Embed Size (px)
Citation preview
Electrolyte Electrolyte EmergencyEmergency
Khrongwong Musikatavorn M.D.Khrongwong Musikatavorn M.D. Emergency UnitEmergency Unit
King Chulalongkorn Memorial King Chulalongkorn Memorial Hospital and Faculty of MedicineHospital and Faculty of Medicine
Chulalongkorn UniversityChulalongkorn UniversityFebruary 10February 10thth 2009 2009

Common life-threatening Common life-threatening Electrolyte disturbances Electrolyte disturbances
Dysnatremias (hyponatremia, Dysnatremias (hyponatremia, hyprenatremia)hyprenatremia)
Dyskalemias (hyperkalemia, Dyskalemias (hyperkalemia, hypokalemia)hypokalemia)
Dyscalcemias (hypercalcemia, Dyscalcemias (hypercalcemia, hypocalcemia)hypocalcemia)
HypomagnesemiaHypomagnesemia
Sodium homeostasisSodium homeostasis
Disease of water homeostasisDisease of water homeostasis
~ 60% of total body composition = water~ 60% of total body composition = water
2/3 = intracellular space 1/3 extracellular 2/3 = intracellular space 1/3 extracellular space (interstitial + intravascular)space (interstitial + intravascular)
Sodium homeostasis and water balance Sodium homeostasis and water balance regulates by renin-angiotensin-aldosterone regulates by renin-angiotensin-aldosterone system and antidiuretic hormone (ADH)system and antidiuretic hormone (ADH)
ADH ADH water reabsorption, stimulated by water reabsorption, stimulated by volume depletion and many other volume depletion and many other conditions conditions

HyponatremiaHyponatremia
Sodium concentration < 135 mmol/LSodium concentration < 135 mmol/L
The most common electrolyte The most common electrolyte abnormality in the hospitalized patientsabnormality in the hospitalized patients11
Mild hyponatremia 15-22% of Mild hyponatremia 15-22% of ambulatory patientsambulatory patients22
1. N Engl J Med 2000;342:1581-92. Clin Chim Acta 2003;337:169-72

HyponatremiaHyponatremia
Hypo-osmolarity hypotonicity Hypo-osmolarity hypotonicity hyponatremiahyponatremia
excess of free waterexcess of free water
Hyper-osmolarity hypotonicity Hyper-osmolarity hypotonicity hyponatremiahyponatremia
Hyper-osmolar agents: hyperglycemia, Hyper-osmolar agents: hyperglycemia, mannitolmannitol
PseudohyponatremiaPseudohyponatremia
HyponatremiaHyponatremiaDecrease volume of extracellular fluidDecrease volume of extracellular fluid
Renal sodium lossRenal sodium loss
Diuretics, osmotic agents, adrenal Diuretics, osmotic agents, adrenal insufficiency, salt wasting nephropathyinsufficiency, salt wasting nephropathy
Extrarenal sodium lossExtrarenal sodium loss
Diarrhea, vomiting, excessive Diarrhea, vomiting, excessive sweating, “third space loss” sweating, “third space loss”
N Engl J Med 2000;342:1581-9

HyponatremiaHyponatremia
Increase volume of extracellular fluidIncrease volume of extracellular fluid
Congestive heart failureCongestive heart failure
CirrhosisCirrhosis
Nephrotic syndromeNephrotic syndrome
Renal failureRenal failure
PregnancyPregnancy
N Engl J Med 2000;342:1581-9

HyponatremiaHyponatremia Normal volume of extracellular fluidNormal volume of extracellular fluid
SIAD**SIAD**
Adrenal insufficiencyAdrenal insufficiency
HypothyroidismHypothyroidism
Thiazide diureticThiazide diuretic
Excessive water intakeExcessive water intake
Primary polydipsia, tap-water enema, Primary polydipsia, tap-water enema, accidental ingestion of water, sodium-free accidental ingestion of water, sodium-free irrigant solution irrigant solution
N Engl J Med 2000;342:1581-9

Signs and Symptoms of Signs and Symptoms of hyponatremiahyponatremia
Rate of decrease in [NaRate of decrease in [Na++] and level of [Na] and level of [Na++]]
Usually asymptomatic if [NaUsually asymptomatic if [Na++] ≥ 125 mmol/L] ≥ 125 mmol/L
Headache, nausea, vomiting, anorexia, Headache, nausea, vomiting, anorexia, muscle cramps, lethargy, restlessness, muscle cramps, lethargy, restlessness, disorientationdisorientation
Seizures, coma, permanent brain damage, Seizures, coma, permanent brain damage, respiratory arrest, brain-stem herniationrespiratory arrest, brain-stem herniation

Evaluation of Evaluation of hyponatremiahyponatremia
Rule out hyper-osmolar hyponatremia and Rule out hyper-osmolar hyponatremia and pseudohyponatremia pseudohyponatremia “true” “true” hyponatremiahyponatremia
How is the patient’s volume status? How is the patient’s volume status? Hypervolemic, hypovolumic or euvolemicHypervolemic, hypovolumic or euvolemic
2 litres of 0.9% NaCl over 24-48 hours can 2 litres of 0.9% NaCl over 24-48 hours can be tried if hypovolemia is doubtful be tried if hypovolemia is doubtful 11. Serial . Serial [Na[Na++] follow-up is necessary] follow-up is necessary
Determine the causes of hyponatremiaDetermine the causes of hyponatremia
Hormone depletion should be worked up in Hormone depletion should be worked up in the specific casesthe specific cases
1. N Engl J Med 2007; 356: 2064-72

