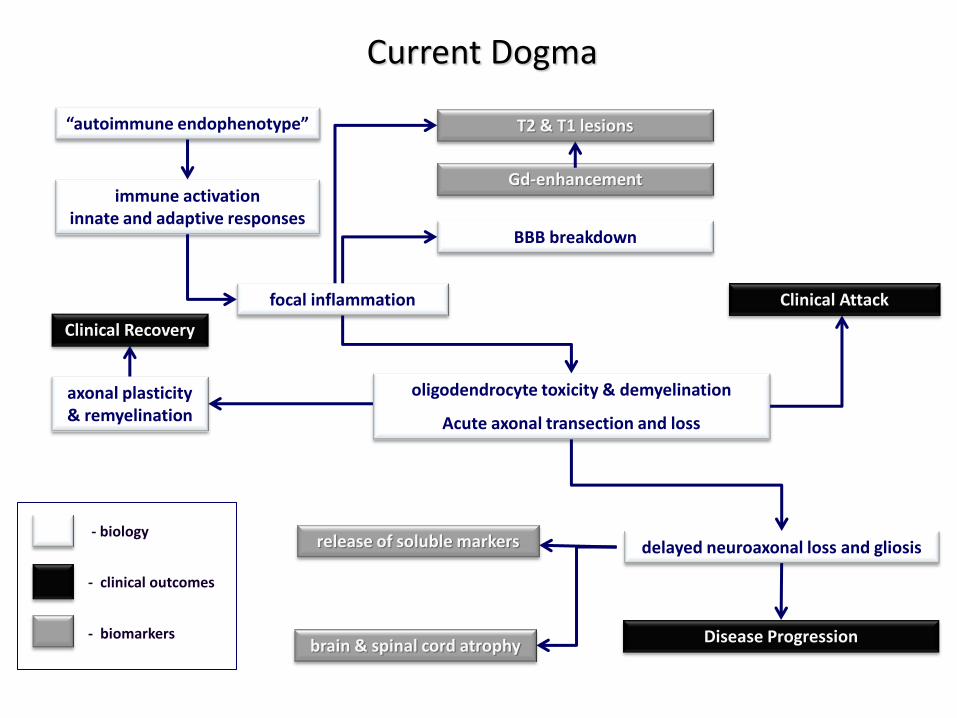
Current Dogma
immune activation innate and adaptive responses
focal inflammation
BBB breakdown
oligodendrocyte toxicity & demyelination
Acute axonal transection and loss
“autoimmune endophenotype”
axonal plasticity & remyelination
delayed neuroaxonal loss and gliosis
Gd-enhancement
T2 & T1 lesions
brain & spinal cord atrophy
release of soluble markers
Clinical Attack
Disease Progression
Clinical Recovery
- biology
- clinical outcomes
- biomarkers
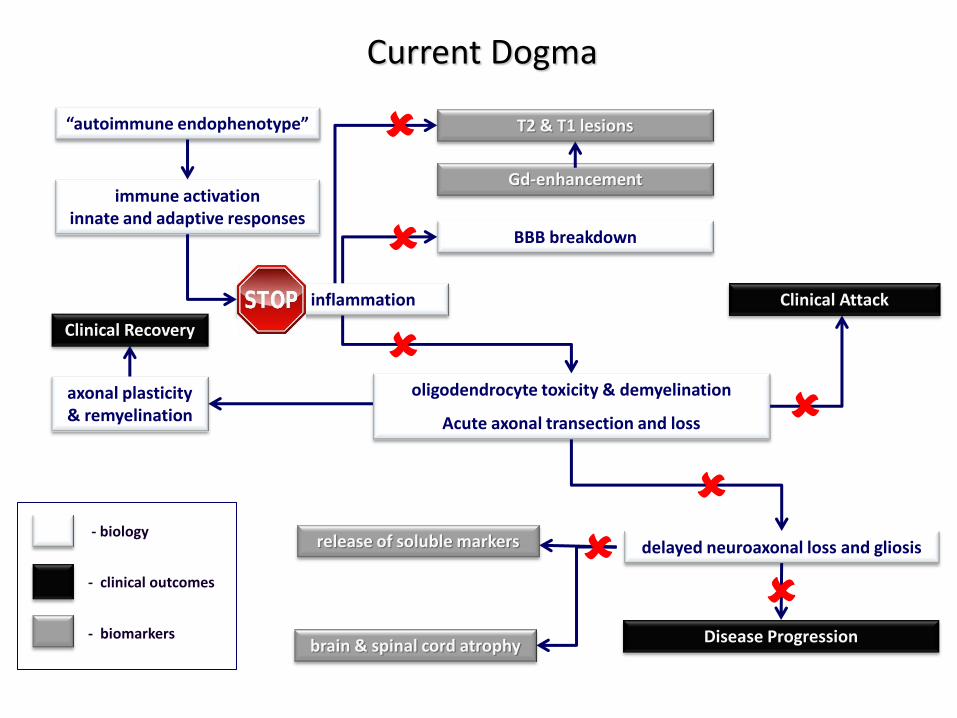
Current Dogma
immune activation innate and adaptive responses
focal inflammation
BBB breakdown
oligodendrocyte toxicity & demyelination
Acute axonal transection and loss
“autoimmune endophenotype”
axonal plasticity & remyelination
delayed neuroaxonal loss and gliosis
Gd-enhancement
T2 & T1 lesions
brain & spinal cord atrophy
release of soluble markers
Clinical Attack
Disease Progression
Clinical Recovery
- biology
- clinical outcomes
- biomarkers
56.0
42.0
27.0
74.0
51.0
39.0
0
10
20
30
40
50
60
70
80
Clinical disease
activity-free
MRI
activity-free
MS disease
activity-free
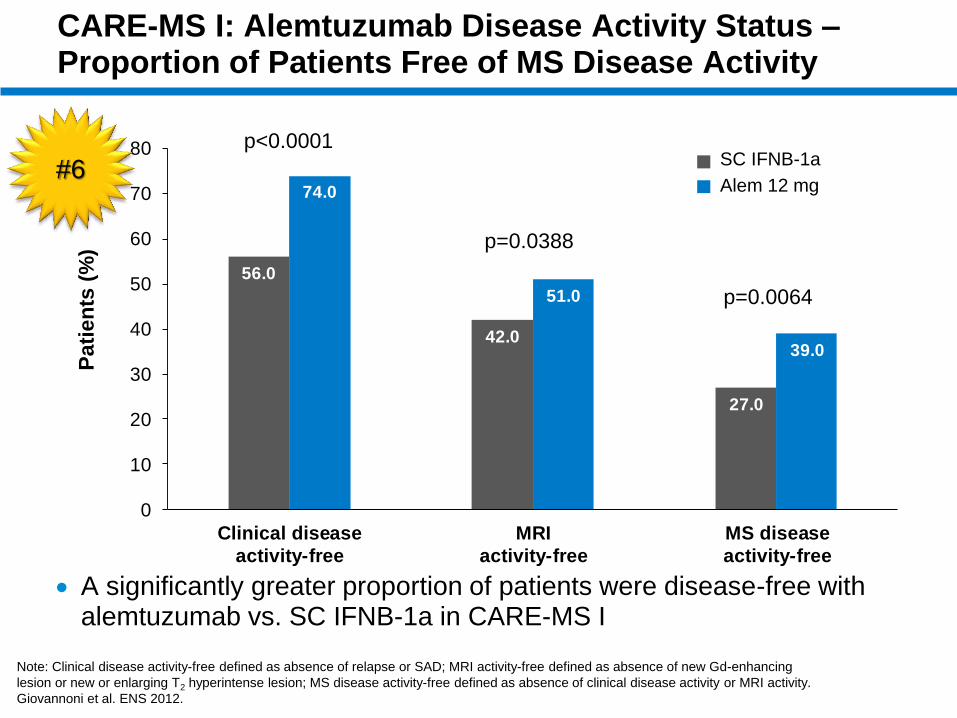
CARE-MS I: Alemtuzumab Disease Activity Status – Proportion of Patients Free of MS Disease Activity
A significantly greater proportion of patients were disease-free with alemtuzumab vs. SC IFNB-1a in CARE-MS I
41.1
Pa
tie
nts
(%
)
Note: Clinical disease activity-free defined as absence of relapse or SAD; MRI activity-free defined as absence of new Gd-enhancing
lesion or new or enlarging T2 hyperintense lesion; MS disease activity-free defined as absence of clinical disease activity or MRI activity.
