Embed Size (px)
Citation preview

TOXICOLOGY Dr Gopisankar M G
Duties of a doctor in suspected poisoning is described under
S.39 CrPC S.175 CrPC
S.193 IPC S.176 IPC S.201 IPC S.202 IPC

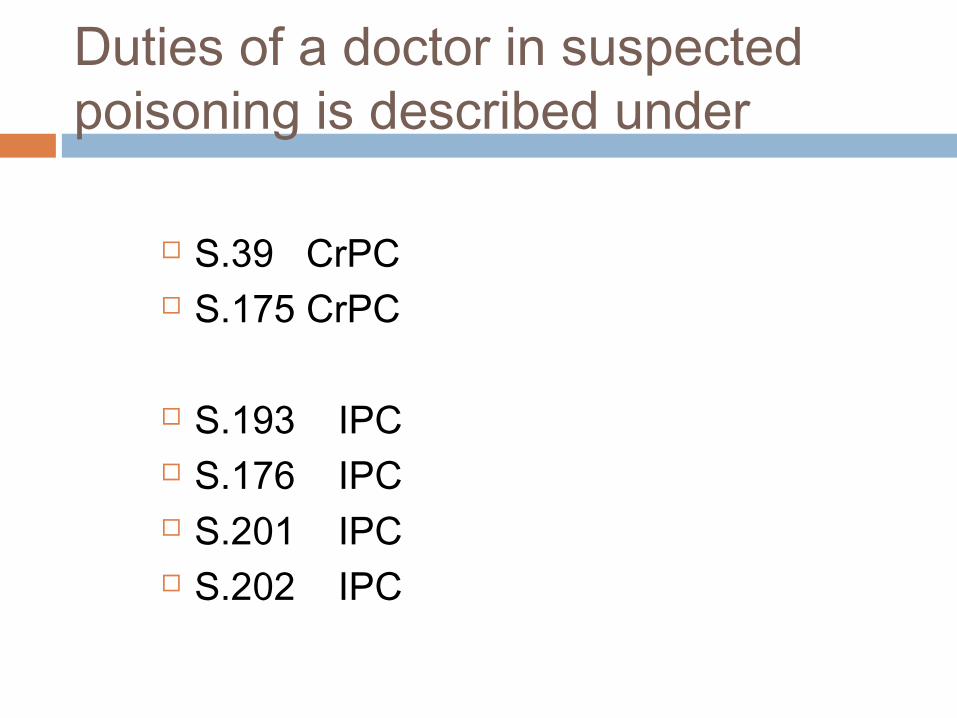
201 –(punishment IPC no. if not done)preserve articles , food, excreta , stomach wash , bottles , capsules , paper packets should be collected and preserved
39 – if a private practitioner is convinced that it is a homicidal poisoning he should inform police officer or magistrate

If 39 not done doctor is punishable under 176 If he is sure that it is suicidal poisoning no
need to inform police since 309 is not included in the section
But under 175 if asked by police officer Dr should give all information
If conceals liable to get punished under 202

False information – section 193 He will be punished

Gastric lavage Within 3 hrs For salycylates,phenothiazenes,antihistaminics,TCA, -- lavage
can be done upto 12 – 18 hours Ewald’s / Baos tube First 250 ml then 500 ml CI – corrosive poisoning except for phenol Complications – 1. Laryngeal spasm2. Aspiration pneumonitis3. Perforation of the stomach4. Sinus Bradycardia

Ipecan cuan ha-emetic

Antidotes
Mechanical /Physical-1. Activated charcoal,2. Demulscents –milk,starch,egg white3. Bulky food Chemical Physilogical / Pharmacological

Activated charcoal
Sedatives,antihistamines,antidepressents,antiepileptics ,etc well absorbed
NOT effective with 1. Corrosives2. Heavy metals3. Cyanide4. Hydrocarbons5. Alcohol
Dose of Activated charcoal
Adults – 60 – 100 gm Children 15 – 30 gm Repeat 50 g every 4 hours Upto 2 days

Chemical antidotesAgNo3 + Nacl Agcl
Albumin for Mercuric Perchloride

Fe for Arsenic

CuSO4 for Phosphorous

Potassium permanganate for cyanide poisoning

Ticnture of iodine for most of alkaloids

Universal antidote = activated charcoal + tannic acid + Magnesium Oxide

Physiological /pharmacological antidotes Exactly opp. Symptoms Chelating agents – 1. BAL –Bi,Ar,Lead,Mercury,Cu2. EDTA –Pb , Hg , Cu , Fe,cadmium ,Nickel3. Pencillamine – chelating agent of maximum
eficacy in heavy metals4. DMSA


some Abortificents
Ergot Calotropis, Cantherides, Oleander, Aconite, Semicarpus


Stupifying agents
Chloral hydrate Datura Cannabis


Delerium
Belladana- Datura

Organophosphate poisoning
Mixed in a solvent called Aromax – kerosine like smell in the body cavity,stomach contents , vomitus , froth, etc
Inactivation of Che becomes irriversible after 24 – 36 hrs
Sign & symptoms – when activity drops to 30% of normal activity
Death – paralysis of the respiratory muscles

Choline esterase test
5 ml of heparinised blood average normal values 77 – 142 in red cells 41 – 140 in plasma Diagnosis can be confirmed by giving 2 mg of
atropine in normal signs of atropinisation and in poisoned releives the symptoms