Evaluation of Evaluation of hyponatremiahyponatremia
Hypo-osmolarity hypotonicity Hypo-osmolarity hypotonicity hyponatremia = hyponatremia = true hyponatremiatrue hyponatremia
Direct serum osmolarity measurement Direct serum osmolarity measurement or calculated osmolarityor calculated osmolarity
effective osmolarity < 275 mOsm/kgeffective osmolarity < 275 mOsm/kg
Measured osmolarity – BUN(mg/dl)/2.8 Measured osmolarity – BUN(mg/dl)/2.8
Or 2[NaOr 2[Na++] + glucose(mg/dl)/18] + glucose(mg/dl)/18
N Engl J Med 2007; 356: 2064-72

Treatment of Treatment of hyponatremiahyponatremia
Aggressiveness of the treatmentAggressiveness of the treatment
Is patient symtomatic of Is patient symtomatic of hyponatremia?hyponatremia?
Volume status of the patientVolume status of the patient
Detection and treatment of the Detection and treatment of the preventable causes of hyponatremiapreventable causes of hyponatremia
Serial monitoring of [NaSerial monitoring of [Na++] during ] during treatmenttreatment

Symptomatic Symptomatic hyponatremiahyponatremia
“an emergency “an emergency condition”condition” Aggressive sodium correctionAggressive sodium correction
3% NaCl (513 mmol/L) in the rate of 1-2 3% NaCl (513 mmol/L) in the rate of 1-2 mmol/L/hourmmol/L/hour
In hypervolemic or euvolemic patient, furosemide In hypervolemic or euvolemic patient, furosemide should be used with hypertonic salineshould be used with hypertonic saline
The symptoms usually improve within the few The symptoms usually improve within the few hourshours
Rapid correction can be very harmfulRapid correction can be very harmful
Serial monitoring of [NaSerial monitoring of [Na++]]

Correction of Correction of hyponatremiahyponatremia
Generally not faster than 0.5 mmol/L/hour or 12 Generally not faster than 0.5 mmol/L/hour or 12 mmol/L in 24 hoursmmol/L in 24 hours
Varies from 8-20 mmol/L/dayVaries from 8-20 mmol/L/day
Too rapid = Osmotic demyelination syndrome (ODS)Too rapid = Osmotic demyelination syndrome (ODS)
Central pontine myelinolysis (CPM) and Central pontine myelinolysis (CPM) and extrapontine (EPMextrapontine (EPM
Biphasic course of neurological deteriorationBiphasic course of neurological deterioration
Dysarthria, dysphagia, flaccid quadriplegia (CPM)Dysarthria, dysphagia, flaccid quadriplegia (CPM)
Movement disorder (eg. Parkinsonism) in EPMMovement disorder (eg. Parkinsonism) in EPM
J Neurol Neurosurg Psychiatry 2004;75(Suppl III):iii22–iii28

Calculation of sodium Calculation of sodium deficitdeficit
Traditional formulaTraditional formula
(Desired[Na(Desired[Na++] – Measured[Na] – Measured[Na++])x(0.6)(Weight in ])x(0.6)(Weight in kilograms) = kilograms) =
mmol[Nammol[Na++]administered]administered
Eg : Symptomatic hyponatremic man 70 kg.needs 2 Eg : Symptomatic hyponatremic man 70 kg.needs 2 mmol/L raising of his [Nammol/L raising of his [Na++] (105 to 107 mmol/L) within ] (105 to 107 mmol/L) within 2 hours with 3% NaCl (Na2 hours with 3% NaCl (Na++ 513 mmol/1000 ml) 513 mmol/1000 ml)
(107-105)X(0.6)(70) (107-105)X(0.6)(70) ≅ ≅ 84 mmol84 mmol of Na of Na+ + = 84/513 = = 84/513 = 0.16 0.16 litre of 3%litre of 3%
0.16 litre (160 ml) given in 2 hours, so the rate of IV is 0.16 litre (160 ml) given in 2 hours, so the rate of IV is 160/2 160/2
= = 80 ml/hr80 ml/hr

Calculation of sodium Calculation of sodium deficitdeficit
N Engl J Med 2007; 356: 2064-72

Syndrome of Syndrome of Inappropriate Inappropriate
Antidiuresis (SIAD) Antidiuresis (SIAD) The most common cause of The most common cause of
hyponatremiahyponatremia
Euvolemic patientsEuvolemic patients
Inappropriate secretion of ADHInappropriate secretion of ADH
Many etiologiesMany etiologies

Causes of SIADCauses of SIAD
Malignant diseasesMalignant diseases
Pulmonary disordersPulmonary disorders
CNS disordersCNS disorders
DrugsDrugs : antidepressants and antipsychotics, : antidepressants and antipsychotics, chlorpropamide, clofibrate, vincristine, chlorpropamide, clofibrate, vincristine, cyclophosphamide, ifosfamide, Narcotics, cyclophosphamide, ifosfamide, Narcotics, “ectasy”, NSAIDs“ectasy”, NSAIDs
Nausea, Pain, StressNausea, Pain, Stress
Diagnosis of SIADDiagnosis of SIAD
Decrease effective osmolarity < 275 mOsm/kgDecrease effective osmolarity < 275 mOsm/kg
Urine Osm > 100 mOsm/kgUrine Osm > 100 mOsm/kg
Clinical euvolemiaClinical euvolemia
Urine sodium > 40 mmol/L with normal salt Urine sodium > 40 mmol/L with normal salt intakeintake
Normal thyroid and adrenal functionNormal thyroid and adrenal function
No recent diuretic use No recent diuretic use

