Embed Size (px)
Citation preview
T helper-17 cells
Jafar Ali
M.Phil 2nd
QUAID-i-AZAM UNIVERSITY ISLAMABAD
Th 17 cells
T helper 17 cells (Th17) are a subset of T helper cells producing interleukin 17 (IL-17)
discovered in 2007. distinct from Th1 and Th2 cells defence play a role in inflammation and tissue injury autoimmune disease such as multiple sclerosis Rheumatoid arthritis
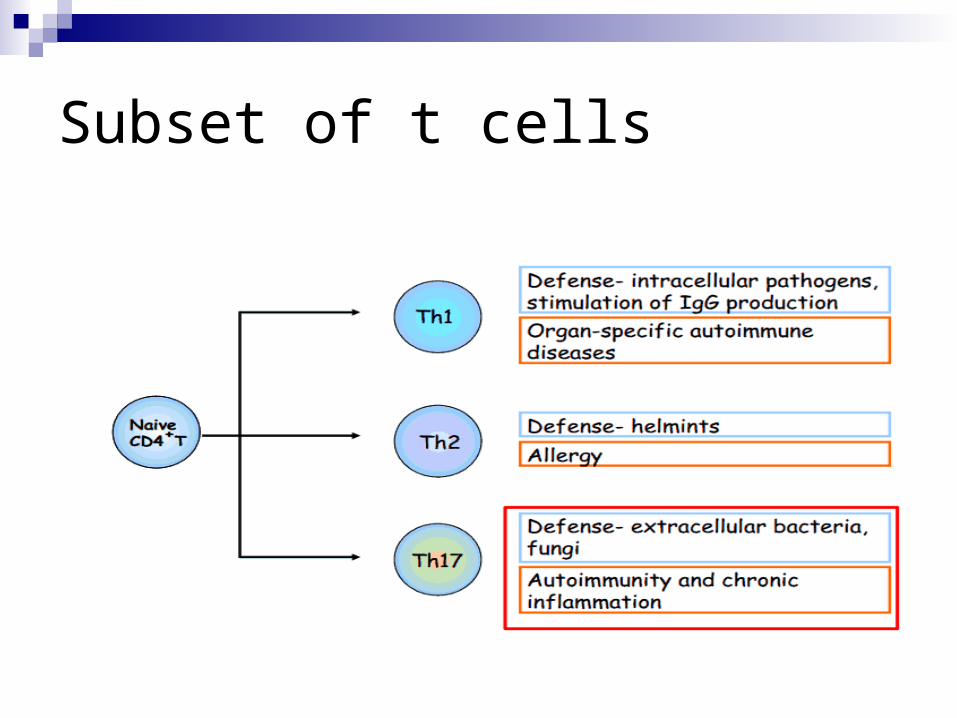
Subset of t cells
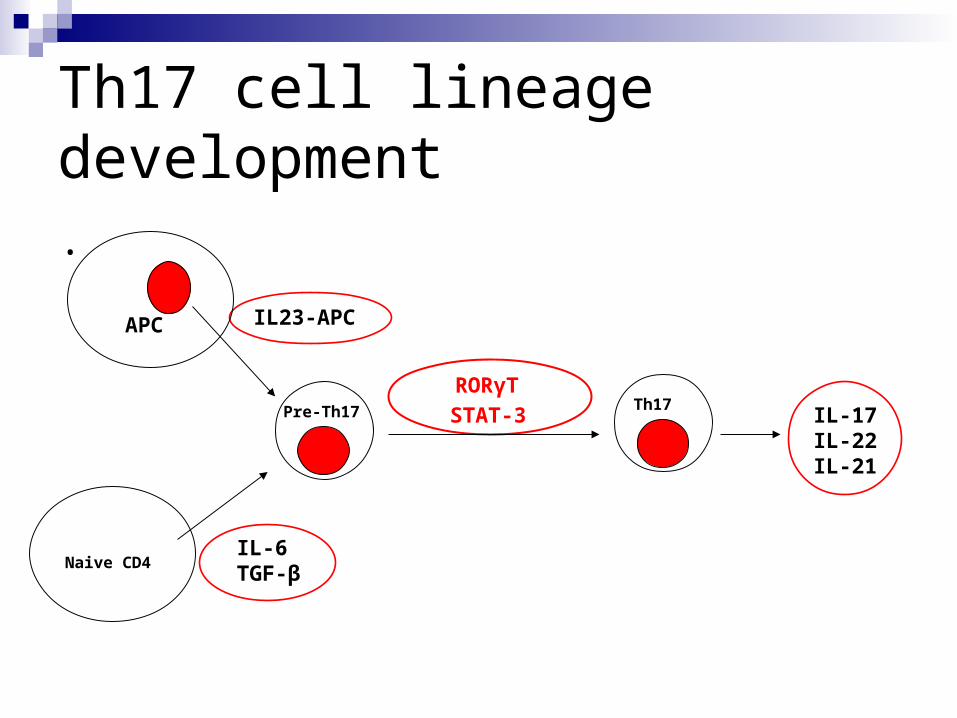
Th17 cell lineage development
.
