Embed Size (px)
Citation preview

The Epidemic of Type 2 Diabetes During Childhood
Francine Ratner Kaufman, M.D.Professor of PediatricsThe Keck School of Medicine of USCHead, Center for Diabetes and EndocrinologyChildrens Hospital Los Angeles

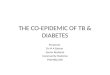
Natural History of Type 2 Diabetes
GeneticsusceptibilityEnvironmentalfactors
NutritionObesityPhysical inactivity
Hyperinsulinemia HDL-C TriglyceridesAtherosclerosisHypertension
AtherosclerosisHyperglycemiaHypertension
RetinopathyNephropathyNeuropathy
BlindnessRenal failureCHDAmputation
Onset ofdiabetes Complications
Disability
DeathOngoing hyperglycemiaIGTInsulin resistance

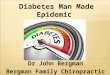
New-onset NIDDM diagnosed among youth ages 8-21 years at Arkansas Children’s Hospital
21
3
1
67
13
17
0
2
4
6
8
10
12
14
16
18
1988 1989 1990 1991 1992 1993 1994 1995
Year of Diagnosis
Num
ber
of P
atie
nts
Scott et al. Pediatr. 1997

Characteristics - Case Series of 578 Patients at Diagnosis with Type 2
Fagot-Camgagna et al J Pediatr 2000
• Mean Age 12-14 years
• Girls > Boys 1.7:1
• Obese BMI >85th %
• Minority Groups 94%
• Strong Family History 74-100%
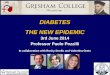
• Acanthosis Nigricans 56-92%

Characteristics Case Series of 578 Patients at Diagnosis
• Diagnosis made by Symptoms, not Screening• HbA1c 10-13%• Weight loss 19-62%• Glucose in urine 95%• Ketosis 16-79% • DKA 5-10%• Absence of Islet Autoimmunity >85-95%• Preservation of C-peptide >0.8-1nmol/l
Campagna et al J Pediatr 2000

Acanthosis Nigricans

TREATMENT OF
TYPE 2 DIABETES IN
CHILDREN AND TEENS

Treatment Protocols Multidisciplinary Team
• Set Glycemic Targets
• Diabetes Education – Patient and Family
• Role of Intensive Lifestyle
• Pharmacotherapy
• Regimens Advocated– What are the outcome measures to
assess efficacy, effectiveness

TREATMENT GOALS
• Glucose control, HbA1c <7%– Eliminate symptoms of hyperglycemia – Reduce microvascular complications
• Maintenance of reasonable body weight
• Improve cardiovascular risk factors
• Improvement in physical and emotional well-being

Glycemic Targets*
ParameterParameter NormalNormal GoalGoal Action SuggestedAction Suggested
Fasting (or Fasting (or Preprandial) Preprandial)
GlucoseGlucose<100<100 < 120< 120 <80 or >140<80 or >140
PostprandialPostprandialGlucoseGlucose
<140<140 <180<180 >180>180
Bedtime GlucoseBedtime Glucose <120<120 90 to 15090 to 150 <90 or >160<90 or >160
HbAHbA1c1c(DCCT Method)(DCCT Method) <6%<6% <7%<7% >8%>8%
Glucose values are plasma (mg/mL).Glucose values are plasma (mg/mL).
*Combined WHO recommendations and ADA guidelines.DCCT=Diabetes Control and Complications Trial.

ROLE OF FAMILY IN MANAGEMENT
• African-American Family Study• Group 1, direct family supervision• Group 2, no direct supervision• Group 1 ending HbA1c = 7.1+ 0.8%• Group 2 ending HbA1c = 12.3 + 0.6%• P=<0.0005
Bradshaw, J Pediatr Endocrinol Meta 15, 2002

Intensive Lifestyle Rationale
• Lifestyle and environment are risk factors • Consensus - modifying lifestyle primary goal• Might lead to remission
BUT• Mixed results in adult studies
– More or less effective in kids?
• Labor intensive and expensive – Do they work in the “real world” and school ?