Treatment of SIADTreatment of SIAD
Failure to correct with 0.9% NaClFailure to correct with 0.9% NaCl
Symptomatic SIAD : 3% NaCl infusion 1-2 Symptomatic SIAD : 3% NaCl infusion 1-2 mmol/L for 2 hourmmol/L for 2 hour
Not faster than 0.5 mmol/L/hour in 24 hoursNot faster than 0.5 mmol/L/hour in 24 hours
Serial [NaSerial [Na++] monitoring] monitoring
Chronic SIAD : fluid restriction, salt and Chronic SIAD : fluid restriction, salt and protein dietprotein diet

HypernatremiaHypernatremia
Sodium concentration > 145 mmol/LSodium concentration > 145 mmol/L
Free water or hypotonic fluid lossFree water or hypotonic fluid loss
Iatrogenic : hypertonic sodium Iatrogenic : hypertonic sodium administrationadministration
Happened in the patients with failure Happened in the patients with failure to water access and thirst eg. Elderly, to water access and thirst eg. Elderly, infant, neurological impairment, infant, neurological impairment, intubated patient intubated patient

Signs and symptoms of Signs and symptoms of hypernatremiahypernatremia
Rate of increase in [NaRate of increase in [Na++] and level of ] and level of [Na[Na++]]
confusion, weakness, alteration of confusion, weakness, alteration of consciousness, seizure and comaconsciousness, seizure and coma
Vascular rupture from brain shrinkage Vascular rupture from brain shrinkage : eg. SAH: eg. SAH
Too rapid decreasing in [NaToo rapid decreasing in [Na++] = ] = cerebral edemacerebral edema

Treatment of Treatment of hypernatremiahypernatremia
Detection and correction of the Detection and correction of the causes causes : Fever, GI loss, withdrawal of : Fever, GI loss, withdrawal of diuretic, change in high-sodium diet diuretic, change in high-sodium diet formulationformulation
Hypotonic fluid administrationHypotonic fluid administration : oral : oral or IV routeor IV route
0.9% NaCl should be avoided 0.9% NaCl should be avoided unless unless circulatory failurecirculatory failure

Hypotonic fluid Hypotonic fluid administrationadministration
Give the hypotonic fluid of which the patients have Give the hypotonic fluid of which the patients have lostlost
Pure water insensible loss (Fever, respiratory) = Pure water insensible loss (Fever, respiratory) = pure waterpure water
GI or skin loss = hypotonic saline eg. 0.45% NaClGI or skin loss = hypotonic saline eg. 0.45% NaCl
Oral route can be pure waterOral route can be pure water
IV route = 5% dextrose in water, 0.2% NaCl, 0.45% IV route = 5% dextrose in water, 0.2% NaCl, 0.45% NaClNaCl

Calculation of water Calculation of water deficit deficit
N Engl J Med 2000;342:1493-9

Calculation of water Calculation of water deficit deficit
Example of calculationExample of calculation
Hypernatremic 60 kg. man with [NaHypernatremic 60 kg. man with [Na++] 158 mmol/L was ] 158 mmol/L was considered to correct his sodium with IV 0.45% NaClconsidered to correct his sodium with IV 0.45% NaCl
Change in [NaChange in [Na++] with 1 litre of 0.45% NaCl in this ] with 1 litre of 0.45% NaCl in this patient patient ==
(infusate Na(infusate Na++ - serum Na - serum Na++)/TBW+1 = (77-158)/(0.6))/TBW+1 = (77-158)/(0.6)(60)+1(60)+1
= -2.16 mmol/L= -2.16 mmol/L
And, we want to correct his [NaAnd, we want to correct his [Na++] down to 150 mmol/L ] down to 150 mmol/L in 24 hours (Δ 8 mmol/L). So, in 24 hours, we have to in 24 hours (Δ 8 mmol/L). So, in 24 hours, we have to give him 8/2.16 give him 8/2.16 ≅≅3.7 litre of 0.45% NaCl3.7 litre of 0.45% NaCl, the rate is , the rate is 154 ml/hr154 ml/hr

Calculation of water Calculation of water deficit deficit
Traditional formula can be used :Traditional formula can be used :
water deficit = (total body water) X (1-water deficit = (total body water) X (1-[140÷serum sodium concentration]) [140÷serum sodium concentration])
But can But can underestimate in the case of hypotonic underestimate in the case of hypotonic fluid lossfluid loss
The o.5 mmol/L/hour is the same rule for The o.5 mmol/L/hour is the same rule for hyponatremia to avoid cerebral edema from hyponatremia to avoid cerebral edema from rapid decrease in [Narapid decrease in [Na++]]
Serial monitoring of serum [NaSerial monitoring of serum [Na++]]

Potassium [KPotassium [K++] ] homeostasishomeostasis
Important in function of muscle and nerve Important in function of muscle and nerve conductivityconductivity
Most intracellular, 2% in the extracellular Most intracellular, 2% in the extracellular compartmentcompartment
Normal serum concentration of [KNormal serum concentration of [K++] 3.5 – 5 ] 3.5 – 5 mmol/L mmol/L
Potassium handling 90% by kidneyPotassium handling 90% by kidney
Patients with impaired renal function are at risk Patients with impaired renal function are at risk of hyperkalemiaof hyperkalemia
HyperkalemiaHyperkalemia
Serum K concentration Serum K concentration > 5 mmol/L > 5 mmol/L
mild hyperkalemia 5-5.9 mmol/Lmild hyperkalemia 5-5.9 mmol/L
moderate 6.0-7.0 mmol/Lmoderate 6.0-7.0 mmol/L
severe ≥ 7.0 mmol/L severe ≥ 7.0 mmol/L
≥ ≥ 10 mmol/L usually fatal10 mmol/L usually fatal
Circulation 2005; 112: IV-121-IV-125

