Embed Size (px)
Citation preview

Temperomandibular joint. NORMAL ANATOMY,RADIOLOGY & APPLIED ASPECT
BY : ASHISH RANGHANI
PG STUDENT PART 1
DEPARTMENT OF ORAL MEDICINE & RADIOLOGY
04/11/2015

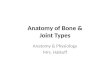
Anatomy-Bone
• Zygomatic▫ Arch
• Sphenoid
• Temporal
• Mandible▫ Head

Introduction
• The temporomandibular joint (TMJ), also known as the mandibular
joint, is an ellipsoid variety of the right and left synovial joints
forming a bicondylar articulation.
• The most important functions of the
temporomandibular joint (TMJ) are mastication
and speech

UNIQUE FEATURE OF TMJ
Bilateral diarthrosis – right & left function together
Articular surface covered by fibrocartilage instead of hyaline cartilage
In contrast to other diarthrodial joints TMJ is last joint to start develop, in about 7th week in utero

COMPONENTS
•Mandibular condyle
•Articular surfaces of Temporal bone
•Capsule
•Articular disc
•Ligaments
•Muscular component

THE MANDIBULAR CONDYLE
• An ovoid process seated atop a narrow mandibular neck. It’s the articulating surface of the mandible.
• It is convex in all directions but wider latero-medially (15 to 20 mm) than antero-posteriorly (8 to 10mm).

• The medial pole is directed more posteriorly.
• Thus, if the long axes of two condyles are extended medially, they meet at approximately the basion on the anterior limit of the foramen magnum, forming an angle that opens toward the front ranging from 145° to 160°
It has a medial and lateral pole

• The lateral pole of the condyle is rough, bluntly pointed, and projects only moderately from the plane of ramus, while the medial pole extends sharply inward from this plane.
• The articular surface lies on its anterosuperior aspect, thus facing the posterior slope of the articular eminence of the temporal bone.

CRANIAL COMPONENT OR ARTICULAR
SURFACE OF TEMPORAL BONE

•The articular surface of the temporal
bone is situated on the inferior aspect
of temporal squama anterior to
tympanic plate.

ARTICULAR EMINENCE
• This is the entire transverse bony bar that forms the anterior root of zygoma. This articular surface is most heavily traveled by the condyle and disk as they ride forward and backward in normal jaw function.
ARTICULAR TUBERCLE
• This is a small, raised, rough, bony knob on the outer end of the articular eminence.
• It projects below the level of the articular surface and serves to attach the lateral collateral ligament of the joint.

E: Articular eminence; enp:
entogolenoid process;
t:articular tubercle; lb:
lateral border of the
mandibular fossa; pep:
preglenoid
plane; Gf: glenoid fossa

Articular Disc
• The articular disc is the most important anatomic structure of the TMJ.
• It is a biconcave fibrocartilaginous structure located between the mandibular condyle and the temporal bone component of the joint.
• Its functions to accommodate a hinging action as well as the gliding actions between the temporal and mandibular articular bone.

• The articular disc is a roughly oval, firm, fibrous plate.
1. anterior band = 2 mm in thickness,
2. posterior band = 3 mm thick,
3. thin in the centre intermediate band of 1 mm thickness.
More posteriorly there is a bilaminar or retrodiscal region.
• It is shaped like a peaked cap that divides the joint
into a larger upper compartment and a smaller
lower compartment.

• Hinging movements take place in the lower compartment and gliding movements take place in the upper compartment.
• The superior surface of the disc - saddle-shaped
to fit into the cranial contour,
• The inferior surface - concave to fit against the mandibular condyle.

FIBROUS CAPSULE
Thin sleeve of tissue completely surrounding the joint. Extends from the circumference of the cranial articular surface to the neck of the mandible.

• Anteriorly, the capsule has an
orifice through which the lateral
pterygoid tendon passes. This
area of relative weakness in the
capsular lining becomes a source
of possible herniation of intra-
articular tissues, and this, in
part, may allow forward
displacement of the disk.

Mainly 4 forms are
seen-
1. Convex-58%
2. Flat- 25%
3. Pointed-12%
4. Round- 3%
( mainly in children)

Temporomandibular Ligaments

Anatomy- Ligaments
Sphenomandibular
Stylomandibular
-limits protrusion movement
Joint capsule
Lateral ligament
-limits depression, posterior movement

Collateral Ligaments
• The ligament on each side of the jaw is designed in two distinct layers.
• The wide outer or superficial layer is usually fan-shaped and arises from the outer surface of the articular tubercle and most of the posterior part of the zygomaticarch.
• There is often a roughened, raised bony ridge of attachment on this area.

