Embed Size (px)
Citation preview

1
the diabetes epidemic and its
impact on Thailand
Researched and written by:

2
Diabetes is a chronic disease that requires life-long treatment and greatly increases the risk of serious, costly complications including heart attack, stroke, kidney failure, blindness and limb amputa-tion1,2.
Today, 382 million people in the world have diabetes3.
The number of people with diabetes is increasing in every country in the world3.
DIABETES, A GLOBAL EPIDEMIC

3
“No country is immune to the threat and no country is fully equipped to re-pel this common enemy alone. The coming fight will require a united stand with the full support of the international community, for this is a battle the world cannot afford to lose.”Prof Jean Claude Mbanya, President of the International Diabetes Federation, 2009-2012IDF press release, 18 October 2009
“If we fail to give people with diabetes the long and healthy lives we are capable of giving them, we will not be forgiven.”Bill Clinton, US President, 1993-2001Keynote lecture at the ‘Global Changing Diabetes Leadership Forum’, New York, 2007
“Without tackling the diabetes epidemic which is now gripping our world, we will, I fear, find many of our ambitions for the future simply impossible to achieve.”Kofi Annan, Secretary-General of the United Nations, 1997-2006Keynote lecture at the ‘Unite to Change Diabetes Forum’, Moscow, 2008
“We believe addressing the prevention and control of chronic noncommu-nicable diseases offers a window of opportunity to create healthy develop-ment. Unless this opportunity is seized by donors, governments and other partners, the current progress on the internationally agreed developmentgoals will be undermined and countries will face unbearable costs to theireconomies and health systems. The world is thus at a unique tipping point in the history of public health; an opportunity that will rapidly fade if no timely action is taken.”.Prof Pierre Lefebvre, Chairman of the World Diabetes Foundation, 2003-presentAnnual Review of the World Diabetes Foundation, 2010
“Cancer, diabetes, and heart diseases are no longer the diseases of the wealthy. Today, they hamper the people and the economies of the poor-est populations even more than infectious diseases. This represents a public health emergency in slow motion.”Ban Ki-Moon, Secretary-General of the United Nations, 2007-presentUnited Nations global summit on non-communicable disease, New York, 2011
“In the absence of urgent action, the rising financial and economic costs of these diseases will reach levels that are beyond the coping capacity of even the wealthiest countries in our world.”Margaret Chan, Director-General of the World Health Organisation, 2007-present The First Global Ministerial Conference on Healthy Lifestyles and Noncommunicable Disease Control, Moscow, 2011

4
Today, 3.2 million people have diabetes in Thailand3.
By 2035 an additional 1.1 million Thai adults will live with diabetes3.
An estimated 183 people die of the consequences of diabetes in Thailand... every day3.
DIABETES IN THAILAND

5
PREFACEChanging lifestyles lead to overweight and obesity, which has now become one of the leading causes of chronic non-communicable diseases (NCDs), also known as lifestyle diseases. These diseases are currently spreading globally and becoming increasingly more severe. If they are not adequately ad-dressed, the NCDs will likely cause more morbidity, disability, mortality, and substantial healthcare burden and economic loss.
Thailand is also facing the problem and is attempting to address the threats of five major preventable lifestyle diseases including diabetes mellitus, hypertension, heart diseases, cerebrovascular disease and cancers. The attempt to tackle these diseases is included as one of the major development goals in the 10th and 11th National Economic and Social Development Plan. We realise the need for multisectoral engagement in order to adequately address the problems, the Ministry of Public Health (MoPH), the National Economic and Social Development Board (NESDB) and Mahidol University have collaborated to develop the ‘Thailand Healthy Lifestyle Strategic Plan 2011-2020’ in response. The cabinet has, in principle, approved this national strategic plan and its implementation mechanism, which will be used as a framework to advance coordinated and united efforts of program implementation at all levels, with the aim to campaign for a new, healthy way of life which reduces risk factors, morbidity, compli-cations, disability, mortality and financial burden at individual, family, community, society and national levels.
H.E. Mr. Pradit SintavanarongMinister of Public Health, Thailand, 2013

6
Diabetes is a threat to Thai society, to avert the worst, clear priorities should be set for the future management of diabetes. First, screening should be increased; screening for diabetes in high risk populations as well as sys-tematic annual screening for diabetes complications in patients already diagnosed. Second, the factors affect-ing poor treatment outcomes in the majority of patients not well controlled today have to be identified and addressed. These priorities address the need for early diagnosis and successful intervention to help prevent and delay the onset and progression of the serious and costly complications of diabetes.
Third, policy should specify clear targets. Fourth, a monitoring framework should be provided and used to track progress towards these targets, requiring further improvement in data availability. Up-to-date data on the medi-cal and economic burden of diabetes at the national level and at least a regional level is essential to identify needs and monitor progress. Priority areas for data collection include the incidence of diabetes in children and adults, the prevalence of GDM, the cost of diabetes and its complications and finally treatment compliance and outcomes at an individual level. Some data is available from individual studies, however systematic and longi-tudinal data collection is essential. The NHES survey is conducted regularly and includes good data on diabetes prevalence, however these surveys are only conducted every 5 to 7 years.
Fifth, promotion of a healthy lifestyle for the prevention of diabetes has to be stepped up through education and quality health information delivered to the public. Efforts to address these issues have already started in some areas of the country but not nationwide. In order to achieve this, a multisectoral effort including concert-ed policy actions from a variety of policy makers (beyond the Ministry of Public Health) and of public opinion leaders as well as interventions involving public and private delivery channels is required.
Professor Chaicharn DeerochanawongDiabetes and Endocrinology Unit, Department of MedicineRajavithi Hospital, Rangsit Medical School, Bangkok, Thailand
Diabetes mellitus was the first chronic noncommunicable disease that was brought up to the attention of the National Epidemiology Board of Thailand. In 1987, a Task Force for Control of Diabetes Mellitus was estab-lished. One year after gathering all existing data, a technical report was released with the title ‘Diabetes Mel-litus in Thailand 1987: Review and Prospective’. The report called for the need of standardised data collection in all aspects of diabetes including epidemiology, care process, management outcome, risk factors and com-plications. Updating diabetes knowledge for practising physicians, care teams and education for patients and caregivers was required among many priorities of care delivery. For almost two decades of accumulated works, an improvement in many areas was recorded in the ‘Diabetes Situation in Thailand 2007’. The progress was recently summarised by Prof. Chaicharn Deerochanawang and published in Globalisation and Health in 2013.
The National Health Security Office (NHSO) also paid attention to the importance of holistic management of diabetes mellitus and foresaw the necessity of improving the quality of care and outcomes. A working group of NHSO and diabetes experts launched a ‘Clinical Practice Guideline for Diabetes Mellitus’ in 2008. The NHSO and the Ministry of Public Health guided and supported the implementation of the clinical practice guidelines countrywide. A chronic care model has been initiated to facilitate efficient and effective care of diabetes in Thailand.
This booklet represents another version illustrating the burden and impact of diabetes mellitus in Thailand. Bringing diabetes care and outcomes to a higher quality level is a big challenge to all care providers with high expectations of success.
Wannee Nitiyanant, M.D.President, Diabetes Association of ThailandUnder the Patronage of Her Royal Highness Princess Maha Chakri Sirindhorn
FOREWORD

7

8

9
1. ExECUTIvE SUMMARyMuch progress has been made in recent years, but there is still room for improvement in tackling the growing diabetes challenge in Thailand. Successfully controlling type 2 diabetes will help millions with the disease lead a longer, healthier life but will also significantly contribute in the prevention of other chronic diseases, due to their shared risk factors, underlying determinants and opportunities for intervention.
The burden of chronic diseasesUntil recently, communicable diseases have been the primary cause of mortality and morbidity across the globe. The balance is however tipping towards non-communicable diseases (NCDs). Chronic diseases are one of the great-est challenges for Thailand. The most common of these diseases are cardiovascular disease (heart disease and stroke), cancer, respiratory disease and diabetes4, together they account for a substantial proportion of total mortality and disability5. Within the scope of a decade, the share of all deaths in Thailand by NCDs has increased from 59% in 2002 to 71% in 20086.
An integrated approach Most healthcare systems today are organised to treat the acute symptoms of disease and manage conditions sepa-rately. We are less advanced when it comes to integrated prevention efforts, early detection and care and treatment for chronic non-communicable diseases. An integrated patient-centred approach will capitalise on common treat-ment needs and thus have a greater impact.
In the case of type 2 diabetes treatment, research has shown the benefits of an integrated approach. Intensify-ing treatment to include tight control of multiple diabetes risk factors such as high blood glucose, blood pressure and cholesterol have been found to significantly reduce the risk of death from cardiovascular causes and the development of end-stage renal disease7.
What you can find in this book‘The diabetes epidemic and its impact on Thailand’ beginswith an introduction to diabetes and describes the seri-ous complications that may occur when the disease is not
adequately controlled. Following this, the burden of dia-betes in Thailand is discussed, reviewing available data on the prevalence of diabetes and discussing the human and financial burden of the disease in Thailand.
‘The Rule of Halves’ is then introduced as a simple concept to reveal the real challenges of managing diabetes success-fully. The book continues with a review of the quality of diabetes care and the current diabetes health in Thailand, stressing the importance of women’s and children’s health in the following section.
The book then asks the important question “What needs to change?”, outlining the benefits of early detection and the need for education and data collection. Finally, this book shares experiences from across the globe, showcas-ing successful national health strategies and local diabetes projects.
The objectives we have in mindAs effective interventions exist for the prevention and control of chronic diseases such as diabetes, the evidence investigated and summarised in this book aims to pro-vide payers, policymakers, patient associations, the expert community and other stakeholders in Thailand at a local, regional and national level with a clear demonstration of the challenges presented by diabetes and offers possible solutions.
It is hoped this book will contribute to the development of sustainable improvements in diabetes prevention and detection, and the provision of affordable, effective care throughout Thailand.
AcknowledgementWe thank Prof. Chaicharn Deerochanawong; this booklet draws inspiration and important insight and knowledge from his recently published review article ‘Diabetes man-agement in Thailand: a literature review of the burden, costs, and outcomes’. His paper can be downloaded from: http://www.globalizationandhealth.com/content/9/1/11.

10

11
TABlE OF CONTENTS
Preface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Foreword. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
1. Executive summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2. About diabetes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3. Diabetes in Thailand . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
4. The human burden . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
5. The financial burden . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
6. The rule of halves . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
7. Current diabetes health in Thailand . . . . . . . . . . . . . . . . . . . . . . . . 26
8. Women, diabetes and the next generation . . . . . . . . . . . . . . . . . . . 30
9. What needs to change?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
10. Prevention provides the greatest potential for gain . . . . . . . . . . . . . 33
11. Improving outcomes by early detection . . . . . . . . . . . . . . . . . . . . . . 35
12. Patient self-management, education and support . . . . . . . . . . . . . . 37
13. Treatment towards target . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
14. Measure, share, improve . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
15. Conclusion: diabetes affects Thailand, at every level. . . . . . . . . . . . . 41
16. Sharing experiences. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
17. About Novo Nordisk . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
18. Diabetes glossary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
19. References. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47

12

13
2. ABOUT DIABETESDiabetes is defined by a failure of the pancreas to produce insulin or toproduce and utilise sufficient insulin to keep blood glucose under control8.
Diabetes and InsulinDiabetes is a chronic disease that occurs when the pancreas is no longer able to make insulin, or when the body cannot make good use of the insulin that it does produce8.
Insulin is a hormone made by the pancreas whose main ac-tion is to enable glucose to be transported from the blood into the cells of the body so it can be used for energy. It acts like a key that opens the door for the food (glucose) to leave the bloodstream and get into the body’s cells9.
When not enough insulin is produced, or when it is not used effectively, glucose builds up in the blood (known as hyperglycaemia). Over the long-term high glucose levels are associated with damage to the body and failure of various organs and tissues8.
Types of diabetesType 1 diabetes is usually caused by an autoimmune reac-tion where the body’s defence system attacks and destroys the insulin-producing cells. The disease may affect people of any age, but usually develops in children or young adults. People with type 1 diabetes are dependent on insulin injec-tions for survival8. Type 2 diabetes accounts for at least 90% of all cases of di-abetes. It is characterised by insulin resistance and a relative insulin deficiency, either or both of which may be present at the time of diagnosis. It most commonly occurs after the age of 40 and is strongly associated with overweight and obesity which contributes to insulin resistance10. Increasing-ly, type 2 diabetes also affects overweight children, adoles-cents and young adults11.
Both type 1 and type 2 diabetes are serious. There is no such thing as mild diabetes8.
GDM (Gestational Diabetes Mellitus) is a form of diabetes occuring during pregnancy. Estimates of its prevalence differ across the world depending on diagnostic criteria, however it may develop in as many as one in 6 pregnancies worldwide12. GDM is associated with complications to both mother and baby such as larger than normal babies and higher rates of foetal abnormalities. Although the diabetes typically disappears after delivery, both women with GDM and their offspring are at increased risk of developing type 2 diabetes later in life8.
Other types of diabetes exist, including latent autoimmune diabetes in adults (lADA). This is sometimes referred to as type 1.5 diabetes, as people present signs of both type 1 and type 2 diabetes. At least 10% of all cases of type 2 diabetes have some symptoms of type 1 diabetes13.
Pre-diabetes occurs when blood glucose levels are higher than normal but not high enough for a diagnosis of ‘full-blown’ diabetes. People with pre-diabetes are at high risk of developing type 2 diabetes and have an increased risk of cardiovascular disease9.
Symptoms and diagnosisThe onset of type 1 diabetes is usually sudden and dramatic while the symptoms of type 2 diabetes can often be mild or absent, making it hard to detect8. All too often type 2 diabetes is only diagnosed when presenting to the doctor with the first signs of complications or during a random test. As early detection and treatment can decrease the risk of developing the complications of diabetes, it is important to recognise its symptoms, which include14:
• Tiredness• Feeling of thirst• Frequent urination• Feeling hungry
• Blurry vision• Slow healing cuts• Tingling or numbness in hands or feet
living with diabetesIt is not easy to hear a diagnosis of diabetes. There is no cure and people will often have seen headlines of what can go wrong or frequently will have witnessed first-hand the negative effects of uncontrolled diabetes9.
It entails a number of physical problems which affect both private and working life and may require additional sup-port from friends or family. These may include discomfort caused by high blood sugar, such as tiredness and frequent infections, or discomfort caused by low blood sugar such as palpitations and mood swings.
The stress involved can often lead to depression, especially for young people with diabetes, so support form healthcare professionals and family members is vital. If people with diabetes have access to adequate support, they are more confident and more able to manage their own treatment effectively.