HyperkalemiaHyperkalemia

Signs and Symptoms of Signs and Symptoms of HyperkalemiaHyperkalemia
Muscle weakness, flaccid paralysis, Muscle weakness, flaccid paralysis, paraesthesia, depressed deep tendon paraesthesia, depressed deep tendon reflexes or respiratory distressreflexes or respiratory distress
May be overlooked as a symptom in patient May be overlooked as a symptom in patient with underlying diseaseswith underlying diseases
Asymptomatic patient still life-threatenedAsymptomatic patient still life-threatened
Patients with suspicious clinical background Patients with suspicious clinical background of hyperkalemia must be checked for serum of hyperkalemia must be checked for serum [K[K++] and EKG ] and EKG

EKG abnormalities of EKG abnormalities of HyperkalemiaHyperkalemia
Cardiac presentation : EKG abnormality, arrhythmia, Cardiac presentation : EKG abnormality, arrhythmia, cardiac arrestcardiac arrest
Depends on level and rate of increase in [KDepends on level and rate of increase in [K++]]
Earliest EKG change started when [KEarliest EKG change started when [K++] > 5.5 mmol/L ] > 5.5 mmol/L = =
Symmetrical tall peaked T wave (only 20% of Symmetrical tall peaked T wave (only 20% of patients)patients)11
EKG usually changes when [KEKG usually changes when [K++] > 6.7 mmol/L] > 6.7 mmol/L
1. Br Med J 2002;324:1320-4

EKG abnormalities of EKG abnormalities of HyperkalemiaHyperkalemia

EKG abnormalities of EKG abnormalities of HyperkalemiaHyperkalemia
Tall peaked T wave
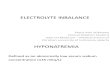
EKG abnormalities of EKG abnormalities of HyperkalemiaHyperkalemia
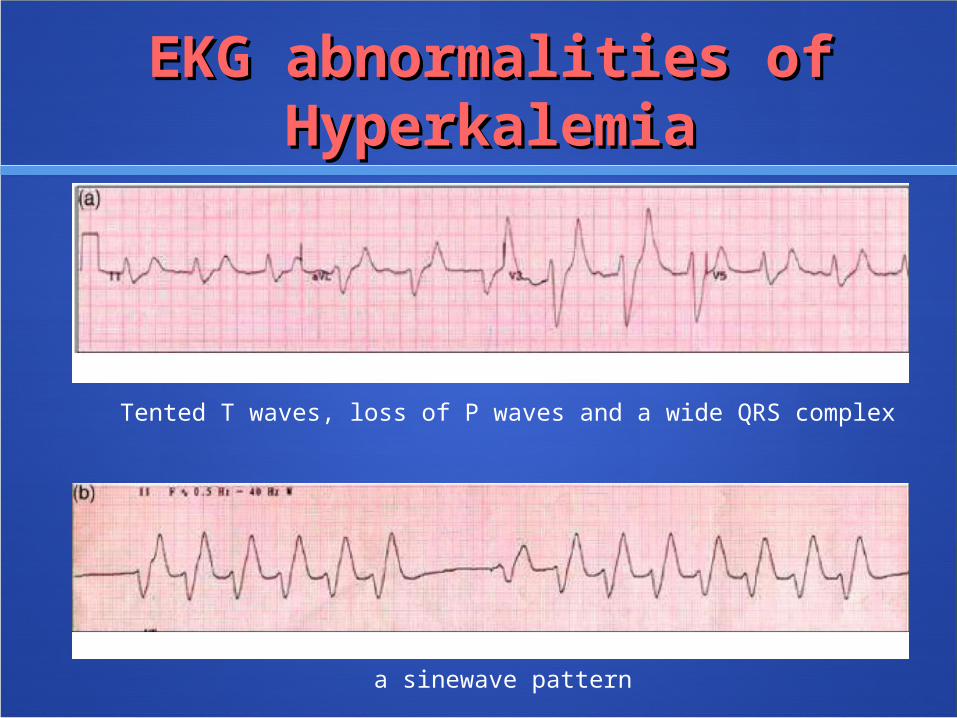
Tented T waves, loss of P waves and a wide QRS complex
a sinewave pattern

EKG abnormalities of EKG abnormalities of HyperkalemiaHyperkalemia
Severe bradycardia
Ventricular tachycardia

Arrhythmia from Arrhythmia from hyperkalemiahyperkalemia
Bradycardia may be unresponsive to Bradycardia may be unresponsive to transcutaneous, transvenous and atropine, even transcutaneous, transvenous and atropine, even in the patient with permanent pacemaker in the patient with permanent pacemaker 11
Calcium can worsen the bradyarrhythmia to Calcium can worsen the bradyarrhythmia to asystole asystole 22
Asystolic cardiac arrest due to hyperkalaemia is Asystolic cardiac arrest due to hyperkalaemia is usually fatal if the serum potassium is not usually fatal if the serum potassium is not returned to normal returned to normal 33
Hemodialysis during CPR had been reported to Hemodialysis during CPR had been reported to successful results successful results 4,5,64,5,6 1. Resuscitation 2004;62:119-20
2. Semin Dial 2000;13:279-803. Am Heart J 1974;88:360-714. Inten Care Med 1989;15:325-65. Crit Care Med 1981;9:556-76. Intensive Care Med 1994;20:287-90

