Embed Size (px)
Citation preview

Stroke- What's new?
Dr Ahmad Shahir MawardiDepartment of NeurologyHospital Kuala Lumpur
28th July 2015

Anything "new"??
Depends on how "new" is defined
Tx of stroke is more than aspirin/ statin/ physiotherapy
What's new
• Reperfusion therapy
• Endovascular therapy
• Mx of haemorhagic stroke/ICH
• Stroke rehabilitation
• Novel therapy

Epidemiology
• Annually 15 million people worldwide suffer a stroke– 5 million die– 5 million are left permanently disabled.
• Top 4 leading causes of death in ASEAN countries,– death rate :
• 10.9/100 000 (Thailand)• 54.2/100 000 (Singapore).

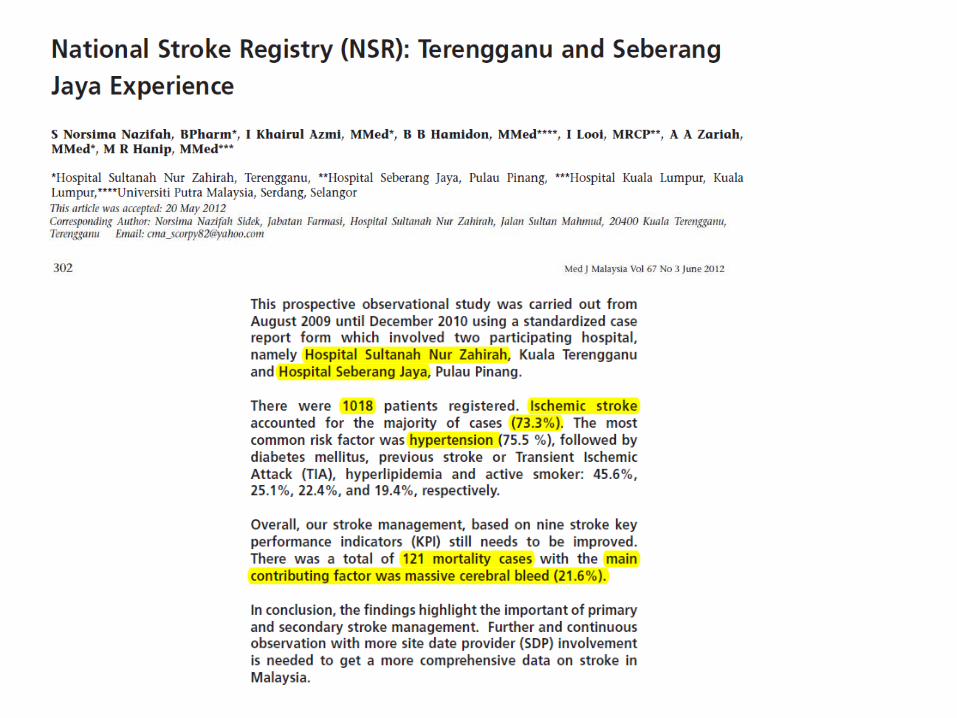
Malaysia's data
• In Kelantan, 158 stroke patients were admitted to HUSM between January 1997 and December 1998.– 56·3% ischemic stroke– 36·1% primary intracerebral hemorrhage– 7·6% subarachnoid hemorrhage.
• 246 stroke patients admitted to Penang Hospital from December 1998 to November 1999– 74·8% ischemic stroke – 25·2% hemorrhagic stroke
Malaysia's data
• 163 ischemic stroke patients were admitted to HUKM from June 2000 until January 2001– 62·6% lacunar infarct – 26·4% middle cerebral infarct – 11·0% other manifestations – The mortality rate: 11·7%, with a mean age of 62·2 years
• UMMC 83 ischemic stroke patients were admitted between June 2000 and November 2000– hyperhomocysteinemia was found to be a risk factor for ischemic
stroke (odds ratio 5·3) – Depression was reported in (66%) 3-6 months poststroke
• It has been reported that six new stroke cases occur in Malaysia every hour
Malaysia's data
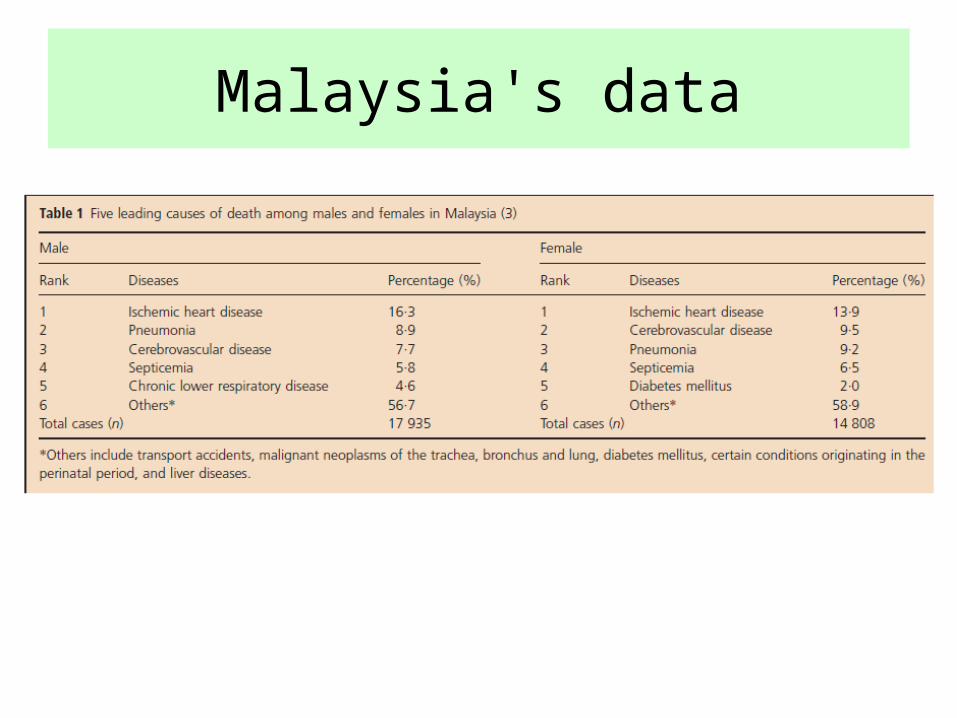
Malaysia's data
Acute Stroke
• sudden non-convulsive, focal neurological deficit resulting from vascular disease
• could be divided into » Acute ischemia infarction » Intraparenchymal hemorrhage» Subarachnoid hemorrhage
**a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention
Transient Ischemic Attack
• Old definition - (Clinically-based)– brief episode of neurologic dysfunction
< 24 hours resulting from focal temporary cerebral ischemia
• New definition - (Tissue-based)– transient episode of neurologic dysfunction
caused by focal brain, spinal cord, or retinal ischemia, without acute infarction*
**a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention
1. Reperfusion therapy