RORγT
STAT-3
Naive CD4
APC
Th17 IL-17IL-22IL-21
IL23-APC
IL-6TGF-β
Pre-Th17
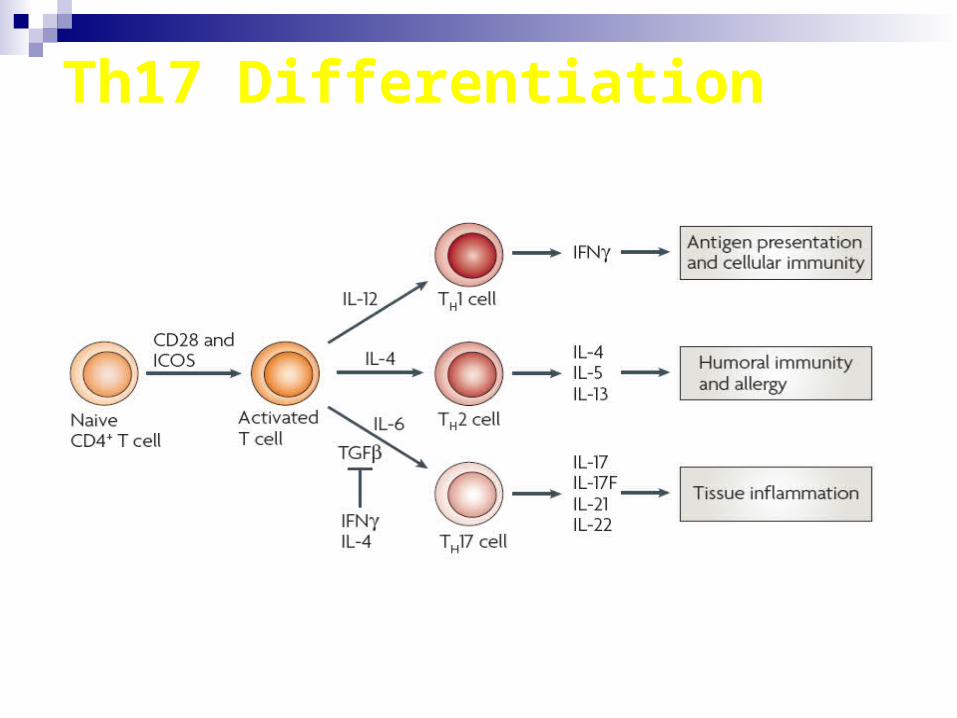
Th17 Differentiation
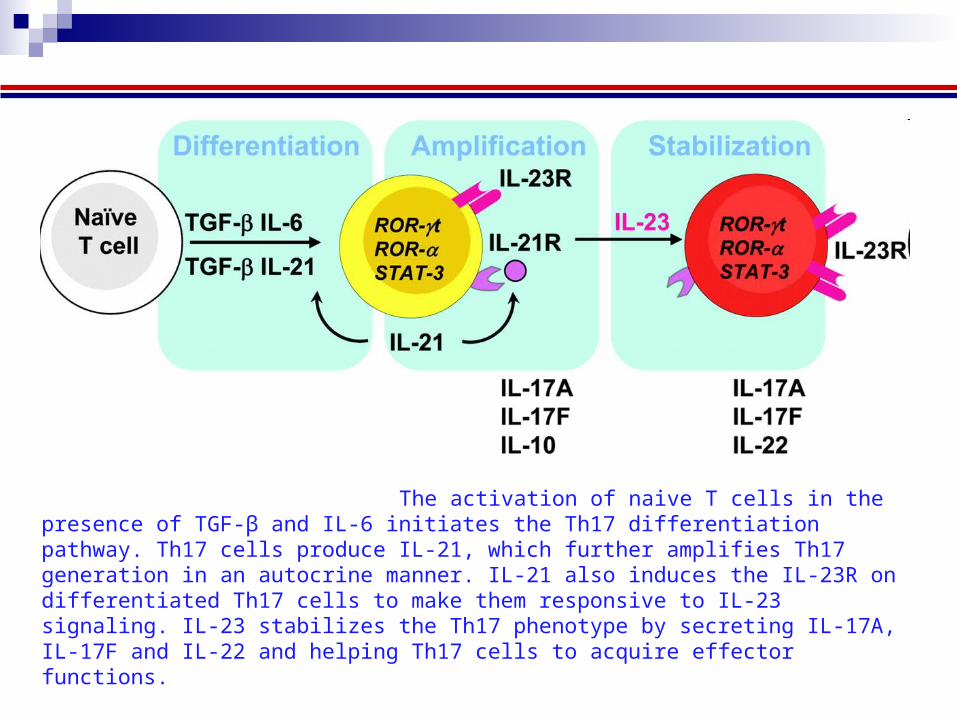
Steps in the generation of Th17 cells.
The activation of naive T cells in the presence of TGF-β and IL-6 initiates the Th17 differen The activation of naive T cells in the presence of TGF-β and IL-6 initiates the Th17 differentiation pathway. Th17 cells produce IL-21, which further amplifies Th17 generation in an autocrine manner. IL-21 also induces the IL-23R on differentiated Th17 cells to make them responsive to IL-23 signaling. IL-23 stabilizes the Th17 phenotype by secreting IL-17A, IL-17F and IL-22 and helping Th17 cells to acquire effector functions. h further amplifies Th17 generati
(Awasthi and Kuchroo, International Immunology, 2009)
Transcriptional regulation RORᴽt……….. necessary and sufficient to induce IL-17
expression ROR∞….. With RORᴽt promotes differntiation of Th 17
cells Runx1, to Il17 promoter and RORᴽt will give optimal IL-
