Embed Size (px)
Citation preview
Thyroid storm Thyrotoxic crisis
Mansoura faculty of medicine
Clinical pharmacology department
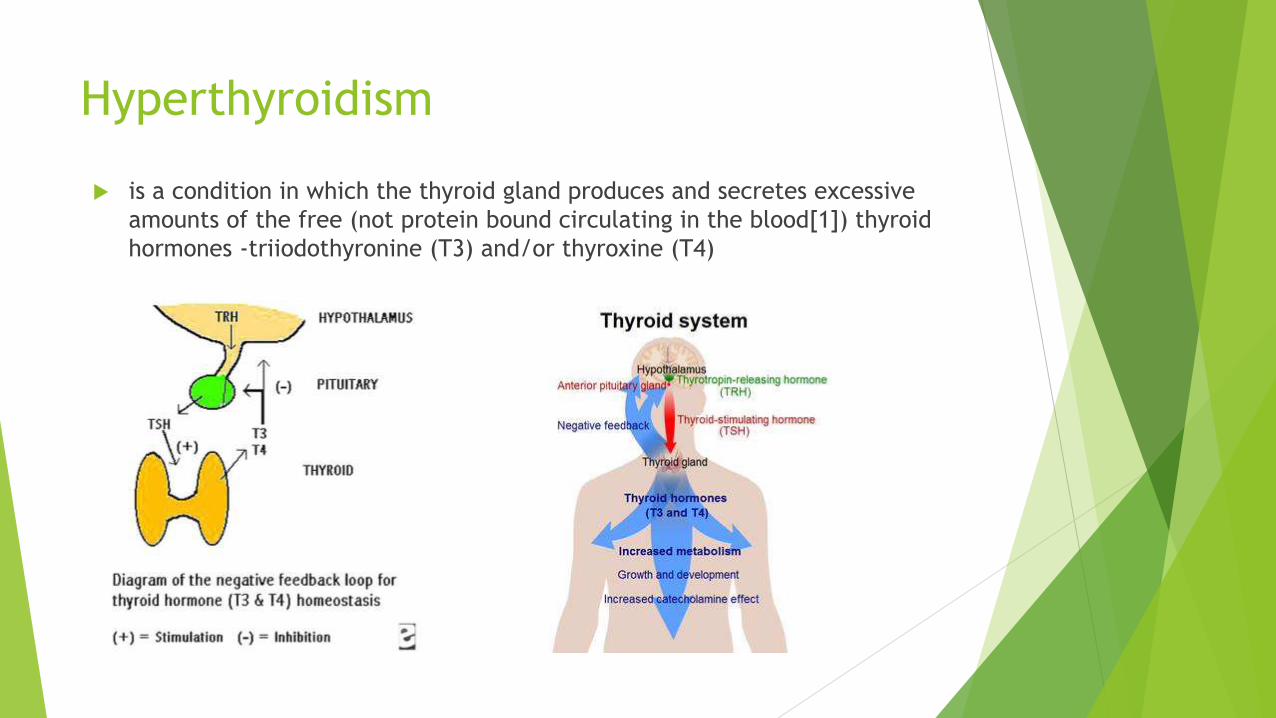
Hyperthyroidism
is a condition in which the thyroid gland produces and secretes excessive
amounts of the free (not protein bound circulating in the blood[1]) thyroid
hormones -triiodothyronine (T3) and/or thyroxine (T4)
causes Graves’ disease
Viral infection-------------------lead to sub acute thyroiditis (de quervain )
Neoplasms –like functioning thyroid adenomas autonomously functioning toxic nodules and toxic, multi nodular goiters (TMNGs)
from taking too much thyroid medication. In these cases the thyroid gland itself is not overactive, but there is still too much thyroid hormone in the blood. Untreated, thyrotoxicosis can lead to serious medical complications such as heart rhythm disturbances and Osteoporosis, caused from the long-term effects of hormone overproduction.
Another condition, called subclinical hyperthyroidism, may be diagnosed when you have low levels of thyroid stimulating hormone (TSH) but normal levels of thyroid hormone. Your doctor may treat asymptomatic (without symptoms) subclinical hyperthyroidism to avoid future symptoms.