Giovannoni et al. ENS 2012.
p<0.0001
p=0.0388
p=0.0064
SC IFNB-1a
Alem 12 mg #6
#7
Epstein Bar Virus
Genetics
Vitamin D
Smoking
Risks
Adverse events
Differential Diagnosis
MRI
Evoked Potentials
Lumbar puncture
Blood Tests
Diagnostic Criteria
Cognition
Depression
Fatigue
Bladder
Bowel
Sexual dysfunction Tremor
Pain Swallowing
Spasticity Falls
Balance problems Insomnia
Restless legs Fertility
Clinical trials
Gait
Pressure sores
Oscillopsia
Emotional lability
Seizures
Gastrostomy
Rehab
Suprapubic catheter
Intrathecal baclofern
Physio- therapy
Speech therapy
Occupational Therapy
Functional neurosurgery
Colostomy
Tendonotomy
Studying
Employment Relationships
Travel
Vaccination
Anxiety
Driving
Nurse specialists
Counselling
Family counselling
Relapses
1st line
2nd line
Maintenance Escalation Induction
Monitoring
Disease-free
Disease progression
DMTs
Side Effects
Advanced Directive
Exercise
Diet
Alternative Medicine
Pregnancy Breast Feeding
Research
Insurance
Vision
Palliative Care
Assisted suicide
Social services
Legal aid Family counselling
Prevention
Diagnosis
DMT Symptomatic
Therapist
Terminal
Counselling
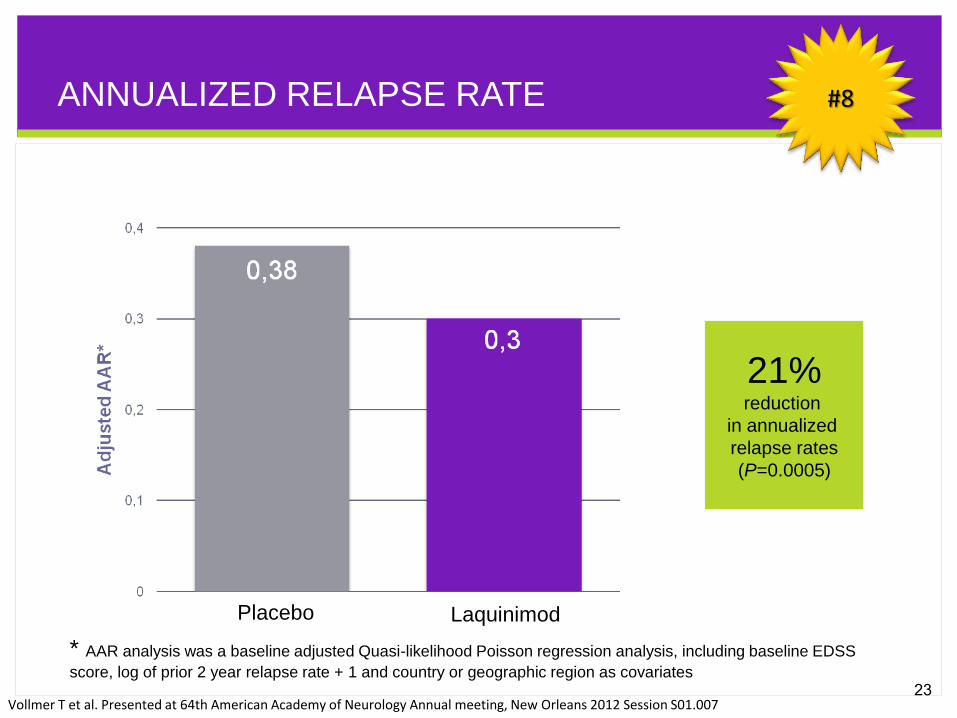
**
Placebo Laquinimod
21% reduction
in annualized
relapse rates
(P=0.0005)
ANNUALIZED RELAPSE RATE
23
* AAR analysis was a baseline adjusted Quasi-likelihood Poisson regression analysis, including baseline EDSS
score, log of prior 2 year relapse rate + 1 and country or geographic region as covariates
Vollmer T et al. Presented at 64th American Academy of Neurology Annual meeting, New Orleans 2012 Session S01.007