Treatment of Treatment of hyperkalemiahyperkalemia
Calcium chloride and calcium gluconateCalcium chloride and calcium gluconate
- Antagonize cardiac membrane excitability - Antagonize cardiac membrane excitability
- Prevention arrhythmia in life-threatening ECG - Prevention arrhythmia in life-threatening ECG changechange
- 10% calcium chloride 10 ml (Calcium 6.8 - 10% calcium chloride 10 ml (Calcium 6.8 mmol) mmol)
- 10% calcium gluconate 10 ml- 10% calcium gluconate 10 ml (Calcium 2.2 (Calcium 2.2 mmol)mmol)
- may need higher dose- may need higher dose
- Efficacy of Calcium <- Efficacy of Calcium < 1 hour 1 hour

Treatment of Treatment of hyperkalemiahyperkalemia
Insulin/glucose, Sodium bicarbonate, Beta Insulin/glucose, Sodium bicarbonate, Beta agonistagonist
- K- K++ shifting to intracellular compartment shifting to intracellular compartment
- Insulin/Glucose- Insulin/Glucose lower K 0.65-1 mmol/L in 60 lower K 0.65-1 mmol/L in 60 minmin
- Sodium bicarbonate is less efficient than- Sodium bicarbonate is less efficient than insulin/glucose andinsulin/glucose and beta agonist and in the beta agonist and in the patient without acidosispatient without acidosis 1 1
- Insulin/50% glucose : 10 units IV/ 25 grams - Insulin/50% glucose : 10 units IV/ 25 grams glucoseglucose
- Sodium bicarbonate : 1 mmol/kg IV- Sodium bicarbonate : 1 mmol/kg IV
- Salbutamol : 0.5 mg IV/ 20 mg NB- Salbutamol : 0.5 mg IV/ 20 mg NB
1. Nephrol Dial Transplant 2003;18:2215-8

Treatment of Treatment of hyperkalemiahyperkalemia
Exchange resinsExchange resins
- Calcium or sodium polystyrene sulfonate- Calcium or sodium polystyrene sulfonate
- Slow onset (1-2 hours)- Slow onset (1-2 hours)
- Reports not significantly decrease [K- Reports not significantly decrease [K++]] 1,2 1,2
- 15-30 grams PO/PR- 15-30 grams PO/PR
1. Cochrane Database System Rev 2005;2(Issue). Art. No.: CD003235
2. J Am Soc Nephrol 1998;10:1924-30

Treatment of Treatment of hyperkalemiahyperkalemia
HemodialysisHemodialysis
- - The The most reliable most reliable method to lower method to lower serum potassium levelserum potassium level
- In life-threatening hyperkalemia, - In life-threatening hyperkalemia, hemodialysis must be emergently hemodialysis must be emergently scheduled despite administration scheduled despite administration potassium-lowering agentspotassium-lowering agents

Indication for emergency Indication for emergency hemodialysis in hemodialysis in hyperkalemiahyperkalemia
Severe hyperkalemia with impaired Severe hyperkalemia with impaired renal functionrenal function
Life-threatening arrhythmia from Life-threatening arrhythmia from hyperkalemia unresponsive to hyperkalemia unresponsive to medical treatmentmedical treatment J Crit Care 2006;21: 316-21

Indication for hospital Indication for hospital admission in admission in hyperkalemiahyperkalemia
EKG abnormalities other than peaked EKG abnormalities other than peaked T waveT wave
Severe hyperkalemia (> 8 mmol/L)Severe hyperkalemia (> 8 mmol/L)
Renal failureRenal failure
Medical comorbiditiesMedical comorbiditiesArch Intern Med 2000;160: 1605-11
HypokalemiaHypokalemia
Serum KSerum K++ ≤ ≤ 3.5 mmol/L 3.5 mmol/L
mild 3.0 -3.5 mild 3.0 -3.5 mmol/Lmmol/L
moderate 2.5 - 3.0 moderate 2.5 - 3.0 mmol/Lmmol/L
severe < 2.5 severe < 2.5 mmol/Lmmol/L

Causes of hypokalemiaCauses of hypokalemia
Resuscitation 2006;70: 10-25

Signs and Symptoms of Signs and Symptoms of hypokalemiahypokalemia
Fatigue, weakness, leg cramps, Fatigue, weakness, leg cramps, constipationconstipation
In severe cases, rhabdomyolysis, In severe cases, rhabdomyolysis, ascending paralysis and respiratory ascending paralysis and respiratory difficulties difficulties