14
Diabetic retinopathy is the leading cause of blindness among working-aged adults around
the world17. As many as 1 in 2 people with long-standing diabetes in Thailand will devel-op mild to moderate eye complications such
as blurred vision37 whereas 1 in 10 will experi-ence vision threatening eye complications15.
higher risk of stroke
3-4Strokes occur when the flow of oxygen to the brain is interrupted, most often caused by a blood clot that blocks blood vessels in the brain. Diabetes accelerates atherosclerosis, the hardening of arteries, which leads to accu-mulation of plaque and when this ruptures a stroke may occur. Stroke occurs 3 to 4 times as often in people with diabetes compared to those without diabetes20,47,48. For people below 65 years of age the risk is 15 times higher20.
Diabetes complicationsDiabetes can lead to many serious health problems, usually after a number of years and particularly if diabetes is not de-tected early or well treated. Consistently high blood glucose levels can damage the small blood vessels in the eyes (retinopa-thy), kidneys (nephropathy) and the nerves (neuropathy); these are called micro-vascular complications. High blood glucose also affects larger blood vessels by accelerating the build-up and inflammation of plaque (atherosclerosis) which contributes to stroke, coronary heart disease and peripheral artery disease; these are called macro-vascular complications. People with diabetes have a 2-fold excess risk of a wide range of vascular diseases18 and are also more likely to die from these142. Other, non-vascular, complications of diabetes include teeth and gum problems and infections and people with diabetes also have a higher risk of cancer and are more likely to develop depression18.
Kidney disease is caused by dam-age to small blood vessels in the kidneys leading to the kidneys becoming less efficient or to fail al-together. People with kidney failure require dialysis or kidney transplan-tation for survival. Diabetes is the leading cause of kidney failure in Thailand, 6 to 7 people start renal replacement therapy every day42. have nerve
damage Diabetes can cause damage to the nerves throughout the body when blood glucose
and blood pressure are too high17. The major-ity of people with diabetes will develop some form of nervous system damage16 leading to
impaired sensation or pain in extremities of the body, including the feet or hands, slowed
digestion of food and erectile dysfunction.
70%
experience foot ulcers
10%
loss of feeling in the feet from nerve damage can allow injuries to go unnoticed, leading to infections. As diabetes slows healing of wounds, serious ulcers may develop affecting ten percent of people with diabetes. In Thai-land, 3 to 4% of people with long-standing diabetes undergo a lower limb amputation as a consequence of progressing ulcers37.
times
Coronary heart disease is caused by plaque building up along the inner walls
of the arteries (atherosclerosis) of the heart which narrows the arteries and
restricts the blood flow. This may cause a heart attack. For both men and women with diabetes the risk of fatal coronary
heart disease is elevated, the risk for women with diabetes is higher (3.5 times)
than in men (2.1 times)85
higher risk of fatal heart disease
3times
of kidney failure in Thailand
#1cause
vision threatening eye complications
10%people
people
early deathDiabetes is associated with a 2-fold higher risk of death48,142 and, diagnosed at age 50, diabetes reduces a person’s life expectancy by 6 to 8 years 18,136.6-8
years
people
+

15
Diabetes is a chronic, progressive disease that requires life-long treatment and greatly increases the risk of serious, costly complications including heart attack, stroke, kidney failure, blindness and limb amputations.
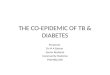
How is diabetes managed?People with type 1 diabetes have lost the ability to pro-duce insulin themselves and insulin therapy is required to stay alive9. Most people with type 2 diabetes begin treatment with dietary changes and increased exercise but unfortunately most patients are unsuccessful in control-ling blood sugar without pharmacotherapy. Tablets that stimulate insulin release or enhance insulin sensitivity are typically the first medications used in treatment19.
As the number of insulin producing cells (Beta-cells) inevi-tably decline over time, blood sugar rises and further phar-macotherapy is required to maintain control10. Treatment guidelines from the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) propose a step-wise intensification. Ultimately, insulin therapy will be required in many people with type 2 diabetes to maintain good glycaemic control21.
Challenges in diabetes managementThe challenges of treating diabetes are many. People with diabetes require extensive education and motivation to comply with pharmacotherapy, monitor glucose levels and participate in self-care to control their disease. Medication requires titration and monitoring and a careful balance has to be maintained between strict glycaemic control required to avoid complications and side-effects such as weight gain and hypoglycaemia (low blood glucose).
Hypoglycaemia is often considered the limiting factor in the successful treatment of diabetes22. Whereas mild hypoglycaemia is definitely unpleasant, if left untreated it can lead to severe hypoglycaemia (very low blood glucose) possibly resulting in unconsciousness and in some cases can even be fatal. Evidence further shows that severe but also moderate hypoglycaemia is associated with an overall increased rate of long-term mortality in type 2 diabetes23.
Delaying the onset of complicationsIt is well established that the risk of micro- and macrovas-cular complications is related to glycaemia as measured by HbA1c. Reducing glucose therefore remains a major focus of therapy. Prospective randomised clinical trials have doc-umented reduced rates of complications in people with diabetes treated to lower glycaemic targets21. Findings from a long-term, landmark study in the UK show that intensive blood-glucose control substantially decreases the risk of microvascular complications24. After 10 years of follow-up these benefits are maintained and demonstrate lower mortality in the intensively controlled group25.
Data from the same study was used to demonstrate that each 1%-point reduction in HbA1c reduces the risk of complications, without an apparent lower threshold26.
Diet and exercise
Tablets
GLP-1
Insulin
Time
Bet
a ce
ll fu
nct
ion
Progression of type 2 diabetes and treatment intensification19

16

17
3. DIABETES IN THAIlANDAn estimated 3.2 million Thai adults have diabetes today; 6.4% of the adult population. This number will increase by more than 1.1 million by 20353.
Diabetes is a serious problemThe growth of diabetes is serious. Increasing obesity in children and adults is to diabetes (and other chronic diseases) what melting glaciers are to climate change: a warning signal of times to come.
The prevalence of diabetes in Thailand - diagnosed and undiagnosed - has grown dramatically in the last decade and if nothing changes its growth will continue. A good indication of the challenge to come is the 4.1 million Thai adults with pre-diabetes today3. This group has impaired glucose metabolism but has not - yet - developed overt diabetes. They are at high risk of developing diabetes in the future unless a significant change in lifestyle is made, often aimed at reducing weight.
Obesity Obesity is an important risk factor for chronic diseases, including diabetes. Obesity, defined as a body mass index (BMI) in excess of 30 kg/m2 but also overweight (BMI >25 kg/m2), greatly increases the risk of developing type 2diabetes.
Being obese leads to more than a seven-fold increase in the risk of developing type 2 diabetes, while being over-weight increases the risk nearly three-fold. Furthermore, people who are severely obese (BMI >35 kg/m2) have a risk of developing type 2 diabetes up to 60 times greater than those with a normal bodyweight27.
In 2009 more than 30% of Thai men and more than 40%
of Thai women were estimated to be overweight, a rate that has doubled over the last 2 decades28,29. Data from the National Health Examination Survey (NHES) shows the prevalence of diabetes to be as high as 1 in 7 in adults with a BMI over 30 kg/m2, more than 3 times as high as in those with a normal BMI30.
Although the typical time of onset of type 2 diabetes is after the age of 50, childhood and adolescent obesity is causing the emergence of type 2 diabetes in the young as a serious health problem. Whereas virtually all (19 out of 20) diagnosed cases of diabetes in the young were identi-fied as type 1 diabetes until 1995, a near-tripling of the obesity prevalence in the same period31 has caused a rapid increase of type 2 diabetes in the young to 1 in 5 cases of diabetes diagnosed.

18
Ageing With the typical onset of type 2 diabetes in Thailand after the age of 50 and with prevalence peaking at 1 in 6 between the ages of 55 and 74, the ageing of the Thai population points towards a rise in the disease burden32.
Population data suggests the number of Thai people over the age of 60 to be close to 20% of the total population by 2030, a doubling since 200033.
UrbanisationSedentary lifestyles and unhealthy diets are more common in urban areas. Not suprisingly, the prevalence of diabetes is higher in urban areas than in rural areas of Thailand. In particular people moving from rural areas to urban areas are at a higher risk of developing diabetes34.
The growth in the number of people with diabetes in Thailand is being fuelled by an ageing population and by increasingly unhealthy lifestyles with poor diets and falling levels of exercise causing a rapid increase in the rate of obesity.

19
The number of people with diabetes will grow by 1.1 million over the coming 2 decades, affecting 1 in 12 adults by 20353.
This growth is being fuelled by an ageing population and a rapid rise in the prevalence of obesity.
Overweight doubles the risk of diabetes, obesity triples the risk of diabetes30.
RAPID GROWTH OF DIABETES IN THAILAND

20
4. THE HUMAN BURDENDiabetes often affects people in their productive years when they carry a substantial responsibility for their families. The complications of diabetes are not only a personal tragedy, families and close ones are impacted and the burden of poorly treated diabetes can push families into poverty.
Diabetes is a leading cause of death As the number of people with diabetes continues to grow, diabetes is establishing itself as a leading cause of death. Diabetes already is the third leading cause of death in women of all ages and the leading cause of death in women over the age of 50. In men, diabetes ranks lower due to the higher mortality levels related to road traffic accidents and HIv/AIDS35.
Leading causes of death in women35
15-49 years 50-74 years >74 years1 HIv/AIDS Diabetes Stroke
2 Traffic acc. Stroke Isch. heart disease
3 Cancer cervix Isch. heart disease Diabetes
4 Stroke Nephritits Respiratory
5 Diabetes Cancer cervix Nephritis
According to estimates of the International Diabetes Federation, 180 Thai people die of the consequences of diabetes every day, nearly 8 every hour3.
ComplicationsThe long-term complications of diabetes are a serious and major burden of the disease. In a 2003 cross-sectional study with participation of 11 hospitals and more than 9.400 patients it was identified that diabetic nephropathy was the most common complication affecting 43.9% of the people with diabetes. This was followed by diabetic retinopathy (30.7%) and ischaemic heart disease (8.1%)36.
A 4-year study conducted from 2006 to 2010 in 1,120 patients reported very similar numbers and also found 24% of patients to have lost protective sensation in the feet due to neuropathy143.
It is important to realise the impact of disease duration on the prevalence of complications. Prolonged uncontrolled blood glucose is a major predictor of diabetes complica-tions24,25,26 and it is expected to see the prevalence of complications increase with diabetes duration. After 15 years of diabetes the prevalence of diabetic retinopathy was found to be 4 times as high as in Thai people with less than 5 years of diabetes37.
Similarly, whereas less than 1% of the people with dia-betes with a disease duration less than 15 years will have had a lower-limb amputation, this is 3.5% in the group with long-standing diabetes37.
Kidney disease (nephropathy)The job of the kidneys is to remove waste products from the blood. Sustained high levels of blood glucose can damage the blood-filtering capillaries in the kidneys and cause them to leak useful proteins into the urine. Small amounts of protein in the urine is called micro-albuminu-ria38 which occurs in up to 40% of Thai people with type 2 diabetes39,40 and increasies to more than 60% with long-standing diabetes37.
Unless diagnosed and treated early, kidney disease will get worse. When larger amounts of protein appear in the urine this is called macro-albuminuria which may result in end-stage renal disease when the kidneys fail and waste products start to build up in the blood. This is very seri-ous and a person with end-stage renal disease requires a kidney transplant or machinal blood filtering (dialysis)38.
Macro-albuminuria occurs in approximately 8% of Thai people with diabetes with 0.5% to 1% requiring dialy-sis or kidney transplantation39,40,41. Diabetes is the most common cause of end-stage renal disease accounting for nearly half of all new cases in Thailand. In 2009, dialysis was initiated in 2,425 Thai people with diabetes or 6 to 7

21
people every day42. In the same year, the total number of people with diabetes on dialysis was 9,487, an increase of 90% compared to 200742.
Eye disease (retinopathy)Tiny blood vessels (capillaries) in and behind the eyes’ retina - responsible for recording images - provide the required energy for the eye to function. When due to sustained high blood glucose the capillaries in the back of the eye balloon and pouches are formed, blurred vision may appear. This most common form of diabetic retinopa-thy is called non-proliferative retinopathy, developing in stages as more and more blood vessels become blocked38. One-in-five Thai people with diabetes has non-proliferative retinopathy41,43,44,45 and with duration of diabetes a major risk factor the prevalence in people with 20 years of diabe-tes was found to be 43%46.
Blood vessels can become so damaged they close off and cause new blood vessels to grow in the retina. This can lead to blood leaking onto the retina or scar tissue form-ing leading to blocked vision. This is called proliferative retinopathy and may ultimately lead to blindness38. Dura-tion of diabetes is again a major risk factor and prevalence of proliferative retinopathy increases from 2% in those with diabetes duration less than 5 years to 10% in those with diabetes for more than 15 years46. Blindness may oc-cur in 1.5% of people with diabetes43 making diabetes a leading cause of blindness.
Regular screening for diabetic retinopathy and aggressive management of associated risk factors (glucose, blood pressure) can help to prevent and delay the prevalence of diabetic retinopathy. laser therapy can help delay its progression and prevent severe visual impairment and blindness.
Cardiovascular disease (CvD)People with diabetes have a higher than average risk of having a heart attack or stroke, striking three to four times as often than in people without diabetes20,47,48. More than half of all people with diabetes globally18 and in Thailand49 will die of cardiovascular disease. People with diabetes of 50 years and older with CvD live on average 7.5 (men) and 8.2 (women) years less than people without diabe-tes50.
Macrovascular complications are reported by 1 in 3 Thai people with long-standing diabetes37. Coronary arterial disease, sometimes called hardening of the arteries, is reported by 1 in 6 and may lead to a heart attack or myo-cardial infarction. Stroke, the no.1 leading cause of death in Thailand35, strikes 4.4% of all people with diabetes36,41. Strokes are caused by a sudden interruption of the blood supply to the brain most often as a result of a blood clot
blocking a blood vessel in the brain or neck38.
Peripheral arterial disease (PAD) occurs when the blood vessels in the legs are narrowed or blocked by fatty depos-its and blood flow to feet and legs decrease, it increases the risk of heart attack and stroke. PAD is not easily diagnosed as it is often symptomless or symptoms are not recognised. In the Thailand Diabetes Registry Project prevalence of PAD was found to be 7.4% in long-standing diabetes37, however a study with specialised diagnostic equipment in a high risk diabetic population in Thailand has demonstrated a prevalence of 60%51.
Foot complicationsPeople with diabetes can develop many different foot problems, most often caused by nerve damage (peripheral neuropathy) when loss of feeling results in injuries going unnoticed. Poor circulation (PAD) in the lower limbs may also contribute to foot problems as feet may be less able to fight infection and heal38.
Nerve damage and PAD make it easier to get ulcers and infections leading to amputations. Twenty-four percent of Thai people with diabetes have loss of protective sensation in the feet143 and 5 to 6% have a history of foot ulcers36,41. Amputations occur in 2% of all people with diabetes41 and in long-standing diabetes 1 in 10 people will have had a foot ulcer and 3.5% will have undergone amputation37.Diabetes is the leading cause of non-traumatic lower limb amputation.
DepressionHaving diabetes is associated with a significantly higher risk of developing depression and other psychological problems compared with the general population38. This may be because of the stress of daily diabetes manage-ment or when facing diabetic complications. According to a 2008 study amongst people with diabetes visiting a Bangkok tertiary university hospital out-patient clinic 28% suffered from depression, with a higher prevalence identi-fied in those with poor glycaemic control52.
Depression not only causes suffering to the individual but can also adversely affect treatment adherence and is as-sociated with poor medical outcomes and high healthcare costs53.
FamiliesA diagnosis of diabetes imposes a lifelong burden, not only on the individual but also on their family, due to the constant need for practical and emotional management of the disease. The social and emotional impact on a family dealing with diabetes may be greater than the direct costs of treatment and lost income.