#8
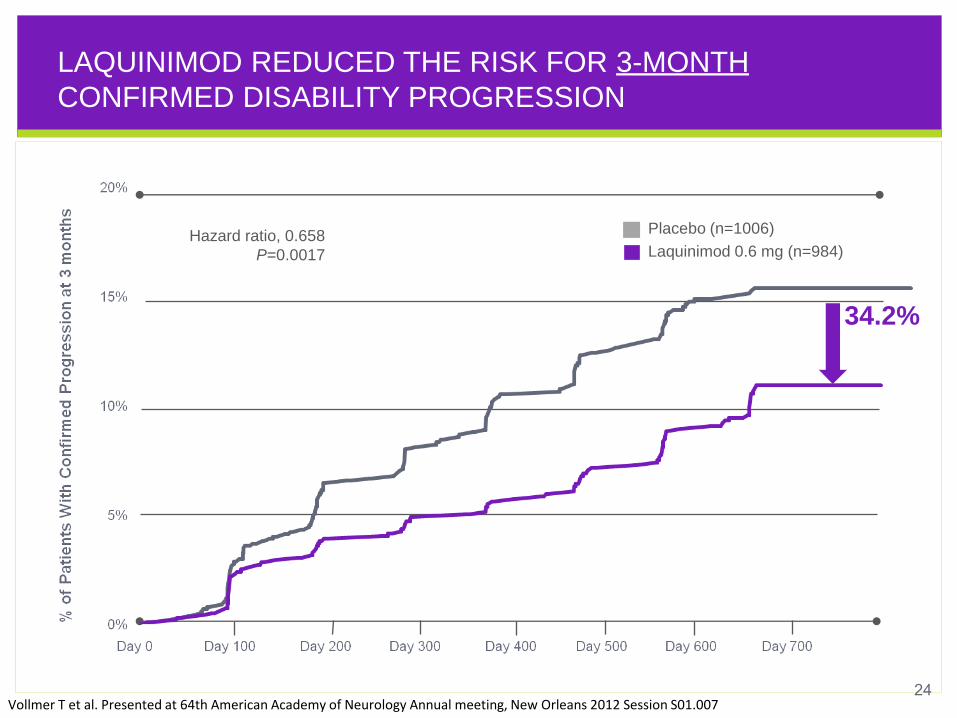
LAQUINIMOD REDUCED THE RISK FOR 3-MONTH
CONFIRMED DISABILITY PROGRESSION
Placebo (n=1006)
Laquinimod 0.6 mg (n=984)
Hazard ratio, 0.658
P=0.0017
34.2%
24 Vollmer T et al. Presented at 64th American Academy of Neurology Annual meeting, New Orleans 2012 Session S01.007
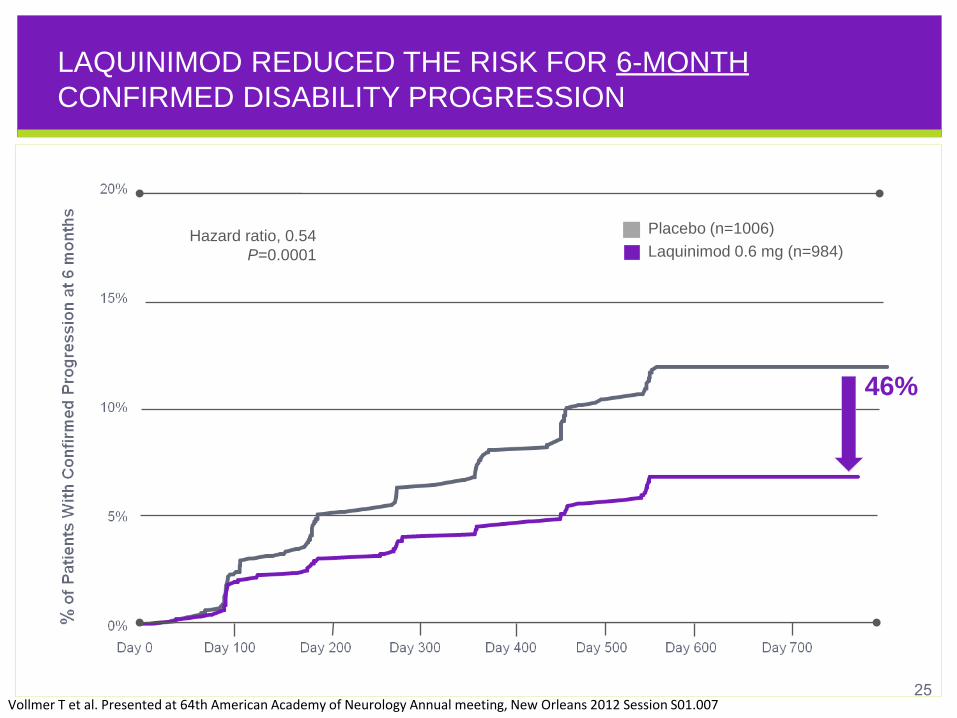
LAQUINIMOD REDUCED THE RISK FOR 6-MONTH
CONFIRMED DISABILITY PROGRESSION
Placebo (n=1006)
Laquinimod 0.6 mg (n=984)
Hazard ratio, 0.54
P=0.0001
46%
25 Vollmer T et al. Presented at 64th American Academy of Neurology Annual meeting, New Orleans 2012 Session S01.007
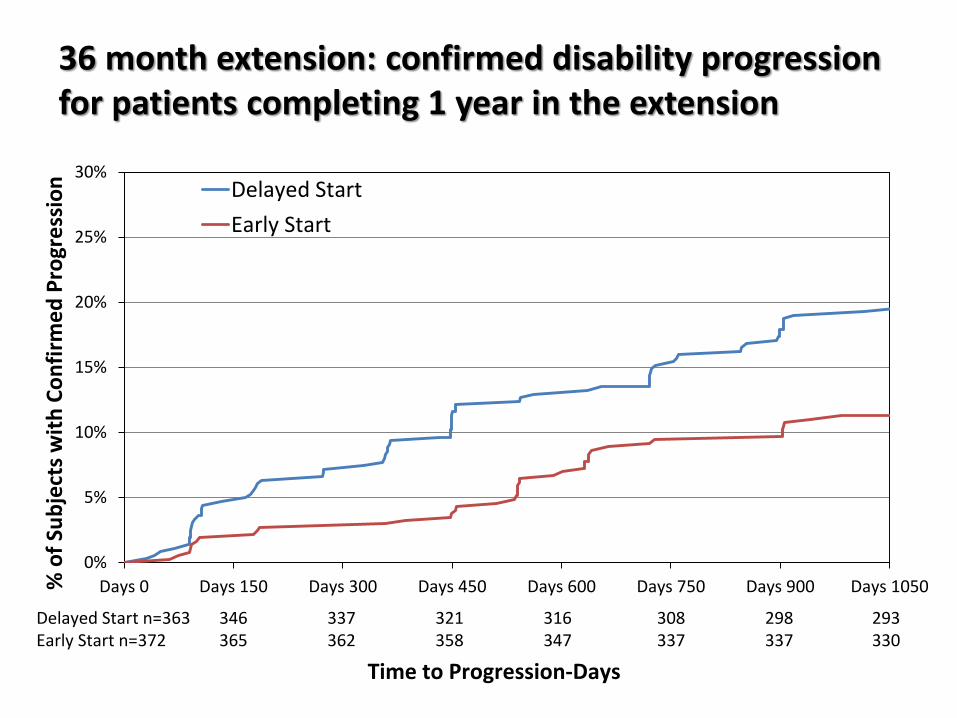
36 month extension: confirmed disability progression for patients completing 1 year in the extension
0%
5%
10%
15%
20%
25%
30%
Days 0 Days 150 Days 300 Days 450 Days 600 Days 750 Days 900 Days 1050
Delayed Start
Early Start
Time to Progression-Days
% o
f Su
bje
cts
wit
h C
on
firm
ed
Pro
gre
ssio
n
Delayed Start n=363 346 337 321 316 308 298 293 Early Start n=372 365 362 358 347 337 337 330
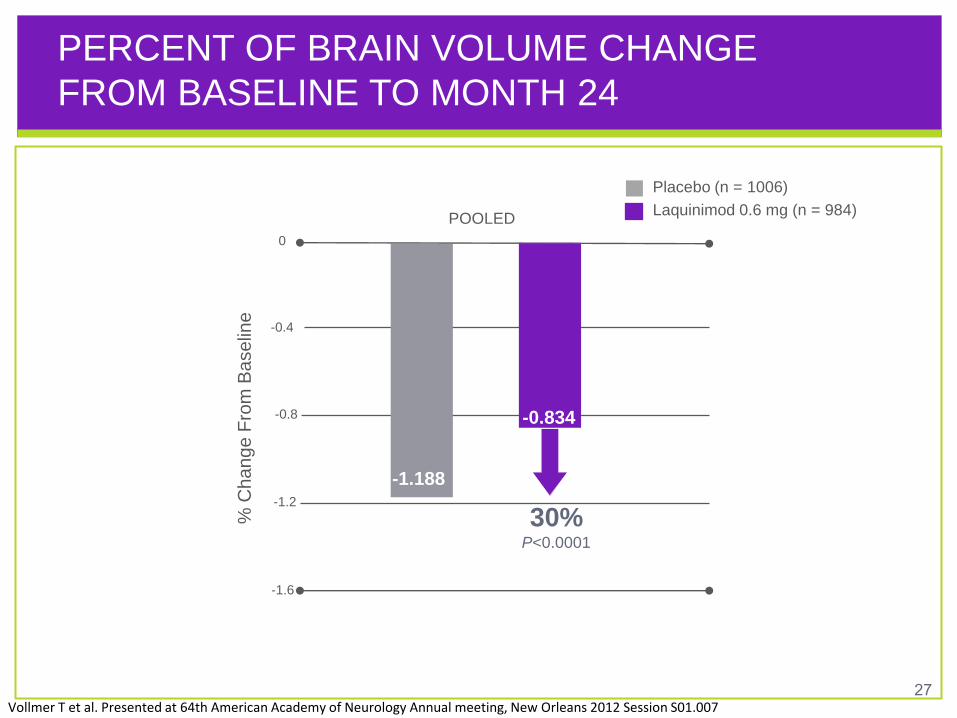
PERCENT OF BRAIN VOLUME CHANGE
FROM BASELINE TO MONTH 24
% C
ha
ng
e F
rom
Ba
se
line
-1.2
-0.4
-1.6
-0.8
Placebo (n = 1006)
Laquinimod 0.6 mg (n = 984)
0
-1.188
-0.834
POOLED
27
30% P<0.0001
Vollmer T et al. Presented at 64th American Academy of Neurology Annual meeting, New Orleans 2012 Session S01.007
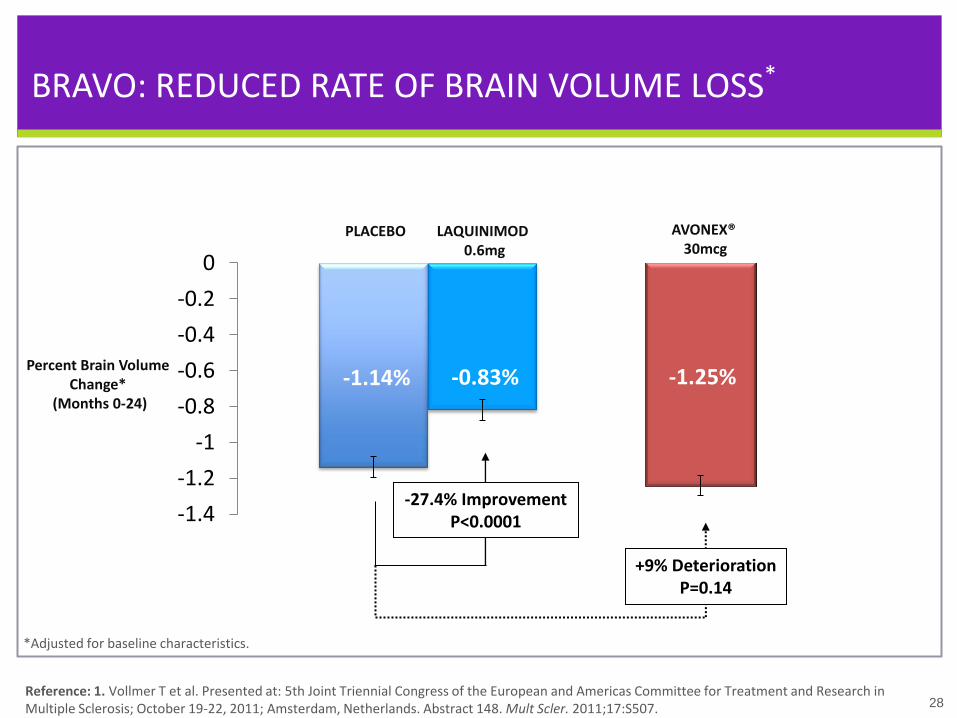
BRAVO: REDUCED RATE OF BRAIN VOLUME LOSS*
*Adjusted for baseline characteristics.