Reperfusion therapy
• Intravenous rt-PA can be given only if the following is available:1. A physician with expertise in the diagnosis and mx of stroke.
2. Appropriate neuroimaging tests are available 24 hours a day
3. Capability to manage the complications of thrombolysis, particularly intracranial haemorrhage.
• Onset:– 4.5 hours– 3 hours ( >80 y.o with DM)
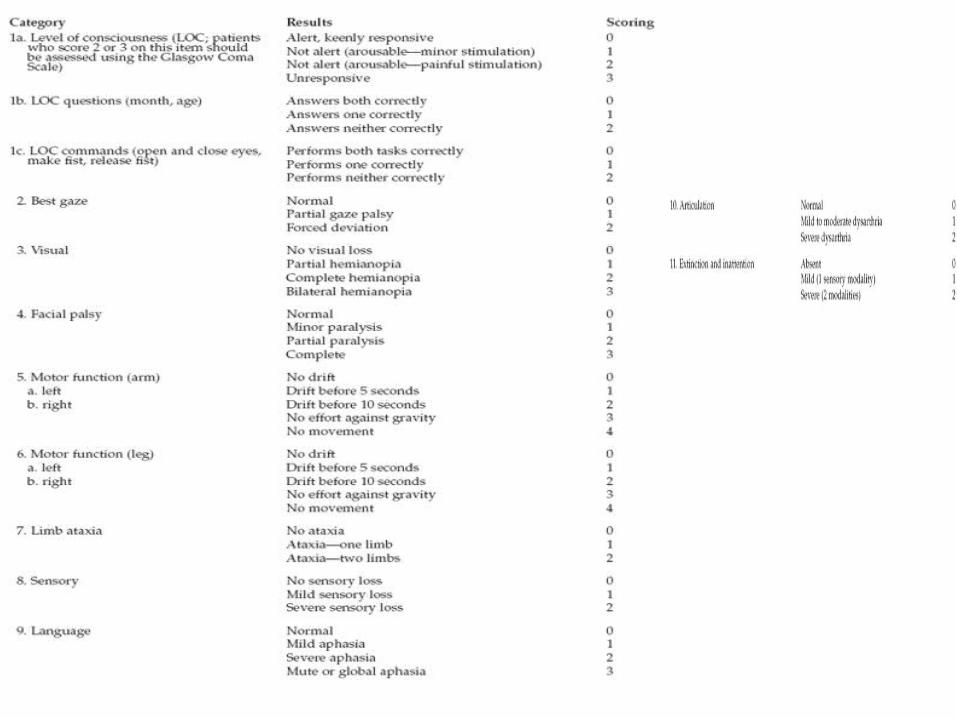
• NIHSS 6-22 (some centre 4-22)
Tips to know the exact onset
• The exact time of “last seen well”• What is the patient doing during the onset?• Where does the patient stay?• Challenge the eye witness regarding the time
Candidate for thrombolysis
1. Diagnosis of ischaemic stroke causing measurable neurological deficit.
2. The neurological signs should not be clearing spontaneously.
3. The neurological signs should not be minor and isolated.
4. Caution should be exercised in treating a patient with major deficits.
5. Onset of symptoms <4.5 hours before beginning treatment.
Candidate for thrombolysis
6. No contraindication for thrombolytic therapy.
7. Blood pressure less than 185mm Hg systolic and/or less than 110mm Hg diastolic.
8. Brain CT is normal or minimal change.
9. The patient or family understand the potential risks and benefits from treatment.
*written consent