22
5. THE FINANCIAl BURDENDying young or living with long-term illness or disability has economic implications. The rapid growth in the number of people with diabetes has a dramatic impact on the direct and indirect cost for the individual with diabetes, the family, the national economy and the government.
The size of the problemAs the number of people with diabetes grows, the disease takes an ever-increasing proportion of national health care budgets. Because of its chronic nature, the severity of its complications and the means required to control them, diabetes is a costly disease, not only for the affected indi-vidual and his/her family, but also for health authorities54.
It is estimated that diabetes accounts for 12% of the total healthcare expenditure globally, although individual country estimates differ widely55. Whereas the estimated average spend on diabetes per person is USD 53 in South East Asia, this is USD 7,900 in the United States56.
The costs of diabetes in Thailandlittle information is available on the actual cost of dia-betes in Thailand. A 2009 micro-costing study of people receiving treatment in a 30-bed public district hospital in North-East Thailand estimated a mean cost of illness of THB 28,200 (1 USD = 31 THB)57 and the Minister of Public Health recently estimated the total cost of diabetes to ap-proach 50 billion THB144.
Although the cost of diabetes is most visible in direct med-ical costs such as dispensing and drug bills; these however make up less than a quarter of the yearly total cost. It is the in-hospital care of complications that contributes most with nearly half of the total cost57.
Economic costs of diabetesDirect non-medical cost contribute 40% to the total cost of illness with cost of informal care alone contributing 28%. The biggest contributor to indirect cost was found to be the cost of permanent disability, contributing 19% to the total cost of illness. The study is likely to have un-derestimated the real cost of illness by as much as 60% as it used minimum wages only to calculate cost of informal care and disability and not GDP per capita57.
The morbitiy and premature mortality rates attributable to chronic diseases highlight the need for effective interven-tions. Dying young or living with long-term illness or dis-ability has economic implications for families and society and the cost to employers and economies is increasing.
Complications drive costData from the Ministry of Public Health on diabetes-related hospitalisations shows a dramatic increase over the past decades, a strong indication of the increasing finan-cial burden of diabetes33. This is supported by actual cost data showing hospitalisation to contribute nearly 50% to the total cost of diabetes illness57.
A patient requiring hospitalisation sees a nearly 10-fold cost increase compared to a patient managed in the out-patient-department. Similarly, a patient with diabetic nephropathy or diabetic foot has a greatly increased cost of illness compared to one without58.

23
With the prevalance of complications of diabetes increas-ing with diabetes duration, it is unsurprising to see that the cost of illness increases with diabetes duration. During the first 5 years of the disease, the median yearly cost is THB 3,400 and is multiplied by more than 6-fold for those with a disease duration over 20-years57. It is the future burden of diabetes that is thus of greatest concern and an investment in prevention, early diagnosis and treatment may save cost later.
The cost of hypoglycaemiaIt is well understood that reducing blood glucose levels helps prevent or delay complications24 and may thus save costs. A key barrier to reducing blood glucose however is hypoglycaemia23. It has been demonstrated that patients are just as worried about hypoglycaemia as they are about complications such as blindness59. Many patients decrease their insulin dose after a hypoglycaemic event resulting in sub-optimal glucose control60. Beyond the indirect impact of hypoglycaemia on treatment compliance there is also a direct medical cost of hypoglycaemia. Severe hypogly-caemic events frequently require medical intervention and hospital admission61.
Data from Thailand on hypoglycaemia is scarce, one study however investigated the clinical risk factors associated with severe hypoglycaemia and recorded the length of stay after being admitted to hospital62. The study showed that at least 2 people with diabetes and severe hypogly-caemia were admitted to the hospital monthly, half of them unconsciousness. The average hospital stay was 6 days resulting in a direct cost per event of nearly THB 22,00058.

24
6. THE RUlE OF HAlvESAccording to the concept of the Rule of Halves63, only around 6% of people with diabetes live a life free from diabetes-related complications.
The silent pandemicWhile diabetes care has improved greatly in recent dec-ades, the International Diabetes Federation estimates 4.8 million people died of diabetes in 20123. This makes diabetes a bigger killer than HIv/AIDS, malaria and tuber-culosis combined64.
The Rule of Halves shows the gravity of diabetes and ex-plores which factors play a role - displaying the inequality of access to the right treatment and support63.
The Rule of HalvesOf all the people with diabetes in the world, only about 50% are thought to have been diagnosed3, meaning a huge part of the population is at risk of developing com-plications that will significantly impair their quality of life.
Due to late diagnosis up to half of all people with diabetes have some evidence of complications at the time of detec-tion65,66. For others the treatment they receive is inad-equate or they do not have access to medicine or doctors who can tell them how to use it. yet others maintain too
high blood sugar because they fear the consequences of low blood sugar (hypoglycaemia), a common side effect of (insulin) treatment.
Ultimately, the Rule of Halves suggests that only around 6% of people with diabetes live a life free from diabetes-related complications.
UN resolutionIn 2006, the IDF and the global diabetes community brought the “UNite for Diabetes” campaign to the highest political forum – the United Nations - to raise awareness. The UN passed Resolution 61/225 in December 2006, af-firming diabetes as a major global health threat.
The UN High-level Summit on Non-Communicable Diseases (NCDs) held in 2011 in New york was a major milestone. The Summit was only the second time the UN General Assembly devoted exclusive attention to a health-related issue and world leaders made unprecedented commitments to accelerate global progress on diabetes and NCDs66.
ACHIEVE TREATMENT TARGETS
ACHIEVE DESIRED OUTCOMES
DIABETES
DIAGNOSED
RECEIVE CARE

25

26
7. CURRENT DIABETES HEAlTH IN THAIlANDPoor glycaemic control increases the risk of long-term complications24. With around half of patients diagnosed and only a third of them reaching treatment targets, many people with diabetes in Thailand are at risk and will develop complications.
Data sourcesAn extensive literature search was conducted for a 2013 review of diabetes management in Thailand, finding 46 peer-reviewed papers68. These provide an accurate and up-to-date insight in the current diabetes health in Thailand and this booklet builds on this. The key sources of diabe-tes data used include:
• National Health Examination Survey (NHES); dis-ease data from a national representative sample of >20,000, conducted in 1991, 1997, 2004 and 2009
• Diabetes Registry Project; including 9,419 people with type 1 and type 2 diabetes, conducted in 2003 with follow-up until 2006 on mortality
• DiabCare Asia; data collection from over 2,300 pa-tients, conducted in 1998, 2001, 2003 and 2008 in Thailand and throughout South East Asia
• InterASIA; survey of nationally representative sample of more than 5,100 people conducted in 2000
• DM/HT study (NHSO research project); large national cross-sectional survey of quality of care in 28,649 people with diabetes from >600 hospitals throughout Thailand, data collected from 2010 to 2012
• A substantial number of other - mostly local - studies contribute to insights in specific sub-groups of people with diabetes or specific diabetes related topics
Diabetes diagnosis in ThailandThe IDF estimates that half of all people with diabetes in Thailand are not aware they have diabetes69. Findings from the NHES suggest that diagnosis rates have improved in recent years to reach 65%, however the NHES uses single Fasting Plasma Glucose measures for diagnostic purposes which may underestimate the prevalence of diabetes, as also acknowledged in the paper70. late diagnosis allows unchecked high blood glucose levels and thus contributes to the risk of the long-term complications of diabetes.
Access to care is not the same for allAccess to doctors and medicines to treat diabetes in Thailand should be adequate since the introduction of the Universal Coverage Scheme (UCS) in 2002. Today the scheme provides access to 75% of the population with the remaining 25% of the population covered by the Civil Servant Medical Benefit Scheme (CSMBS) and the Social Security Scheme (SSS) for formal employees.
Although coverage is universal, access to healthcare staff and medication does differ between the schemes. A comparative study showed a higher proportion of patients from the CSMBS than the UCS accessing secondary and tertiary care71, this is important as more patients were found to successfully reach their HbA1c target when treat-ed in specialised secondary and tertiary care hospitals139.

27
The national DM/HT study conducted by the NHSO (responsible for administering the Universal Coverage Scheme) found its members least successful in achieving an HbA1c level <7.0%139. The more generous health pack-age available and better access to specialised care for civil servants under the CSMBS scheme resulted in 30% more of its members achieving an HbA1c target of less than 7.0% compared to those insured under the UCS139.
With substantially more patients covered by the CSMBS reaching treatment targets, they will experience fewer complications and live a longer life24,25. It has been shown that mortality rates are almost twice as high for people with diabetes covered under the UCS compared to the CSMBS72. The social economic status of participants in the UCS scheme may explain part of the difference, however inequalities in care - such as access to drugs and special-ised health services - are a likely contributer as well68.
Quality of careTo control diabetes with the aim to reduce complications, it is essential to optimise physiological values such as glycaemic levels and blood pressure24 and perform regular examinations for complications116.
HbA1c has become the gold standard to assess glucose control. Evidence suggests the use of this and other tests is suboptimal in Thailand. In a 2008 review of the quality of diabetes care provided at 300 provincial Primary Care Units (PCU), HbA1c testing was found to be conducted annually in 19% of PCUs73. Another study in 48 provincial PCUs conducted in 2009 found 30% of medical files of people with diabetes contained the result of an HbA1c test conducted in the last 12 months74. Without accurate and recent knowledge of how good or how bad glucose control actually is, it must be near impossible to make the right clinical decisions in an effort to reach the targets so important for reducing complications.
With the rapid growth of the number of people with diabetes, primary care has to take on a bigger role in the prevention and management of diabetes. Evidence sug-gests that PCUs may be underfunded and understaffed73.
Annual examinations for complications are recommended as early intervention can prevent worsening of compli-cations116. A review of medical records of people with diabetes visiting the out-patient department of a major Bangkok University hospital found foot examinations conducted in less than 1 in 5 patients, approximately 4 out of 10 received eye examination and a similar number were screened for diabetic nephropathy75. Examinations in tertiary clinics however are conducted more frequently with up to 8 out of 10 people reported to have received eye examinations43.

28
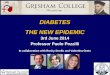
Regional variationThe NHSO’s DM/HT study was conducted from 2010 to 2012 in 602 hospitals in 76 provinces. The data available makes it possible to compare treatment outcomes on a regional level and this reveals considerable variation in average glucose control as measured by HbA1c; the risk of complications in some areas will thus be considerably higher than in others.
Whereas in Bangkok 45% of patients reached target HbA1c of less than 7.0%, in the North-East of Thailand only 23% of patients reached target, approximately half the patients compared to Bangkok139. Some of the individual provinces in the North-East of Thailand show less than 1 in 5 patients reaching target; in Nong Bua lum Phu the success rate is 11% and in Maha Sarakham and Amnart-Charoen it is just below 17%.
Several factors may contribute to this variation, first is the easy access to tertiary care in Bangkok, specialised dia-betes services may be less widespread outside of urban centres. A second factor may be differences in socio-economic situation; the majority of people in the prov-inces are employed in agriculture whereas a much larger proportion of the Bangkok population is higher educated and employed in the service sector.
Further analysis of the wealth of data in the NHSO’s DM/HT study - which is unpublished at the time of writing of this book - will provide further important insight in the differences of the quality of diabetes care offered across Thailand. Such analyses should provide important input to the formulation of national, regional and local healthcare resourcing plans with the ultimate objective to improve outcomes.
Know your ABCStrong evidence exists that controlling blood glucose helps delay and prevent complications25 and with more than half of people with diabetes also suffering from high cholester-ol and high blood pressure it is important to aim for good control of all these three risk-factors7.
A = A1c = Blood GlucoseA1c (or HbA1c) is a measure of average blood glucose levels over the last 2 to 3 months. It shows whether blood glucose stayed close to the target range most of the time or was too high or too low. The American (ADA) and European (EASD) diabetes associations recommend an HbA1c <7.0% for most people with diabetes although for some an HbA1c <6.5% is recommended21.
Thailand has its own guidelines for diabetes treatment endorsed by the Thai Diabetes Association, the Endocrine Society of Thailand and the Ministry of Public Health. The guidelines are updated every three to four years and the latest version was published in 2011140.
Many people in Thailand still rely on a Fasting Plasma Glu-cose (FPG) test to monitor glucose levels as HbA1c is not standard of care. Although valuable, FPG does not give in-sight how good or bad long-term glucose has been, it can only tell how good or bad glucose is at the moment of the test and may provide a too optimistic picture of glucose control. Whereas HbA1c and FPG testing is typically done during regular check-up visits in the hospital, it is essential that patients assume an active role in their care. Struc-tured education of patients is considered to play a critical role alongside self-monitoring of blood glucose (SMBG)116.
SMBG has been recommended for people with diabetes and their health care professionals in order to achieve a
Success rates of patients reaching HbA1c<7.0%139 by NHSO’s BranchPe
rcen
tage
of Th
ai a
dults
reac
hing
HbA
1c <
7.0%
50%
40%
30%
20%
10%
0%
Bang
kok Br
anch
(Reg
ion 13)
Sarabu
ri Br
anch
(Reg
ion 4)
Suratth
ani B
ranc
h
(Reg
ion 11)
Ratch
abur
i Branc
h
(Reg
ion 5)
Phits
anulo
k Br
anch
(Reg
ion 2) Rayo
ng B
ranc
h
(Reg
ion 6)
Song
khla
Bran
ch
(Reg
ion 12)
Nako
rnsa
wan B
ranc
h
(Reg
ion 3)
Chian
g Mai
Bran
ch
(Reg
ion 1)
Natio
nal
N. R
atch
asim
a Br
anch
(Reg
ion 9) Ud
onth
ani B
ranc
h
(Reg
ion 8)
U. R
atch
atha
ni Br
anch
(Reg
ion 10) Khon
Kae
n Br
anch
(Reg
ion 7)