17expression in CD4+ Interleukin regulatory factor 4 (IRF4)….. TH17 induction STAT3………… TH17 cell development and function
is also critically dependent
Disturbances in the homeostasis of Th17 lymphocytes in patients with hyper IgE syndrome (HIES) and chronic granulomatous disease (CGD)
Horvath R.1, Lastovicka J.1, Polouckova A.1, Sedlacek P.2, Bartunkova J.1, Sediva A.1, Spisek R.1
1Department of Immunology, Charles University, 2nd Medical School and Faculty Hospital Motol,
Prague, Czech Republic
Th 17 cell functions
Production of IL-17 cytokines family (IL-17, IL-21, IL-22) which leads to
the chemoattraction of neutrophils
Accumulating Th17 are highly pro - inflammatory and that Th17 cells
with specificity for self-antigens lead to severe autoimmunity- (psoriasis,
Crohn´s disease, multiple sclerosis)
Initially, from studies in mice, Th17 cells were thought to play an important
role in host defense against extracellular pathogens, which are not
efficiently cleared by Th1-type and Th2- type immunity
However, identity of pathogens cleared by Th17 was unknown
Direct evidence for understanding physiological target of Th17 cells came
from studies of patients with mutations in STAT-3, a critical transcription
factor for the differentiation of Th17 cells
Physiological role of Th17 cells in humans
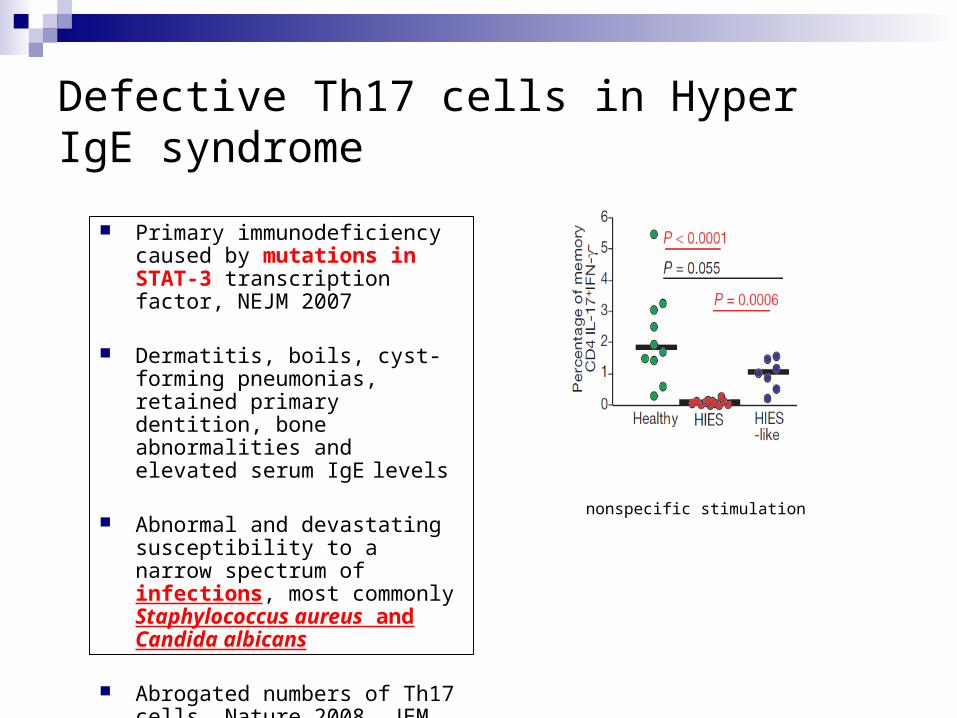
Defective Th17 cells in Hyper IgE syndrome
Primary immunodeficiency caused by mutations in STAT-3 transcription factor, NEJM 2007
Dermatitis, boils, cyst-forming pneumonias, retained primary dentition, bone abnormalities and elevated serum IgE levels
Abnormal and devastating susceptibility to a narrow spectrum of infections, most commonly Staphylococcus aureus and Candida albicans
Abrogated numbers of Th17 cells, Nature 2008, JEM 2008
nonspecific stimulation
Studies in Hyper IgE point to a critical role of Th17 cells in the response
against candidal and staphylococcal infections
However, there are other diseases with similar spectrum of dominant