Graves disease
the most common cause of
hyperthyroidism
It’s autoimmune disease in which
there are abnormal antibodies
(thyroid stimulating
immunoglobulins) activates TSH
receptors
The gland is enlarged and soft

Signs and Symptoms of hyperthyroidism
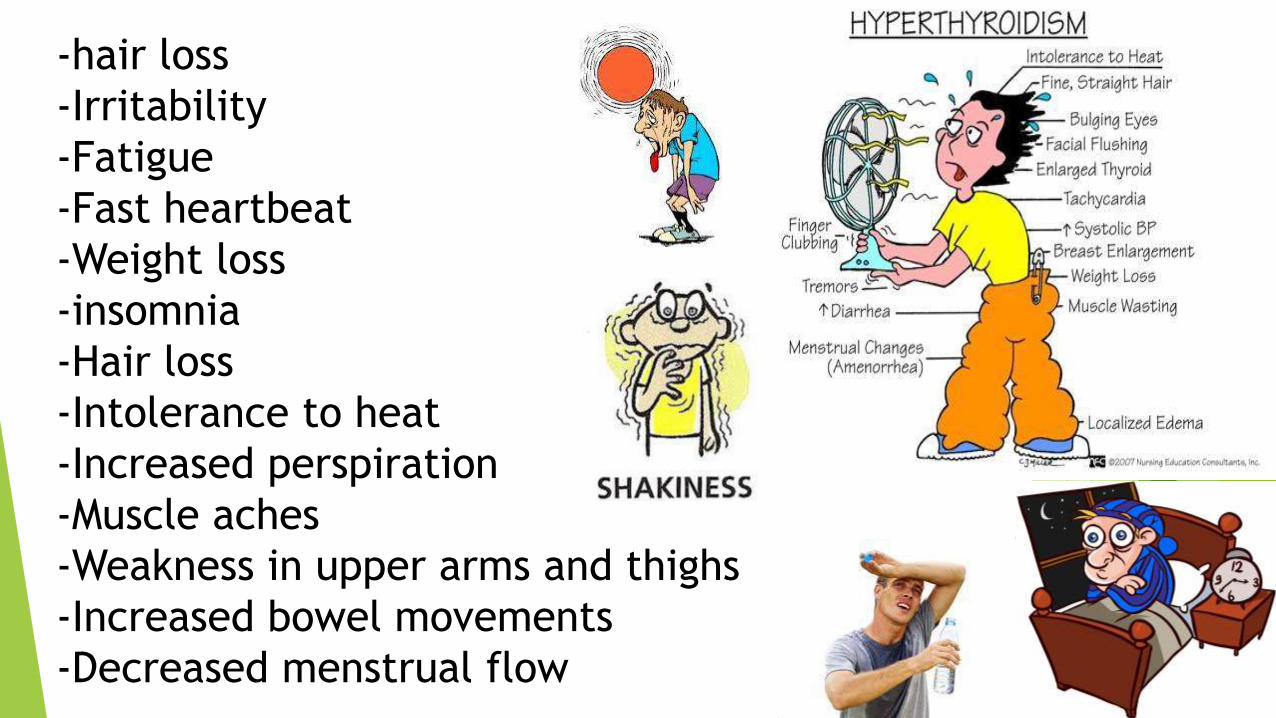
-hair loss
-Irritability
-Fatigue
-Fast heartbeat
-Weight loss
-insomnia
-Hair loss
-Intolerance to heat
-Increased perspiration
-Muscle aches
-Weakness in upper arms and thighs
-Increased bowel movements
-Decreased menstrual flow
Thyrotoxic crisis
Exaggerated or florid state of thyrotoxicosis"
"Life threatening, sudden onset of thyroid hyperactivity"
May represent end stage of a continuum :
– Thyroid hyperactivity to thyrotoxicosis to Thyrotoxic crisis to thyroid storm
"Probably reflects the addition of adrenergic hyperactivity, induced by a nonspecific stress, into the setting of untreated or undertreated hyperthyroidism"
Relation () hyperthyroidism and
thyrotoxicosis
Hyperthyroidism is a type of thyrotoxicosis in which accelerated thyroid
hormone biosynthesis and secretion by the thyroid gland produce
thyrotoxicosis. However, hyperthyroidism and thyrotoxicosis are not
synonymous This is because, although many patients have thyrotoxicosis
caused by hyperthyroidism, other patients may have thyrotoxicosis resulting
from inflammation of the thyroid gland, which causes the release of stored
thyroid hormone but not accelerated synthesis, or they may have
thyrotoxicosis, which is caused by ingestion of exogenous thyroid hormone.
Differentiating between thyrotoxicosis caused by hyperthyroidism and
thyrotoxicosis not caused by hyperthyroidism is important, because disease
management and therapy differ for each form.
Thyroid Storm
Background Etiology
Most cases secondary to Graves' disease
Some due to toxic multinodular goiter
Rare causes :
Acute thyroiditis
Factitious
Malignancies (most do not efficiently produce thyroid hormones)
Very rare in children
Manifestation
Patients may have a known history of thyrotoxicosis. In the absence of previously diagnosed thyrotoxicosis, the history may include symptoms such as irritability, agitation, emotional liability, a voracious appetite with poor weight gain, excessive sweating and heat intolerance, and poor school performance caused by decreased attention span.