29
specific level of glycemic control and to prevent hypo-glycemia141. In Thailand, the glucose strips required for SMBG are not reimbursed and the proportion of patients using SMBG as part of their treatment plan is low at 36% despite most physicians advocating its use80.
All studies reviewed show that unfortunately only a minor-ity of people with diabetes in Thailand manages to achieve their glucose target of HbA1c <7.0%76-82,139. Four out of ten people with a relatively short duration of diabetes reaches target, however those with a longer duration of diabetes generally have a higher level of HbA1c and as few as 1 in 4 will achieve their glucose target139.
On average, one-third of patients achieve an HbA1c <7.0% and a similar proportion has very poor glucose control with HbA1c levels higher than 9.0%139. These patients have a considerable excess risk of developing complications and early death24,25.
B = Blood Pressure Elevated blood pressure (hypertension) and blood glucose are - together - responsible for much of the risk increase of cardiovascular complications. Hypertension as a co-morbidity is very common with prevalence ranging from approximately 40% in studies with recently diagnosed patients77 to up to 80% in studies with patients with dia-betes duration of more than 10 years82.
Despite more than 8 out of 10 people with diabetes re-ceiving anti-hypertensive medication in the Diabetes Reg-istry Project, as few as 14% achieved treatment targets83. Since 2003, the time of data collection for the Diabetes Registry Project, access to anti-hypertensive medications has improved dramatically and in the recent DM/HT study 52% of people with diabetes had blood pressure below target of 130/80 mmHg139, similar to the results from the 4-year Thai DMS Diabetes Complications project com-pleted in 2010143.
C = CholesterolThe third risk factor for many of the long-term complica-tions is elevated levels of bad cholesterol (dyslipidaemia). Dyslipidaemia is present in as many as 80% of people with diabetes. Before the introduction of the Universal Care Scheme 55% of all patients were prescribed lipid-lowering agents with a further 30% requiring but not receiving this type of medication84. Cheap generic statins have made access to medicine much easier and as many as 8 out of 10 people with diabetes today take lipid lowering medica-tion80 with 44% reaching recommended lDl levels <100 mg/dl139.
Current diabetes health; conclusionAll studies in people with diabetes report that glucose control is sub-optimal in Thailand. Approximately one-third of all patients achieve the target HbA1c of <7.0% however fewer do so as diabetes duration increases. It is also important to identify that control tends to be better for people managed in tertiary care and by implication is better for those with better access to tertiary care and bet-ter medicines.
To delay or even prevent complications and to prolong a healthy life, glucose control has to improve. From the evidence presented in this chapter, access to specialised healthcare staff, medicine, education and self-man-agement tools may all provide good starting points for improving quality of care and improving outcomes for people with diabetes. Action plans should be developed taking regional needs in account as marked differences can be observed in treatment outcomes across provinces.
Measuring progress is important and the NHSO’s DM/HT project is a good example of how powerful insights can be obtained to direct healthcare strategies and develop actionable plans to improve care.

30
8. WOMEN, DIABETES AND THE NExT GENERATIONGender influences the development of risk factors and diseases and affects health risks, access to and utilisation of healthcare.
Women are at greater risk than menIn women with diabetes, the risk of death from coronary heart disease is about 50% greater than in men85. It also appears that the effects of hyperglycaemia in combination with other risk factors such as smoking, hypertension, hy-percholesterolaemia and overweight are more harmful to women than men86. In type 1 diabetes, women are twice as likely as men to suffer neural and retinal problems87.
These gender differences in mortality and risk of complica-tions may be explained by more frequently occurring high levels of bad cholesterol and high blood pressure in wom-en85. Another potential reason is that pre-menopausal women with diabetes lose the natural protection against heart disease that non-diabetic women have86.
Diabetes kills more Thai women than menIn Thailand, more than twice as many women die of diabetes than men. At ages 50-74, diabetes is ranked as 7th cause of death in men whereas it is ranked as the 1st leading cause of death in women, responsible for 1 in 8 deaths36. Although independent factors such as road-traf-fic and HIv / Aids mortality play a role in explaning these differences, it is also true that in Thailand more women
than men have diabetes; 8.3% vs. 6.6%70. This may be explained by a 50% higher prevalence of overweight and obesity in women compared to men29.
The foundations of life are laid in early lifeIn addition to the genes they pass on to their offspring and the direct biological influene imparted during preg-nancy (through the uterine environment), women can also influence the next generation by feeding and caring for their children and encouraging them to adopt a healthy lifestyle88. Healthy habits, such as eating a balanced diet, exercising and not smoking, are learnt early in life, and are associated with parental examples89.
Interventions that account for a life-course approach to chronic diseases highlight that chronic disease risks increase with age and that interventions made early in life produce a substantial risk reduction later in life.
Gestational diabetesThe value of a healthy pregnancy cannot be underesti-mated, directly, Gestational Diabetes Mellitus (GDM) is as-sociated with an elevated risk of birth complications. From a diabetes perspective, women diagnosed with GDM are seven times more likely to develop type 2 diabetes later in
Impact of intervention to chronic diseases

31
life compared with women without GDM90. Furthermore, children of mothers with GDM or pre-existing diabetes are more likely to develop diabetes themselves in later life91,92.
According to WHO criteria, GDM affects 1 in 7 preg-nancies in Thailand93 and with the stricter criteria of the International Association of the Diabetes and Pregnancy Study Groups as many as 23% of pregnancies in Thailand was found impacted by GDM12. Reason for the preva-lence estimates to vary significantly are the differences in screening methodology, testing procedures and diagnos-tic criteria applied in various studies and the controversy around these. It is evident though that if and when close follow-up and testing is applied, prevalence of GDM is high. This was recently confirmed by a prospective study in Chulalongkorn hospital which identified up to 1 in 5 women with GDM142.
Fact is, as young Thai women approach the age of first birth their level of physical activity is going down and at age 18 is less than a third it was at age 1394. Prevalence of overweight and obesity in women increases rapidly after age 18 and nearly a third of women is overweight26 at the time when their first child is born95. With a rising aver-age age of marriage in Thailand96, together with weight a key risk factor for GDM, the prevalence of GDM is set to increase.
Children with type 1 diabetesThe incidence of type 1 diabetes in Asia and Thailand is low in comparison to Europe. Whereas 30 to 40 children
per 100,000 are diagnosed with type 1 diabetes annu-ally in Northern Europe97, this number is as low as 1.6 per 100,000 children in Bangkok98 and possibly even lower at 0.6 per 100,000 children in Northern99 and Southern100 Thailand. Genetic susceptibility may play a role101 and it has been suggested that a lower exposure to sunlight and vitamin D contributes to the higher incidence in Europe102.
It is also worthwhile to note that in Thailand, the inci-dence rate of type 1 diabetes appears to be much higher in girls than in boys, for reasons not explained.
Tomorrow’s challenge: children with type 2 diabetesAlthough the incidence of type 1 diabetes in Thai children is suspected to increase98-100, there is more concern for the increase in the number of children with type 2 diabetes coinciding with the rapidly increasing prevalence of obe-sity in children31.
The paediatric department of Ramathibodi hospital has seen the proportion of children with type 2 diabetes in-crease from virtually none in the 1990s to 40% of all cases by 2005103. Similar data is reported from Siriraj hospital where 30% of all children with newly diagnosed diabetes in 2004 were diagnosed with type 2104. The incidence rate of type 2 diabetes in children can be expected to have increased further in the last years but no recent data was discovered to provide further insight. Better data availabil-ity should help contribute to an appropriate health policy response.

32
The social and financial burden of diabetes is large and growing fast. Most of the cases of type 2 diabetes are preventable and most of the long-term complications can be delayed or prevented.
If we fail to act now, the future costs will be even higher.
long-term rather than short-term thinking is essential. Investment in measures to prevent diabetes, to diagnose the disease early and treat it well is critical and urgent. Strong systems are also needed to track progress and drive improvement.
• Measure: collect information on as local a level as possible• Share: publish this information and identify the best practices• Improve: learn from the differences, exchange best practices and
implement them to improve outcomes for people with diabetes
9. WHAT NEEDS TO CHANGE?

33
Primary prevention of chronic diseasesPrevention programmes must be recognised as a corner-stone in a global response to the chronic disease bur-den105. By encouraging and facilitating a healthier lifestyle with a balanced diet, moderate exercise, and an avoidance of tobacco and alcohol, primary prevention aims to pre-vent people from developing chronic diseases.
large clinical trials as well as ‘real-world’ prevention programmes have provided evidence that lifestyle inter-ventions can prevent or delay the onset of type 2 diabetes in people at high risk107. Specifically, the risk of develop-ing type 2 diabetes can be reduced by 58% over a 3 to 5 year period for people with impaired glucose tolerance by intensive lifestyle modification programmes108,109. A risk reduction of 31% can be achieved through pharmacologi-cal intervention109.
The key to successful prevention is lifestyle changes, such as weight reduction, increased physical activity, and dietary modifications to increase dietary fibre and reduce total and saturated fat intake. The more of these lifestyle goals or healthy behaviours that are achieved, the lower the incidence of type 2 diabetes107,110.
This has clear benefits for the individual and society, as preventing or delaying the onset of diabetes will reduce the occurrence of costly and irreversible diabetes-related complications.
The complex nature of chronic diseases, including diabe-tes, requires a sustainable and comprehensive approach to prevention. Ideally, prevention programmes should combine broad population-based primary prevention while simultaneously targeting disadvantaged groups and peo-ple at high risk of developing a chronic disease105.
10. PREvENTION PROvIDES THE GREATEST POTENTIAl FOR GAINDiabetes and other chronic diseases, especially for people at high risk, canbe delayed or even avoided by prevention programmes.
Common risk factorsThe chronic disease burden is largely caused by shared modifiable risk factors, including diet, physical activity, alcohol and tobacco105. Based on these common risk fac-tors, a common approach could reap significant rewards.
A community-based prevention programme – for example, one that encourages a healthy diet – could have the ben-efit of reducing the rise in diabetes, but also of reducing the risk of other chronic diseases. Furthermore, multiple risk factors are often present within the same individual.

34
As a ‘health in all policies’ approach is needed111, it is necessary to collaborate to ensure the success of health promotion and disease prevention interventions; health-care professionals, payers, education providers, the food industry, the media, urban planners, politicians and non-governmental organisations must join forces to utilise pre-vention efforts112. Furthermore, alignment of all national policies including agriculture, trade, industry and transport is needed to promote improved diets and increased physi-cal activity4.
Primary prevention is often cost- effectivePrevention programmes improve health in the long term but can involve costs in the short term. Furthermore, in the case of chronic diseases, the health benefits – and cost savings – are only realised many years after having imple-mented such prevention programmes. Health budgets are
often allocated to activities that provide tangible benefits in the short term – even if the benefit to society in the medium to long term is smaller, compared with investing in prevention programmes112.
However, ‘best buys’ in terms of prevention exist. These interventions have a significant public health impact, and are highly cost-effective, inexpensive and feasible to implement. Such interventions in terms of lifestyle include promotion of public awareness about diet and physical activity through mass media, reduced salt in food and replacement of trans-fats105.
By encouraging reduced consumption of tobacco,alcohol and unhealthy food, improving awarenessof healthy lifestyles and using financial incentives,prevention programmes can effectively tackle the leadingcauses of NCDs and their underlying risk factors112.
Thailand Healthy lifestyle StrategyRecognising the need for multi-sectoral collaboration to tackle the emerging burden of chronic non-communicable diseases, the National Economic and Social Development Board (NESDB), the Ministry of Public Health (MoPH) and the Institute of Nutrition of Mahidol University (MU), have collaborated to prepare the Thailand Healthy lifestyle Strategic Plan for 2011 to 2020113.
In this strategic document the ultimate long-term goal outlined is to increase life expectancy free of lifestyle dis-eases, decrease mortality from and expenses for treatment of lifestyle diseases.
Key medium term targets are aimed at reducing obesity and increasing physical activity. It also recognises that successful intervention requires leaders of all sectors to collaboratively push the identified policies.
The strategic plan was approved in principle by the cabinet in 2011 although no detailed action plan has been pub-lished covering its implementation towards target.