pathogens where the characteristics of Th17 have not been tested
We thus decided to test Th17 cells compartment in chronic granulomatous
disease
Defective Th17 cells in Hyper IgE syndrome
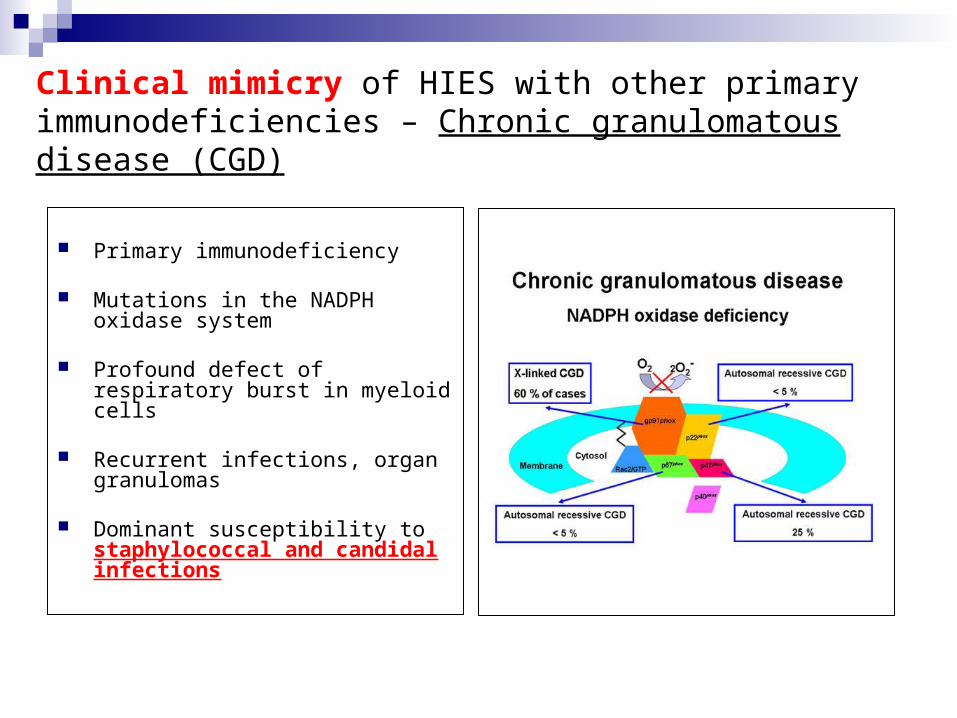
Clinical mimicry of HIES with other primary immunodeficiencies – Chronic granulomatous disease (CGD)
Primary immunodeficiency
Mutations in the NADPH oxidase system
Profound defect of respiratory burst in myeloid cells
Recurrent infections, organ granulomas
Dominant susceptibility to staphylococcal and candidal infections
Aim of the study
Analyze and compare the characteristics of Th17 compartment in
HIES and CGD patients
Patients and methods
4 patients from 3 families with HIES 7 patients with CGD (2 patients underwent allo-BMT) Mutations in STAT-3 and NADPH oxidase - genetics ELISA
0 102 103 104 105
0
102
103
104
105 4.12
0.51
0 102 103 104 105
0
102
103
104
105
0.13
1.67
0 102 103 104 105
0
102
103
104
105 2.32
1.98
0 102 103 104 105
0
102
103
104
105 5.91
0.49
