Embed Size (px)
Citation preview

Venous Thromboembolism in
Pregnancy
Farah Siddiqui
Consultant Fetal and Maternal Medicine
University Hospitals of Leicester

MBRRACE 2016
No statistically significant
decrease in the maternal
death rate in the UK
between 2009-11 and 2012-
14.
Unlikely to achieve the
Government aspiration of
reducing maternal deaths by
50% by 2030
200 women who died in 2012–14
135 women gave birth to:-
141 infants,
105 (74%) survived
The women who died left behind a further
253 children
A total of 358 motherless children remain.


Thrombosis and Thromboembolism
Mortality rates 1985-2008

VTE in pregnancy
Pulmonary emboli and DVT
~ 1/1000 pregnancies antenatally
~2/1000 pregnancies in puerperium

Pregnancy is a hypercoagulable state
• At term 500ml blood flows through the placental bed per minute
• Without effective and rapid haemostasis a woman would die from blood loss
• Myometrial contraction
• Then fibrin deposition of the placenta bed.

Clotting factors in pregnancy

Pregnancy Fulfils All of the
Virchows Triad• Stasis
– Compression of the iliac
veins
– Gravid uterus
– Vein dilatation
– Immobilization
• Vascular damage
– Vascular compression at
delivery
– Damage to vessels at
delivery c
section>>operative
vaginal birth
• Hypercoagulable
– More thrombus
generation
– Less clot dissolution

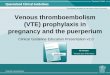
Distribution of VTE in pregnancy and
the puerperium
Jacobsen et al. A J Obstet Gynecol 2008; 18(2);233.e1

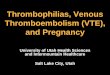
Absolute and relative rates of VTE by
risk factors
• Sultan AA et al Blood 2013;121(19):3953-61

The National Maternity Audit- RCOG
October 2017
The current pregnant population
• Smoking status – 14.1% were smoking in England
– 18% in Wales
• >50% pregnant women had a BMI>25
• 20% were obese with a BMI of 30 or over.
• 50% of births are to women aged 30
• 15% are aged 35 or over at booking in their first pregnancy.
• Caesarean section rates are increasing national average =20%


• 27 year old homeless lady booked in a Northern DGH
• History of binge drinking, smokes 20/day, learning
difficulties
• Mother died of unprovoked massive PE aged 35
• First pregnancy massive PPH, admitted to ITU, Left
pulmonary embolus 2 weeks later.
• 32 weeks attended A+E severe dyspnoea and chest
pain and leg swelling
• Polyhydramnios
Case study LB

Presentation


MBRRACE
• May present with dyspnoea without chest
symptoms
• Paroxysmal dyspnoea is abnormal
• Orthopnoea is abnormal
• All chest pain (necessitation attendance to
hospital) should be investigated
Importance of careful history:-
Prevalence of ultimately diagnosed PE in pregnant women with suspected
PE is 2-6%


Dilemma in Investigating VTE
• Clinical signs and symptoms of PE are nonspecific.– 82% present with dyspnoea
– 49% present with abrupt onset chest pain
– 20% present with cough
• Similarly DVT– Leg swelling is common
– Cramps are common
• Wells score in pregnancy– Clinicians should be aware that, at present, there is no evidence
to support the use of pretest probability assessment in the management of acute VTE in pregnancy. (RCOG)

DVT
US may miss below knee/ above
inguinal ligament
If us negative and high level of
suspicion of dvt
Continue anticoagulation and
repeat US in 5- 7 days

Dilemmas in Investigation VTE
D dimersD dimers- high negative predictive value out side of pregnancy• D dimers- high negative predictive value out side of pregnancy
• D dimer levels raise in pregnancy and takes 4- 6 weeks to normalize post delivery
• Numerous case reports emerging of VTE with normal D dimers
• Even low levels should be interpreted with caution in particularly in patients on thromboprophylaxis and with a history of symptoms >1-2 weeks