35
11. IMPROvING OUTCOMES By EARly DETECTIONEarly detection and appropriate intervention presents an opportunity to improve outcomes for people with diabetes and other chronic diseases.
Is early detection warranted?In 2013, the International Diabetes Federation3 estimated 4.1 million Thai adults had impaired glucose tolerance and are at increased risk of developing diabetes in the future. This represents 8.4% of the Thai adult population and is expected to affect more than 1 in 10 Thai adults by 2035.
Why detect early?The purpose of early detection is to detect a disease with no apparent symptoms and improve the patient’s outlook by timely treatment. Health checks can identify people who are undiagnosed or at high risk of developing a dis-ease and allow for treatment and prevention. Criteria for identifying when health checks are effective measures to improve public health have been developed:
1. The disease should constitute a public health issue of sufficient severity
2. The disease should be well understood and have early detectable phases when symptoms are not apparent
3. Interventions in the early phase should be effective in preventing or delaying onset of the disease and its complications
4. A safe, reliable and accepted testing procedure exists
Targeted, opportunistic case finding – based on national risk factors for type 2 diabetes and heart disease – where the population to be screened is selected by simple ques-tionnaires, can meet these criteria111,114.
Why detect diabetes early?Diabetes-related complications can be potentially post-poned or avoided through early detection111, assuming appropriate treatment and management and appropri-ate preventive measures. Furthermore, it has been found that people who have a high cardiovascular risk should be treated with a multi-drug regimen and counselling, which reduces the risk of developing heart attacks, strokes and kidney disease105.
Early intervention can be effective and, even if the inter-vention is stopped after some years, the patient may ben-efit from fewer complications in the long term because of the early lifestyle changes and early intensive treatments25.
Cost-effectiveness of early detectionIdeally, policy decisions should be made on the basis of strong, long-term clinical evidence115. However, for early detection and health-check programmes, this is unlikelyto occur116 due to time, cost and ethical considerations.In the absence of this information, modelling futureoutcomes becomes relevant115. Recent modelled results oftype 2 diabetes health-check programmes have indicatedcost-effectiveness in given settings117. Other earlydetection interventions, including providing aspirin to peo-ple with a heart attack and controlling blood glucoselevels in people with diabetes, have also been identifiedas cost-effective, often being inexpensive and feasible toimplement105.

36

37
12. PATIENT SElF-MANAGEMENT, EDUCATION AND SUPPORTMulti-disciplinary strategies that help motivate, educate and supportpeople to manage their condition are an essential part of chronic care.
Effective self-management cannot be assumedA large proportion of people with diabetes and other chronic conditions have difficulties following their pre-scribed treatment and as a result do not achieve optimal treatment outcomes118,119; less than 50% of people with diabetes have satisfactory blood glucose, cholesterol and blood pressure control81,83,84. Many factors play a role in influencing self-management in chronic illness and multi-disciplinary strategies are needed at national and local levels118.
In diabetes, and other self-managed chronic conditions, it is the person with the condition and their family mem-bers, rather than the healthcare team, who are ultimately responsible for managing daily treatment. lack of confi-dence in managing the disease and the effectiveness of treatment are some of the factors playing a key role in diabetes self-management120.
Other factors include the complexity and lack of under-standing of treatments and dosing, especially for patients receiving multiple medications for different conditions118. In type 2 diabetes, psychological barriers to initiation or in-tensification of treatment among patients and healthcare professionals also contribute to delays in initiating required medical therapy121.
Without the patient involved, treat-ment will be less effectiveDiabetes treatment guidelines also highlight the central role of education and self-management issues for the management of diabetes122. National policies and pro-grammes for the prevention and management of chronic illnesses, such as diabetes, depend on an in-depth under-standing of the social, psychological and behavioural as-pects of the condition and its treatment. Multi-disciplinary strategies that help motivate, educate and support people to manage their condition are an essential part of chronic care.
The World Health Organisation’s (WHO’s) innovative framework for care of chronic conditions123 calls for chron-ic care policies to focus efforts on the activated patient and enable effective roles for the family and the com-
munity in healthcare systems. The International Alliance of Patient Organisations’ (IAPO’s) declaration on patient-centred healthcare124 highlights the need for involvement of patients in all phases of healthcare change.
Better adherence to diabetes treatment is associated with better management and lower healthcare utilisation125
and the evidence on the effectiveness of self-management support is growing126-127.
A model for patient-centred carelittle research on the status of provision of quality assured and evidence-based diabetes self-management education is available from Thailand, an area for special focus and attention in the future.
The figure below summarises the key areas that have been shown in large studies to influence a patient’s ability to self-manage and achieve a good quality of life with diabetes. Future health policy frameworks should encour-age better practices and evidence-based strategies for addressing all of these dimensions in an evidence-based and cost-effective way.
With less than 50% of people with diabetes achieving sat-isfactory control of blood glucose, cholesterol and blood pressure, there is a need to strengthen healthcare systems and to ensure patient-centred care across various levels ofhealthcare4.

38
13. TREATMENT TOWARDS TARGETEffective treatment after diagnosis can help to extend and improve the lives of millions - and produce long-term cost-savings at the same time.
ScenariosIn recent years much evidence has shown that enhancedtreatment improves the long-term prospects of the person with diabetes7,25. Computer simulation models can help to clarify the impact of enhanced treatment on benefits and costs. The CORE Diabetes Model is well validated128 and allows a calculation of long-term outcomes, based on the best data available from published trials. Diabetes man-agement strategies can thus be compared in different pa-tient populations in a variety of realistic clinical settings129.
BaselineAccording to the data collected in the UKPDS25 the aver-age person with diabetes - diagnosed at age 52 - can ex-pext to develop minor complications after 8-10 years and after 14-16 years the first major complications. Amongst these complications, 1 in 5 people will develop severe vi-sion loss and 15% will suffer from endstage renal disease.
Enhanced treatmentWith enhanced treatment aimed at HbA1c <7.0%21 both minor and major complications can be delayed by 2-4 years compared to baseline and life expectancy is ex-tended by 2 years with strong effects on life quality. The number of people with endstage renal disease will be 60% lower compared to baseline130.
Early diagnosisEarly diagnosis and effective intervention will further delay the onset of minor and major complications with fewer
than half the people suffering from severe vision loss com-pared to the baseline scenario. life expectancy is extended by 1 more year130.
Economic cost of diabetesThe CORE Diabetes Model can also be used to calculate the direct economic costs of diabetes, including the cost of medication, management and complications. Analysis in a UK setting shows that more effective treatment at an earlier stage will increase the early costs, in particular that of medication, but costs will be reduced in the longer term by delaying or preventing the expensive hospital treatment needed for a wide range of complications such as end-stage renal disease and diabetic retinopathy130.

39
14. MEASURE, SHARE, IMPROvEBy effectively measuring and sharing data – utilising the potential of healthinformatics – the lives of people with diabetes can be improved.
The power of measuring and shar-ing dataCare for chronic diseases, including diabetes, cannot be improved until there is a solid understanding of the level of care today. Only when outcomes are consistently and continually measured and compared can strategies, treatment methods and healthcare systems be improved. Collection of indicators of healthcare and outcomes and analysis based on income level, age, sex and ethnicity is necessary to allow policymakers to adequately assess the effects of interventions and allocation of healthcare budg-ets and ensure progress towards equality89,111. By measur-ing and sharing data – utilising the potential of health informatics – the lives of people with diabetes, and other chronic diseases can be improved.
Measuring and sharing quality–of-care data increase knowledge which can lead to improved care for people with chronic diseases such as diabetes. It can also contrib-ute to better awareness and understanding of a disease and relevant treatment practices. There are many ways to measure quality of care of people with chronic diseases; for example, monitoring potentially preventable hospital admissions is a good indicator of the quality of diabetes primary care131.
Several countries in Europe collect data on diabetes in a national diabetes registry132,133. A diabetes registry that captures information on quality of care offers great potential for continuous monitoring and improvement134.
However, collecting information on risk factors such as tobacco use, unhealthy diet, lack of physical activity and alcohol consumption is also necessary89.
In Thailand, there is no national diabetes registry continu-ously monitoring diabetes control and quality of care. Two separate initiatives with a relatively large sample size give some insight in the development over time, the National Healthy Examination Surveys (conducted in 1991, 1997, 2004 and 2005) and the DiabCare Study series (conducted in 1998, 2001, 2003 and 2008). More than 10 stud-ies have been identified providing insight in control and quality of care at one time-point for a single hospital or province. There is no systematic way in which these data are collected and shared to discuss good practices.
Changing Diabetes® Barometer135
A constructive model to share solutions and raise aware-ness of problems in the control of diabetes and quality of care is provided by the Changing Diabetes Barometer. Its three cornerstones are Measure, Share and Improve. The Barometer aims to illustrate the link between the quality of diabetes care provided, reduction in complications and socio-economic costs, thus providing all stakeholders with the opportunity to make informed choices.
The Barometer’s doctrine is that ‘only when outcomes are measured and shared can improvements be made’, inspiring stakeholders to adopt and follow good practice examples.

40
15. CONClUSION: DIABETES AFFECTS THAIlAND... AT EvERy lEvEl...
...the person with diabetes
It is the person with diabetes that feels the impact of a diagnosis most directly. The realisation that life expectancy is shortened by 6-8 years18,134, that lifelong medication is required and that lifestyle adjustments have to be made often hits hard.
People with diabetes worry about the possibility of long-term complications but also about hypoglycaemia and how their diabetes may impact work and family income59. Having diabetes is associated with a significantly higher risk of developing depression and other psychological problems compared with the general population52,53.
Although Thailand has nationally organised healthcare that includes coverage for essential medicine and hospitalisation, these direct costs are only part of the total cost of illness with the patient and familes having to shoulder the cost of informal care, travel, work absence and disability58.
...family and carers
Treatment for all aspects of chronic diseases such as diabe-tes may not be accessible, available or affordable, and the life-long burden of treatment and management costs can push families into poverty89. The social and emotional im-pact on a family dealing with diabetes is often greater than the direct costs of treatment and lost income alone.
Furthermore, as older and socially disadvantaged groups of-ten have multiple chronic diseases and risk factors, effectivetreatment often demands numerous medications89,118 andthe elderly are the greatest consumers of prescriptiondrugs89. For this reason, adherence to long-term therapycan be a challenge118. Stigma and discrimination also playa role, and certain chronic diseases such as diabetes candiminish employment opportunities111. This compoundsthe interrelationship between poverty and ill health89.
Diabetes has been shown to have a substantial negative impact on family relationships and social life, leading to a reduction in health-related quality of life137. The availability of social support plays a crucial role in people with diabetes being able to adhere to treatment and manage their condi-tion successfully118.
...employers and the national econ-omy
Dying young or living with long-term illness or disabilityhas economic implications for families and society and thecost to employers and national economies is increasing.
Poor health of employees causes productivity losses due to lost working time through absenteeism, sub-optimal performance due to physical and psychological problems, sickness, early retirement and premature death.
Research on the economic impact of diabetes and other chronic diseases is still in its early stages globally and information from Thailand is scarce. The morbidity and premature mortality rates attributable to chronic diseases highlight effective interventions for chronic disease that could bring significant health and economic gain to many countries including Thailand.

41

42
16. SHARING ExPERIENCESThere are already many successful programmes in and around Asia that are tackling diabetes in innovative and effective ways. Sharing information and ideas about ‘what works’ is one of the most positive options for the future.
Thailand: retinopathy screeningRetinopathy is one of the most common long-term com-plications of diabetes and early detection and treatment can help to slow progression and prevent blindness.
Two mobile eye units equipped with digital camera and laser therapy machine were built supported by a donation from the World Diabetes Foundation and a charity donation from the Royal Danish Embassy in Thailand in 2009. The mobile clinics work under grant support from the National Health Security Office and the Ministry of Public Health in coopera-tion with the Royal College of Ophthal-mologists and Diabetes Association of Thailand.
Two years of Service in 43 provinces, fundoscopic pictures were taken in 822,573 patients and diabetic retinopathy was detected in 101,783 cases (12.4%). laser therapy was performed in 14,493 eyes138.
Italy: measuring and sharing quality of care dataThe Italian Association of Diabetologists (AMD) realised the importance of measuring and sharing quality-of-care data to reduce the burden of diabetes. For this reason it began collecting diabetes quality indicators from all diabe-tes outpatient clinics in 2004.
The initiative now involves 250 diabetes clinics throughout Italy, covering a total of over 400,000 people with type 1 or type 2 diabetes. The quality-of-care data collected are compared with re-alistic gold standards established by identifying the best centres operating in the same healthcare
system under similar conditions. This approach represents a key feature of the continuous quality-improvement ef-fort implemented in Italy.
Results are then publicised through a specific publication(AMD Annals) and on a dedicated page of the AMD
website, and discussed with investigators at an annualmeeting. The project is conducted without allocationof extra resources or financial incentives, but through aphysician-led effort made possible by the commitment ofthe specialists involved.
The participation of clinicians in the AMD Annalsinitiative has already proven effective in improvingprocess and intermediate outcomes indicators.
Israel: continuous improvement of a chronic care modelSince 1997, a diabetes programme has been in place in Israel run by one of the major health insurers, Clalit Health Services. It includes adaptation of clinical guide-lines, continuous medical education, improved national electronic health records and software to support health-care professionals making clinical decisions. The scheme provides a way of ensuring that patient information can be consistently accessed and tracked, and is incorporated in the electronic medical file of each patient, thus requir-ing minimal training to use.
The system helps to facilitate preventive care, and faster and more accurate detection. It has also been found to increase the time that healthcare professionals can spend with patients, and reduces costs by reducing du-plicate testing and unnecessary procedures. Currently, it covers 100% of the population of Clalit Health Services. In recent years, all of the other health maintenance organisations in Israel have adopted a similar solution to combat diabetes, and they all work together
under the auspices of the Israeli Diabetes Barometer.
Building primarily on the quality indicators in this diabetes programme, a National Programme for Quality Indicators for Health was established in 2004. To date, the pro-gramme has had positive results, with the proportion of people with diabetes receiving the necessary blood tests increasing four-fold. Furthermore, improvements in the proportion of people with diabetes adequately control-ling their cholesterol and blood glucose levels have been observed: the proportion of people with diabetes in good control rose from 28% in 1999 to 53% in 2007.