Reference: 1. Vollmer T et al. Presented at: 5th Joint Triennial Congress of the European and Americas Committee for Treatment and Research in Multiple Sclerosis; October 19-22, 2011; Amsterdam, Netherlands. Abstract 148. Mult Scler. 2011;17:S507.
28
27.5% Reduction P<0.0001
28
*Adjusted for baseline characteristics.
-27.4% Improvement P<0.0001 -1.4
-1.2
-1
-0.8
-0.6
-0.4
-0.2
0
LAQUINIMOD 0.6mg
PLACEBO
-1.14% -0.83% Percent Brain Volume
Change* (Months 0-24)
-1.25%
AVONEX® 30mcg
+9% Deterioration P=0.14
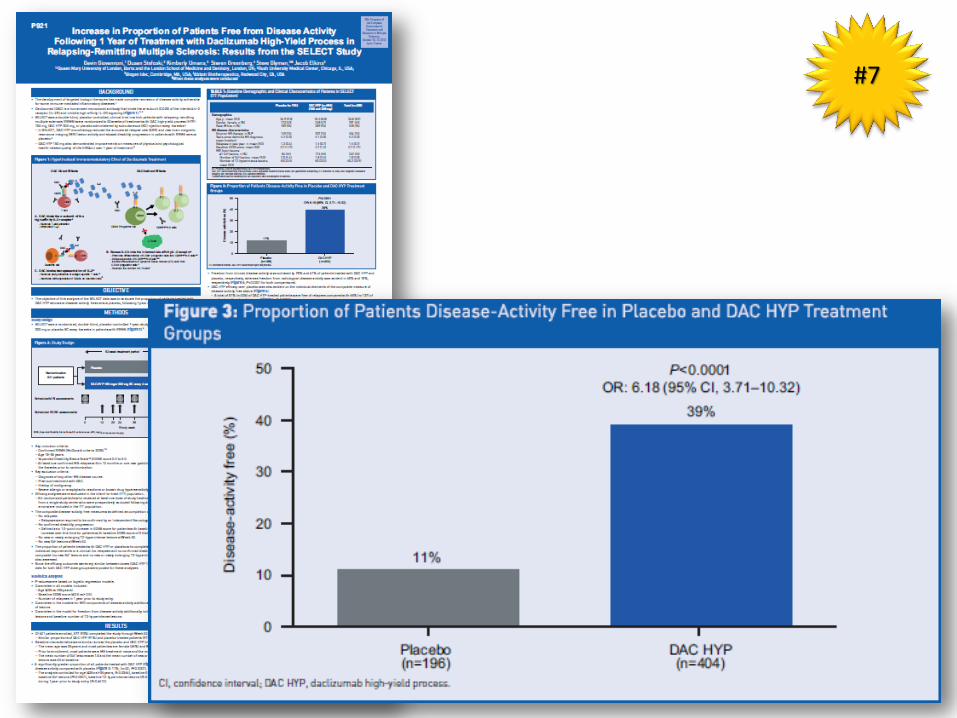
Primary Results of the SELECTION Trial of
Daclizumab HYP in Relapsing Multiple
Sclerosis
Gavin Giovannoni1, Ralf Gold2, Krzysztof Selmaj3,
Eva Havrdova4, Xavier Montalban5, Ernst-Wilhelm
Radue6, Dusan Stefoski7, Manjit McNeill8, Jitesh
Rana8, Jacob Elkins8, and Gilmore O’Neill8
1Queen Mary University of London, Barts and The London School of Medicine and Dentistry, London,
UK; 2St. Josef-Hospital/Ruhr-University Bochum, Bochum, Germany; 3Medical University of Lodz, Lodz,
Poland; 4Charles University in Prague, Prague, Czech Republic; 5Hospital Vall d'Hebron University,
Barcelona, Spain; 6University Hospital Basel, Basel, Switzerland. 7Rush University Medical Center,
Chicago, IL. USA; 8Biogen Idec, Cambridge, MA, USA
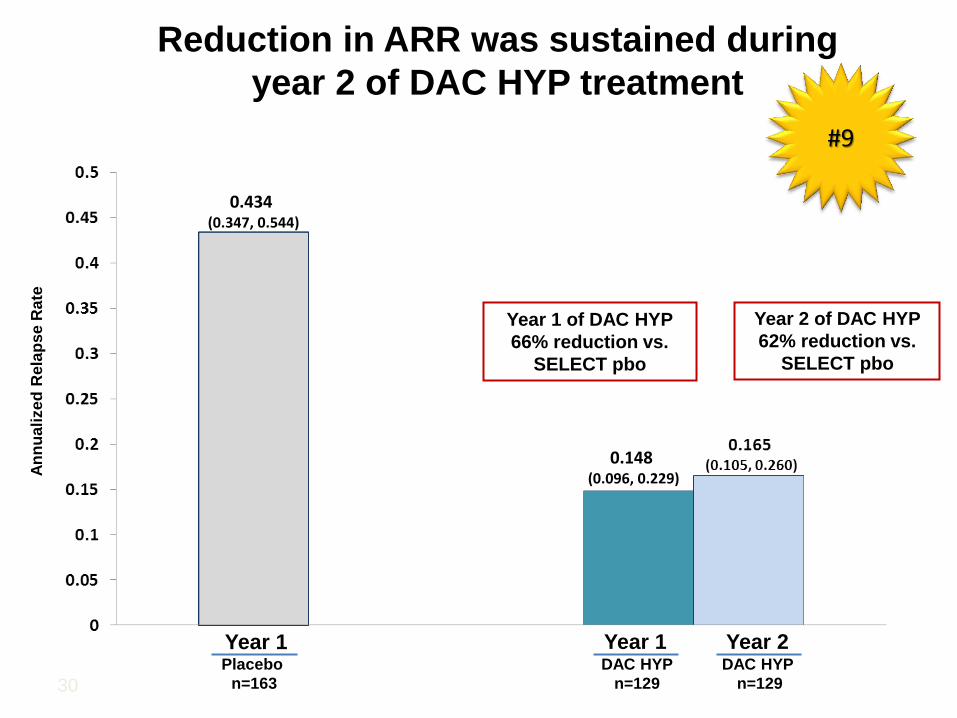
Reduction in ARR was sustained during
year 2 of DAC HYP treatment
30
0.434 (0.347, 0.544)
Year 2 of DAC HYP
62% reduction vs.