HbA1c Statistics for CHLA 2002Type 2:
n Average ± SD
All patients 100 8.0 ± 2.3
Males 44 8.3 ± 2.2
Females 56 7.8 ± 2.3
Age < 5 years 0
Age 5-10 years 3 6.0 ± 0.9
Age 11-16 years 71 8.0 ± 2.2
Age >16 years 26 8.3 ± 2.5


Mechanisms To Lower Glucose Stimulate
insulin secretion
muscle glucose uptake
Correct insulin
deficiency
glucose production
Retard carbohydrate
absorption
Insulin or insulin analogues X
Sulfonylureas X
Thiazolidinediones X X
Biguanides X X
Repaglanide X
Alpha-glucosidase inhibitors X

TYPE 2 DIABETES . . . A PROGRESSIVE DISEASE
Progressive Decline of -Cell Function in the UKPDS
0
20
40
60
80
100
10 9 8 7 6 5 4 3 2 1 0 1 2 3 4 5 6Years
-C
ell F
un
cti
on
(%
)
Adapted from UK Prospective Diabetes Study (UKPDS) Group. Diabetes. 1995; 44:1249-1258.
6-4

Treatment of Type 2 DM in Children
diet/exercisemonthly review x 3 mo
HbA1c <7%
FPG <120 mg/dl
continue
HbA1c>7%, FPG>120
metforminHbA1c>7% FPG>120
add sulfonylurea? TZD?
add insulin

DiagnosisDiagnosisAsymptomatic
Start with insulin and diet, exercise
Diet and exercise
Monthly review, A1c q 3 m
>7%>7%
Add metformin
Attempt toWean insulin
Add sulfonylureaSilverstein, RosenbloomJ Pediatr Endcrinol Metab, 13,2000
BG 250 mg/dlBG 250 mg/dl
Add Insulin
<7%<7%
>7%>7%
>7%>7%

SStudies to tudies to TTreat reat OOr r PPrevent revent PPediatric ediatric TType ype 22
DDiabetesiabetes((STOPP-T2DSTOPP-T2D))
The TODAY TrialThe TODAY Trial

STOPP-T2 TREATMENTPRIMARY AIM
To compare the efficacy of 3 treatment regimens– Metformin– Metformin + lifestyle– Metformin + TZD
On Time to Treatment Failure and on Glycemic Control

Outcome Measures• Glycemic Controls
• Insulin Sensitivity and Secretion
• Body Composition
• Fitness and Physical Activity
• Nutrition
• Microvascular complications
• CVD Risk
• Quality of Life
• Cost

How Do We Differentiate
Type 1 Diabetes from Type 2 Diabetes

Differentiation Between Type 1 and 2
• 48 with type 2 vs 39 with type 1
• Type 2
– Ethnicity, 1st degree relative, BMI>24, +C-peptide, acanthosis
Type 2 Type 1
DKA 33% 53%
C-peptide 2.2+2.2 ug/l 1.8+3.5 ug/l
Abs 8.1% ICA
30% GAD 35%IAA
Hathout et al Pediatrics 107e102,June,2001

Barriers to Accurate Classification
• 20-25% newly diagnosed TIDM obese
• > 15% of minority populations have FH T2DM baseline
• 3X increase FH of T2DM in patients with T1DM
• Overlap C-P measurements at onset & first year or so
• > 30% T2DM with ketosis at onset

CO-MORBIDITIES

ComorbiditiesPercent of Patients >8 years with
BP >97th PercentileType 1 Type 2
Systolic 3.4% 20.1%
Diastolic 1% 6%

Outcomes in First Nation Youth in Canada
Dean, et al, Diabetes, 2002
Young adults, 18-33 years of age, Diagnosed before age 17 years
Due to poor glycemic control 9% mortality rate 6.3% dialysis rate38% pregnancy loss
During 10-15 year observation period

100 PIMA CHILDREN & ADOLESCENTS
AT DIAGNOSIS
7% high cholesterol (>200 mg/dL)
18% hypertension (BP>140/90)
22% microalbuminuria (alb/Cr >30)
AFTER TEN YEARS [mean HbA1c 12%]
60% microalbuminuria
17% macroalbuminuria (alb/Cr >300)

Screening
Of Children and Youth for
Type 2 Diabetes
and Prediabetes

Who Should be Tested for Type 2- Case Finding
ADA/AAP RecommendationsDiabetes Care 23:2000
• Age > 10 years or onset of puberty• BMI > 85th%• First or Second Degree Relative• Race/Ethnic Group• Signs of Insulin Resistance –
– Acanthosis nigricans– Hypertension– PCOS– Dyslipidemia

Tests To Diagnose Diabetes
• FPG – Preferred • 2-h OGTT - Preferred• 2-h Postprandial or random post meal• HbA1c
• In context of health visit• Every 2 years

ADA/NIDDK Screening Recommendations For Prediabetes in
AdultsDiabetes Care, 25:2002
• Case Finding
• Test: – >45 years, BMI > 25 kg/m2 – <45 years with + FH, GDM, baby > 9 lbs,
dyslipidemia, hypertension, non-Caucasian – At 3 yr intervals, if negative