43
Clalit is Israel’s largest health maintenance organisation,covering about 70% of all people with diabetes in Israel.With government support, it initiated the registry in 1996, and now has an extensive collection of diabetes quality indicators. The registry has been accompaniedby a range of workshops and activities with the aim of improving diabetes care.
UK: structured diabetes self-man-agement education (DESMOND)A recent study involving 824 adult patients from 207 gen-eral practices in the UK found that people who received a group-based, patient-centred structured diabetes self-management education course had greater improvements in weight loss and smoking cessation compared with people who did not. The education programme, Diabe-tes Education and Self-Management for On-going and Newly Diagnosed (DESMOND), was carried out by the UK National Health Service.
DESMOND is a structured patient education and management pro-gramme designed for newly diagnosed people with type 2 diabetes. It aims to support people in identifying health risks and developing personalised goals while also providing emotional and social support. This study also evaluated the cost-effectiveness of the DESMOND programme, and conclud-ed that it is likely to be cost-effective
compared with usual care for people with type 2 diabetes.
The programme fulfils the National Institute for Health and Clinical Excellence national guidelines and quality criteria for education, and is available through a quality assured process on a national basis. The education model has been adapted in the Netherlands and, more recently, in Austral-ia, and provides inspiration for potential wider use.
Saudi Arabia: better diabetes care through specialised diabetes centersIn response to the high prevalence rates of diabetes in the region, the Ministry of Health in Saudi Arabia developed and supported a plan to establish more specialised diabe-tes centres in the different parts of the Kingdom. These centres provide education, training, and treatment and management plans for people with diabetes.
As diabetic foot complications are a leading cause of lower-limb amputation, some of these centres were given specific responsibility for increasing awareness among
healthcare providers and people with diabetes of dia-betic foot care and the prevention of complications. The preliminary results from these centres suggest that the programme has been successful in increasing awareness and decreasing the rate of amputation. Furthermore, the success of these programmes have been effective in all lo-cations, with satisfactory results being achieved in tertiary care facilities as well as remote hospitals affiliated to the Ministry of Health.
Thailand: holistic diabetes careMost healthcare systems today are organised to treat the acute symptoms of disease and manage conditions sepa-rately. Diabetes is a complicated chronic disease and ef-fective management requires a multi-disciplinary approach addressing glucose management, lifestyle modification, management of complications and not in the least patient education. An integrated patient-centred approach will capitalise on common treatment needs and is thus set to have a greater impact.
Trained in the United States, Professor Thep Himathongkam returned to Thai-land to find the implementation of a ho-listic team-based model of diabetes care such as he had observed in the world-famous Joslin Diabetes Center in Boston, USA, very challenging. In 1985 Dr Thep established the Theptarin Diabetes and Thyroid Center with the goal to create a model for holistic treatment of diabetes in Thailand. The model emphasised the empowerment of people with diabetes to care for themselves and the integrat-
ed diabetes care team comprised of an endocrinologist, a diabetes nurse educator and a dietitian.
The facility was modest at first, with only eight beds, and struggled to attract medical professionals and patients, but as awareness of diabetes increased, patient demand grew and the center gained increasing recognition and started to expand its size and services. The hospital be-came the first in Thailand to offer a specialised diabetic foot clinic for wound care and prevention and opened a ‘lifestyle Building’ to promote the prevention of diabetes and related chronic diseases.
Although a private hospital, it is unusual in its commit-ment to public education and professional capacity build-ing and has successfully sought partnerships with donors and corporations to fund these activities. The World Diabetes Foundation has funded several of its programmes and it partners with multinational companies to help its employees keep healthy.

44
17. ABOUT NOvO NORDISKNovo Nordisk is a global healthcare company with 90 years of innovation and leadership in diabetes care.
Novo Nordisk in shortNovo Nordisk is a global healthcare company with 90 years of innovation and leadership in diabetes care. In 1923, our Danish founders began a journey to change diabetes. Today, we are thousands of employees across the world with the passion, the skills and the commitment to continue this journey to prevent, treat and ultimately cure diabetes. The company also has leading positions within haemophilia care, growth hormone therapy and hormone replacement therapy. Headquartered in Denmark, Novo Nordisk employs approximately 35,000 employees in 75 countries, and markets its products in more than 180 countries.
Building on the past - looking to the futureTwo small Danish companies, Nordisk (1923) and Novo (1925), started production of the revolutionary new drug insulin that had just been discovered by Canadian scien-tists. Competing intensely with one another, the compa-nies developed into two of the best in their field responsi-ble for many innovations, such as the breakthrough insulin NPH (Neutral Protamine Hagedorn) introduced in 1950 and the world’s first insulin injection device launched in 1985.
Still in the early days of their existence, both Novo and Nordisk established their own hospitals to offer better treatment and provide outlook on a normal life for people with diabetes. The hospitals were combined in 1992 to form the Steno Diabetes Centre, an internationally recog-nised centre of excellence in diabetes treatment, educa-tion and translational research.
The companies merged in 1989, creating Novo Nordisk, one of the world’s largest biotechnology groups and a group that has been expanding rapidly ever since. Today, the Novo Nordisk Way shows responsibility to patients, employees, communities and investors. We will in the future continue to build on the legacy left by the found-ers of Novo Nordisk and do whatever it takes to change diabetes. Our history tells us it can be done.
Changing diabetes®
Changing diabetes® is a commitment to answer theneeds of people with diabetes in every decision andaction. This means delivering targeted treatments based
on a deep understanding of individual needs, and doingso with financial, social and environmental responsibility.
But treatment is only part of the solution to the diabetes challenge. This is why we advocate for concerted action to address the pandemic, challenging systems, political priorities and health expectations worldwide. In addition, we collaborate with global organisations and governments in driving diabetes awareness, prevention and equal access to care.
Through our actions we will break the curve of the dia-betes pandemic, and we will measure and report on our progress. Until we defeat diabetes, we will continue to support people in living fuller, healthier and more produc-tive lives.
World Diabetes FoundationThe World Diabetes Foundation (WDF) is dedicated to cre-ate awareness, care and relief to people with diabetes in the developing world. At its heart lies the promise of equal access to diabetes care.
The WDF was launched as an independent, non-profit organisation through a grant from Novo Nordisk, and tries to help where it will count the most - in developing countries where 80% of the world’s explosion in diabetes is expected to occur.
Since 2001, the WDF has supported several projects in Thailand with 2 examples described in chapter 16 of this booklet, for more information on the WDF please visit www.worlddiabetesfoundation.org.

45
18. DIABETES GlOSSARyAcute = describes something that happens suddenly Albuminuria = condition in which the urine has more than
normal amounts of albumin (a protein), this may be a sign of nephropathy (kidney disease)
Antibodies = proteins made by the body to protect itself from “foreign” substances such as bacteria or viruses. Type 1 diabetes is caused by antibodies destroying the beta cells that make insulin
Artery = large blood vessel that carries blood with oxygen from the heart to all parts of the body
Atherosclerosis = clogging, narrowing and hardening of large and medium-sized blood vessels, this may lead to stroke, heart attack, eye and kidney problems
Autoimmune disease = disorder of the immune system, when body tissue is mistakenly attacked and destroyed by antibodies produced
Beta cell = cells in the pancreas that make insulin Blood glucose = main sugar (energy) found in the bloodBlood glucose level = amount of glucose in blood, ex-
pressed as mmol/lBlood glucose monitoring = checking blood glucose level
on a regular basis in order to manage diabetes, a blood glucose meter and glucose test strips are needed
Blood pressure = the force of blood exerted on the inside walls of blood vessels, expressed as a ratio, for example: 120/80, read as “120 over 80”
Blood vessels = tubes that carry blood to and from all parts of the body (arteries, veins and capillaries)
Body mass index (BMI) = measure to evaluate body weight relative to a person’s height, expressed as kg/m2. Scores indicate underweight (<18.5), normal weight (18.5 - 25), overweight (25 - 30) or obese (>30)
Capillary = the smallest type of blood vessel. Carries oxy-gen and glucose to the cells and waste products pass back from the cells into the blood
Cardiovascular disease (CvD) = disease of the heart and blood vessels (arteries, veins and capillaries)
Cataract = clouding of the lens of the eyeCholesterol = a type of fat used by the body to make
hormones and build cell walls, too much lDl (“bad”) cholesterol is harmful
Chronic = describes something that is long-lastingComa = a sleep-like state in which a person is not con-
scious, in diabetes may be caused by very high or very low blood glucose
Complications = harmful effects of diabetes Coronary heart (or artery) disease (CHD, CAD) = heart
disease caused by narrowing of the arteries that sup-ply blood to the heart, when blood supply is cut off it results in a heart attack
Diabetes mellitus = chronic disease that occurs when insulin is no longer produced or when the body cannot make good use of the insulin it produces
Diagnosis = the determination of a disease from its signs and symptoms
Dialysis = the process of cleaning wastes from the blood artificially, this is normally done by the kidneys, if kid-neys fail blood must be cleaned artificially
Dyslipidaemia = higher than normal fat and cholesterol levels in the blood, contributes to cardiovascular disease
Epidemic = widespread occurrence of a diseaseEpidemiology = branch of medicine dealing with the inci-
dence, distribution, and possible control of diseases and other factors relating to health
Fasting plasma or blood glucose (FPG / FBG) = blood glucose level after overnight fasting, used to diagnose (pre-) diabetes and tool to monitor glucose control in people with diabetes
Fat = 1. one of the three main nutrients in food, found in butter, oil, nuts, meat and some dairy products, 2. in the body excess calories are stored as body fat
Gestational diabetes mellitus = a type of diabetes that develops during pregnancy and usually disappears upon delivery, increases the risk of diabetes later in life
Glaucoma = an increase in fluid pressure inside the eye that may lead to loss of vision
Glucose = one of the simplest forms of sugar
HbA1c = test that measures average blood glucose levels over the past 2 to 3 months
Hormone = chemical produced in one part of the body and released into the blood to trigger or regulate par-ticular body functions, insulin is a hormone triggering uptake of glucose from the blood into cells
Hyperglycemia = excessive blood glucose, measured after fasting or after a meal (postprandial)
Hypertension = high blood pressure, condition when blood flows through the blood vessels with greater force than normal, increases risk of heart attack, stroke, kidney problems and death
Hypoglycemia = occurs when blood glucose is lower than normal and if left untreated may lead to unconscious-ness, coma and even death, warning signs include hunger, shakiness, perspiration, dizziness and confusion
Impaired fasting glucose (IFG) = condition where level of glucose is higher than normal but not high enough for a diagnosis of diabetes
Impaired glucose tolerance (IGT) = condition where level of glucose is higher than normal but not high enough for a diagnosis of diabetes
Incidence = measure of how often a disease occurs; the number of new cases of a disease among a certain group of people for a certain period of time
Insulin = a hormone functioning as a key, opening cells for the uptake of glucose from the blood for energy
Insulin analogues (or modern insulin) = modified insulin molecule with desirable properties, resulting in very fast or long action to allow better glucose control, a lower risk of hypoglycaemia or more convenient use
Insulin resistance = the body’s inability to respond to and use the insulin it produces, often caused by obesity
Intensive therapy = treatment for diabetes in which blood glucose is kept as close to normal as possible, involves frequent insulin injections and self-monitoring of blood glucose, frequent adjustment of dose and type of medi-

46
cation, meal planning and lifestyle intervention
Kidney failure = chronic condition when the kidneys no longer work, dialysis or kidney transplantation is re-quired to survive
Kidneys = the two bean-shaped organs that filter wastes from the blood and form urine
lipid = a term for fat in the bodylipid profile = blood test that measures total cholesterol,
triglycerides, and HDl cholesterol. lDl (“bad”) choles-terol is then calculated from the results, one measure of the risk of cardiovascular disease
Macrovascular disease = disease of the large blood vessels, such as those found in the heart, caused when lipids and blood clots build up in the large blood vessels, re-sulting in atherosclerosis, coronary heart disease, stroke, and peripheral vascular disease
Metabolic syndrome = tendency of several conditions to occur together, including obesity, insulin resistance, diabetes or pre-diabetes, hypertension and high lipids
Microvascular disease = disease of the small blood vessels, such as those found in the eyes, nerves, and kidneys, occurs when the walls of the vessels become abnor-mally thick but weak, they then bleed, leak protein, and slow the flow of blood to the cells
Mmol/l = millimoles per liter, unit of measure that indi-cates the concentration of a substance in a liter of fluid
Myocardial infarction = an interruption in the blood supply to the heart because of narrowed or blocked blood ves-sels, also called a heart attack
Nephropathy = kidney disease, diabetes can damage the small blood vessels in the kidneys leading to the kidneys becoming less efficient or to fail altogether
Neuropathy = disease of the nervous system, causing pain, numbness or a tingling feeling (mostly) in legs and feet
Non-communicable disease (NCD) = non-infectious medical condition or disease, including heart disease, hypertension, cancer and diabetes, also called lifestyle diseases as many of the risk factors such as smoking, poor diets and lack of excersise can be changed making it possible to prevent many of these diseases
Obesity = a condition in which a greater than normal amount of fat is in the body, more severe than over-weight, when body mass index (BMI) is 30 or more
Oral glucose tolerance test (OGTT) = test to diagnose (pre-) diabetes, a high-glucose beverage is given after an overnight fast, blood samples at 2 to 3 hour intervals are compared with a standard to show how the body uses glucose over time
Oral hypoglycemic agents (OHA) or oral anti-diabetics (OAD) = medicines taken by mouth to reduce blood glucose levels
Overweight = an above-normal body weight, when body mass index (BMI) is between 25 and 30
Pancreas = organ that makes insulin and enzymes for digestion, located behind the lower part of the stomach and about the size of a hand
Peripheral vascular or arterical disease (PvD / PAD) = disease of the large blood vessels of the arms, legs, and
feet; occurs when major blood vessels are blocked and do not receive enough blood; symptoms include aching pains and slow-healing foot sores
Plasma = fluid part of bloodPolydipsia = excessive thirst; may be a sign of diabetesPolyphagia = excessive hunger; may be a sign of diabetesPolyuria = excessive urination; may be a sign of diabetesPostprandial blood glucose (PPG) = the blood glucose level
1 to 2 hours after a mealPre-diabetes = a condition in which blood glucose levels
are higher than normal but are not high enough for a diagnosis of diabetes, indicates increased risk for devel-oping diabetes and for heart disease and stroke
Prevalence = the number of people in a given group or population who are reported to have a disease
Protein = 1. nutrient in food such as meat, fish, milk, eggs, and dried beans; 2. building block for cell structure, hormones such as insulin, and other functions
Proteinuria = the presence of protein in the urine; indicat-ing that the kidneys are not working properly
Renal = having to do with the kidneysRenal failure = chronic condition when the kidneys no
longer work, dialysis or kidney transplantation is re-quired to survive
Retinopathy = eye disease caused by damage to the small blood vessels in the retina; loss of vision may result
Risk factor = anything that raises the chances of a person developing a disease
Side effects = unintended action(s) of a drugStroke = condition caused by damage to blood vessels in
the brain; may cause loss of ability to speak or to move parts of the body
Sugar = 1. a class of carbohydrates with a sweet taste, including glucose, fructose and sucrose; 2. a term used to refer to blood glucose.
Symptoms = physical or mental sign indicating a disease or medical condition
Type 1 diabetes = condition characterized by high blood glucose levels caused by a total lack of insulin; occurs when the body’s immune system attacks and destroys the insulin-producing beta cells in the pancreas; usually develops in young people but can appear in adults
Type 2 diabetes = condition characterized by high blood glucose levels caused by either a lack of insulin or the body’s inability to use insulin efficiently; develops most often in middle-aged and older adults but can appear in young people in particular in combination with obesity
Ulcer = a deep open sore or break in the skin
vascular = relating to the body’s blood vesselsvein = a blood vessel that carries blood to the heart
Waist circumference = measure of the waist to evaluate bodyweight and risk of obesity related health problems
Wound care = steps taken to ensure that a wound heals correctly; in diabetes wounds heal less rapidly and get more easily infected which may lead to amputation