Sphenomandibular Ligament
• Arises from the angular spine of the sphenoid and petrotympanic fissure.
• Runs downward and outward.
• Insert on the lingula of the mandible.

• The ligament is pierced by the myelohyoid nerve and vessels.
• This ligament is passive during jaw movements, maintaining relatively the same degree of tension during both opening and closing of the mouth.

Stylomandibular Ligament
• This is a specialized dense, local concentration of deep cervical fascia extending from the apex and being adjacent to the anterior aspect of the styloid process and the stylohyoid ligament to the mandible’s angle and posterior border.

• This ligament then extends forward as a broad fascial layer covering the inner surface of the medial pterygoid muscle.
• The anterior edge of the ligament is thickened and sharply defined.
• This ligament becomes tense only in extreme protrusive movements. Thus, it can be considered only as an accessory ligament of uncertain function.

SYNOVIAL FLUID
• It is clear, straw-colored viscous fluid.
• It diffuses out from the rich cappillary network of the synovial membrane.
Contains:
• Hyaluronic acid which is highly viscous
• May also contain some free cells mostly macrophages.

Functions:
• Lubricant for articulating surfaces.
• Carry nutrients to the avascular tissue of the joint.
• Clear the tissue debris caused by normal wear and tear of the articulating surfaces.

OCCLUSION
• The way the teeth fit together may affect the TMJ complex.
• A stable occlusion with good tooth contact and interdigitation provides maximum support to the muscles and joint, while poor occlusion (bite relationship) may cause the muscles to malfunction and ultimately cause damage to the joint itself.
• Instability of the occlusion can increase the pressure on the joint, causing damage and degeneration.

VASCULARISATION
• Branches of External Carotid Artery
1. Superficial temporal artery
2. Deep auricular artery
3. Anterior tympanic artery
4. Ascending pharyngeal artery
5. Maxillary artery

• The Blood supply to TMJ is only Superficial, i.e. there is no blood supply inside the capsule
• TMJ takes its nourishment from Synovial fluid

Anatomy- Arterial Supply
• Deep Auricular
• Anterior Tympanic
• Middle Meningeal
• Maxillary
• External carotid

VENOUS SUPPLY
• venous plexus
• maxillary vein
• Tranverse facial vein.
• Superficial temporal vein.

Nerve supply
• Auriculotemporal
• Deep temporal
• Massetric nerve

Anatomy- Nerves
• Auriculotemporal (sensory) MMA*
• Inferior alveolar (sensory)▫ mylohyoid nerve-
mylohyoid m.
• Lingual (sensory)• Buccal (sensory)• muscular branches (to
muscles of mastication)
Chorda tympani

RELATIONS

Anteriorly - Mandibular notchLateral pterygoidMasseteric nerve and artery

Posteriorly - parotid glandSuperficial temporal vesselsAuriculotemporal nerve

Medially - Tympanic plate (separates from ICA)
spine of sphenoid
Auriculotemporal & chorda tympanynerve
middle meningeal arterymaxillary artery
Laterally –Skin and fasciaParotid glandTemporal branches of facial nerve

Superiorly –
middle cranial fossa
middle meningeal vessels
Inferiorly –
maxillary artery &
vein

Joint movements……
• Rotational / hinge movement in first 20-25mm of mouth opening
• Translational movement after that when the mouth is excessively opened.

• Translatory movement – in the superior part of the joint as the disc and the condyle traverse anteriorly along the inclines of the anterior tubercle to provide an anterior and inferior movement of the mandible.

• Hinge movement – the inferior portion of the joint between the head of the condyle and the lower surface of the disc to permit opening of the mandible.

Depression Of Mandible
Lateral pterygoidDigrastricGeniohyoidMylohyoid
Elevation of MandibleTemporalisMasseterMedial Pterygoids
Protrusion of MandibleLateral PterygoidsMedial Pterygoids
Retraction of MandiblePosterior fibres of Temporalis

Anatomy- Muscles
• Masseter▫ elevates and protrudes
mandible
• Temporal▫ elevates and retracts
mandible
Innervation:
Mandibular (V3)

Anatomy- Muscles
• Lateral Pterygoid▫ Bilaterally- protraction▫ Unilaterally- contralateral
swing
• Medial Pterygoid▫ Elevation, protrusion,
unilaterally: grinding
Innervation: Mandibular (V3)
Digastric-opening


THANK YOU