Embed Size (px)
Citation preview
SUPRASELLAR MASS: CT SCAN OF A CHILD
Dr Rekha Khare MD Radiology
CLINICAL PRESENTATION
A male child of about eight months was brought by his parents to CT room for head CT scan
Parents noticed the bulging of left eye for few weeks
Vision was poor/ blind left eye There was no other constitutional symptoms
CLINICAL EXAMINATION
Apparently child was found normal except PROPTOSIS Left eye
Routine laboratory exam were with in normal limit
COMMON CAUSES OF PROPTOSIS
V_ Vascular (arterio venous malformation) E_ Endocrinal ( thyrotoxicosis ) I_ Infection/ Inflammation N_ Neoplasm ( Primary/ Secondary ) ( Local/ Intracranial ) VEIN……
WHAT TO SEE ON CT SCAN?
eye ball eye muscles ( extra ocular ) retro bulbar space optic nerve bony socket adjoining paranasal sinus/ nasal cavity intracranial tissue
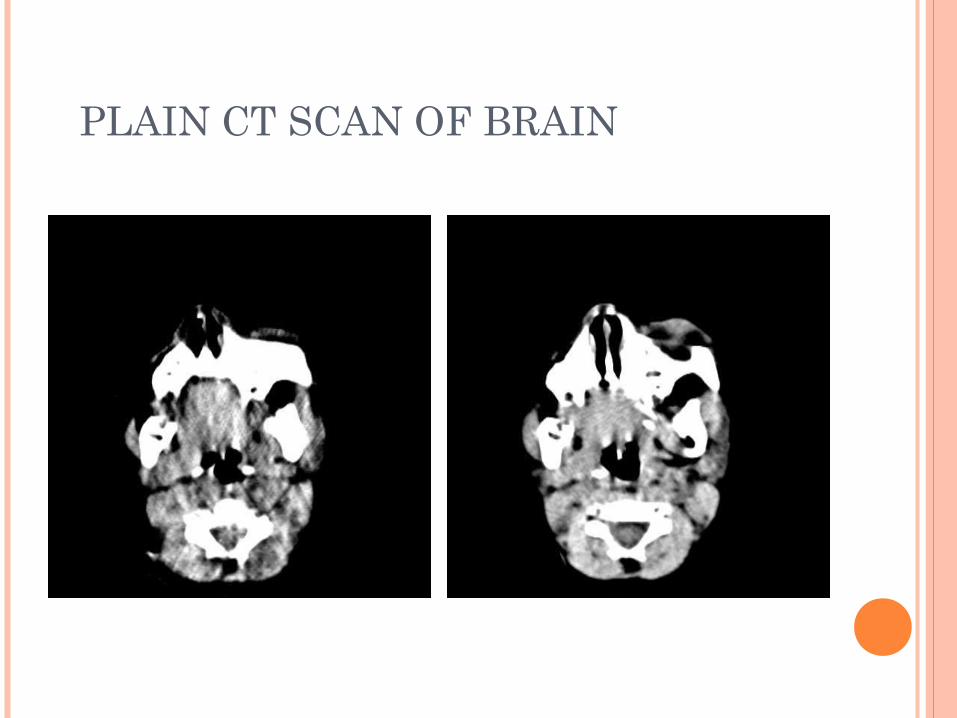
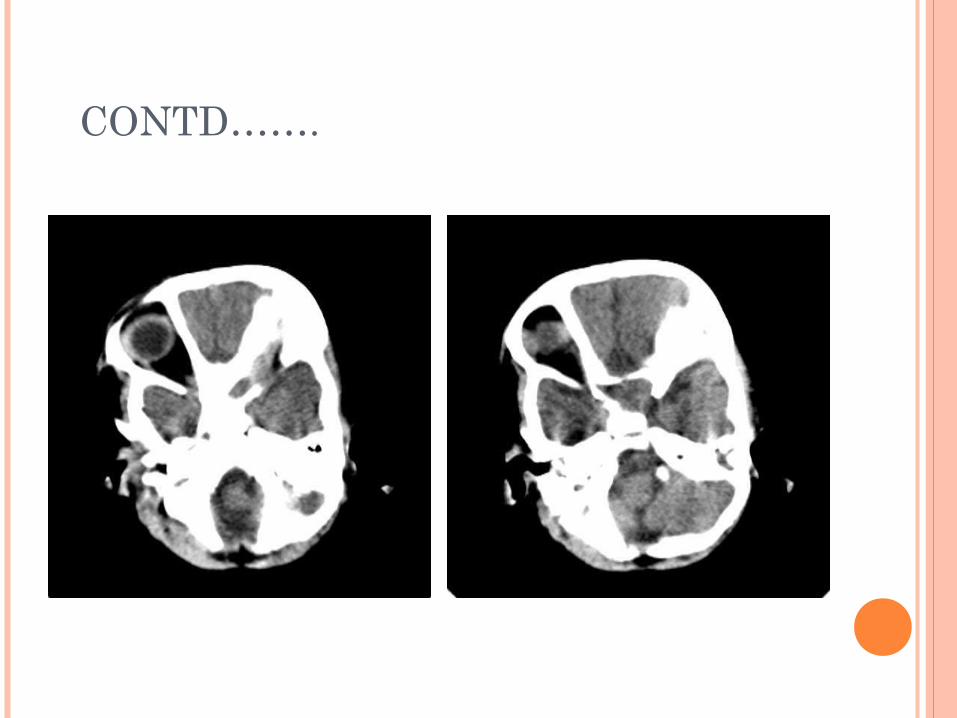
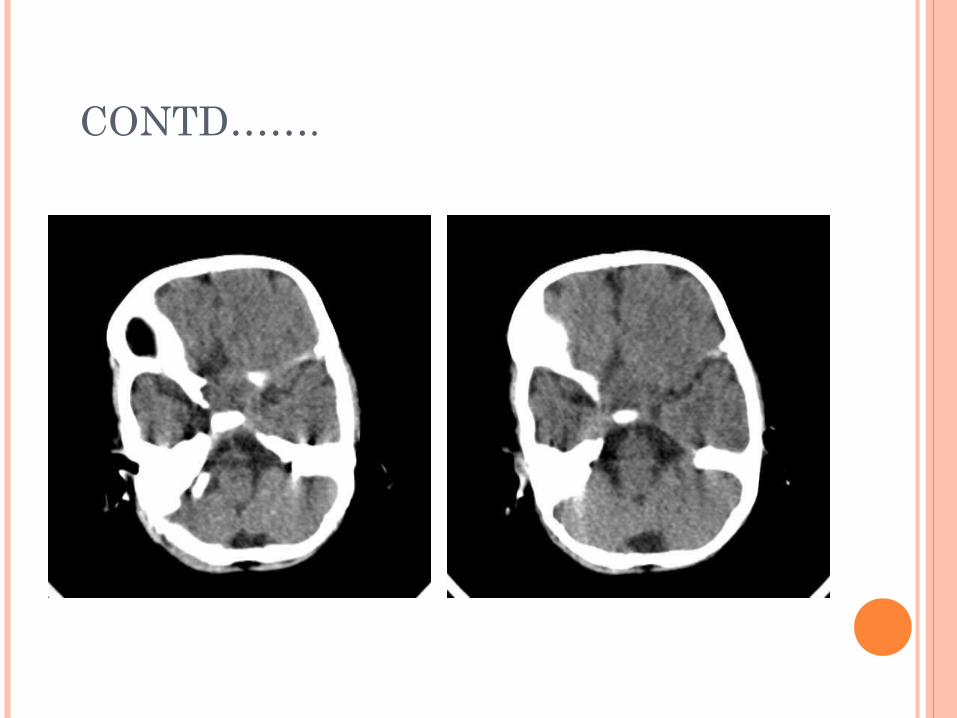
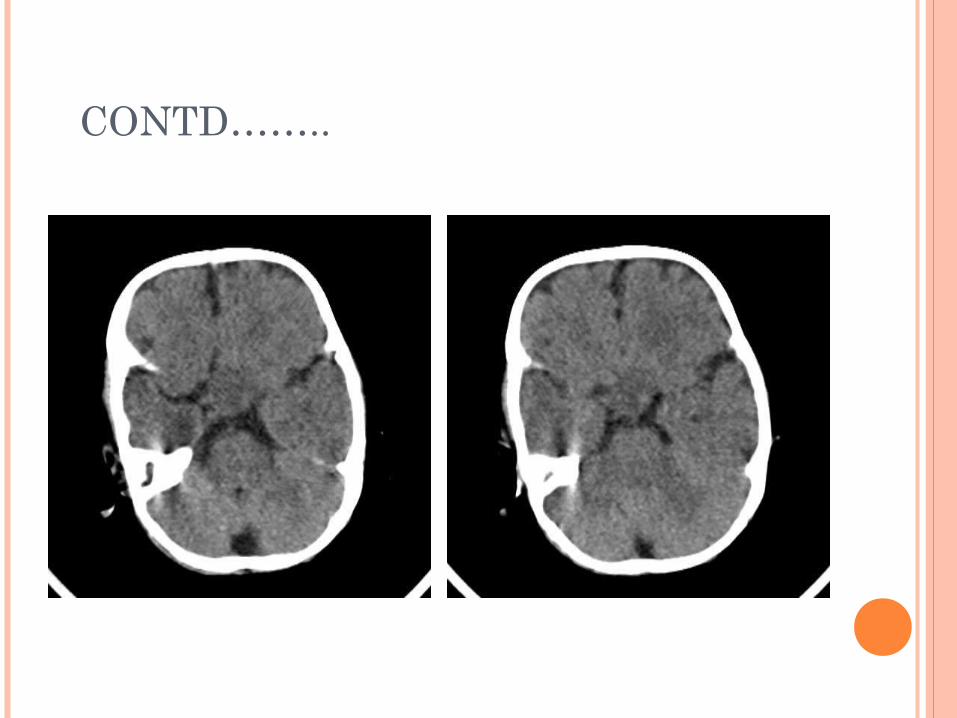
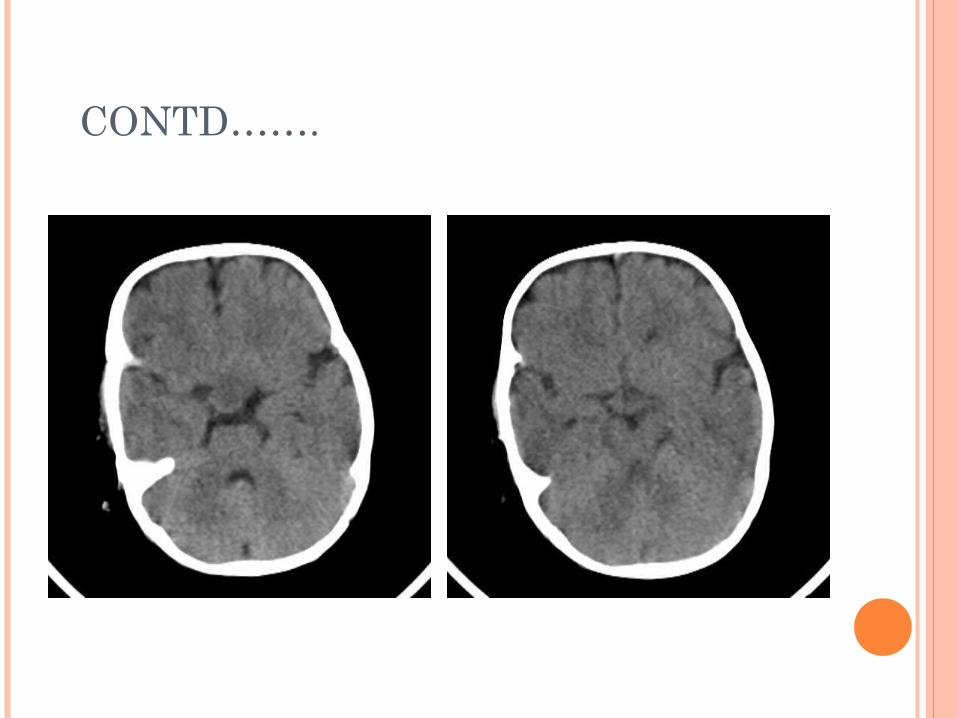
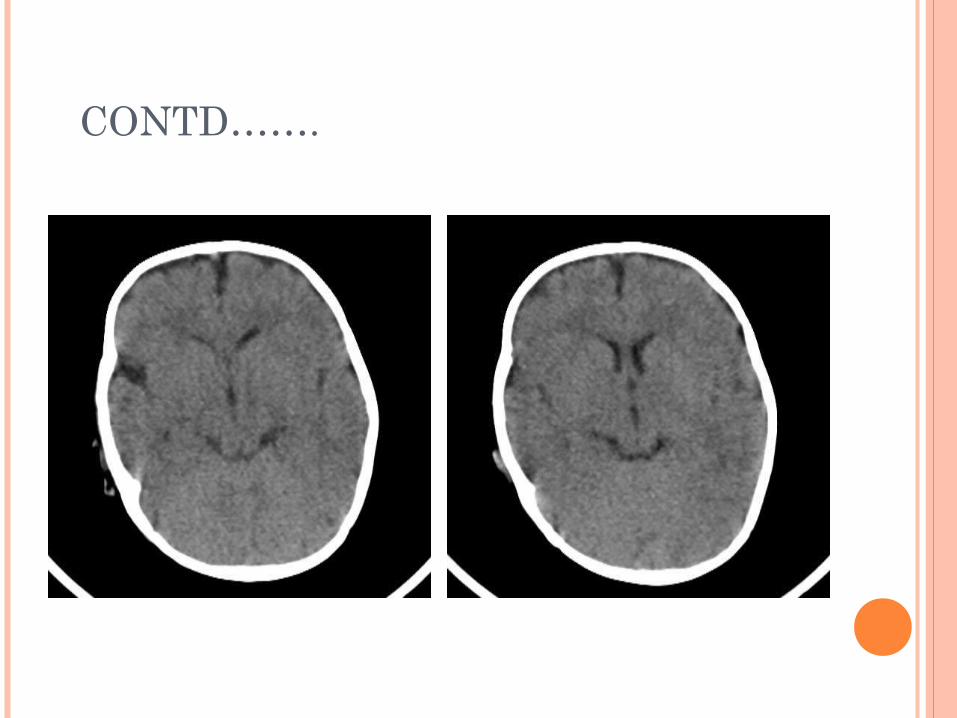
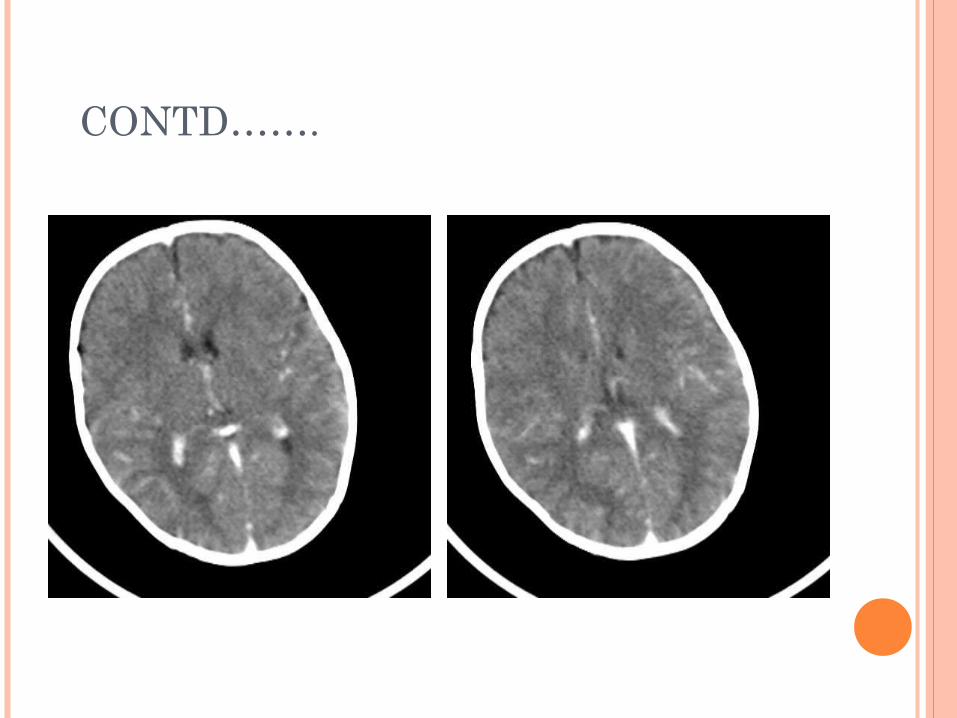
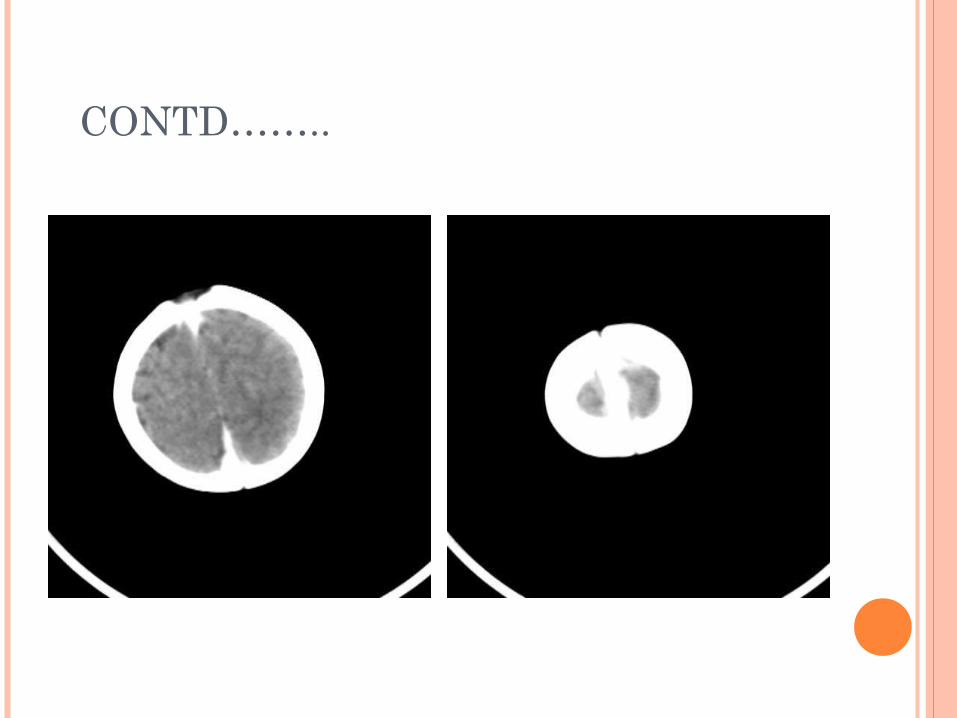
PLAIN CT SCAN OF BRAIN
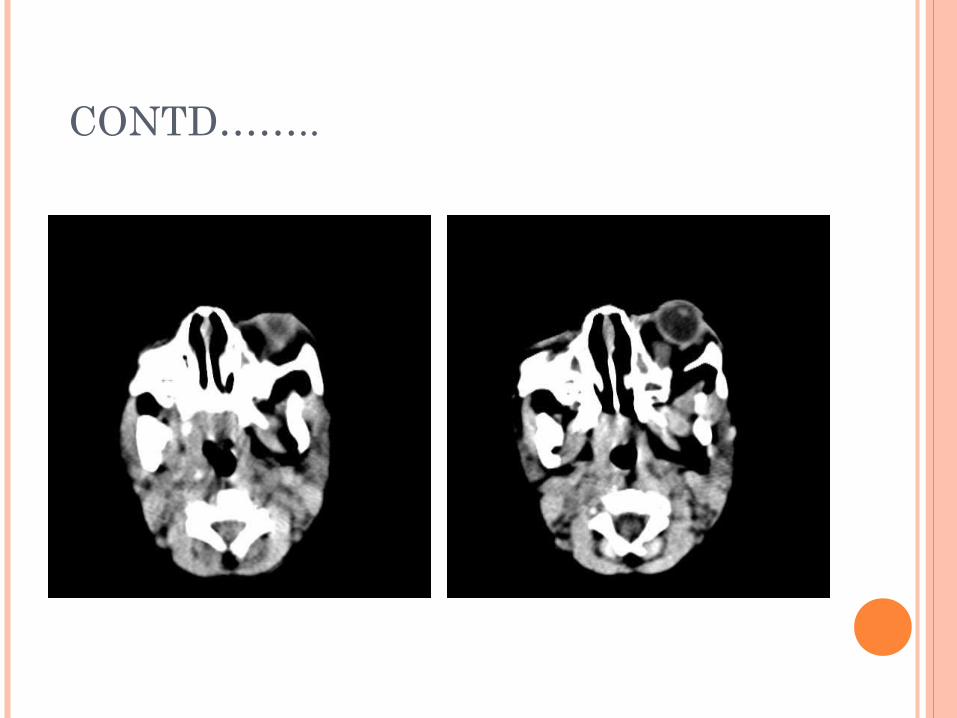
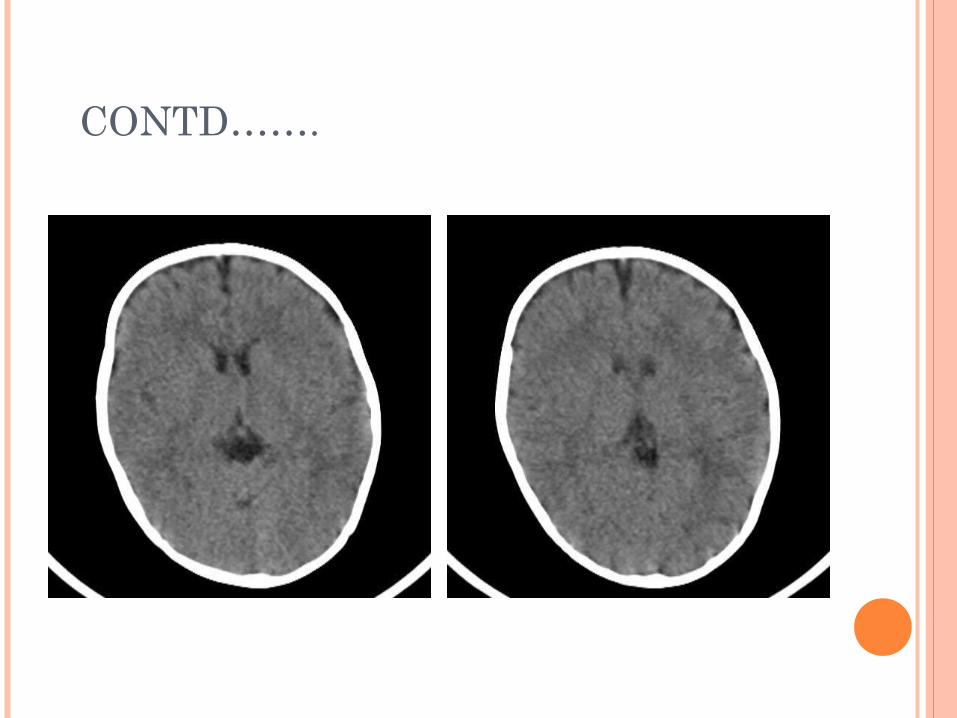
CONTD……..
