Embed Size (px)
Citation preview

Teneligliptin
The emerging gliptin
Akshata RaoMedical Services

Diabetes in Indian subcontinent
Retrieved from http://www.cadiresearch.org/topic/diabetes-indians/diabetes-in-the-indian-subcontinent

Choice of agents in current use
Sulphonylureas
Insulin
Thiazolidinediones
Biguanides
Alpha-glucosidase inhibitors
Meglitinides

Each therapy has a drawback
Tripathi 2005, 5th Edition Nature Reviews 2007 :6 :109-110
Pharmacology and Therapeutics 2010:125; 328-361

DPP-4 Inhibitors - A major addition to Diabetes Armamentarium
Major DPP-4 inhibitors currently available :-
Sitagliptin
Vildagliptin
Saxagliptin
Linagliptin

Highest potency
Long half – life
Safety in renal patients
Safety in hepatic patients
Approved by *Ministry of Health, Labour and Welfare (MHLW) Japanese Pharmaceutical and Medical Devices Agency (PMDA) in
2012
Accessed from http://www.pmda.go.jp/files/000153594.pdf
Ministry of Health, Labour and Welfare (MHLW) Japanese Pharmaceutical and Medical Devices Agency - Both are governing bodies which is responsible for final drug approval in Japan
Teneligliptin – Novel and potent addition to gliptin category
Important features to be noted

Teneligliptin – Structural features
Introduction of the ‘’anchor lock domain’’, which binds to the S2 extensive subsite - Higher potency and selectivity
Forms a stable gliptin-DPP-4 enzyme complex due rigid 5 ring “J structure - Longer Half life
Carbonyl group derived from the peptide mimetic, forms a hydrogen bond (strongest bond) DPP4 enzyme - Higher potency
Biochemical and Biophysical Research Communications 434 (2013) 191–196

Unique binding capability
Occupies a larger area of 2.08nm2
Effect on the outcome 1500 fold higher
activity
As compared to Vildagliptin and
Saxagliptin
5 fold higher activity
As compared to Sitagliptin

Unique mode of excretion
Teneligliptin excreted by two modes of excretion i.e. by liver and kidney . (Liver - 45.4% and kidney - 46.5%

Teneligliptin Vs other gliptins – Interaction with DPP-4 enzymes.
Journal of Diabetes Mellitus, 2016, 6, 113-131

Teneligliptin Vs other gliptins – Pharmacokinetic comparison
Journal of Diabetes Mellitus, 2016, 6, 113-131

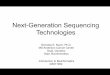
Teneligliptin in renally compromised patients

In special population(Renal Impairment)
Design Prospective, non-randomized study with 43 diabetic ESRD patients ; Teneligliptin 20 mg/day (n=14) and Control group ( n= 29) Control group treated with voglibose, vildagliptin, miglitol, Meglitinides
Duration 28 weeks
Patient characteristics
ESRD diabetic patients with Serum Creatinine levels* (Teneligliptin group = 9.1mg/dl and Control group = 10.3 mg/dl
End-points Blood glucose levels , Glycated Albumin levels (GA) and HbA1C(%)
Normal creatinine levels *- 0.6 to 1.2 milligrams (mg) per deciliter (dL) in adult males and 0.5 to 1.1 milligrams per deciliter in adult females Int Urol Nephrol (2014) 46:427–432
Safety and efficacy of teneligliptin: a novel DPP-4 inhibitor for hemodialysis patients with type 2 diabetes.

Teneligliptin significantly improves the glycemic states in Diabetic ESRD patients
Blood glucose decreased significantly in the teneligliptin group from 4 weeksGA level in the teneligliptin group dropped significantly after 4 weeksHbA1c in the teneligliptin group declined significantly from 8 weeks
P<0.05 P<0.05
p = 0.057
Int Urol Nephrol (2014) 46:427–432
Duration – 28 weeks

Teneligliptin also improves glycemic states in patients switching from conventional Oral Anti-Diabetic drugs
Blood glucose level decreased 21–60 mg/dl at 28 weeks after teneligliptin administration. GA dropped 1.7–2.3 % by 28 weeks and HbA1c fell 0.3–0.8 % by 24 weeks.
Int Urol Nephrol (2014) 46:427–432

Conclusion
• Teneligliptin is well tolerated, safe, and significantly improves glycemic
control in diabetic patients with ESRD.
• No serious side effects or hypoglycemia relating to teneligliptin is seen
during the study.
• Teneligliptin 20 mg is probably stronger than Vildagliptin 50 mg for
dialysis patients.
• Teneligliptin is expected to be a powerful DPP-4 inhibitor of ESRD.
Int Urol Nephrol (2014) 46:427–432

Teneligliptin in Indian patients

Study of Anti-hyperglycemic Activity of Teneligliptin in Patients of T2DM
Design Uncontrolled, open label, observational study with patients who were uncontrolled on metformin were selected. Teneligliptin 20 mg/day was added to current treatment.
Duration 12 weeks
Patient characteristics
Patients of T2DM attending OPD of Dhanashree Hospital, Pune were included in the study after obtaining informed written consent
End-points Fasting blood sugar level, Post prandial blood sugar level and HbA1C (%)
Indian J Pharmacol. 2015 Dec; 47(Suppl 1): S57–S177.