47
19. REFERENCESWe thank all authors, researchers and reviewers that have provided the necessary knowledge and insight to make this project possible.1. The Health and Social Care Information Centre, National Diabetes
Audit 2010-2011 Report 2: Complications and Mortality, 2012; leeds, UK
2. Hex, N. et al., Diabetic Medicine, 2012; 29: 855-862: Estimating the current and future costs of Type 1 and Type 2 diabetes in the UK, in-cluding direct health costs and indirect societal and productivity costs
3. International Diabetes Federation, IDF Diabetes Atlas, 6th edition, 2013; accessed 19 November 2013; http://www.idf.org/diabetesatlas
4. Beaglehole, R. et al. for The lancet NCD Action Group and the NCD Alliance, Lancet, 2011; 377: 1438-1447: Priority actions for the non-communicable disease crisis
5. World Health Organisation, Global Health Observatory, accessed 7 May 2013; http://www.who.int/gho/countries/tha.pdf
6. Prasartkul, P. et al., in: Thai Health 2012, Institute for Population and Social Research, 2012; Mahidol University, Thailand: Morbidity and Mortality
7. Gaede, P. et al., New England Journal of Medicine, 2003; 348: 383-393: Multifactorial intervention and cardiovascular disease in patients with type 2 diabetes
8. International Diabetes Federation, About Diabetes, accessed 7 May 2013; www.idf.org/about-diabetes
9. American Diabetes Association, living with Diabetes, accessed 15 June 2013; www.diabetes.org/living-with-diabetes
10. Fowler, M.J., Clinical Diabetes, 2010; 28 (1): 42-46: Diabetes Founda-tion, Diabetes: Magnitude and Mechanisms
11. D’Adamo E. et al., Diabetes Care, 34 (Suppl.2): S161-165: Type 2 Diabetes in youth: Epidemiology and Pathophysiology
12. Sacks D.A. et al., Diabetes Care, 2012; 35: 526-528: Frequency of Gestational Diabetes Mellitus at Collaborating Centers Based on IADPSG Consensus Panel-Recommended Criteria
13. Stenstrom G. et al., Diabetes, 2005; 54 (Suppl.2): S68-72: latent Autoimmune Diabetes in Adults; Definition, Prevalence, B-cell Func-tion and Treatment
14. American Diabetes Association, Diabetes Basics, accessed 04 July 2013; www.diabetes.org/diabetes-basics
15. yau J.W.y. et al., Diabetes Care, 2012; 35: 556-564: Global preva-lence and major risk factors of diabetic retinopathy
16. Centers for Disease Control and Prevention, National Diabetes Fact Sheet, 2011; www.cdc.gov/diabetes/pubs/factsheet11.htm
17. International Diabetes Federation, Complications of Diabetes, ac-cessed 4 July 2013; www.diabetes.org/complications-diabetes
18. The Emerging Risk Factors Collaboration, N Engl J Med, 2012; 364: 829-841: Diabetes Mellitus, Fasting Glucose, and Risk of Cause-Specific Death
19. Fowler M.J., Clinical Diabetes, 2010; 28 (3): 132-136: Diabetes Foun-dation, Diabetes Treatment: Oral Agents
20. Khoury J.C. et al., Stroke, 2013; 44: 1500-1504: Diabetes mellitus: a risk factor for ischemic stroke in a large bi-racial population
21. Inzucchi S.E. et al., Diabetes Care, 2012; 35: 1364-1379: Manage-ment of Hyperglycemia in Type 2 Diabetes: A Patient-Centered Ap-proach - Position Statement of the ADA and the EASD
22. Fowler M.J., Clinical Diabetes, 2011; 29 (1): 36-39: Diabetes Founda-tion, The Diabetes Treatment Trap: Hypoglycaemia
23. Seaquist E.R. et al., Diabetes Care, 2013; 36: 1384-1395: Hypogly-caemia and Diabetes: A Report of a Workgroup of the American Diabetes Association and The Endocrine Society
24. UK Prospective Diabetes Study (UKPDS) Group, Lancet, 1998; 352: 837-853: Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complica-tions in patients with type 2 diabetes (UKPDS 33)
25. Holman R.R. et al., N Engl J Med, 2008; 359: 1577-1589: 10-year follow-up of intensive glucose control in type 2 diabetes
26. Stratton I.M. et al., BMJ, 2000; 321: 405-412: Association of glycae-mia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study
27. Abdullah A. et al., Diab Res Clin Pract, 2010; 89 (3): 309-319: The magnitude of association between overweight and obesity and the risk of diabetes: a meta-analysis of prospective cohort studies
28. Aekplakorn W. et al., Obesity Reviews, 2009; 10: 589-592: Preva-lence of obesity in Thailand
29. Aekplakorn W., Presentation on National Health Examination Survey, Thailand, www.pmaconference.mahidol.ac.th/index.php?/option=com_docman&task=doc_download&gid=226&Itemid=.
30. Aekplakorn W., Asia-Pacific J Public Health, 2010; 23 (3): 298-306: Prevalence, treatment, and control of metabolic risk factors by BMI status in Thai adults: National Health Examination Survey III
31. likitmaskul S. et al., J Pediatric End & Metab, 2003; 16: 71-77: Increasing prevalence of type 2 diabetes mellitus in Thai children and adolescents associated with increasing prevalence of obesity
32. Aekplakorn W., Diabetes Care, 2007; 30 (8): 2007-2012: Prevalence and management of diabetes and associated risk factors by regions of Thailand, Third National Health Examination Survey 2004
33. Bureau of Policy and Strategy, Ministry of Public Health, Thailand Health Profile Report 2008-2010, www.eng.moph.go.th/index.php/health-situation-trend
34. Aekplakorn W. et al., Diabetes Care, 2003; 26 (10): 2758-2763: The prevalence and management of diabetes in Thai adults, The Interna-tional Collaborative Study of Cardiovascular Disease in Asia
35. Porapakkham y. et al., Population Health Metrics, 2010; 8 (14): 191-198: Estimated causes of death in Thailand, 2005: implications for healthy policy
36. Rawdaree P. et al., J Med Ass Thailand, 2006; 89 (Suppl. 1): S1-9: Thailand Diabetes Registry (TDR) Project: Clinical status and long-term vascular complications in diabetic patients
37. leelawattana R. et al., J Med Ass Thailand, 2006; 89 (Suppl. 1): S54-59: Thailand Diabetes Registry Project: Prevalence of vascular complications in long-standing type 2 diabetes
38. American Diabetes Association, Complications, accessed 09 July 2013; www.diabetes.org/living-with-diabetes/complications
39. Aekplakorn W. et al., Diab Res Clin Pract, 2009; 84: 92-98: Microal-buminuria and metabolic risk factors in patients with type 2 diabetes in primary care setting in Thailand
40. Ngarmukos C. et al., J Med Ass Thailand, 2006; 89 (Suppl. 1): S37-42: Thailand Diabetes Registry Project:
41. Unpublished, Novo Nordisk data on file, DiabCare 2008 study results42. Praditpornsilpa K (editor), Thailand Renal Replacement Therapy
year 2009, Nephrology Society of Thailand: www.nephrothai.org/nephrothai_boffice/images_upload/news/255/files/thailand_renal-replacement_therapy_2009-reduce.pdf
43. Chetthakul T. et al., J Med Ass Thailand, 2006; 89 (Suppl. 1): S27-36: Thailand Diabetes Registry Project: Prevalence of diabetic retinopathy and associated risk factors in type 2 diabetes mellitus
44. Supapluksakul S. et al., J Med Ass Thailand, 2008; 91 (5): 716-722: The prevalence of diabetic retinopathy in Trang province determined by retinal photography and comprehensive eye examination
45. Silpa-archa S. et al., J Med Ass Thailand, 2012; 95 (Suppl. 4): S43-S49: Prevalence and associated risk factors of diabetic retinopathy in Chandrubeksa Hospital, directorate of medical services, Royal Thai Air Force
46. Jenchitr W. et al., J Med Ass Thailand, 2004; 87 (11): 1321-1326: Prevalence of diabetic retinopathy in relation to duration of diabetes mellitus in community hospitals of lampang
47. Gregg E.W. et al., Ann Intern Med, 2007; 147: 149-155: Mortality trends in men and women with diabetes, 1971 to 2000
48. Campbell P.T. et al., Diabetes Care, 2012; 35: 1835-1844: Diabetes and cause-specific mortality in a prospective cohort of one million US adults
49. Pratipanawatr T. et al., J Med Ass Thailand, 2010; 93 (Suppl. 3): S12-20: Thailand Diabetes Registry Cohort: predicting death in Thai diabetic patients and causes of death
50. Franco O.H. et al., Arch Intern Med, 2007; 167: 1145-1151: Associa-tions of diabetes mellitus with total life expectancy and life expec-tancy with and without cardiovascular disease
51. Chuengsamarn S. et al., J Med Ass Thailand, 2010; 93 (Suppl. 2): S32-38: Prevalence and risk factors of peripheral arterial disease in type 2 diabetic patients at HRH Princess Maha Chakri Sirindhorn Medical Center
52. Thaneerat T. et al., Asian Biomedicine, 2009; 3 (4): 383-390: Preva-lence of depression, hemoglobin A1c level, and associated factors in outpatients with type 2 diabetes