Dilemmas in Investigation- ECG
Physiological ECG changes during pregnancy:
• atrial and ventricular ectopics
• left shift in the QRS axis
• small Q wave and inverted T wave in lead III
• ST segment depression and T wave
inversion in the inferior and lateral leads.
Study of ECG in VTE found that the ECG was abnormal in 41% of women with acute
PE;
T wave inversion (21%),
S1 Q3 T3 pattern (15%)
right bundle branch block (18% antenatal; 4.2% post natal).
Blanco-Molina A, Rota LL, Di Micco P, Brenner B, TrujilloSantos J, Ruiz-Gamietea A, et al.; RIETE Investigators. Venous thromboembolism during
pregnancy, postpartum or during contraceptive use. Thromb Haemost 2010;103:306–11

Chest X ray• Chest X-ray (CXR) useful in excluding
– pneumonia, pneumothorax, lobar collapse.
• CXR is normal in >50% of pregnant patients with
objectively proven PE
• The radiation dose to the fetus from a CXR
performed at any stage of pregnancy is negligible
(less than 0.01 mSv).
• A CXR should be performed before deciding upon
further diagnostic tests ie ?VQ ?CTPA
Abnormal features on CXR caused by PE
Atelectasis,
Effusion,
Focal opacities,
Regional oligaemia
Pulmonary oedema.

Arterial Blood Gases
Limited diagnostic value both in pregnancy and in non pregnant
Respiratory alkalosis is common in both pregnancy and PE
One study showed that only 10% had an arterial po2 <60 and 2.9% had
oxygen saturations <90%
The presence of hypoxaemia and a normal c-xray should
raise the suspicion of PE in pregnancy

VQ scan or CTPA??
• A matched case–control study in the UK investigated 143 women with
antenatal PE;
– 91 (65%) had a V/Q scan, low dose perfusion scan (Q)
– 42 (30%) had CTPA performed,
– 22 (16%) had echocardiography and
– 16 (11%) were diagnosed by angiography.
– Forty women (28%) were diagnosed using a combination of
techniques.
� Negative predictive values (99% and 100% for CTPA and Q scans
respectively)
� No significant difference between the number of positive, nondiagnostic
and normal scans

CTPA vs V/Q scan
Higher rate of inconclusive scans in pregnancy with CTPA 37.5% and V/Q 4%
(Cahill et al 2008)
CTPA has potential advantages over V/Q
�CTPA is more readily available
� delivers a low radiation dose to the fetus
�and can identify other pathology including pneumonia (5–
7%), pulmonary oedema (2–6%) and rarely aortic dissection
Ventilation/perfusion (V/Q) scanning is a useful first imaging test for suspected
PE in pregnancy; however, in one study, 21% of scans were non-diagnostic,
which meant that further imaging was required (Bourjeily et al. 2010).

CTPA vs VQ scan-
Risk to Mother vs Risk to Fetus
Increased risk of fatal childhood cancer to the age of 15 following in utero
radiation exposure =0.006% per mGy (1 in 17000 per mGy)
The fetal radiation exposure associated with CTPA= 0.1 mGy
with V/Q = 0.5 mGy
Breast tissue is sensitive to radiation exposure in pregnancy due to hormonally
induced increased glandular activity (especially in young women)
10m Gy radiation (CTPA) to a woman’s breasts increases her lifetime risk of
developing breast cancer by 13.6% above her background risk
For a 25-year-old whose background risk of developing breast cancer in the
following 10 years is 0.1%, the extra risk from 10mGy of radiation increases the
risk by 13.6% of 0.1%, which is 0.0136% extra.
V/Q scan should be the first choice in young women esp if there is a family h/o
breast ca or has had a previous CTPA

Radiation dose of VQ scan and CTPA
FETAL AND MATERNAL RADIATION DOSES ASSOCIATED WITH DIAGNOSTIC TESTS FOR PULMONARY EMBOLISM
Diagnostic Test Fetal Dose (mGy) Maternal Dose (Whole Body Effective Dose in mSv)
CXR 0.002 0.1
V/Q 0.32 – 0.74 4–18
CTPA 0.03 – 0.66 1–25
Flight New York to London 0.5