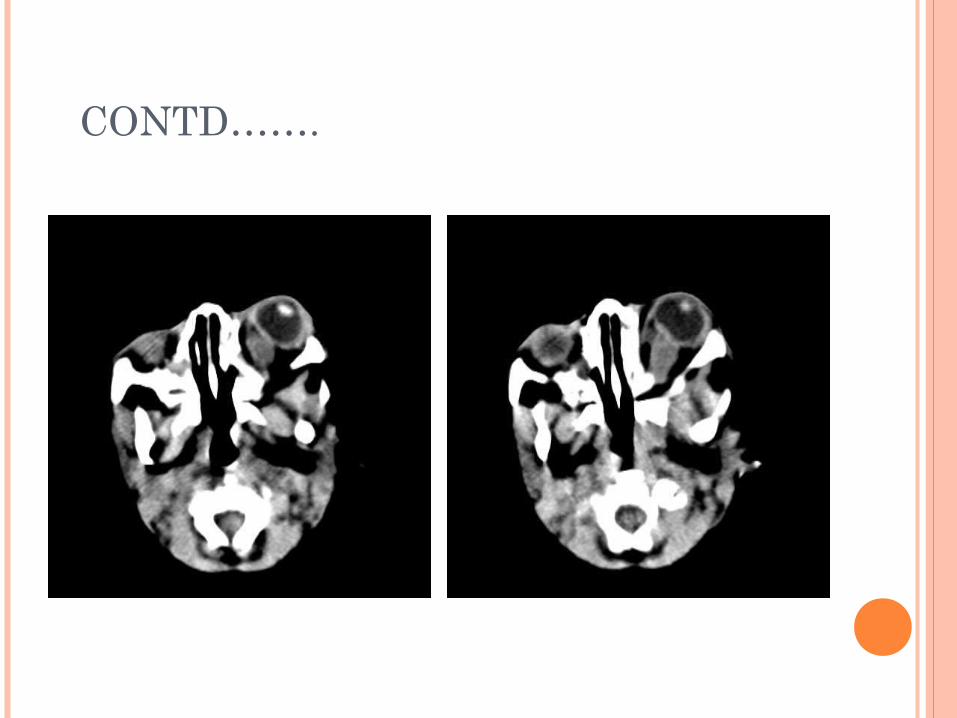
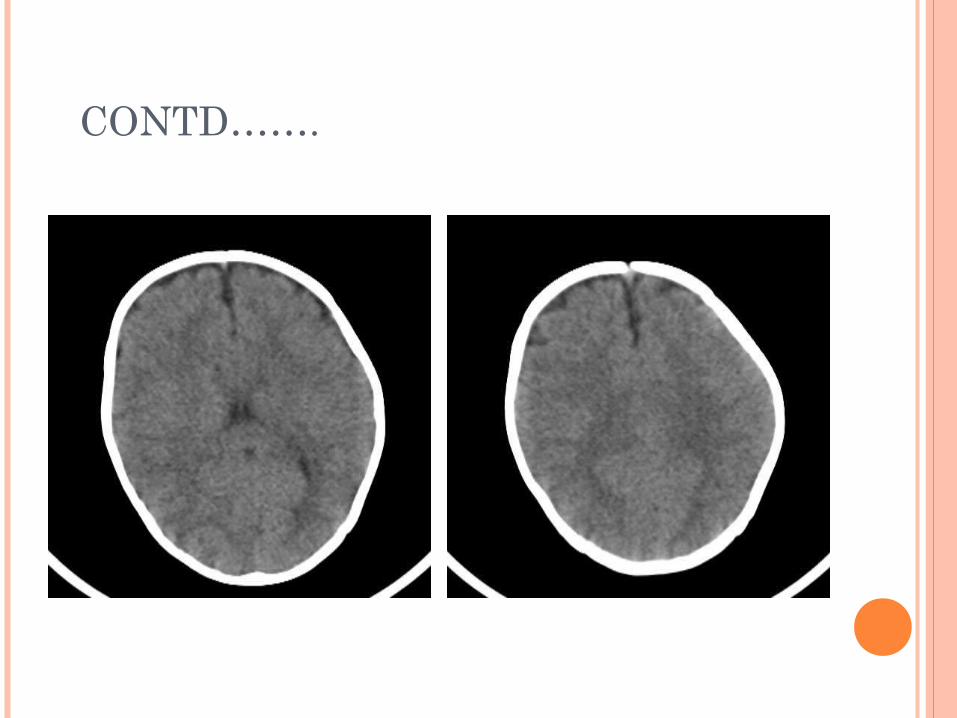
CONTD…….
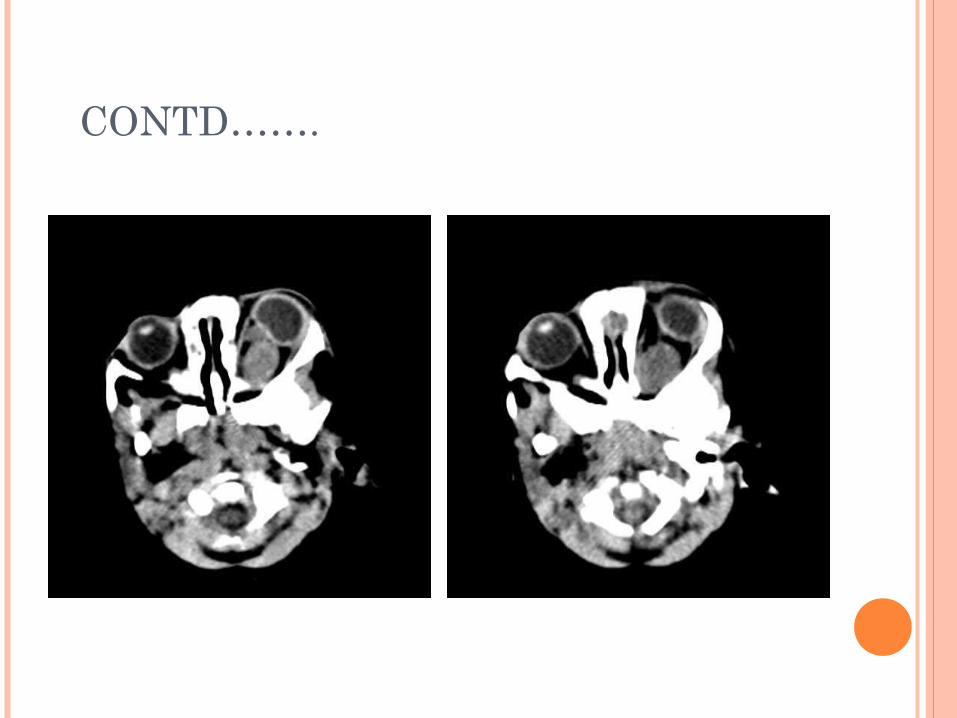
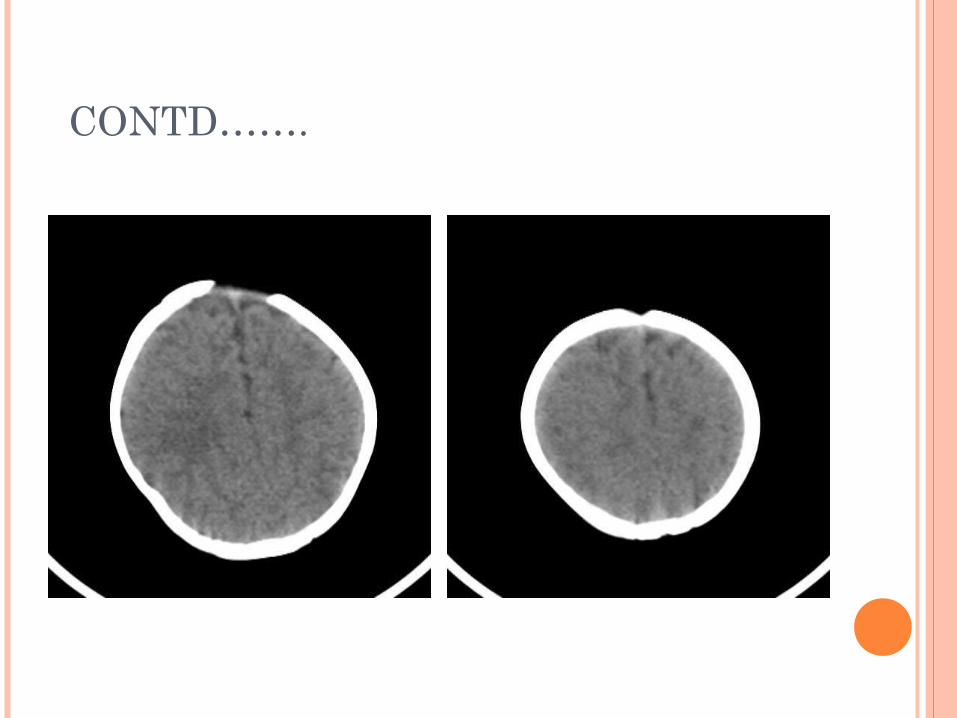
CONTD…….