General symptoms
GIT
Neurologic
Cardiac
General symptoms
Fever
Profuse sweating
Poor feeding and weight loss
Respiratory distress
Fatigue (more common in older adolescents)
GIT symptoms Neurological symptoms
Nausea and vomiting
Diarrhea
Abdominal pain
Jaundice[3]
Anxiety (more common in
older adolescents)
Altered behavior
Seizures, coma
Cardiac symptoms
Hypertension with wide pulse pressure
Hypotension in later stages with shock
Tachycardia disproportionate to fever
Signs of high-output heart failure
Cardiac arrhythmia (Supraventricular arrhythmias are
more common, [eg, atrial flutter and fibrillation], but
ventricular tachycardia may also occur.)
causes
Thyroid storm is precipitated by the following factors in individuals with thyrotoxicosis:
Sepsis
Surgery
Anesthesia induction[5]
Radioactive iodine (RAI) therapy[6]
Drugs (anticholinergic and adrenergic drugs such as pseudoephedrine; salicylates; nonsteroidal anti-inflammatory drugs [NSAIDs]; chemotherapy[7] ) and iodinated contrast agents[8]
Excessive thyroid hormone (TH) ingestion
Withdrawal of or noncompliance with antithyroid medications
Diabetic ketoacidosis
Direct trauma to the thyroid gland
Vigorous palpation of an enlarged thyroid
Toxemia of pregnancy and labor in older adolescents; molar pregnancy
Thyroid storm in children
Thyroid storm can occur in children with thyrotoxicosis due to any cause but
is most commonly associated with Graves disease. Other reported causes of
thyrotoxicosis associated with thyroid storm include the following:
Trans placental passage of maternal thyroid-stimulating immunoglobulins in
neonates
McCune-Albright syndrome with autonomous thyroid function[9]
Hyper functioning thyroid nodule
Hyper functioning multinodular goiter
Thyroid-stimulating hormone (TSH)–secreting tumor
With down syndrome and turner syndrome
Laboratory Studies
Thyroid storm diagnosis is based on clinical features, not on laboratory test
findings. If the patient's clinical picture is consistent with thyroid storm, do not
delay treatment pending laboratory confirmation of thyrotoxicosis.
Thyroid studies :Results of thyroid studies are usually consistent with
hyperthyroidism and are useful only if the patient has not been previously
diagnosed.
CBC count: CBC count reveals mild leukocytosis, with a shift to the left.
Liver function tests (LFTs): LFTs commonly reveal nonspecific abnormalities such
as elevated levels of alanine aminotransferase (ALT), aspartate aminotransferase
(AST),
ABG and urinalysis: Measurement of blood gas and electrolyte levels and
urinalysis testing may be performed to assess and monitor short-term
management.
Imaging Studies
The following imaging studies may be indicated:
Chest radiography: Chest radiography may reveal cardiac enlargement due to congestive
heart failure……Radiography may also reveal pulmonary edema caused by heart failure
and/or evidence of pulmonary infection.
CT scanning: Head CT scanning may be necessary to exclude other neurologic conditions if
diagnosis is uncertain after the initial stabilization of a patient who presents with altered
mental status.
ECG is useful in monitoring for cardiac arrhythmias. Atrial fibrillation is the most common
cardiac arrhythmia associated with thyroid storm. Other arrhythmias such as atrial flutter
and, less commonly, ventricular tachycardia may also occur.

Treatment
Medical Care
immediately provide supplemental oxygen, ventilatory support, and intravenous fluids. Dextrose solutions are the preferred intravenous fluids to cope with continuously high metabolic demand.
Aggressively control hyperthermia
antiadrenergic drugs (e.g., propranolol) to minimize sympathomimetic symptoms.
Administer antithyroid medications to block further synthesis of thyroid hormones (THs).
Administer iodine compounds (Lugol iodine or potassium iodide) orally or via a nasogastric tube to block the release of THs (at least 1 h after starting antithyroid drug therapy). If available, intravenous radiocontrast dyes such as ipodate and iopanoate can be effective in this regard. These agents are particularly effective at preventing peripheral conversion of T4 to T3.
Medical care
Administer glucocorticoids (hydrocortisone ) 50mg i.v /6h to decrease
peripheral conversion of T4 to T3. This may also be useful in preventing
relative adrenal insufficiency due to hyperthyroidism.
Treat the underlying condition, if any, that precipitated thyroid storm and
exclude comorbidities such as diabetic ketoacidosis and adrenal insufficiency.
Infection should be treated with antibiotics.
Rarely, as a life-saving measure, plasma pheresis has been used to treat thyroid
storm in adults.
Iodine preparations should be discontinued once the acute phase resolves and
the patient becomes afebrile with normalization of cardiac and neurological
status. Glucocorticoids should be weaned and stopped and the dose of
thioamides adjusted to maintain thyroid function in the normal range. Beta-
blockers may be discontinued once thyroid function normalizes.
Medical care
High-dose propylthiouracil (PTU) is preferred because of its early
onset of action and capacity to inhibit peripheral conversion of T4 to
T3. The US Food and Drug Administration (FDA) had added a boxed
warning, the strongest warning issued by the FDA, to the prescribing
information for PTU.
If the patient is given PTU during treatment of thyroid storm, this
should be switched to methimazole at the time of discharge unless
methimazole is contraindicated. If there is a contraindication for the
use of methimazole, alternative methods to treat hyperthyroidism
should be considered after discharge, such as radioactive iodine or
surgery
Surgical Care
Patients with Graves disease who need urgent treatment of hyperthyroidism
but have absolute contraindications to thioamides may be managed acutely
with beta-blockers, iodine preparations, and glucocorticoids as described.
Subsequently, thyroidectomy may be performed after about 7 days of iodine
administration. Iodine reduces the vascularity of the gland and the risk for
thyroid storm.