ADA/NIDDK Recommendations In Adults
Diabetes Care, 25:2002
• How to Test: – In context of health care visit
– FPG, 2-h OGTT
• Intervention: – Prediabetes counsel for weight loss and PA, Follow-
up counseling
– Monitor for DM q 1-2 years, CVD risk factors
– Avoid drug therapy

PreventionREDUCTION
In Obesity
Pharmacotherapyvs
Lifestyle

Agents that can be Used for Obesity
Agents that can be used for Obesity• Sibutramine
– Blocks central reuptake of norepinephrine, serotonin
– Suppresses appetite
– Increases energy expenditure
• Orlistat
– Inhibits pancreatic lipase
– Increases fecal fat loss

Prevention with Metformin
• Six month study in 29 obese, hyperinsulinemic adolescents, positive family history
• Randomized, double-blinded, placebo-controlled
• Freemark, Bursey, SPR, Boston, 2000. Freemark, Bursey Pediatrics 107:2001

Prevention with MetforminMetformin Placebo
P value
BMI 1.3% <0.05 2.3%
FPG 84.8 to
74.8
77.2 to
82.6
Fasting Insulin
31.3 to
19.3
<0.02 No change
No change
Insulin sensitivity
HbA1c
Lipids
Glucose Disposal

The Diabetes Prevention Program
A Randomized Clinical Trial to Prevent Type 2 Diabetes
in Persons at High Risk
The DPP Research Group

0 1 2 3 4
0
10
20
30
40Placebo (n=1082)Metformin (n=1073, p<0.001 vs. Plac)Lifestyle (n=1079, p<0.001 vs. Met , p<0.001 vs. Plac )
Percent developing diabetes
All participants
All participants
Years from randomization
Cu
mu
lativ
e in
cid
enc
e (
%)
Placebo Metformin
Lifestyle
Type 2 Diabetes PreventionType 2 Diabetes PreventionRisk reductionRisk reduction31% by metformin31% by metformin58% by lifestyle58% by lifestyle
The DPP Research Group, NEJM 346:393-403, 2002

Prevention of Type 2 with Lifestyle Intervention Tuomilehto, et al , Turku ADA 2000
• Intervention – 523 IGT, mean age 55, BMI 31
• Diet, exercise, frequent visits vs advice yearly
Weight
Loss
1st Year 2nd Year 4th Year
Intervention -4.2 -3.5 26 cases
10%
Control -0.8 -0.8 57 Cases
22%
Incidence of diabetes reduced – 58% (p=.0003)

PUBLIC HEALTH
RESPONSE

National Comprehensive Obesity-Diabesity Prevention Strategy
• Educational
• Behavioral
• Environmental
– Increase understanding and awareness– Change behavior– Ability to make the right choices

Key Targets
• Communities– Joint use schools, parks, libraries, organizations
• Workplace– Wellness programs, insurance,
• Government– Funding, policies
• Individual/Family– Behavior change
• Health Sector• Schools
– PE, nutrition services, health education

Breast Feeding
• Decrease in obesity• In Pima population, dose related decrease in
risk of type 2 with breast feeding• Most significant with exclusive breast feeding• Breast feeding regimen
– exclusive for 6 months– total for 12 months
Simmons D, Lancet 97, 157

Breast Feeding
• Native Canadian Population
• 4-Fold decrease in type 2 diabetes in adolescents
• Exclusive Breast Feeding
Young et al, Arch Pediatr Adolesc Med, 2002

Promotion of: RETURN TO ENERGY BALANCE
• Water intake
• Fruits and Vegetables
• Limiting Juice
• Avoiding Sugar Containing Sodas
• Decreasing Saturated Fat
• Near Eliminating High Density/Low Nutrient Foods

School Could Be A Setting For
• Public education
• Epidemiological studies
• Early intervention with at-risk groups
• Screening and early detection

SStudies to tudies to TTreat reat OOr r PPrevent revent PPediatric ediatric TType ype 22 DDiabetesiabetes((STOPP-T2DSTOPP-T2D))
• Population based trial
• Increase physical activity
• Nutrition promotion
• Social Marketing, Behavioral Component
• Biologic outcome measures – primary– Reduction in risk factors

CONCLUSIONS
• Why are Children Obese– Too much food, no activity
• Insulin Resistance and Relative Beta Cell Failure– Intrauterine environment, postnatal feeding
• Type 2 Diabetes– Symptomatic presentation, treatment algorithms,
screening
• Public Health/Advocacy – School policies, legislative agenda
– Concentrate on pre and perinatal periods