EKG abnormalities in EKG abnormalities in hypokalemiahypokalemia
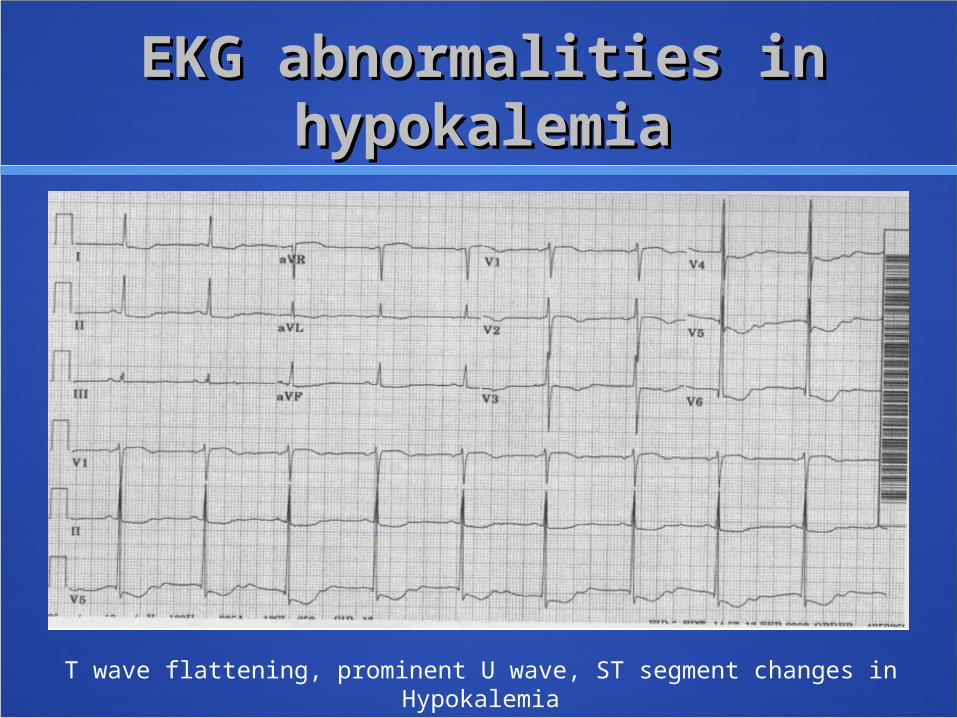
T wave flattening, prominent U T wave flattening, prominent U wave, ST segment changes wave, ST segment changes
Long QT interval, Torsade de Long QT interval, Torsade de pointes, VT orpointes, VT or VFVF
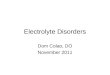
EKG abnormalities in EKG abnormalities in hypokalemiahypokalemia
T wave flattening, prominent U wave, ST segment changes in Hypokalemia

EKG abnormalities in EKG abnormalities in hypokalemiahypokalemia
Prominent U wave (arrow) in hypokalemia

Treatment of Treatment of hypokalemiahypokalemia
The causes of hypokalemia must be correctedThe causes of hypokalemia must be corrected
Adequate rehydration Adequate rehydration in renal or GI potassium in renal or GI potassium lossloss
Serum KSerum K+ + decreases 0.3 mmol/L in every 100 decreases 0.3 mmol/L in every 100 mmol of total body potassium storagemmol of total body potassium storage, depends , depends on patient’s body masson patient’s body mass 1 1
In non-life-threatening condition, serum KIn non-life-threatening condition, serum K++ should be gradually corrected orally or should be gradually corrected orally or intravenously, guided by serum Kintravenously, guided by serum K+ + monitoringmonitoring
Should be very careful in patient with impaired Should be very careful in patient with impaired renal functionrenal function 1. New Eng J Med 1998;339:451-8

Treatment of Treatment of hypokalemiahypokalemia
Maximal recommended intravenous dose = 20 Maximal recommended intravenous dose = 20 mmol/hourmmol/hour
In unstable arrhythmia, KIn unstable arrhythmia, K++ can be given can be given 2 mmol/min 2 mmol/min in 10 minutes, followed by 10 mmol in 5-10 minutesin 10 minutes, followed by 10 mmol in 5-10 minutes
In cardiac arrest due to hypokalemia, KIn cardiac arrest due to hypokalemia, K++ can be can be given given 20 mmol over 2-3 minutes20 mmol over 2-3 minutes, followed by 1 , followed by 1 minute bolus of MgSOminute bolus of MgSO44
Magnesium sulfate (MgSOMagnesium sulfate (MgSO44) 1-2 grams should be ) 1-2 grams should be given without laboratory confirmation given without laboratory confirmation
(8 mmol of elemental Mg = 1 gram of MgSO(8 mmol of elemental Mg = 1 gram of MgSO44))
Resuscitation 2006;70: 10-25

Calcium homeostasisCalcium homeostasis
Parathyroid hormone (PTH) and vitamin DParathyroid hormone (PTH) and vitamin D
PTH PTH increase Ca increase Ca2+ 2+ by increase GI absorption by increase GI absorption and bone resorptionand bone resorption
Active vitamin D (1α,25(OH)Active vitamin D (1α,25(OH)22DD33) ) increase increase CaCa2+2+ and PO and PO44
3- 3- absorption of small intestineabsorption of small intestine
Increasing level of CaIncreasing level of Ca2+2+ and vitamin D level has and vitamin D level has negative feedback to suppress PTH secretionnegative feedback to suppress PTH secretion
Normal serum CaNormal serum Ca2+ 2+ level 8 – 10 mg/dL (2.1 – 2.6 level 8 – 10 mg/dL (2.1 – 2.6 mmol/L)mmol/L)

HypercalcemiaHypercalcemia
Serum calcium >Serum calcium > 10 mg/dL 10 mg/dL
Mild hypercalcemia < 12 mg/dLMild hypercalcemia < 12 mg/dL
Moderate hypercalcemia 12-14 Moderate hypercalcemia 12-14 mg/dLmg/dL
Severe hypercalcemia > 14 mg/dLSevere hypercalcemia > 14 mg/dL

Signs and Symptoms of Signs and Symptoms of hypercalcemiahypercalcemia
nausea, vomiting, anorexia, weakness, nausea, vomiting, anorexia, weakness, constipation 0rconstipation 0r alteration of mental alteration of mental statusstatus
Can be mimic the symptoms of Can be mimic the symptoms of patient’s malignancy patient’s malignancy
polyuria, nocturia orpolyuria, nocturia or dehydration dehydration
Sometimes patients can be presented Sometimes patients can be presented as acute pancreatitis or peptic ulcer as acute pancreatitis or peptic ulcer