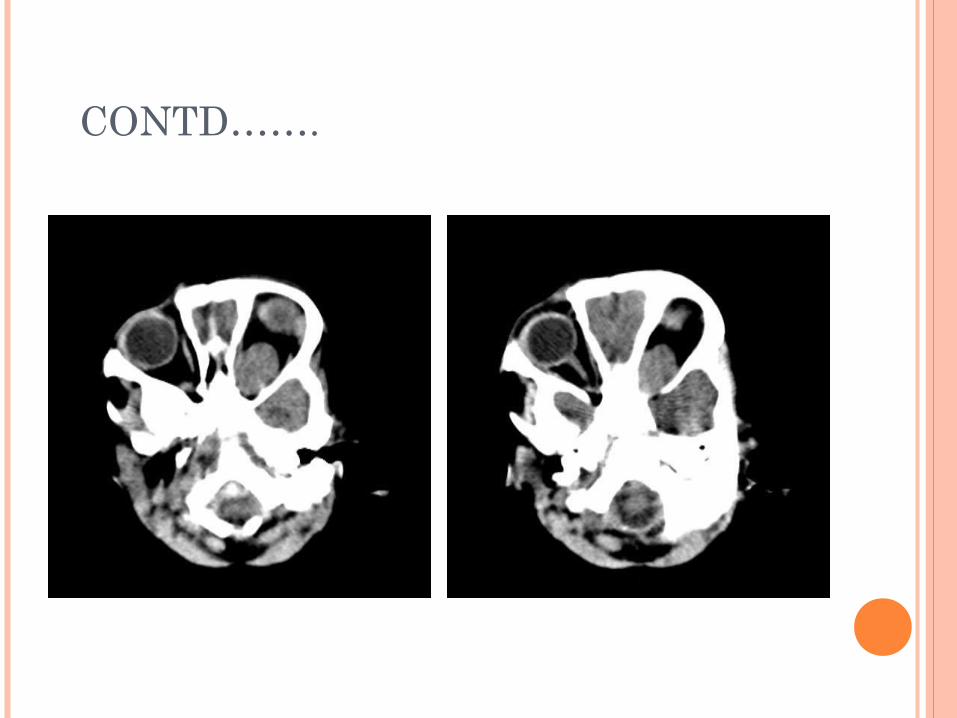
CONTD…….
CONTD…….
CONTD…….
CONTD……..
CONTD…….
CONTD…….
CONTD…….
CONTD…….
CONTD…….
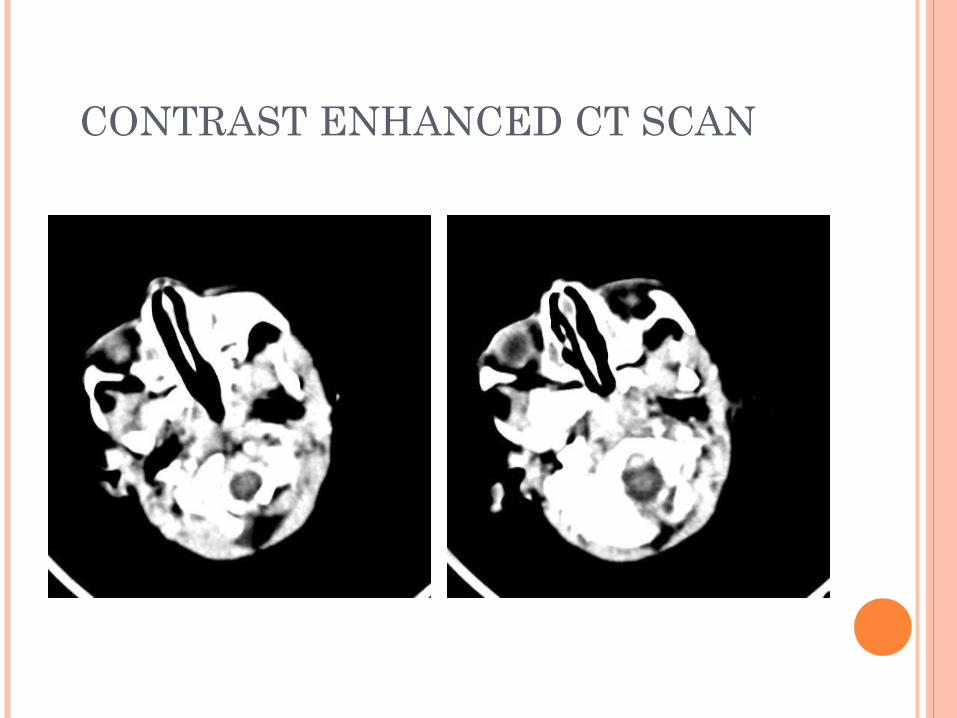
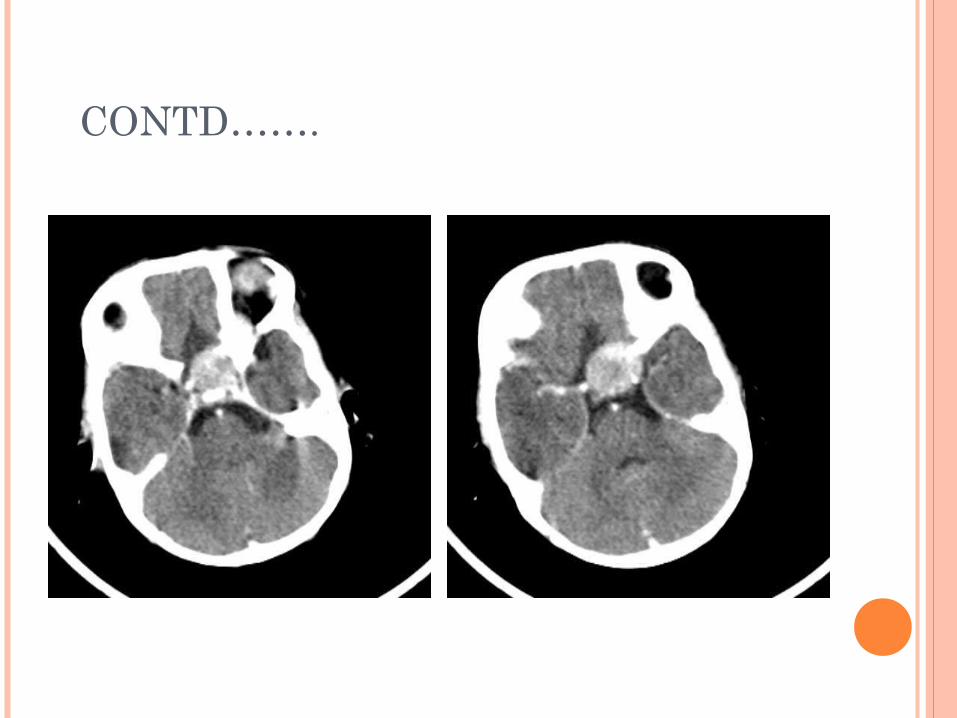