0 102 103 104 105
0
102
103
104
105
0.078
3.5
0 102 103 104 105
0
102
103
104
105 1.25
2.87
0 102 103 104 105
0
102
103
104
105 6.51
0.76
0 102 103 104 105
0
102
103
104
105 6.97
0.36
0 102 103 104 105
0
102
103
104
105 1.91
1.55
0
0,5
1
1,5
2
2,5
3
3,5
Controls HIES CGD
% o
f IL
-17
+ C
D4
+ c
ell
s0
2
4
6
8
10
12
14
Controls HIES CGD%
of
IFN
ga
mm
a+
CD
4+
ce
lls
IFN
gam
ma
- P
E
IL-17 A647
Controls HIES CGD
AB
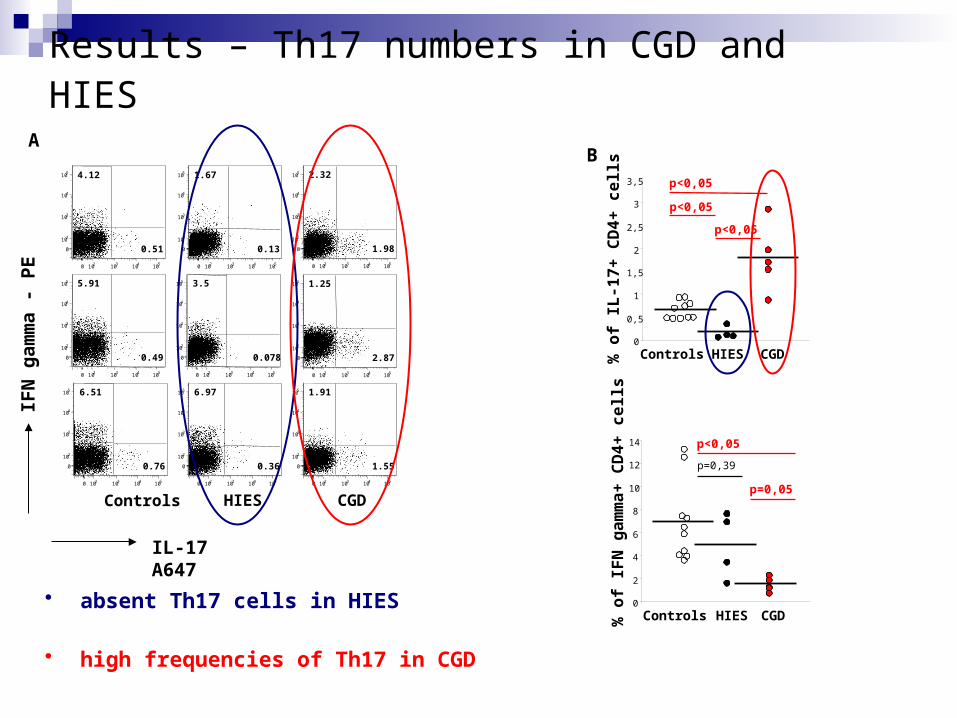
Results – Th17 numbers in CGD and HIES
p<0,05
p<0,05
p<0,05
p=0,39
p<0,05
p=0,05
• absent Th17 cells in HIES
• high frequencies of Th17 in CGD
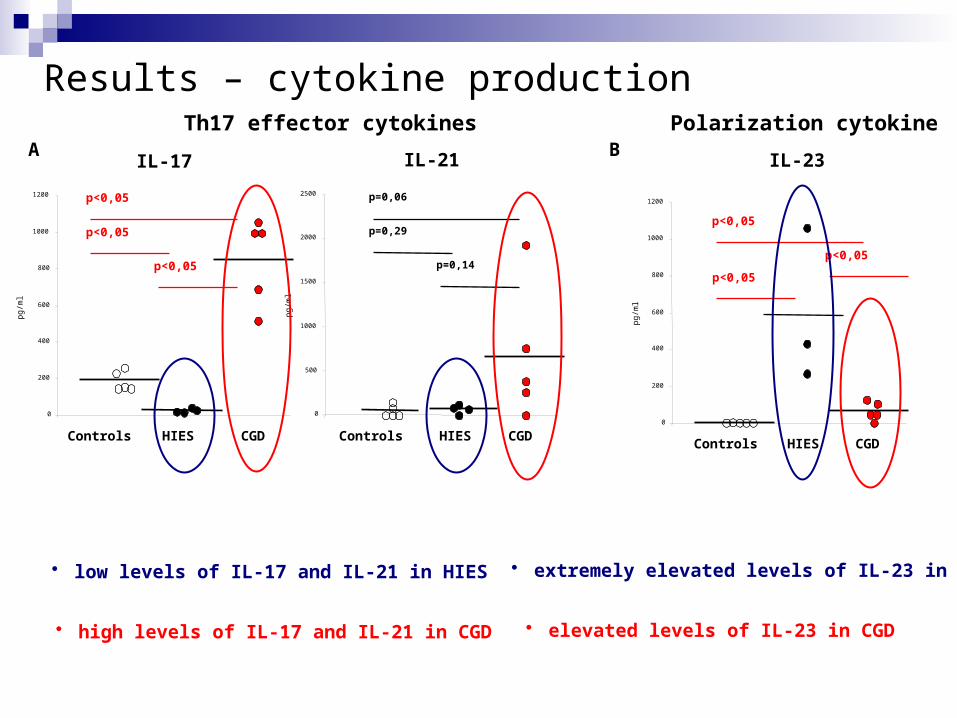
Results – cytokine production
IL-17
0
200
400
600
800
1000
1200
pg/
ml
Controls HIES CGD
A IL-21
0
500
1000
1500
2000
2500
pg/
ml
Controls HIES CGD
p<0,05
p<0,05
p<0,05
p=0,06
p=0,29
p=0,14
IL-23
0
200
400
600
800
1000
1200
pg/
ml
Controls HIES CGD
p<0,05
p<0,05
p<0,05
• low levels of IL-17 and IL-21 in HIES
B
• high levels of IL-17 and IL-21 in CGD
• extremely elevated levels of IL-23 in HIES