Choline esterase estimation

Dimethoate , methyl diazinon , Schraden , Phorate ..---- oximes not effective
Post Mortem appearance Signs of Asphyxia Congestion – face,all internal organs Cyanosis of lips,fingers , nose Blood stained froth--Respiratory path ,
mouth and nose Stomach content with smell of
kerosene Organophosphorous can be detected in
putrified bodies

Oxims
DAM – Di Acetyl Monoxime Praldioxime Iodide Pralidoxime chloride

Endrin –Plant penicillin

Zinc Phosphide
Fatal dose 5g Fatal period 24
hrs

Aluminium Phosphide
Release phosphine
MOA – inhibition of cytochrome oxidase
Fatal dose -1-3 tab
Fatal period – 1 hour to 4 days

Sulphuric acid Poisoning

Treatment of Sulphuric acid poisoning
Avoid gastric lavage 250 ml of water / milk / milk of magnesia /
lime water – within 30min Demulcents Prednisolone 60 mg / day - to prevent
esophageal stricture and shock If stricture develops – 4cm diameter Hg filled
bougie should be passed daily Give nothing by mouth Topica l paste of Magnesium oxide / sodium
bicarbonate


PM change
Stomach – soft , spongy , black mass , when readily disintegrates when touched

Treatment of vitriolage
Wash with plenty of water Soap of Sodium or Potassium carbonate Thick paste of magnesium oxide / carbonate
is applied Eyes – irrigated with Dilute Sodium
bicarbonate solution Later a few drops of olive oil or castor oil is
applied to the eyes
Nitric acid

Sign and symptoms
Greater abdominal distension due to gas formation
Tissues are stained yellow In esophagu and stomach …the corrosion of
the mucus membrane may not be associated with yellow colour –Brown or Brown black due to acid hemetin

HCl
Corrosion is less severe Stomach contains brownish fluid The folds of the whole stomach mucosa are
brownish Perforation is rare Acute inflammation and edema of the
respiratory passage are common

Oxalic acid
10% Rarely damage the skin Corrodes mucus membrane Vomitus – coffee ground appearance- altered
blood and mucus Hypocalcemia

Treatment of Oxalic Acid poisoning
Stomach wash – Calcium lactate or gluconate Antidote – preparation of Calcium Lime water , Calcium gluconate ,Calcium
chloride Parathyroid extracts bowel may be evacuated
by enema or castor oil

Carbolic acid
Carboluria – further oxidation of hydroquinone and pyrocatechol in the urine cause green colouration
Chronic Poisoning – Phenolic Marasmus-Anorexia , headache ,wt loss ,headache ,darkurine , and oochronosis
Oochronosis – pigmentation of skin and sclera

Post Mortem findings in carbolic acid poisoning i) Esophagus - Mucosa is tough, corrugated,
arranged in longitudinal folds.
ii) Stomach - Mucosal folds are swollen covered by opaque,
coagulated mucous membrane which is thickened and leathery. Partial separation of necrotic mucosa.
iii) Duodenum, - Similar to stomach upper SI iv) Liver, Spleen - Whitish, hardened patch where
stomach has been in contact.
v) Kidneys - Haemorrhagic nephritis vi) Brain - Congested, edematous vii) Blood - Dark, semifluid, only partially coagulated.

Formic acid
Action – corrosive actioo on GI mucosa Causes hemolysis leading to acute renal
failure ATP synthesis is diminished T/T –Milk –Folinic acid 1mg /Kg 4th hourly

Arsenic Poisoning


Metallic arsenic is not poisonous as it is not absorbed from the alimentary canal
Arsenic trioxide / white Arsenic
MOA – binds and inhibits Pyruvate oxidase which is a mitochondrial enz
Affects vascular endothelium – increased permiabilityesp in the intestinal canal
Irritation of the mucucs membrane Depression of the NS Interfers with glycolysis

Signs & symptoms
1. Fulminant type 2. Gatro enteric type3. Narcotic

Fulminent tyoe
Massive doses – 3 -5 gm Arsenic death in 1 – 3hrs – due to shock & peripheral vascular failure

Gastro enteric type Common form of acute poisoning Mostly half an hour after ingestion Sweetish metallic taste Constriction of the throat and difficulty in
swallowing Burning and colicky pain in the esophagus,
stomach and bowel Purging Stools – frequently and involuntary first
Dark coloured stinking and bloody resembles rice water stools
Garlicky odour in breath and feces may be noted
Death is usually due to circulatory failure

Narcotic Form
Giddiness Formication and tenderness of the muscle Delerium coma and death Arseniurated hydrogen direct poison to Hb
hemolysis ,hemoglobinuria , renal failure Death is almost instantaneous

Treatment of Arsenic Poisoning
Emetics should not be used Alkalis should not be used Wash with large amount of warm water /
milk Ferric oxide BAL DMPS DMSA Penicillamine Demulscents Glucose saline with Sodium bicarbonate Hemodyalisis and exchange transfusion

PM appearance – acute

PM appearance- chronic

Mercury
Mercuric Egg white Ca – EDTA should not be used as it is
nephrotoxic with mercury PM – if the patient survives forfew days
..LI shows necrosis due to the reexcretion of mercury into the large bowel

Chronic poisoning – Hydrargyrism
PRESENCE OF TISSUE DEPOSITS OF Cu -CHALCOSIS




INORGANIC POISONING
Phosphorus

Preservation for viscera in case of suspected poisoning Stomach and its contents Upper part of small intestine and its contents
30 m Liver 200 300 g Kidney – half of each Blood 30 ml Urine 30 ml

Preservatives
Saturated sodium chloride- all except Corrosives
Rectified spirit KF