Teneligliptin Vs other gliptins

Impact of teneligliptin on oxidativestress and endothelial function in type 2
diabetes patients with chronic kidney disease: a case–control study
Cardiovasc Diabetol (2016) 15:76
Design Open-label, prospective, randomized study with 45 diabetic CKD patients who received sitagliptin for at least 12 months were randomized to either continue sitagliptin (n = 23) or switch to teneligliptin (n = 22)
Duration 24 weeks
Patient characteristics
type 2 diabetes with (HbA1c) >6.5 %, CKD (eGFR) <60 mL/min/1.73 m2 or microalbuminuria >30 mg/g Cr] [14], and treatment with sitagliptin for 1 year or longer
End-points HbA1c, eGFR, or urinary albumin excretion levels, endothelialfunction by reactive hyperaemia index (RHI), reactive oxygen metabolites (ROMs) measured by the d-ROMS test

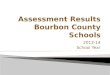
Results
Baseline After 3 months Fasting blood
glucose (mg/dl)172.4 124.5
Post prandial blood glucose
225.5 176.4
HbA1C (%) 9.5 8.6
Cardiovasc Diabetol (2016) 15:76
Conclusion: Teneligliptin can be considered as an effective alternative for
add-on treatment in patients of T2DM uncontrolled on metformin monotherapy.

Results
Cardiovasc Diabetol (2016) 15:76

Results
Changes in RHI Changes in d-ROMs
Cardiovasc Diabetol (2016) 15:76

Conclusion
• Teneligliptin exhibits beneficial effects on both oxidative stress and
endothelial function in Japanese patients with type 2 diabetes and CKD.
• Teneligliptin exhibits beneficial effects on both oxidative stress and
endothelial function in Japanese patients with type 2 diabetes and CKD.
• The antioxidative effect of Teneligliptin is brought about by the sulphur
atom present in the molecule
Cardiovasc Diabetol (2016) 15:76

Efficacy of linagliptin and teneligliptin for glycemic control in type 2 diabetic
patients with chronic kidney disease: assessment by continuous glucose
monitoring; a pilot study
Diabetology International pp 1-7 First online: 09 March 2016
Design randomized and crossover in design in 13 type 2 diabetes patients with CKD treated with teneligliptin at 20 mg/day or linagliptin at 5 mg/day for 6 days then switched to the other agent for another 6 days.)
Duration 12 days
Patient characteristics
type 2 diabetes patients with CKD who maintained glycosylated hemoglobin (HbA1c) levels at <9 % by diet and exercise and had estimated glomerular filtration rates (eGFRs) \60 ml/min 1.73 m2.
End-points Mean amplitude of glucose excursions (MAGE)

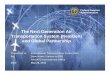
Results
Twenty-four-hour mean sensor glucose levels before treatment and
after 6 days of treatment with linagliptin/ teneligliptin in 13
patients.
Mean amplitude of glycemic excursions (MAGE) before treatment and after 6 days treatment with linagliptin/teneligliptin.Values are mean ± standard deviation. **P<0.01, vs before treatment
no significant difference between thetwo groups (p = 0.05).
Diabetology International pp 1-7 First online: 09 March 2016

Conclusion
• In type 2 diabetes patients complicated by CKD, the effects of treatment
with linagliptin and teneligliptin on CGM-based MAGE were comparable.
• Because both agents significantly reduced the 24-h mean sensor glucose
levels and AUC 180 but did not increase the incidence of hypoglycemia,
they have comparable efficacy and safety in type 2 diabetes patients
complicated by CKD.
Diabetology International pp 1-7 First online: 09 March 2016

Design Open label , non-randomised parallel group study (8 subjects in each group)HealthyMild hepatic impairment Moderate hepatic impairment
Evaluation parameters
All Teneligliptin Pharmacokinetic parameters and safety parameters
In special population(Hepatic impairment)
Clinical Pharmacology in Drug DevelopmentVolume 3, Issue 4, pages 290–296, July/August 2014
Objective – To determine the pharmacokinetic and safety of single oral administration of therapeutic doses of 20 mg Teneligliptin in subjects with mild and moderate hepatic impairment as compared to healthy
subjects
Pharmacokinetics and safety of teneligliptin in subjects with hepatic
impairment