Causes of Causes of hypercalcemiahypercalcemia
Increase bone resorptionIncrease bone resorption
Primary hyperparathypoidism, Hypercalcemia Primary hyperparathypoidism, Hypercalcemia of malignancy, hyperthyroidism, Paget’s of malignancy, hyperthyroidism, Paget’s diseasedisease
Increase intestinal absorptionIncrease intestinal absorption
Renal failure (often with vitamin D Renal failure (often with vitamin D supplementation), Milk-alkaline syndrome, supplementation), Milk-alkaline syndrome, Hypervitaminosis D (Chronic granulomatous Hypervitaminosis D (Chronic granulomatous disease, lymphoma, increase intake of vitD)disease, lymphoma, increase intake of vitD)
MiscellaneousMiscellaneous : thiazide, lithium toxicity, : thiazide, lithium toxicity, immobilization, TPN, Familial hypocalciuric immobilization, TPN, Familial hypocalciuric hypercalcemiahypercalcemia

Differential diagnosis of Differential diagnosis of hypercalcemiahypercalcemia
History : malignancy, drugs eg. Thiazide, History : malignancy, drugs eg. Thiazide, lithium, renal failure, urolithiasis etc.lithium, renal failure, urolithiasis etc.
Serum PTH level Serum PTH level
Emergency treatment of Emergency treatment of hypercalcemiahypercalcemia
general supportive care andgeneral supportive care and treatment of primary diseasetreatment of primary disease
RehydrationRehydration
Enhancement of renal calcium Enhancement of renal calcium excretionexcretion
Inhibition of bone resorption Inhibition of bone resorption

Emergency treatment ofEmergency treatment ofhypercalcemiahypercalcemia
Rev Endocr Metab Disord. 2003; 4: 167-75
Emergency treatment ofEmergency treatment ofhypercalcemiahypercalcemia
RehydrationRehydration
- Hypercalcemic patients always dehydrate- Hypercalcemic patients always dehydrate
- 0.9% NaCl 3,000 ml/day (up to 6,000)- 0.9% NaCl 3,000 ml/day (up to 6,000)
- Promote urine flow to increase urinary Ca- Promote urine flow to increase urinary Ca2+ 2+
excretionexcretion
- Should be careful in elderly patient or that - Should be careful in elderly patient or that with with
cardiovascular problems cardiovascular problems

Emergency treatment ofEmergency treatment ofhypercalcemiahypercalcemia
Enhancement of urinary calcium Enhancement of urinary calcium excretionexcretion
Loop diuretic : furosemide 20-120 Loop diuretic : furosemide 20-120 mg every 2-6 hoursmg every 2-6 hours
Complication : volume depletion, Complication : volume depletion, hypokalemia, hypomagnesemia hypokalemia, hypomagnesemia

Emergency treatment ofEmergency treatment ofhypercalcemiahypercalcemia
Inhibit bone resorptionInhibit bone resorption
Calcitonin 4 -8 IU/kg IM or SQCalcitonin 4 -8 IU/kg IM or SQ
onset 2-4 hoursonset 2-4 hours
Indicated in patients who cannot tolerate Indicated in patients who cannot tolerate large volume expansion or moderate to large volume expansion or moderate to severe hypercalcemiasevere hypercalcemia
Tachyphylaxis and hypersensitivity Tachyphylaxis and hypersensitivity

Emergency treatment ofEmergency treatment ofhypercalcemiahypercalcemia
BisphosphonatesBisphosphonates
Pamidronate 90 mg or Zoledronate 4 mg Pamidronate 90 mg or Zoledronate 4 mg
High potency but slow onset (48 hours)High potency but slow onset (48 hours)
Moderate to severe hypercalcemiaModerate to severe hypercalcemia
Adjusted with decrease in renal functionAdjusted with decrease in renal function
Nausea/vomiting, flu-like symptoms, Nausea/vomiting, flu-like symptoms, hypophosphatemia hypophosphatemia
EmergencyEmergency treatmenttreatment ofofhypercalcemiahypercalcemia
Reduction of intestinal calcium Reduction of intestinal calcium absorptionabsorption
Inhibit vitamin D Inhibit vitamin D
Prednisolone 40-100 mg OD orPrednisolone 40-100 mg OD or Dexamethasone 4-8 mg bidDexamethasone 4-8 mg bid / tid/ tid
Only hypercalcemia from Only hypercalcemia from lymphoproliferative orlymphoproliferative or granulomatous granulomatous diseasedisease
GI hemorrhage, hyperglycemia, GI hemorrhage, hyperglycemia, osteoporosis orosteoporosis or Cushing’s syndrome Cushing’s syndrome

HypocalcemiaHypocalcemia
Serum calcium < 8 mg/dLSerum calcium < 8 mg/dL
Corrected calcium = Serum Corrected calcium = Serum calcium + 0.8[4-serum albumin calcium + 0.8[4-serum albumin (g/L)](g/L)]

CausesCauses ofof hypocalcemiahypocalcemia

SignsSigns andand SymptomsSymptoms ofof hypocalcemiahypocalcemia
Increase neuroexcitibilityIncrease neuroexcitibility :: tingling, numbness, tingling, numbness, muscle twitching and spasms muscle twitching and spasms
In severe cases, tetany, seizure orIn severe cases, tetany, seizure or cardiac cardiac arrhythmiasarrhythmias
Symptoms depend on rate of decrease in CaSymptoms depend on rate of decrease in Ca2+2+. . Patients can be asymtomatic even very low Patients can be asymtomatic even very low serum Caserum Ca2+2+
Some can present with phychiatric symptoms, Some can present with phychiatric symptoms, cataract, increase intracranial pressure or bone cataract, increase intracranial pressure or bone pain pain