48
53. Egede E. et al., Diabetes Care, 2002; 25 (3): 464-470: Comborbid depression is associated with increased health care use and expendi-ture in individuals with diabetes
54. World Health Organisation, Fact sheet no. 236, accessed 21 July 2013; http://www.who.int/mediacentre/factsheets/fs236/en/#
55. Zhang P. et al., Diab Res Clin Pract, 2010; 87: 293-301: Diabetes Atlas: Global healthcare expenditure on diabetes for 2010 and 2030
56. American Diabetes Association, Diabetes Care, 2013; 36 (4): 1033-1046: Economic cost of diabetes in the U.S. in 2012
57. Chatterjee S. et al., Health and Social Care in the Community, 2011; doi: 10.1111/j.1365-2524.2010.00981.x: Cost of diabetes and its complications in Thailand: a complete picture of economic burden
58. Riewpaiboon A. et al., Int J Pharmacy Practice, 2011; 19: 342-349: Cost analysis for efficient management: diabetes treatment at a public district hospital in Thailand
59. Pramming S. et al., Diabetic Medicine, 1990; 8: 217-222: Sympto-matic hypoglycaemia in 411 type 1 diabetic patients
60. Brod M. et al., Value in Health, 2011; 14 (5): 665-671: The impact of non-severe hypoglycemic events on work productivity and diabetes management
61. leese G.P. et al., Diabetes Care, 2003; 26 (4): 1176-1180: Frequency of severe hypoglycemia requiring emergency treatment in type 1 and type 2 diabetes
62. Sanchai T. et al., J Med Assoc Thai, 2011; 94 (12): 1435-1440: Severe hypoglycemia in type II diabetes at Nakornping General Hospital: a study on clinical risk factors
63. Wilber J.A. et al., Am J Med, 1972; 52: 653-663: Hypertension - a community problem
64. International Diabetes Federation, IDF Diabetes Atlas, 5th edition, 2011; www.idf.org/diabetesatlas/5e/mortality, accessed on 21 July 2013
65. Spijkerman A.M.W. et al., Diabetes Care, 2003; 26 (9): 2604-2608: Microvascular complications at time of diagnosis of type 2 diabetes are similar among diabetic patients detected by targeted screening and patients newly diagnosed in general practice
66. Plantinga l.C. et al., Clin J Am Soc Nephrol, 2010; 5: 673-682: Prevalence of chronic kidney disease in US adults with undiagnosed diabetes or prediabetes
67. United Nations, Sixty-sixth General Assembly, http://www.un.org/News/Press/docs/2011/ga11138.doc.htm, accessed on 20 July 2013
68. Deerochanawong C. et al., Globalization and Health, 2013; 9 (11): 18pp, http://www.globalizationandhealth.com/content/9/1/11: Diabetes management in Thailand: a literature review of the burden, costs, and outcomes
69. International Diabetes Federation, IDF Diabetes Atlas, 5th edi-tion, 2012 update, 2012; http://www.idf.org/diabetesatlas/5e/Up-date2012, IDFAtlas5E_Detailed_Estimates.xls, accessed 21 July 2013
70. Aekplakorn W. et al., Diabetes Care, 2011; 34: 1980-1985: Preva-lence and management of diabetes and metabolic risk factors in Thai adults, The Thai National Health Examination Survey Iv, 2009
71. Tatsanavivat P. et al., J Med Assoc Thai, 2012; 95 (Suppl. 7): S254-S261: Comparative effectiveness of three national healthcare schemes in Thailand: in-hospital medical expenses for diabetes and hypertension in 2010
72. Pratipanawatr T. et al., J Med Assoc Thai, 2010; 93 (Suppl. 3): S12-S20: Thailand Diabetes Registry Cohort: predicting death in Thai diabetic patients and causes of death
73. Koshakri R. et al., Thai J Nurs Rev, 2009; 13 (3): 167-180: Quality of diabetes care in PCUs in Central Thailand
74. Sathira-Angkura T. et al., J Med Assoc Thai, 2011; 94 (12): 1513-1520: Factors associated with the effectiveness of diabetes care at primary care settings
75. Sriwijitkamol A. et al., J Med Assoc Thai, 2011; 94 (Suppl 1): S168-174: Assessment and prevalences of diabetic complications in 722 Thai type 2 diabetes patients
76. Mayurasakorn K. et al., J Med Assoc Thai, 2009; 92 (8): 1094-1101: Glycemic control and microvascular complications among type 2 diabetes at primary care units
77. Aekplakorn W. et al., Diab Res Clin Pract, 2009; 84: 92-98: Microal-buminuria and metabolic risk factors in patients with type 2 diabetes in primary care setting in Thailand
78. Worawongprapa O. et al., J Med Assoc Thai, 2008; 91 (5): 641-647: Glycemic control in diabetes with metabolic syndrome in community hospital
79. Nitiyanant W. et al., Diab Res Clin Pract, 2008; S1-S127: P-41: level of glycemic control and patterns of oral antihyperglycemic therapy among patients with type 2 diabetes mellitus (T2DM) in Thailand
80. DiabCare 2008; Novo Nordisk data on file 81. Kosachunhanun N. et al., J Med Assoc Thai, 2006; 89 (Suppl. 1): S66-
S71: Thailand Diabetes Registry Project: Glycemic control in Thai type
2 diabetes and its relation to hyperglycemic agent usage82. Wongkongkam K. et al., Eur J Cardiov Nursing, 2012; 11 (1): 70-76:
Factors influencing the presence of peripheral arterial disease among Thai patients with type 2 diabetes
83. Bunnag P. et al., J Med Assoc Thai, 2006; 89 (Suppl. 1): S72-S77: Thailand Diabetes Registry Project: Prevalence of hypertension, treat-ment and control of blood pressure in hypertensive adults with type 2 diabetes
84. Pratipanawatr T. et al., J Med Assoc Thai, 2006; 89 (Suppl. 1): S60-S65: Thailand Diabetes Registry Project: current status of dyslipidemia in Thai diabetic patients
85. Huxley R. et al., BMJ, 2006; doi: 10.1136/bmj.38678.389583.7C: Excess risk of fatal coronary heart disease associated with diabetes in men and women: meta-analysis of 37 prospective cohort studies
86. DECODE Study Group, Diabetologia, 2003; 46: 608-617: Gender dif-ference in all-cause and cardiovascular mortality related to hypergly-caemia and newly-diagnosed diabetes
87. Monti M.C. et al., J Clin End Metab, 2007; 92 (12): 4650-4655: Familial risk factors for microvascular complications and differential male-female risk in a large cohort of Amercian families with type 1 diabetes
88. World Diabetes Foundation, Global Alliance for Women’s Health, Int J Gyn Obstet, 2009; 104: S46-S50: Diabetes, women and develop-ment: meeting summary, expet recommendations for policy action, conclusions and follow-up actions
89. World Health Organisation, 2006; Gaining Health: The European strategy for the prevention and control of noncommunicable dis-eases, http://www.euro.who.int/__data/assets/pdf_file/0008/76526/E89306.pdf, accessed on 30 July 2013
90. Bellamy l. et al., Lancet, 2009; 373: 1773-1779: Type 2 diabetes mel-litus after gestational diabetes: a systematic review and meta-analysis
91. Clausen T.D. et al., Diabetes Care, 2008; 31 (2): 340–346: High prevalence of type 2 diabetes and pre-diabetes in adult offspring of women with gestational diabetes mellitus or type 1 diabetes: the role of intrauterine hyperglycemia.
92. Fetita l.S. et al., J Clin End Metab, 2006; 91: 618–624: Consequenc-es of fetal exposure to maternal diabetes in offspring.
93. Deerochanawong C. et al., Diabetologia, 1996; 39 (9): 1070-1073: Comparison of National Diabetes Data Group and World Health Organization criteria for detecting gestational diabetes mellitus
94. Konharn K. et al., Asia Pac J Public Health, 2012; doi: 10.1177/1010539512459946: Differences between weekday and weekend levels of moderate-to-vigorous physical activity in Thai adolescents
95. Ministry of Public Health and Ministry of Social Development and Human Security, Thailand Country Report, 2008; presented at The 6th ASEAN & Japan High Level Officials Meeting on Caring Societies: “Healthy Next Generation”
96. Prasartkul, P. et al., in: Thai Health 2012, Institute for Population and Social Research, 2012; Mahidol University, Thailand: Birth
97. The DIAMOND Project Group, Diabetic Medicine, 2006; 23 (8): 857-866: Incidence and trends of childhood Type 1 diabetes worldwide 1990–1999
98. Tuchinda C. et al., J Med Assoc Thai, 2002; 85 (6): 648-652: The epidemiology of type 1 diabetes in Thai children.
99. Panamonta O. et al., J Med Assoc Thai, 2011; 94 (12): 1447-1450: The rising incidence of type 1 diabetes in the northeastern part of Thailand.
100. Patarakujvanich N. et al., J Med Assoc Thai, 2001; 84 (8): 1071-1074: Incidence of diabetes mellitus type 1 in children of southern Thailand.
101. Park y., Annals of the New York Academy of Sciences, 2006; 1079 (1): 31-40: Why Is Type 1 Diabetes Uncommon in Asia?
102. Mohr S.B. et al., Diabetologia, 2008; 51 (8): 1391-1398: The associa-tion between ultraviolet B irradiance, vitamin D status and incidence rates of type 1 diabetes in 51 regions worldwide.
103. Mahachoklertwattana P., Siriraj Med J, 2006; 58: 771-773: Obesity and type 2 diabetes in children and adolescents: current situation and future trends in Thailand
104. Santiprabhob J. et al., J Med Assoc Thai, 2007; 90 (8): 1608-1615: Etiology and glycemic control among Thai children and adolescents with diabetes mellitus
105. World Health Organization, First Global Ministerial Conference on Healthy lifestyles and Noncommunicable Disease Control. Discus-sion paper: Prevention and control of NCDs: priorities for investment, 2011; http://www.who.int/nmh/publications/who_bestbuys_to_pre-vent_ncds.pdf, accessed on 30 July 2013
106. United Nations, Prevention and control of non-communicable dis-eases, report of the Secretary-General, follow-up from the high-level meeting on non-communicable diseases, 2011; http://www.un.org/ga/search/view_doc.asp?symbol=A/66/83&lang=E, accessed on 03

49
August 2013107. lindström J. et al., Horm Metab Research, 2010; 42: S37-S57: Take
action to prevent diabetes - the IMAGE toolkit for the prevention of type 2 diabetes in Europe.
108. Tuomilehto J. et al., N Engl J Med, 2001; 344: 1343-1350: Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance
109. Knowler W. et al., N Engl J Med, 2002; 346 (6): 393-403: Reduc-tion in the incidence of type 2 diabetes with lifestyle intervention or metformin.
110. lindström J. et al., Lancet, 2006; 368: 1673-1679: Sustained reduc-tion in the incidence of type 2 diabetes by lifestyle intervention: the follow-up results of the Finnish Diabetes Prevention Study
111. International Diabetes Federation, Global Diabetes Plan 2011-2021, 2011; http://www.idf.org/global-diabetes-plan-2011-2021, accessed 02 August 2013
112. Organisation for Economic Co-operation and Development, OECD Health Ministerial Meeting, session 2: Healthy Choices, 2010; http://www.oecd.org/dataoecd/14/13/46098333.pdf, accessed 02 August 2013
113. Bureau of Policy and Strategy, Ministry of Public Health, Thai-land Healthy Lifestyle Strategic Plan 2011-2020; http://bps.moph.go.th/content/thailand-healthy-lifestyle-strategic-plan-be-2554-2563-2011-2020, accessed 13 August 2013
114. Sheehy A.M. et al., Mayo Clinic Proceedings, 2009; 841: 38-42: Back to Wilson and Jungner: 10 good reasons to screen for type 2 diabetes
115. Glumer C. et al., Diabetologia, 2006; 49: 1536-1544: What deter-mines the cost-effectiveness of diabetes screening?
116. American Diabetes Association, Diabetes Care, 2012; 35 (Suppl. 1): S11-S63: Position statement: standards of medical care in diabetes - 2012
117. Kahn R. et al., Lancet, 2010; 375: 1365-1374: Age at initiation and frequency of screening to detect type 2 diabetes: a cost-effectiveness analysis
118. World Health Organisation, Adherence to long-term therapies: evi-dence for action, 2003; http://www.who.int/chp/knowledge/publica-tions/adherence_full_report.pdf, accessed 02 August 2013
119. Bailey C. et al., Int J Clin Practice, 2011; 653: 314-322: Patient adher-ence to medication requirements for therapy of type 2 diabetes
120. Gherman A. et al., Diabetes Educator, 2011; 373: 392-408: How are adherent people more likely to think? A meta-analysis of health beliefs and diabetes self-care
121. Peyrot M. et al., Diabetes Care, 2006; 29: 953: Resistance to insulin therapy among patients andproviders: results of the cross-national Diabetes Attitudes, Wishes, and Needs (DAWN) study - response to Phillipov and Phillips
122. International Diabetes Federation, 2012 Clinical Guidelines Task Force, Global Guideline for Type 2 Diabetes, 2012; http://www.idf.org/sites/default/files/IDF-Guideline-for-Type-2-Diabetes.pdf, accessed on 02 August 2013
123. World Health Organization, Innovative Care for Chronic Conditions: Building Blocks for Action, 2002; http://www.who.int/chp/knowl-edge/publications/icccglobalreport.pdf, accessed 02 August 2013
124. International Alliance of Patients’ Organizations, Declaration on Pa-tient-Centered Healthcare, 2006; http://www.patientsorganizations.org/attach.pl/712/1051/IAPO%20Declaration%20on%20Patient-Centred%20Healthcare%20Poster.pdf, accessed on 02 August 2013
125. Asche C. et al., Clinical Therapeutics, 2011; 331: 74-109: Review of diabetes treatment adherence and the association with clinical and economic outcomes.
126. Williams G.C. et al., Current Diabetes Reports, 2002; 22: 145-152: Patient-centered diabetes self-management education
127. Norris S.l. et al., Diabetic Medicine, 2006; 235:544–556: Effec-tiveness of community healthworkers in the care of persons with diabetes
128. Palmer A.J. et al., Curr Med Res Opinion, 2004; 20 (Suppl 1): S27–S40: validation of the CORE diabetes model against epidemiological and clinical studies
129. Palmer A.J. et al., Curr Med Res Opinion, 2004; 20 (Suppl 1): S5–S26: The CORE diabetes model: projecting long-term clinical outcomes, costs and cost-effectiveness of interventions in diabetes mellitus (Types 1 and 2) to support clinical and reimbursement decision-making
130. IMS Health, Medical Ambition II, in: Changing Diabetes Barometer First Report, Novo Nordisk, 2007; http://www.novonordisk.com/im-ages/about_us/changing-diabetes/PDF/leadership%20forum%20pdfs/Barometer/Barometer%20Report%20-%20FINAl%20vERSION.pdf, accessed 05 August 2013
131. Organisation for Economic Co-operation and Development, OECD Health Policy Studies - Improving Value in Health Care: Measuring
Quality, 2010: http://www.oecd.org/health/ministerial/46098506.pdf, accessed on 05 August 2013
132. Gudbjörnsdottir S. et al., Diabetes Care, 2003; 26: 1270-1276: The national diabetes register in Sweden: an implementation of the St. vincent Declaration for quality improvement in diabetes care
133. Carstensen B. et al., Scand J of Public Health, 2011; 39 (Suppl.): 58-61: The National Diabetes Register
134. Adolffson E.T. et al., Prim Care Diabetes, 2010; 4 (2): 91-97: The Swedish national survey of the quality and organization of diabetes care in primary healthcare - Swed-QOP
135. Novo Nordisk, Changing Diabetes Barometer First Report, 2007; http://www.novonordisk.com/images/about_us/changing-diabetes/PDF/leadership%20forum%20pdfs/Barometer/Barometer%20Re-port%20-%20FINAl%20vERSION.pdf, accessed 05 August 2013
136. Franco O.H., Arch Intern Med, 2007;167:1145-1151: Associations of diabetes mellitus with total life expectancy and life expectancy with and without cardiovascular disease
137. Koopmanschap M. et al., Diabetologia, 2002; 45: S18-S22: Coping with type II diabetes; the patient’s perspective
138. World Diabetes Foundation, http://www.worlddiabetesfoundation.org/projects/thailand-wdf08-395, accessed 07 August 2013
139. National Health Security Organisation, DM/HT study project, 2012: An assessment on quality of care among patients diagnosed with type 2 diabetes and hypertension visiting Ministry of Public Health and Bangkok Metropolitan Administration hospitals in Thailand, 2012: http://www.nhso.go.th/downloadfile/fund/CRCN_55/1.Presentation/1.%E0%B8%A3%E0%B8%B2%E0%B8%A2%E0%B8%87%E0%B8%B2%E0%B8%99%E0%B8%9C%E0%B8%A5%E0%B8%81%E0%B8%B2%E0%B8%A3%E0%B8%9B%E0%B8%A3%E0%B8%B0%E0%B9%80%E0%B8%A1%E0%B8%B4%E0%B8%99%E0%B9%82%E0%B8%84%E0%B8%A3%E0%B8%87%E0%B8%81%E0%B8%B2%E0%B8%A3DM-HT-%E0%B8%9B%E0%B8%B52555.pdf, accessed 13 August 2013
140. Diabetes Association Thailand, Thai Diabetes Treatment Guideline 2011: http://www.diabassocthai.org/index.php?option=com_content&view=article&id=12%3A-2551-&catid=2%3A2011-01-25-09-11-02&Itemid=6&lang=th: accessed 13 August 2013
141. Benjamin E.M., Clinical Diabetes, 2002; 20 (1): 45-47: Self-Monitor-ing of Blood Glucose: The Basics
142. Kongubol A. et al., BMC Pregnancy & Childbirth, 2011; 11: 59: http://www.biomedcentral.com/1471-2393/11/59
143. Krairittichai U. et al., J Med Assoc Thai, 2013; 96 (6): 637-643: A 4-year prospective study on long-term complications of type 2 dia-beteic patients: the Thai DMS Diabetes Complications Project
144. Sintawanarong, P., in: Bangkok Post, 31 October 2013: Diabetes kills 8,000 Thais each year, http://www.bangkokpost.com/print/377376/
145. Chaikledkaew, U. et al., value in Health, 2008; 11 (Suppl.1): S69-S74: Factors affecting healthcare costs and hospitalisations among diabetic patients in Thai public hospitals
Photo credits:Page 5, 12, 36: Kim de Keijzer
The following photos have been obtained from http://www.shutterstock.com with permission for editorial use:
Page 7, 16: Charlie Edwards
Page 10: vlad0209
Page 18, 51: 1,000 Words
Page 31: pixbox77
Page 41: jukurae

50
Notes

51

52
NN
PT/NN
/035/2013
Novo Nordisk Pharma (Thailand) ltd.139 Sethiwan Tower, 4th FloorPan Road, Silom, Bangrak DistrictBangkok, 10500Thailandwww.novonordisk.com