Teneligliptin well-tolerated by patients with hepatic impairment
Parameter Group Ratio of Geometric mean
90% CI (%)
AUC 0-∞ Mild 145.85 122.13-174.17
Moderate 159.41 133-190.37
FDA-recommended “dose-adjustment” boundary of 200%
The AUC for Teneligliptin is within the dose adjustment limit set by FDA
No dose adjustment required for patients with mild to moderated hepatic
impairment
Clinical Pharmacology in Drug DevelopmentVolume 3, Issue 4, pages 290–296, July/August 2014

In special population(Cardiac patients)
Heart Vessels. 2015 Aug 13.
Major findings of the study
An additional treatment with Teneligliptin improved Left ventricular diastolic function and endothelial function.
Teneligliptin treatment exerts cardio-protective effects in T2DM patients with LV dysfunction at an early stage.
An increase in the serum levels of adiponectin* after 3 months of Teneligliptin treatment is seen
adiponectin*- adiponectin plays a role of antiatherosclerotic, antidiabetic, and anti-inflammatory effectsA high plasma level of adiponectin leads to a decrease in cardiovascular events
Teneligliptin improves left ventricular diastolic function and endothelial function
in patients with diabetes.

In special population(Cardiac patients)
International Journal of General Medicine 2016:9 65–71
Effects of teneligliptin on PDMPs and PAI-1 in patients with diabetes on hemodialysis

Future research on possible benefits of Teneligliptin
Obesity Title of the study Year of Publishing Teneligliptin effects
The novel DPP-4 inhibitor teneligliptin prevent
s high-fat diet-induced obesity accompanied with
increased energy expenditure in mice.
Eur J Pharmacol. 2014
Jan 15;723:207-15
Adipocyte hypertrophy and hepatic steatosis induced by
a high-fat diet were suppressed by teneligliptin.
Teneligliptin improves metabolic abnormalities in a
mouse model of postmenopausal obesity.
J Endocrinol. 2015 Oct;227(1):25-36.
Teneligliptin effectively ameliorated the
characteristics of metabolic abnormalities associated
with postmenopausal obesity.. Hepatic steatosis
was also markedly improved.

Future research on possible benefits of Teneligliptin
Non-alcoholic Fatty Liver diseaseTitle of the study Year of Publishing Teneligliptin effects
The Dipeptidyl Peptidase-4 Inhibitor Teneligliptin
Attenuates Hepatic Lipogenesis via AMPK
Activation in Non-Alcoholic Fatty Liver Disease Model
Mice
Int J Mol Sci. 2015 Dec; 16(12):
29207–29218.
Serum alanine aminotransferase and
intrahepatic triglyceride levels were significantly
decreased in teneligliptin-treated mice (p < 0.05).
Teneligliptin increased hepatic expression levels of
phosphorylated AMP-activated protein kinase
(AMPK) protein.

Teneligliptin – Road ahead

Teneligliptin –Clinical trial in cardiac patients
The trial is expected to be completed by June 2019Retrieved from https://clinicaltrials.gov/ct2/show/NCT02449330

Tenegliptin – Dosage and Administration
• Indication • Oral Teneligliptin is approved as an add-on for treatment of adults
with type 2 diabetes mellitus patients who have not responded adequately to treatment with diet and exercise or addition of other anti-diabetic agents such as biguanides, sulfonylureas, thiazolidinediones, glinides, α-glucosidase inhibitors or insulin.
• Dosage • The recommended dosage of Teneligliptin is 20 mg once daily. • Teneligliptin may be administered irrespective of food, preferably
before breakfast. • It is advisable to uptitrate the dosage to 40 mg once daily in patients
who do not achieve adequate glycemic control as required.
Journal of Diabetes Mellitus, 2016, 6, 113-131

Precautions while administering Teneligliptin
• Teneligliptin should be used with caution in patients with severe hepatic
impairment & those with heart failure (NYHA Class III - IV), because of a
lack of clinical experience in these populations.
• Teneligliptin should not be used in patients with history of pancreatitis.
If the patient is already on sulfonylurea & addition of gliptin is
considered, in such cases the dose of sulfonylurea should be halved &
then up-titrated as required to reduce the risk of hypoglycaemia.
• There may be chances of hypoglycemia on co-administration of
Teneligliptin with insulin & hence dosage reduction may be required
Journal of Diabetes Mellitus, 2016, 6, 113-131

THANK YOU!!!!