SELECT pbo
Year 1 of DAC HYP
66% reduction vs.
SELECT pbo
0.148 (0.096, 0.229)
Placebo
n=163
Year 1 Year 1 Year 2 DAC HYP
n=129
DAC HYP
n=129
An
nu
ali
ze
d R
ela
pse
Rate
#9
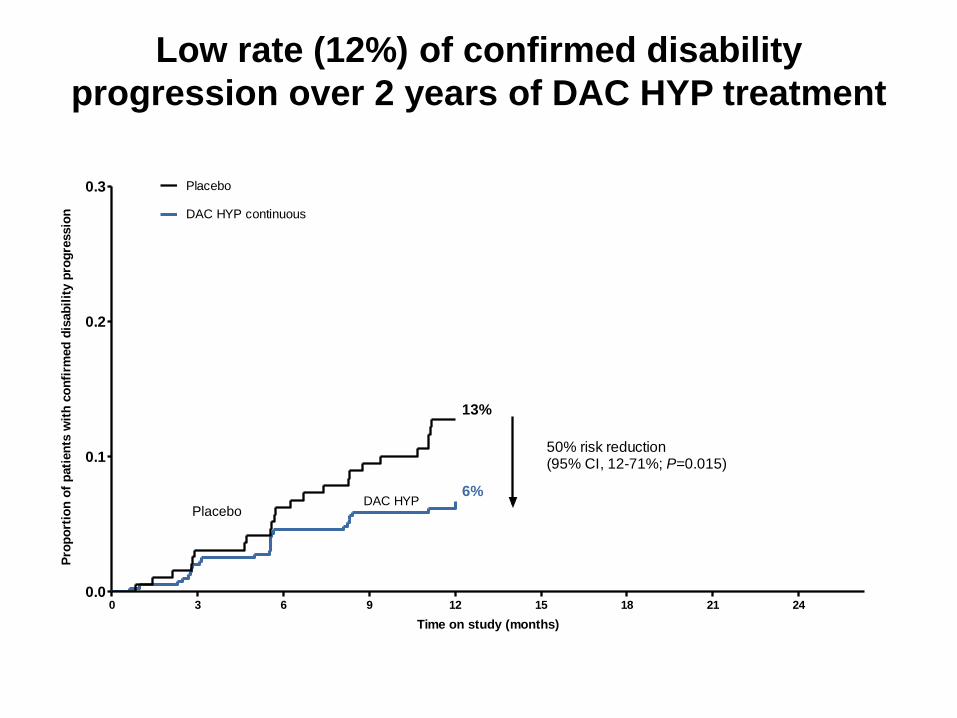
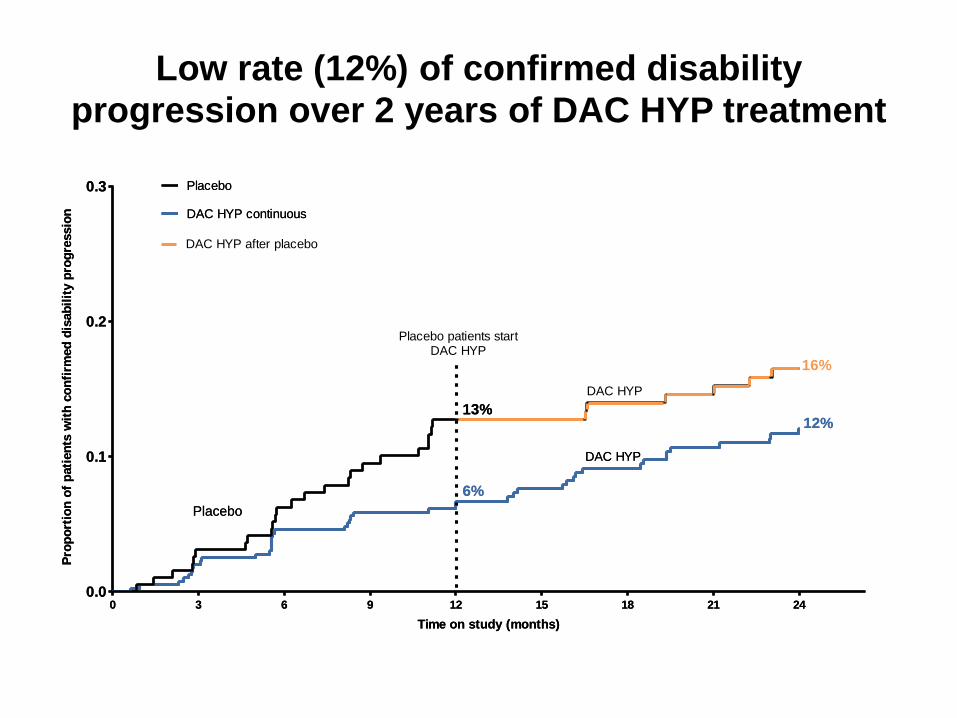
Low rate (12%) of confirmed disability
progression over 2 years of DAC HYP treatment
0.0
0.1
0.2
0.3
DAC HYP continuous
0 12 2463 9 15 18 21
DAC HYP Placebo
Placebo
6%
13%
50% risk reduction(95% CI, 12-71%; P=0.015)
Time on study (months)
Pro
po
rtio
n o
f p
ati
en
ts w
ith
co
nfi
rmed
dis
ab
ilit
y p
rog
ressio
n
0.0
0.1
0.2
0.3
DAC HYP continuous
0 12 2463 9 15 18 21
DAC HYP
Placebo
Placebo
6%
13%12%
Time on study (months)
Pro
po
rtio
n o
f p
ati
en
ts w
ith
co
nfi
rmed
dis
ab
ilit
y p
rog
ressio
n
0.0
0.1
0.2
0.3
DAC HYP continuous
0 12 2463 9 15 18 21
DAC HYP
Placebo
Placebo
16%
12%
DAC HYP
DAC HYP after placebo
6%
13%
Placebo patients startDAC HYP
Time on study (months)
Pro
po
rtio
n o
f p
ati
en
ts w
ith
co
nfi
rmed
dis
ab
ilit
y p
rog
ressio
nLow rate (12%) of confirmed disability
progression over 2 years of DAC HYP treatment
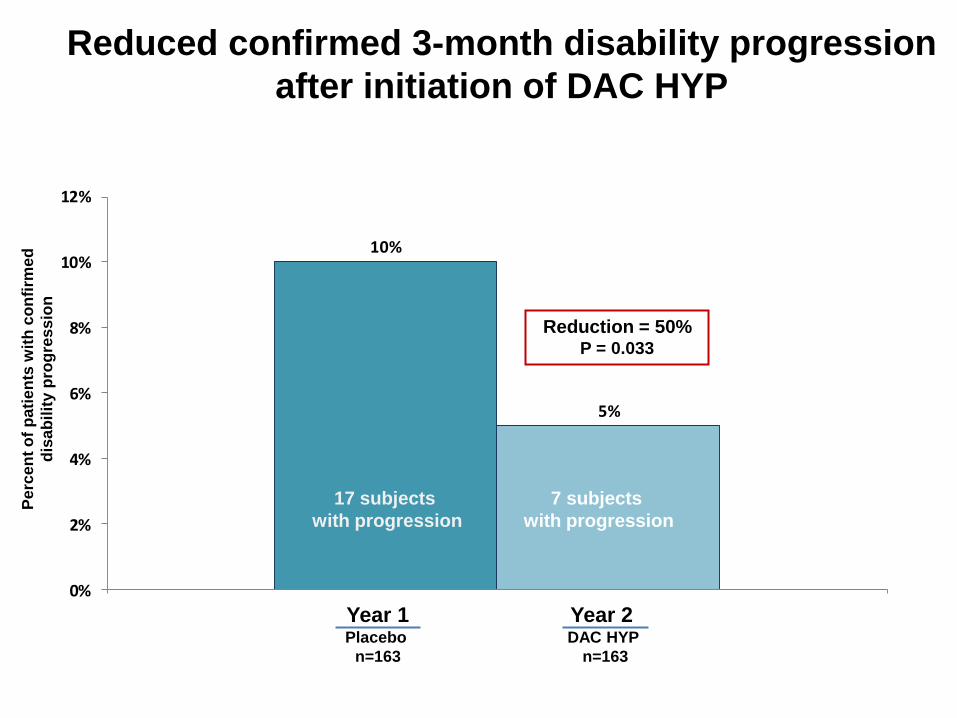
Reduced confirmed 3-month disability progression
after initiation of DAC HYP
10%
5%
0%
2%
4%
6%
8%
10%
12%
Reduction = 50% P = 0.033
17 subjects
with progression
Year 1 Year 2
7 subjects
with progression
Placebo
n=163
DAC HYP
n=163
Pe
rce
nt
of
pati
en
ts w
ith
co
nfi
rme
d
dis
ab
ilit
y p
rog
res
sio
n
#10
Do these two examples suggest that relapses are not related to disease progression?