1. Current use of oral anticoagulant or a promthrombin time (PT) > 15 seconds (INR > 1.7)
2. Use of heparin in the previous 48 hours and a prolonged partial thromboplastin time (PTT)
3. A platelet count < 100,000/mm3
4. Another stroke or any serious head injury in the previous 3 months
5. Major surgery within the preceding 14 days
6. Arterial puncture at noncompressible site within the last 21 days
7. Pre-treatment systolic blood pressure > 185mmHg or diastolic blood pressure > 110mmHg
Contraindication for thrombolysis (I)
8. Neurological signs that are improving rapidly
9. Isolated mild neurological deficits, such as ataxia alone, sensory loss alone, dysarthria alone or minimal weakness
10. Prior intracranial haemorrhage
11. A blood glucose < 2.7mmol/l or > 22.2mmol/l
12. Seizure at the onset of stroke
13. Gastrointestinal or urinary bleeding within the preceding 24 days
14. Recent myocardial infarction
Contraindication for thrombolysis (II)
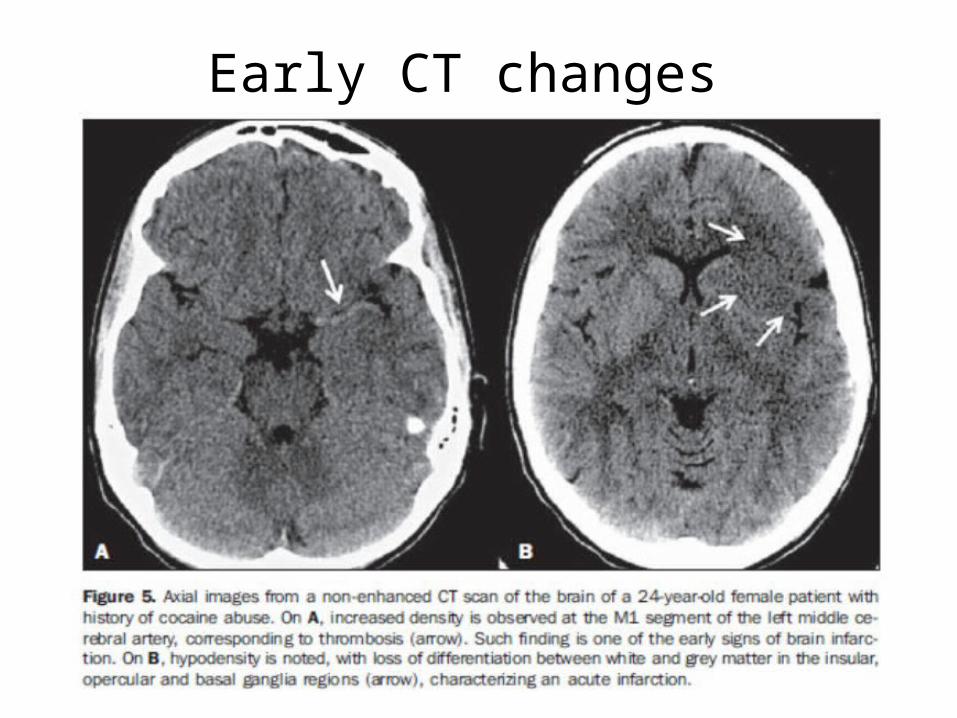
Early CT changes
• “Dot sign”
• loss of grey-white differentiation
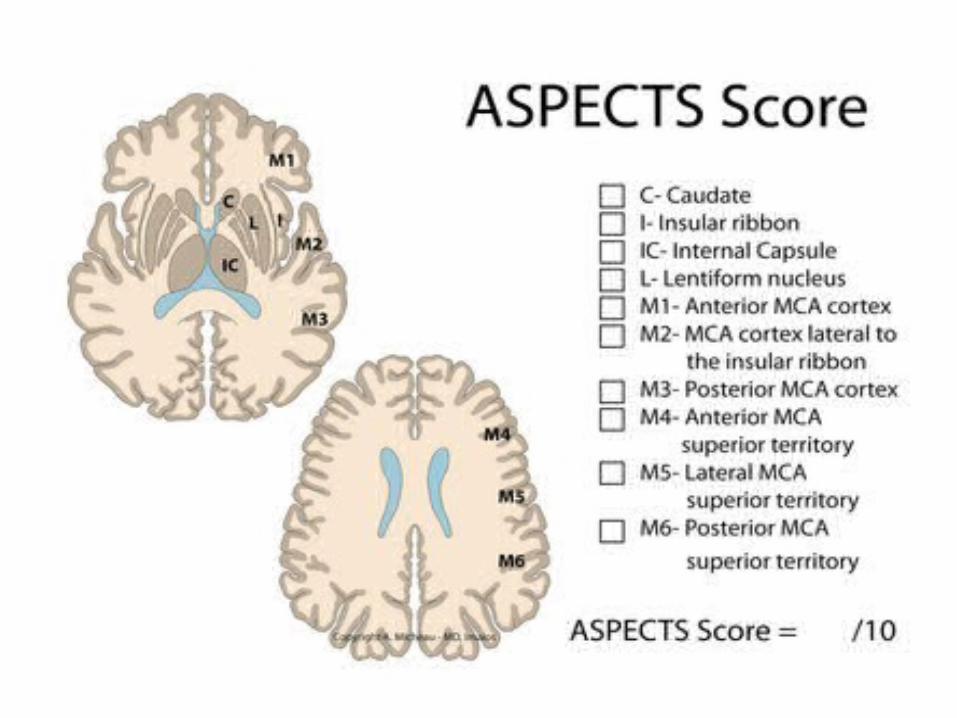