Algorithm for management of vte in
pregnancy

• CXR normal
• VQ scan --There is no perfusion in the right lung.
Perfusion on the left appears unremarkable.
• CTPA --Bilateral PE with nearly complete occlusion of
the right main pulmonary artery and evidence of right
heart straining.
• USS Leg--There is thrombus in the anterior tibial vein.
• Commenced therapeutic LMWH
• Transferred to glenfield
?thrombectomy, ?thrombolysis ?IVC filter
LB

Treatment• Heparin- does not cross the placental
barrier
• Warfarin- embryopathy in the first
trimester (6-12wks)-affects calcium
deposition in bone- facial and limb
defects; later fetal bleeding
• Oral direct thrombin and Factor Xa
inhibitors
• (e.g. dabigatran, rivaroxaban,
apixaban, edoxaban)
Pregnant women were excluded from clinical trials.
These agents are likely to cross the placenta. Fondaparinux
appears to cross the placenta in small quantities. Case reports
of the successful use of fondaparinux in pregnancy but only in
late second trimester or later exposure.

Massive life threatening PE
- with haemodynamic compromise• Thrombolytic therapy should be considered as anticoagulant therapy alone will not
reduce the obstruction in the circulation.
• Start infusion of unfractionated heparin can be given
• A meta-analysis of randomised controlled trials using thrombolytic agents for PE is
better in reducing clot burden and improving haemodynamics.
• Complications:
– Maternal bleeding complications (2.9%)
– Fetal deaths (1.7%).
– Exclude labour
• If the patient is not suitable for thrombolysis or is moribund, a discussion with the
cardiothoracic surgeons consider urgent thoracotomy

Clinically suspected DVT or PE,
treatment
• Low-molecular-weight heparin (LMWH)
• Dose calculated on booking weight, single dose or 2 divided doses
• Anti Xa levels if residual symptoms or high BMI
• For the remainder of the pregnancy and 6wks postnatally
• LMWH are safer than unfractionated heparin– Less bleeding complications, lower recurrence rates
– Risk of PPH-• the observed rate of massive postpartum haemorrhage (more than
1500 ml) was 1.1%, which compares favourably with the rate of massive haemorrhage (0.7%) from one prospective study without the use of LMWH

Management of labour
• When VTE occurs at term, consideration should be given to the use of
intravenous unfractionated heparin which is more easily manipulated.
• LMWH for maintenance therapy omit dose if signs of labour.
• Regional anesthetic or analgesic techniques should not be undertaken
until at least 24 hours after the last dose of therapeutic LMWH.
• LMWH should not be given for 4 hours after the use of spinal anesthesia
or after the epidural catheter has been removed, and the epidural
catheter should not be removed within 12 hours of the most recent
injection
• Active management of third stage

Inferior vena cava filters Indications for temporary IVC filter in the peripartum period
• for patients with iliac vein VTE to reduce the risk of PE
• Proven DVT and who have recurrent PE despite adequate anticoagulation.
• recurrent thromboembolism occurs despite adequate anticoagulation,
• when anticoagulation is contraindicated (such as the peripartumperiod).
• Case reports and case series have reported favourable outcomes with regard to safety and effectiveness on the use of IVC filters in pregnancy.
• The long-term safety of IVC filters is uncertain
• Complications associated with vena cava filters are – migration, an increased risk of lower limb DVT and caval thrombosis
infection.

LB
• Increasingly difficult to ventilate due to polyhydramnios.
• Caesarean Section at 33 weeks in Glenfield.
• Postnatally commenced on Apixaben before discharge.
Thrombophilia screen positive- antithrombin III deficiency.



In women who have additional persistent (lasting more than 7 days postpartum)
risk factors, such as prolonged admission or wound infection, thromboprophylaxis
should be extended for up to 6 weeks or until the additional risk factors are no
longer present

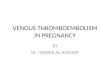
Venous Thromboprophylaxis
Greentop guideline no 37a
Risk scoring

SUMMARY
• VTE is the highest cause of direct deaths
• Think thromboprophylaxis- start early continue
into puerperium
• In suspected VTE- Diagnosis challenging
• Good history taking and consideration of imaging.
• Treatment dose dependant on booking weight
• In proven VTE refer to Haem Obs clnic,
multidisciplinary team approach

Thankyou