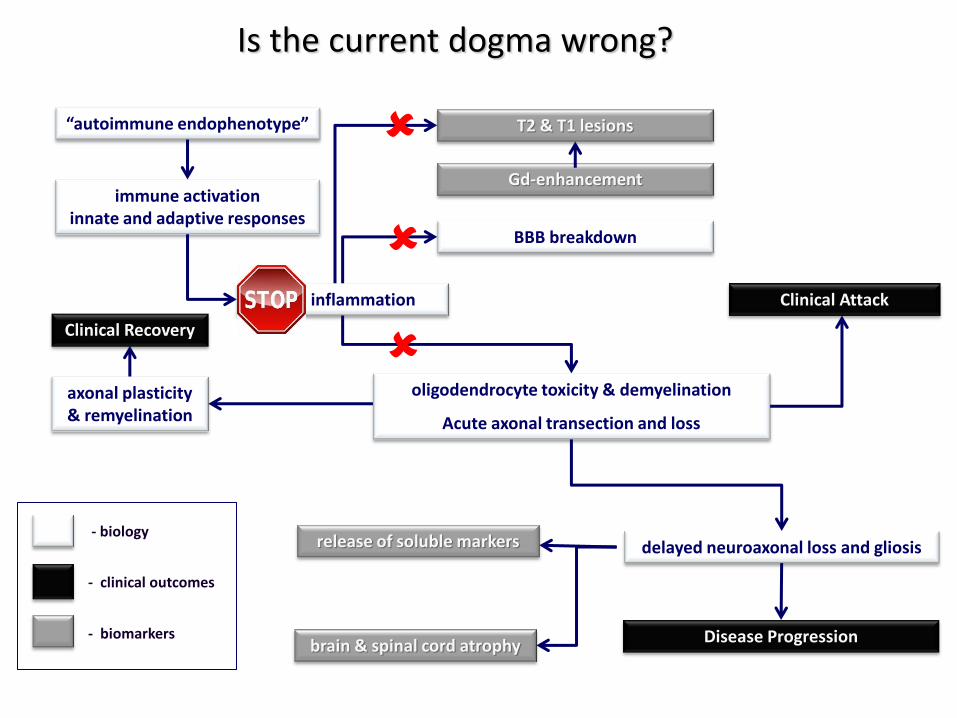
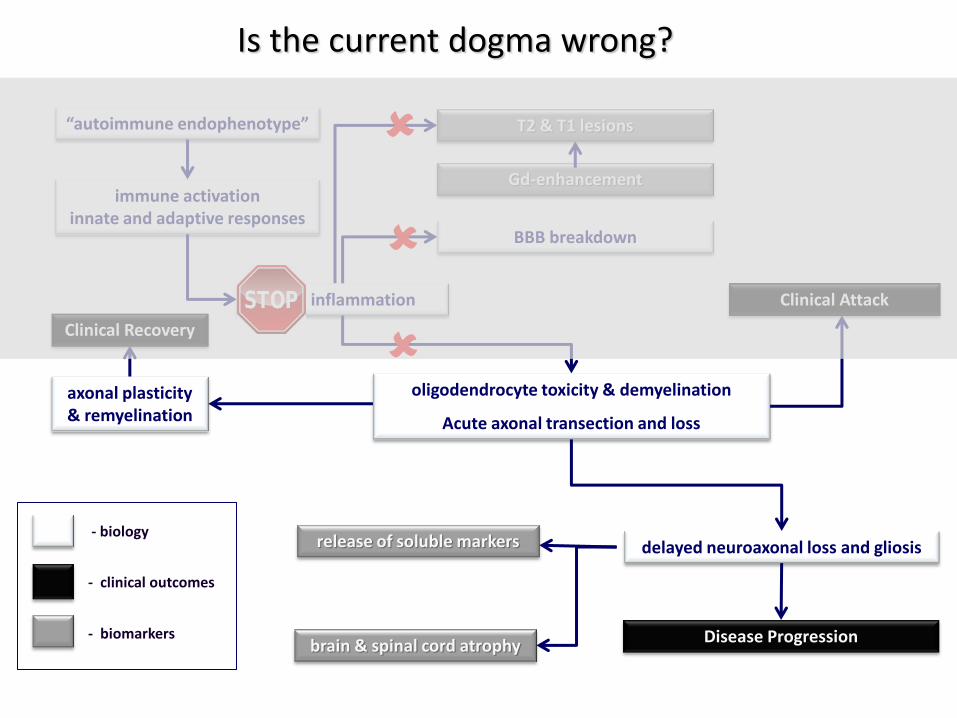
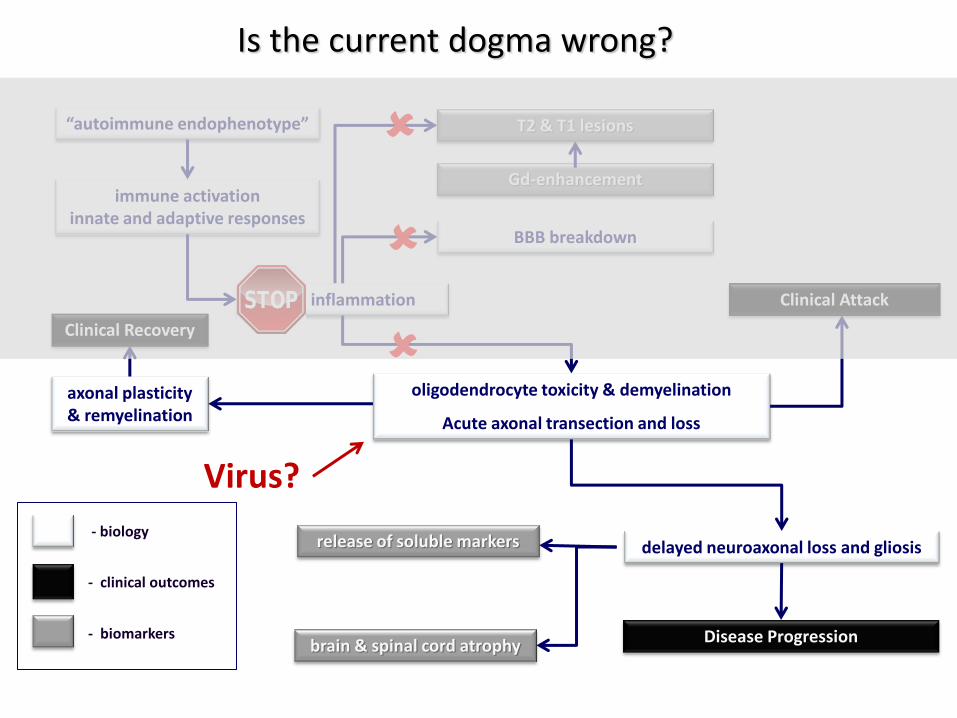
Is the current dogma wrong?