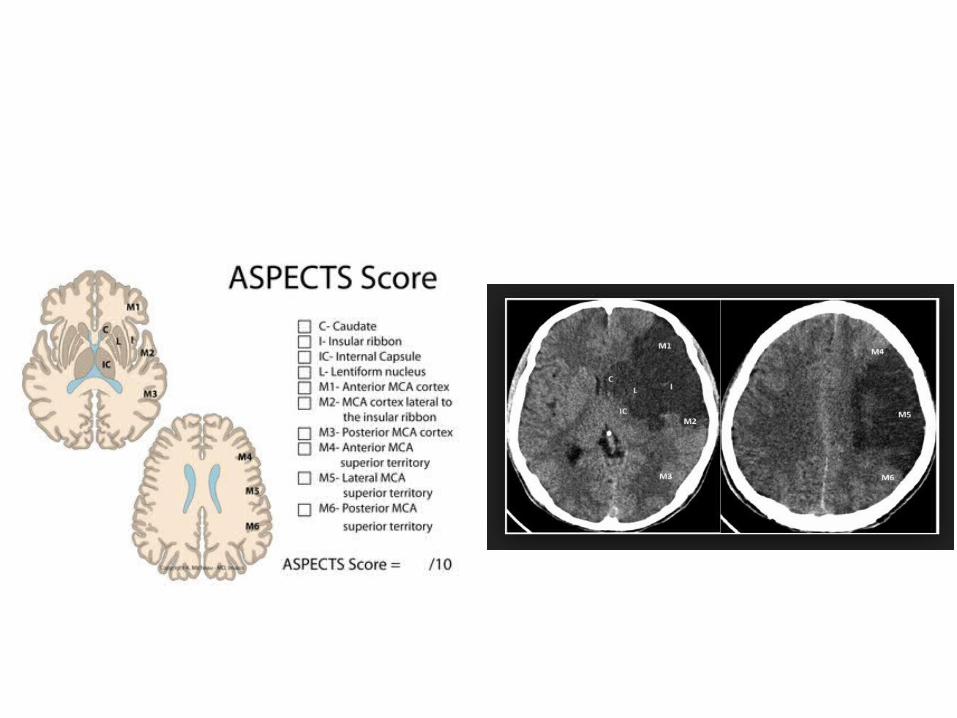
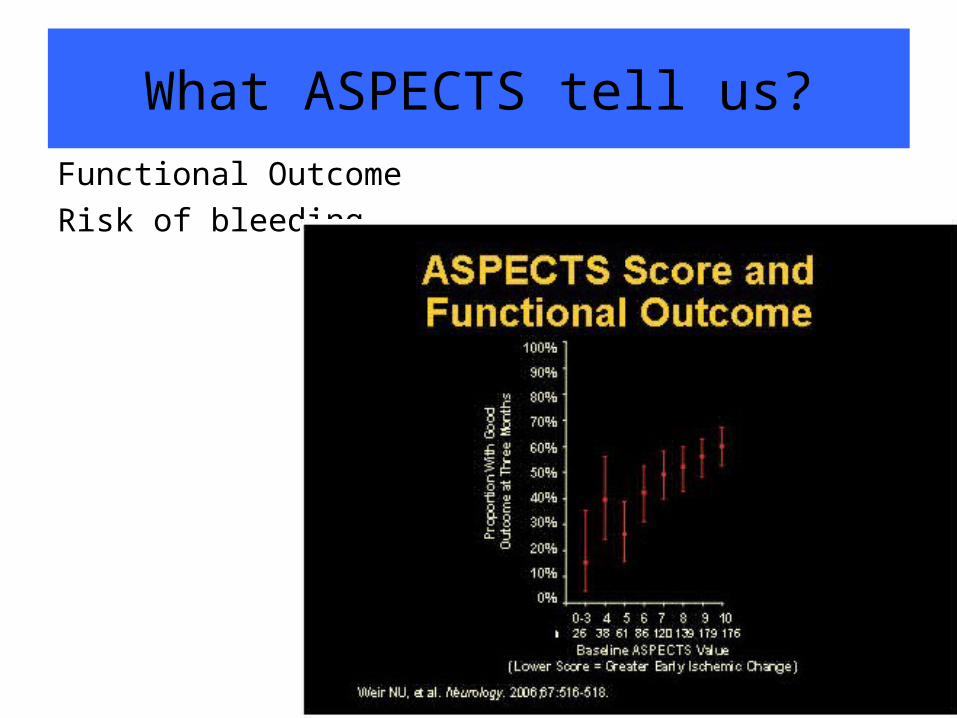
What ASPECTS tell us?
Functional Outcome
Risk of bleeding
Post thrombolysis care (I)1. Admit to ICU or a stroke unit
2. Perform neurological assessments • every 15 minutes during the infusion of rt-PA • every 30 minutes for the next 6 hours • every hour until 24 hours from treatment.
3. If the patient develops severe headache, acute hypertension, nausea or vomiting --> discontinue the rt-PA, obtain a CT scan of brain.
4. Measure blood pressure • every 15 minutes for the first 2 hours• every 30 minutes for the next 6 hours • every hour until 24 hours from treatment.
Post thrombolysis care (I)
5. Increase blood pressure measurements if a systolic blood pressure >180mmHg or diastolic blood pressure >105mmHg is recorded. Administer anti-hypertensive
6. Delay placement of NG tube, CBD, arterial line.
7. Avoid antiplatelet drugs for the first 24 hours after rt-PA.
Neurology HKL experience
• Total of candidate thrombolysed: 30 pts
• Complicated by ICB : 6 pts
• Mortality: 6 pts (various reasons)
2.Endovascular therapy