• elevated levels of IL-23 in CGD
Th17 effector cytokines Polarization cytokine
0 102 103 104 105
0
102
103
104
105
0.84
8.64
0 102 103 104 105
0
102
103
104
105
0.12
1.83
IFN
gam
ma
- P
E
IL-17 A647
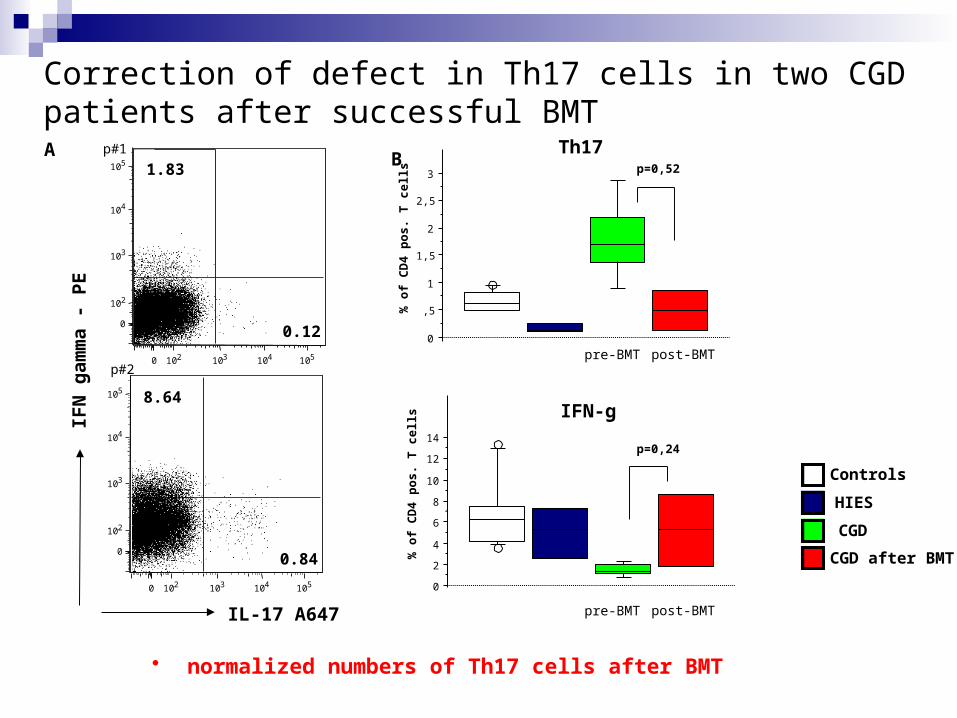
A
Correction of defect in Th17 cells in two CGD patients after successful BMT
0
,5
1
1,5
2
2,5
3
% o
f C
D4
po
s.
T c
ell
s
Th17
CGD
HIES
Controls
0
2
4
6
8
10
12
14
% o
f C
D4
po
s.
T c
ell
sIFN-g
Bp#1
p#2pre-BMT
pre-BMT
CGD after BMT
• normalized numbers of Th17 cells after BMT
p=0,52
p=0,24
post-BMT
post-BMT
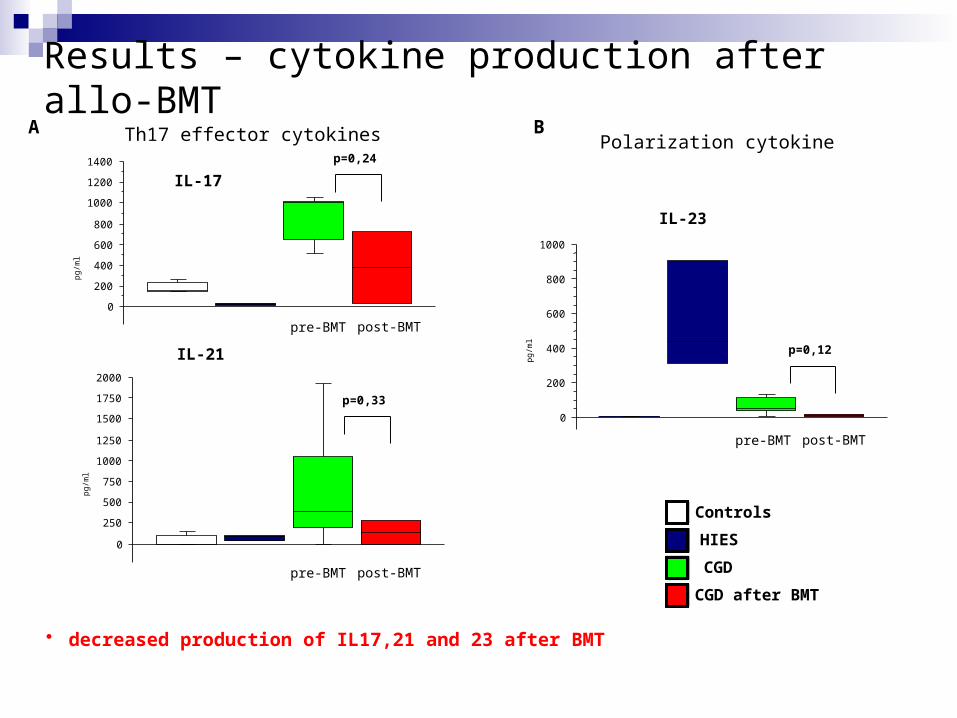
Results – cytokine production after allo-BMT
CGD
HIES
Controls
0
200
400
600
800
1000
1200
1400
pg/
ml
IL-17
0
250
500
750
1000
1250
1500
1750
2000
pg/
ml
IL-21
p=0,24
0
200
400
600
800
1000
pg/
ml
IL-23
A Th17 effector cytokines Polarization cytokineB
pre-BMT
pre-BMT
pre-BMT
CGD after BMT
p=0,33
p=0,12
• decreased production of IL17,21 and 23 after BMT
post-BMT
post-BMT
post-BMT