immune activation innate and adaptive responses
focal inflammation
BBB breakdown
oligodendrocyte toxicity & demyelination
Acute axonal transection and loss
“autoimmune endophenotype”
axonal plasticity & remyelination
delayed neuroaxonal loss and gliosis
Gd-enhancement
T2 & T1 lesions
brain & spinal cord atrophy
release of soluble markers
Clinical Attack
Disease Progression
Clinical Recovery
- biology
- clinical outcomes
- biomarkers
Is the current dogma wrong?
immune activation innate and adaptive responses
focal inflammation
BBB breakdown
oligodendrocyte toxicity & demyelination
Acute axonal transection and loss
“autoimmune endophenotype”
axonal plasticity & remyelination
delayed neuroaxonal loss and gliosis
Gd-enhancement
T2 & T1 lesions
brain & spinal cord atrophy
release of soluble markers
Clinical Attack
Disease Progression
Clinical Recovery
- biology
- clinical outcomes
- biomarkers
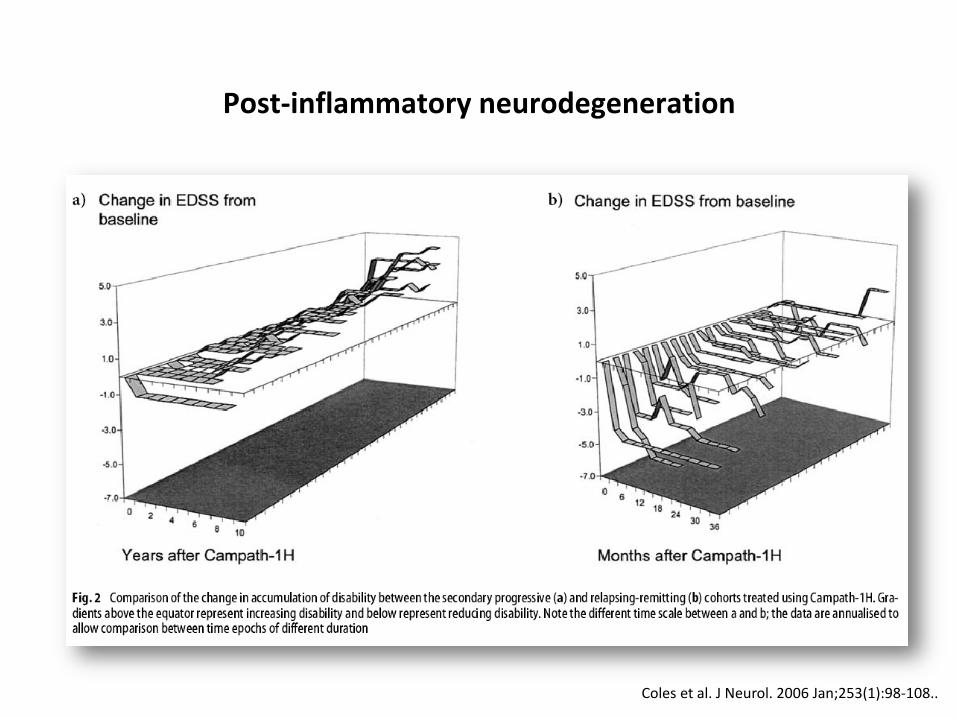
Coles et al. J Neurol. 2006 Jan;253(1):98-108..
Post-inflammatory neurodegeneration
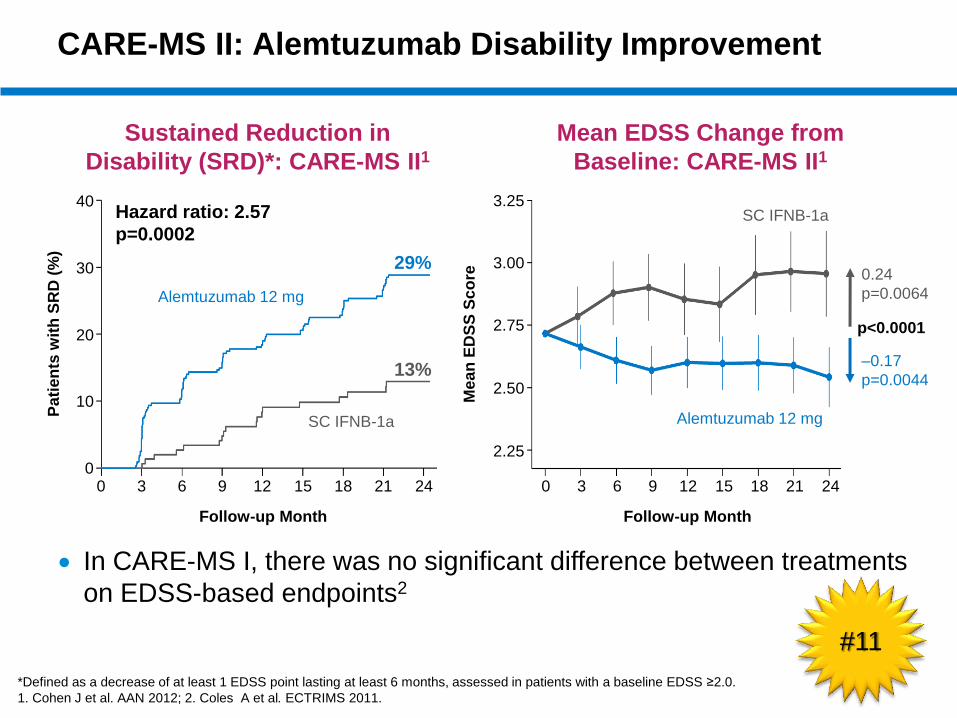
CARE-MS II: Alemtuzumab Disability Improvement
*Defined as a decrease of at least 1 EDSS point lasting at least 6 months, assessed in patients with a baseline EDSS ≥2.0.
1. Cohen J et al. AAN 2012; 2. Coles A et al. ECTRIMS 2011.
Sustained Reduction in
Disability (SRD)*: CARE-MS II1
Mean EDSS Change from
Baseline: CARE-MS II1
Pa
tien
ts w
ith
SR
D (
%)
40
30
20
10
0 0 3 6 9 12 15 18 21 24
Follow-up Month
Hazard ratio: 2.57
p=0.0002
29%
13% ‒0.17
p=0.0044
p<0.0001
0.24
p=0.0064
Me
an
ED
SS
Sc
ore
3.25
3.00
2.75
2.50
2.25
Follow-up Month
Alemtuzumab 12 mg
SC IFNB-1a
0 3 6 9 12 15 18 21 24
SC IFNB-1a
Alemtuzumab 12 mg
In CARE-MS I, there was no significant difference between treatments
on EDSS-based endpoints2
#11
Is the current dogma wrong?
immune activation innate and adaptive responses
focal inflammation
BBB breakdown
oligodendrocyte toxicity & demyelination
Acute axonal transection and loss
“autoimmune endophenotype”
axonal plasticity & remyelination
delayed neuroaxonal loss and gliosis
Gd-enhancement
T2 & T1 lesions
brain & spinal cord atrophy
release of soluble markers
Clinical Attack
Disease Progression
Clinical Recovery
- biology
- clinical outcomes
- biomarkers
Virus?