BackgroundBackground
• In patients with acute ischemic stroke caused by a proximal intracranial arterial occlusion, intraarterial treatment is highly effective for emergency revascularization
• However, proof of a beneficial effect on functional outcome is lacking
Limitation of IV Alteplase Limitation of IV Alteplase
narrow therapeutic time window
Contraindicationsrecent surgery, coagulation abnormalities, and a history of intracranial hemorrhage.
less effective at opening proximal occlusions of the major intracranial arteries (1/3 in ICA infarction)
Intraarterial therapy Intraarterial therapy
2 typesIntraarterial thrombolysis clot retrieval with mechanical devices
Neutral results so far, probably due to long interval before intraarterial treatmentabsence of pretreatment vascular imaging to confirm a proximal intracranial occlusionLimited use of third-generation mechanical thrombectomy devices
ObjectivesObjectives
• Assess whether intraarterial treatment plus usual care would be more effective than usual care alone– in patients with a proximal arterial occlusion in the
anterior cerebral circulation – could be treated intraarterially within 6 hours after
symptom onset
MethodologyMethodology
• Interventional group– Intraarterial treatment (intraarterial
thrombolysis, mechanical treatment, or both) plus usual care (which could include intravenous administration of alteplase)
• Control group– Patients who receives usual care only
Randomization Randomization
• a total of 502 patients underwent randomization in 16 Dutch centers
• single blinded study