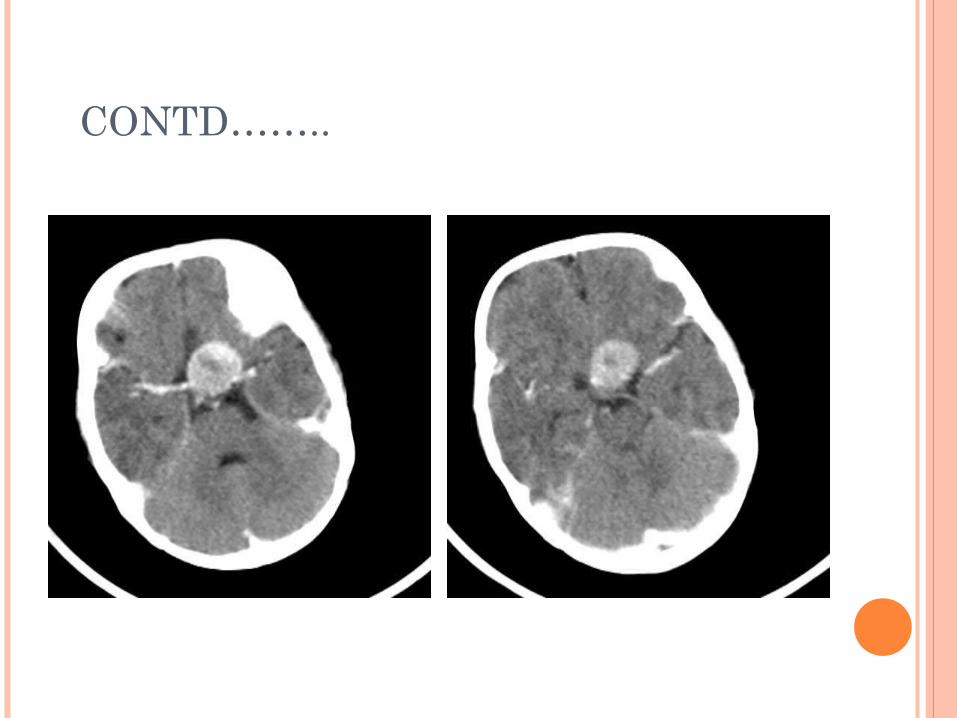
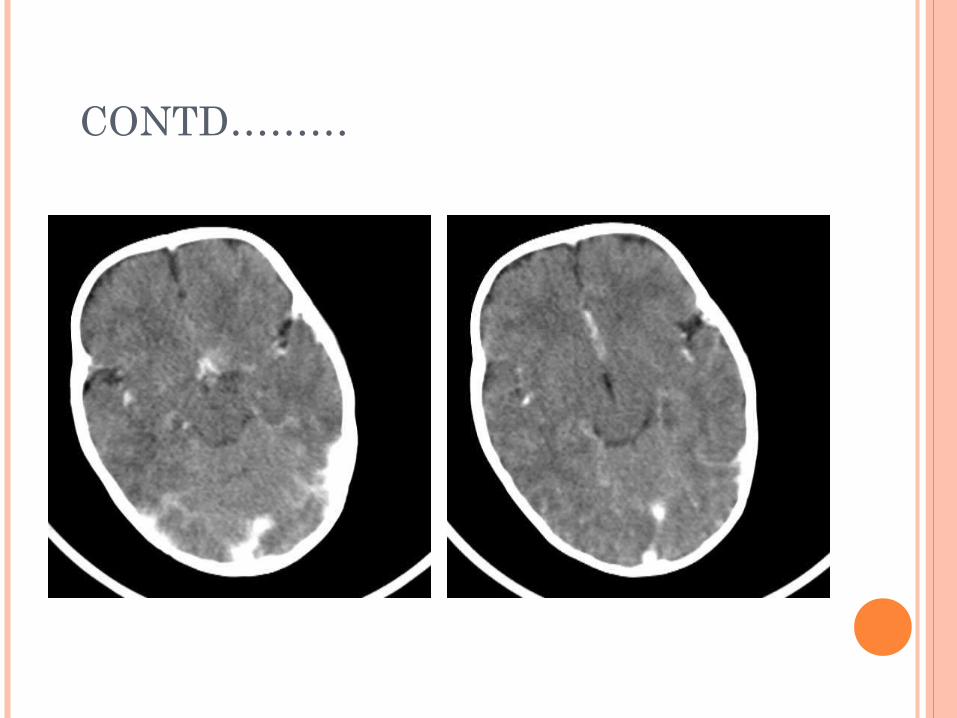
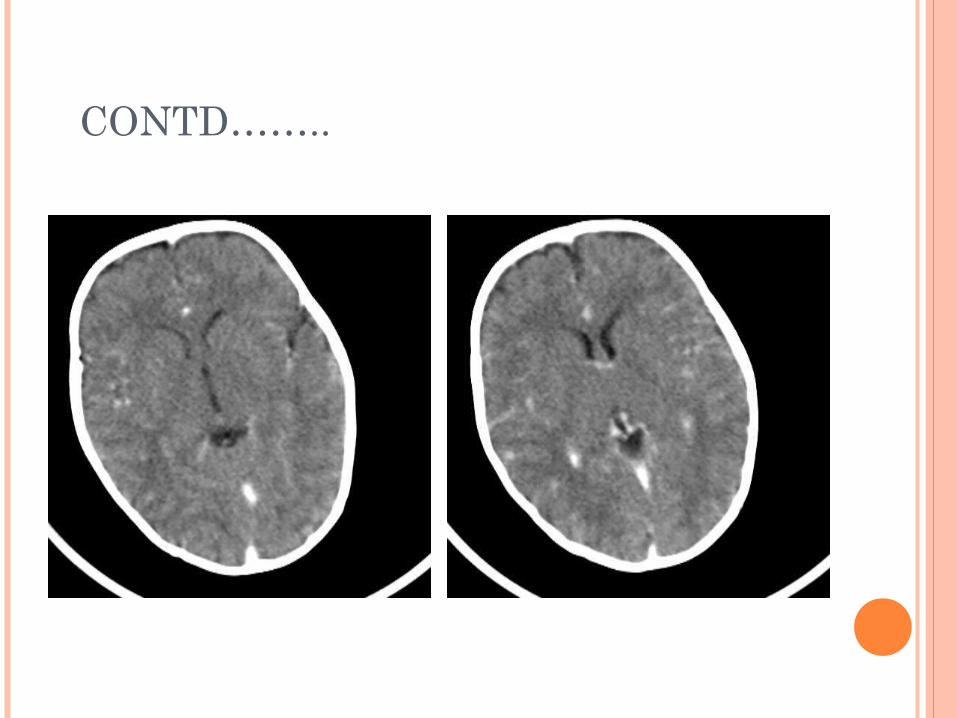
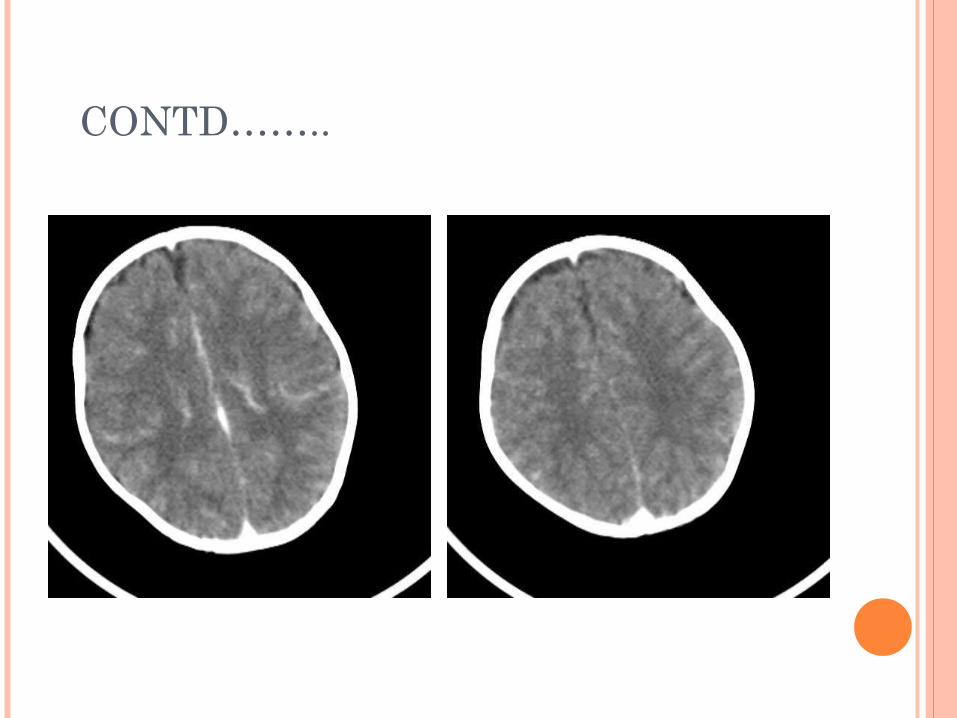
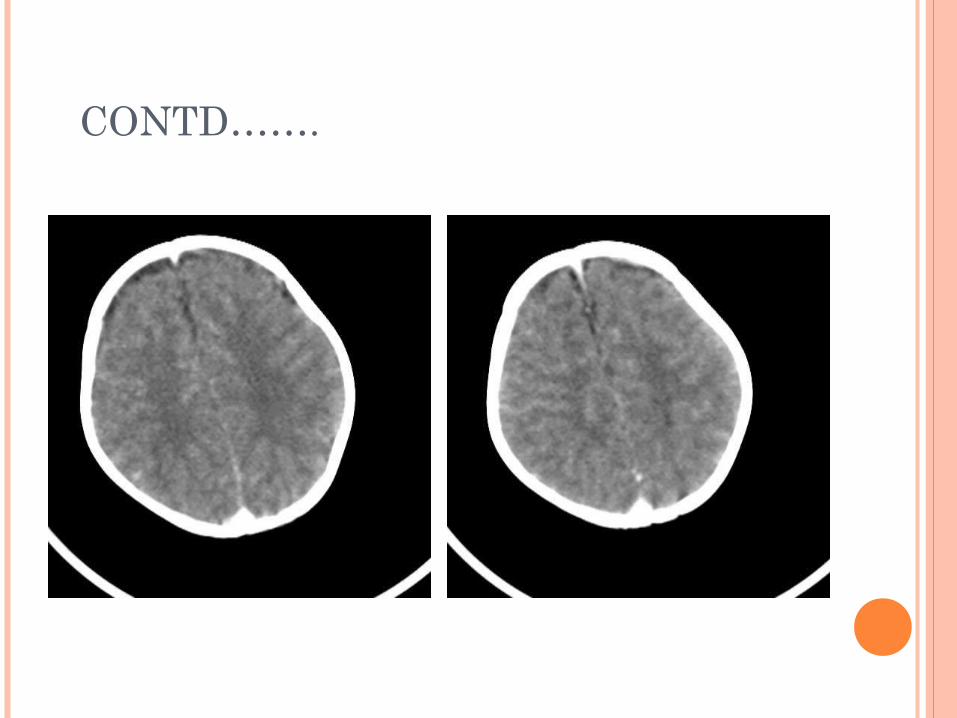
CONTRAST ENHANCED CT SCAN
CONTD…….