SignsSigns andand SymptomsSymptoms ofof hypocalcemiahypocalcemia
Positive Chvostek’sPositive Chvostek’s
More specific = Trousseau’s sign More specific = Trousseau’s sign
Chvostek’s sign
Trousseau’s sign
Br Med J 2008;336;1298-1302

Treatment of Treatment of hypocalcemiahypocalcemia
No need for emergency treatment if No need for emergency treatment if asymptomatic asymptomatic unless the level is less than 7.3 unless the level is less than 7.3 mg/dL (1.9 mmol/L)mg/dL (1.9 mmol/L)
Need for emergency treatment if symptomatic Need for emergency treatment if symptomatic ::
- General supportive care- General supportive care
- EKG monitoring- EKG monitoring
- Threatening condition to airway – laryngeal - Threatening condition to airway – laryngeal spasmspasm
- Calcium replacement - Calcium replacement Br Med J 2008;336;1298-1302

Calcium replacement for Calcium replacement for hypocalcemiahypocalcemia
Calcium gluconate or calcium chlorideCalcium gluconate or calcium chloride
Less irritation in gluconate formLess irritation in gluconate form
10 ml Calcium gluconate 1-2 ampoules diluted in 10 ml Calcium gluconate 1-2 ampoules diluted in 50-100 ml of 5% dextrose solution slowly infused in 50-100 ml of 5% dextrose solution slowly infused in 10 minutes10 minutes
Repeat until the symptoms disappearRepeat until the symptoms disappear
Maintenance dose : 10 ml of calcium gluconate 10 Maintenance dose : 10 ml of calcium gluconate 10 ampoules in 5%dextrose orampoules in 5%dextrose or 0.9% saline rate 50 0.9% saline rate 50 ml/hour ml/hour
Aim to raise [CaAim to raise [Ca2+2+]] in the lower end of normal range in the lower end of normal range Br Med J 2008;336;1298-1302Oxford textbook of medicine. 4th ed. Oxford: Oxford University Press, 2003

HypomagnesemiaHypomagnesemia
Concomitant electrolyte Concomitant electrolyte abnormalities with hypokalemia and abnormalities with hypokalemia and hypocalcemiahypocalcemia
Neuromuscular system and cardiac Neuromuscular system and cardiac arrhythmiaarrhythmia
Normal serum magnesium (MgNormal serum magnesium (Mg2+2+)) level level = 0.7 - 1.0 mmol/L (1.7-2.4 mg/dL) = 0.7 - 1.0 mmol/L (1.7-2.4 mg/dL)

Signs and symptoms of Signs and symptoms of hypomagnesemiahypomagnesemia
Sign and symptom of hypokalemia and Sign and symptom of hypokalemia and hypocalcemiahypocalcemia
Neuromuscular : tetany, carpo-pedal spasm, Neuromuscular : tetany, carpo-pedal spasm, seizure, weakness, psychosisseizure, weakness, psychosis
Cardiovascular : Dysrhythmias (VT and Cardiovascular : Dysrhythmias (VT and torsade de pointe) prolonged QT, prolonged torsade de pointe) prolonged QT, prolonged PR, ST depressionPR, ST depression

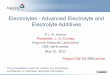
Dysrhythmias in Dysrhythmias in hypomagnesemiahypomagnesemia
QT prolongation (QTc = 0.513 msec)

Dysrhythmias in Dysrhythmias in hypomagnesemiahypomagnesemia
Torsade de pointes

Treatment of Treatment of hypomagnesemiahypomagnesemia
Symptomatic patient – need for emergency Symptomatic patient – need for emergency treatmenttreatment
Hypokalemia and hypocalcemia must be treated Hypokalemia and hypocalcemia must be treated simultaneouslysimultaneously
In seizures or arrhythmias : In seizures or arrhythmias :
MgSO4 1-2 grams (8-16 mEq of elemental Mg) MgSO4 1-2 grams (8-16 mEq of elemental Mg) inin 5-10 min.5-10 min. until symptoms disappearuntil symptoms disappear
Maintenance : 6 grams (48 mEq ofMaintenance : 6 grams (48 mEq of Mg) drip in Mg) drip in 24 hours24 hours to maintain [Mgto maintain [Mg2+2+] and] and restore body restore body total Mgtotal Mg2+2+ storage storage
Magnesium. 1989;8:201-212 J Intensive Care Med 2005; 20: 3-17
Treatment of Treatment of hypomagnesemiahypomagnesemia
Compatibility with certain calcium solutionCompatibility with certain calcium solution
Reduce half of the dosage in the renal failure Reduce half of the dosage in the renal failure patientpatient
[Mg[Mg2+2+] monitoring at lease once a day] monitoring at lease once a day
Mg toxicity in [MgMg toxicity in [Mg2+2+] > 3 – 4 mEq/L] > 3 – 4 mEq/L
hypotension, flushing, nausea, lethargy hypotension, flushing, nausea, lethargy และและ decreased deep tendon reflexes.decreased deep tendon reflexes. In severe In severe cases, respiratory compromise from muscle cases, respiratory compromise from muscle weakness orweakness or cardiac arrestcardiac arrest
Pharmacol Rev. 1977;29:273-300
J Intensive Care Med 2005; 20: 3-17