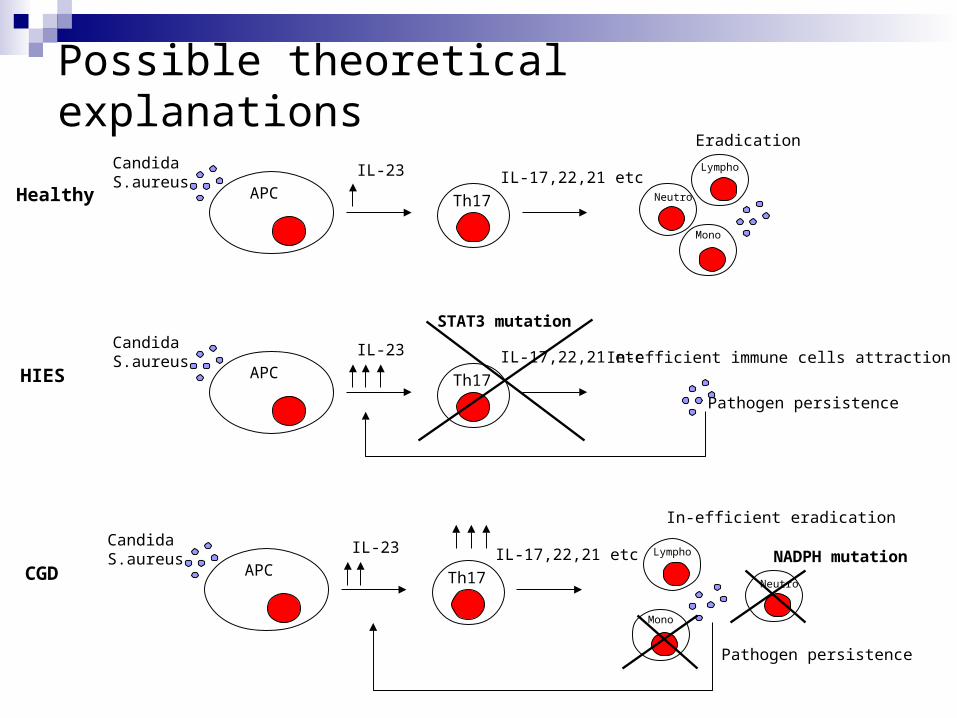
Possible theoretical explanations
Healthy Th17APC
IL-23 IL-17,22,21 etcNeutro
Lympho
Mono
Eradication
CandidaS.aureus
HIES Th17APC
IL-23 IL-17,22,21 etcCandidaS.aureus
STAT3 mutation
In-efficient immune cells attraction
Pathogen persistence
CGD Th17APC
IL-23 IL-17,22,21 etc
Neutro
Lympho
Mono
In-efficient eradication
CandidaS.aureus NADPH mutation
Pathogen persistence
Conclusions
We identified disturbances in the homeostasis of Th17 lymphocytes
in HIES and CGD patients
Absent Th17 cells in STAT-3 deficient HIES patients
Significantly higher frequencies of Th17 cells in CGD
Increase of Th17 cells in CGD is likely to be secondary as a result
of defect in neutrophils
BMT leads to the normalization of elevated Th17 cell numbers and
coresponding IL-17 production
Positive pro-inflammatory loop caused by Th17 cells contributes to
the formation of granulomas
These findings confirm the critical role of Th17 lymphocytes in the
elimination of candidal and staphylococcal infections