CONTD……
CONTD……..
CONTD…….
CONTD……..
CONTD………
CONTD……..
CONTD…….
CONTD……..
CONTD…….
CONTD………
CONTD……..
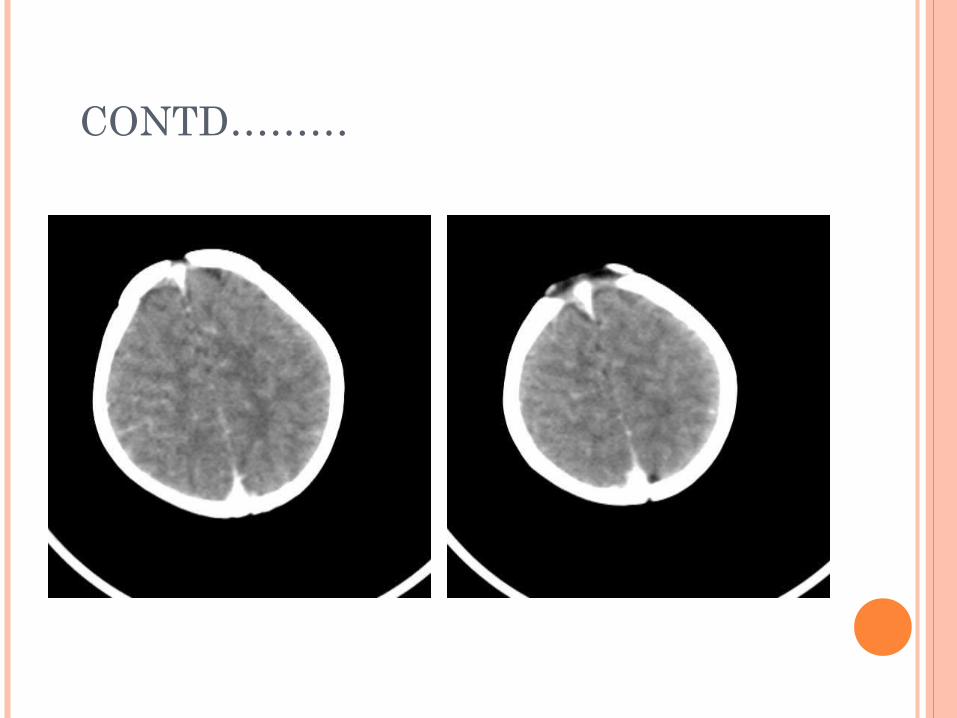
CT FINDINGS IN OUR CASE
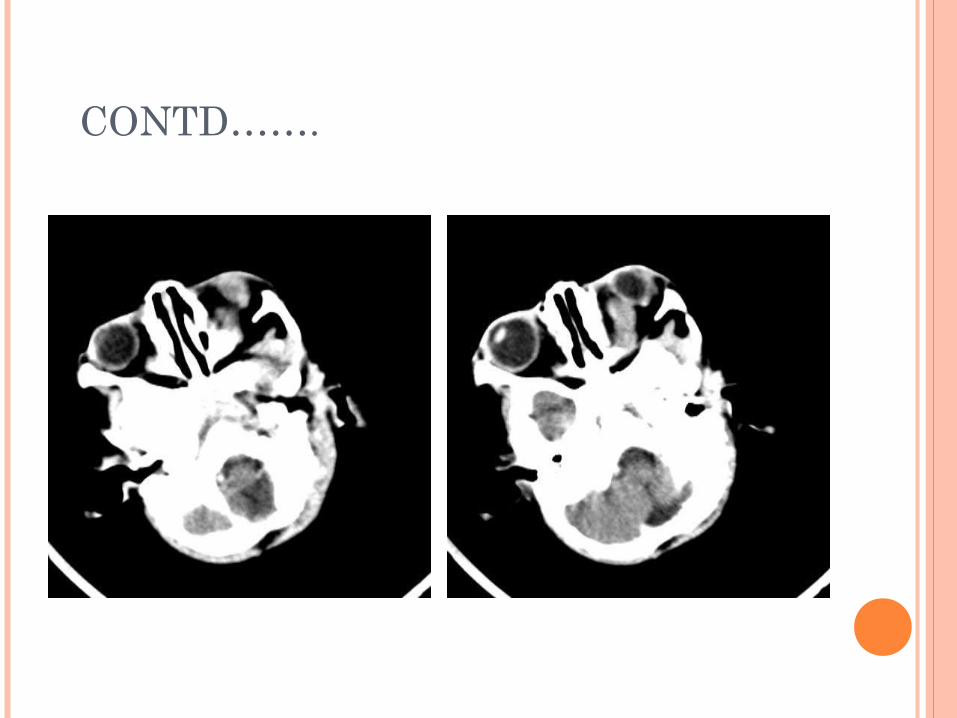
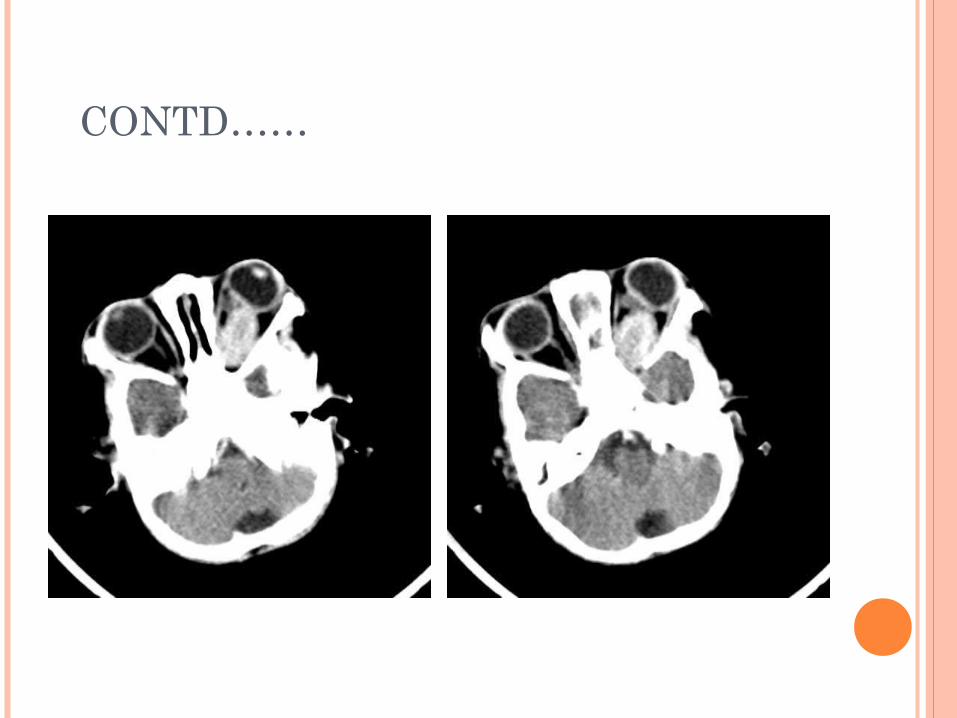
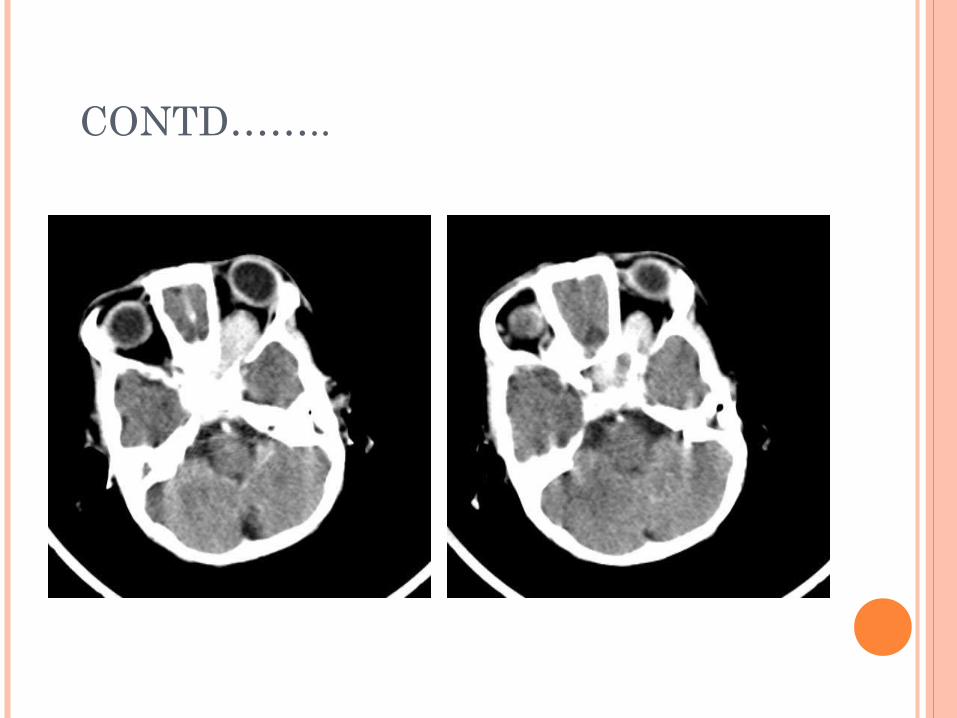
An about 22x22mm hypodense globular mass, highly enhanced slightly heterogeneous in suprasellar region
Mass is extending to left frontal lobe and deepening the floor of sella
Mass is markedly entering to left orbital fossa through optic chiasma, encasing optic nerve sparing extra ocular muscles
DIFFERENTIAL DIAGNOSIS
In contrary to adult age most common suprasellar tumor in child are with decreasing frequency ……
: Craniopharyngioma :Chiasmatic/ Hypothalamic low grade glioma : Germinoma : Lesion attributed to langerhans cell
histiocytosis
SATCHMOE….ANOTHER WAY OF D/D SUPRA/ PARA/ INTRASELLAR MASS
Satchmoe : nick name of “Louis Armstrong”
1. S: Sarcoidosis, sellar tumor2. A: Adenoma, Aneurysm3. T: Teratoma, Tubercular granuloma4. C: Craniopharyngioma, Cyst-Rathke’s cleft 5. H: Hemartoma,Hypothalamic glioma6. Histiocytosis 7. M: Metastasis8. O: Optic nerve glioma, Germinoma9. E: Epidermoid, Eosinophilic granuloma
CRANIOPHARYNGIMA
Large intra and supra sellar mass with cystic& enhancing component as well as calcification in children are virtually
pathognomonic for Craniopharyngioma…… perhaps with only Dermoid in the D/D
**Our case shows no calcification at all
PATHOLOGICAL TYPE
Admantinomatous ….paediatric age group Papillary…..Adult age group Mixed……15%
EPIDEMIOLOGY
There is Bimodal age presentation with 1st peak between 10-14 age almost exclusively of Admantinomatous type
2nd peak young to middle aged mostly papillary sub type
Incidence about 6% of all expanding lesion in childhood
CLINICAL SIGNS/ SYMPTOMS
Increased intracranial tension (headache)
Endocrine dysfunction (Delayed puberty, short stature)
Visual problem
RADIOLOGICAL FEATURES
95% suprasellar, frequently distorting optic chiasma or compressing mid brain causing hydrocephalus
Occasionally intraventricular homogenous soft tissue mass with calcification commonly at 3rd ventricle
CT SCAN FINDINGS
Cystic near CSF density Soft tissue density vivid enhancement Calcification in 90% cases
**calcification is uncommon in papillary variety
CHIASMATIC HYPOTHALAMIC GLIOMA
4-8% childhood intracranial tumor, rare in adults
Common in first decade less than 1yr Male: Female incidence is equal 20-30% children are associated with
neurofibromatosis Progress rapidly
CH GLIOMA CONTD…..
Chiasmatic glioma can involve anything between optic nerve to visual cortex
Almost 25% optic pathways gliomas are confined to optic disc and nerve
40-75% may involve optic chiasma
CLINICAL SIGNS/ SYMPTOMS
Painless PROPTOSIS
Hydrocephalus if involving foramen of monro
**HISTOLOGICALLY: Low grade Glioma
PITUITARY ADENOMA
Rarely present in children
Pituitary micro adenoma: less than 10mm in size
Pituitary macro adenoma: more than 10mm in size expansion of sella is common