Epstein Bar Virus
Genetics
Vitamin D
Smoking
Risks
Adverse events
Differential Diagnosis
MRI
Evoked Potentials
Lumbar puncture
Blood Tests
Diagnostic Criteria
Cognition
Depression
Fatigue
Bladder
Bowel
Sexual dysfunction Tremor
Pain Swallowing
Spasticity Falls
Balance problems Insomnia
Restless legs Fertility
Clinical trials
Gait
Pressure sores
Oscillopsia
Emotional lability
Seizures
Gastrostomy
Rehab
Suprapubic catheter
Intrathecal baclofern
Physio- therapy
Speech therapy
Occupational Therapy
Functional neurosurgery
Colostomy
Tendonotomy
Studying
Employment Relationships
Travel
Vaccination
Anxiety
Driving
Nurse specialists
Counselling
Family counselling
Relapses
1st line
2nd line
Maintenance Escalation Induction
Monitoring
Disease-free
Disease progression
DMTs
Side Effects
Advanced Directive
Exercise
Diet
Alternative Medicine
Pregnancy Breast Feeding
Research
Insurance
Vision
Palliative Care
Assisted suicide
Social services
Legal aid Family counselling
Prevention
Diagnosis
DMT Symptomatic
Therapist
Terminal
Counselling
Epstein Bar Virus
Genetics
Vitamin D
Smoking
Risks
Adverse events
Differential Diagnosis
MRI
Evoked Potentials
Lumbar puncture
Blood Tests
Diagnostic Criteria
Cognition
Depression
Fatigue
Bladder
Bowel
Sexual dysfunction Tremor
Pain Swallowing
Spasticity Falls
Balance problems Insomnia
Restless legs Fertility
Clinical trials
Gait
Pressure sores
Oscillopsia
Emotional lability
Seizures
Gastrostomy
Rehab
Suprapubic catheter
Intrathecal baclofern
Physio- therapy
Speech therapy
Occupational Therapy
Functional neurosurgery
Colostomy
Tendonotomy
Studying
Employment Relationships
Travel
Vaccination
Anxiety
Driving
Nurse specialists
Counselling
Family counselling
Relapses
1st line
2nd line
Maintenance Escalation Induction
Monitoring
Disease-free
Disease progression
DMTs
Side Effects
Advanced Directive
Exercise
Diet
Alternative Medicine
Pregnancy Breast Feeding
Research
Insurance
Vision
Palliative Care
Assisted suicide
Social services
Legal aid Family counselling
Prevention
Diagnosis
DMT Symptomatic
Therapist
Terminal
Counselling
#12
#13
Epstein Bar Virus
Genetics
Vitamin D
Smoking
Risks
Adverse events
Differential Diagnosis
MRI
Evoked Potentials
Lumbar puncture
Blood Tests
Diagnostic Criteria
Cognition
Depression
Fatigue
Bladder
Bowel
Sexual dysfunction Tremor
Pain Swallowing
Spasticity Falls
Balance problems Insomnia
Restless legs Fertility
Clinical trials
Gait
Pressure sores
Oscillopsia
Emotional lability
Seizures
Gastrostomy
Rehab
Suprapubic catheter
Intrathecal baclofern
Physio- therapy
Speech therapy
Occupational Therapy
Functional neurosurgery
Colostomy
Tendonotomy
Studying
Employment Relationships
Travel
Vaccination
Anxiety
Driving
Nurse specialists
Counselling
Family counselling
Relapses
1st line
2nd line
Maintenance Escalation Induction
Monitoring
Disease-free
Disease progression
DMTs
Side Effects
Advanced Directive
Exercise
Diet
Alternative Medicine
Pregnancy Breast Feeding
Research
Insurance
Vision
Palliative Care
Assisted suicide
Social services
Legal aid Family counselling
Prevention
Diagnosis
DMT Symptomatic
Therapist
Terminal
Counselling
Epstein Bar Virus
Genetics
Vitamin D
Smoking
Risks
Adverse events
Differential Diagnosis
MRI
Evoked Potentials
Lumbar puncture
Blood Tests
Diagnostic Criteria
Cognition
Depression
Fatigue
Bladder
Bowel
Sexual dysfunction Tremor
Pain Swallowing
Spasticity Falls
Balance problems Insomnia
Restless legs Fertility
Clinical trials
Gait
Pressure sores
Oscillopsia
Emotional lability
Seizures
Gastrostomy
Rehab
Suprapubic catheter
Intrathecal baclofern
Physio- therapy
Speech therapy
Occupational Therapy
Functional neurosurgery
Colostomy
Tendonotomy
Studying
Employment Relationships
Travel
Vaccination
Anxiety
Driving
Nurse specialists
Counselling
Family counselling
Relapses
1st line
2nd line
Maintenance Escalation Induction
Monitoring
Disease-free
Disease progression
DMTs
Side Effects
Advanced Directive
Exercise
Diet
Alternative Medicine
Pregnancy Breast Feeding
Research
Insurance
Vision
Palliative Care
Assisted suicide
Social services
Legal aid Family counselling
Prevention
Diagnosis
DMT Symptomatic
Therapist
Terminal
Counselling
Conclusions
• Has the emergence of monoclonal therapies cracked relapsing disease?
– How do we define a cure?
– Is DAF status the new treatment aim?
• Progressive MS remains a problem
– The challenge is doing affordable phase 2 & 3 trials
– Do we need new outcome measures (including CSF)?
• How does relapses and progression relate to each other?
– Are the Laquinimod and Daclizumab results trying to tell us something?
• Is the dogma wrong?
– Does MS need a paradigm shift?
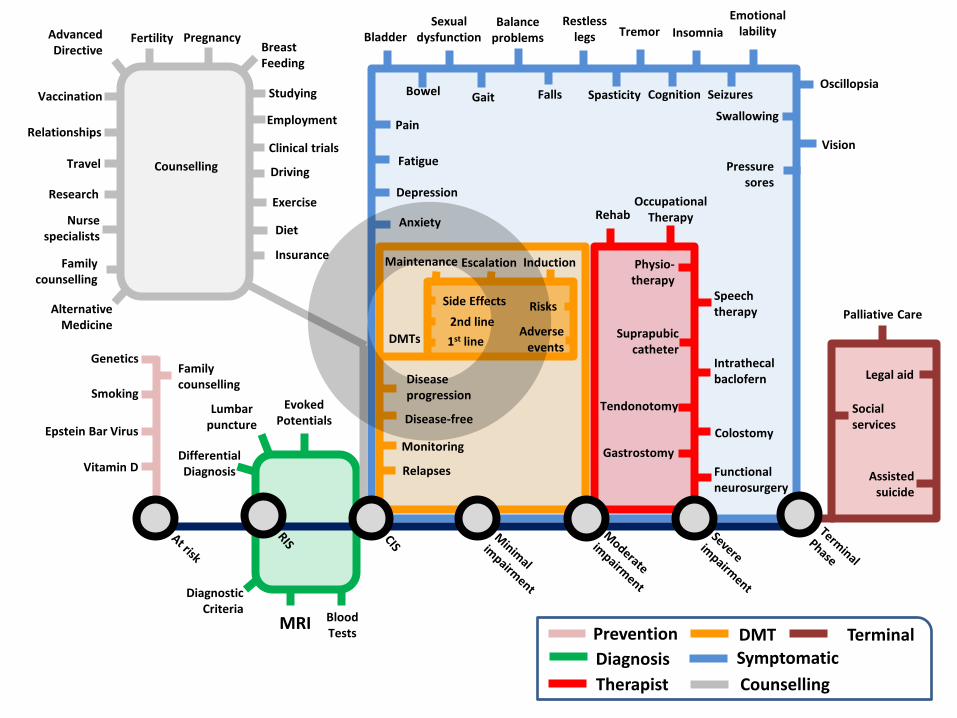
• We need an holistic approach to MS
– MS is a life-long disease with many problems that need to be solved

One-stop shopping for researchers in the field of MS
www.msdiscovery.org
• Reported news about research articles and conference presentations • A database of drugs in the pipeline • Discussion forums • Listings of tissue repositories, scientific meetings, and more • Classic paper summaries
MassGeneral Institute for Neurodegenerative Disease





