Most pediatric pituitary adenomas present after the onset of puberty and present with frequent headaches, changes in visual acuity and, in females, menstrual dysfunction.
Most (19/20) were secretory, with prolactinomas being the most common type.
imaging findings are same like any other suprasellar mass
SUPRASELLAR MENINGIOMA
Benign tumor of meninges usually solid may contain necrotic/ cystic lesion and calcification
Frequently invade the sella turcica
Such tumor can also encase the optic nerve with in optic canal and fossa orbitalis
ARACHNOID CYST AND RATHKE’S CLEFT CYST
Rarely in suprasellar region in children
Clinical symptom: visual symptom, hydrocephalus,
macrocephaly, pyramidal tract sign, precocious puberty
MISCELLANEOUS LESION
A. Hypothalamic hemartoma:
usually small and asymptomatic presenting in two decades
Clinical symptom: hyperactivity syndrome with hyperplasia, behavior disorder, precocious puberty,
gelastie seizure
CONTD…..
B. Lesion of INFUNDIBULUM: : Germinoma : Hypophysitis : Histiocytosis X
SUPRASELLAR GERMINOMA 20% of all Germ cell tumor
Hypo intense on T1, Hyper intense on T2 and extremely intense contrast enhancement
It can create diagnostic dilemma on imaging , can get easily confused with optic/ chiasmatic glioma.
If serum and CSF studies for tumor marker are negative , surgical exploration for biopsy and histological confirmation helps differentiation
FINAL DIAGNOSIS
Our probable diagnosis: Suprasellar germinoma OR Chiasmatic
Hypophyseal Glioma
Patient was sent to advanced center for final diagnosis and further management
Unfortunately there was no feed back
CONCLUSION
Paediatric brain tumor have always been a challenge
They are heterogeneous set of pathologies involving different age groups in childhood and also differ widely from their adult counterparts as far as adjuvant therapies are concerned
Unlike Meningioma and Pituitary Adenoma in adults, Craniopharyngioma, Optic Glioma and Germinoma form the main lesions in paediatric age group
CONTD…..
While safe surgery is the Key in most of adult tumors, Chemo and Radiotherapy are the chief modality in some of these paediatric tumor like GERMINOMA and OPTICO- CHIASMATIC GLIOMA
As epidemiology and management of these tumors is different that’s why it requires dedicated multidisciplinary team approach
REFERENCES
1. Differential Diagnosis of suprasellar mass in children: Warmnth Metz M, Gnekow AK, Muller H, Solynosi L K.Klin Paediatri 2004 Nov Dec 216(6):323;30
2. Pituitary region mass: Dr Ayush Goel and Dr Frank Gaillard etal. Radiopaedia.org/article/Pituitary
3. Sella turcica and parasellar region: Walter Kucharezyk and Marieke Hazewinkel The Radiology assistant
4. Cranipharyngioma: Dr Frank Gaillard etal. Radiopaedia.org/article/craniopharyngioma
REF……CONTD.
5. Suprasellar Meningioma_ a case report: MG Kgoro, A Speclman The south African Radiographer vol.51 no 2 Nov 2013
6. Pituitary macro adenoma: Dr Henry Knipe and Yuranga W etal. Radiopaedia.orgt
7. Paediatric Suprasellar Lesion:. CE Deopujari, Ashish Kumar, VS Karmarkar, NK Biyani,
M Mhatre and NJ shah Journal of Paediatric Neurosciences 2011 Oct(6
supple): 546-555

Thank you Have a good day