Primary outcome Primary outcome
• There was a shift in the distribution of the primary-outcome scores in favor of the intervention.
• The adjusted common odds ratio was 1.67 (95% confidence interval)

Secondary outcomeSecondary outcome
• The NIHSS score after 5 to 7 days was, on average, 2.9 points (95% CI, 1.5 to 4.3) lower in the intervention group than in the control group.

Safety Safety
• No significant between-group difference in the occurrence of serious adverse events during the 90-day follow-up period (P = 0.31)
• 13 of the 233 patients (5.6%) in the intervention group had clinical signs of a new ischemic stroke in a different vascular territory within 90 days
• No significant difference in mortality at 7, 30, or 90 days of follow-up
Procedure-related complicationsProcedure-related complications
• Embolization into new territories outside the target downstream territory of the occluded vessel (8.6%)
• Procedure-related vessel dissections (1.7%)
• Vessel perforations (0.9%).
ConclusionsConclusions
• Patients with acute ischemic stroke caused by a proximal intracranial arterial occlusion of the anterior circulation have a benefit with respect to functional recovery when combination of intravenous thrombolysis and intraarterial treatment are administered within 6 hours after stroke onset

3. Mx of haemorhagic ICH

Front page
Similar result !!
Introduction• This guideline serves :
– An update to previous AHA guideline 2010– As a brief and useful guide on management of ICH
• Consist of 15 sections:– Emergency diagnosis & assessment, causes of ICH, BP
management, in-patient management, mx of raised ICP, role of surgical clot removal, outcome prediction, prevention of recurrent ICH, rehabilitation and future considerations
MEDICAL TREATMENT FOR ICH(Blood Pressure and Outcome in ICH)
• Elevated BP is very common in acute ICH– Stress, pain, increased ICP, premorbid persistent high BP– a/w hematoma expansion, neurological deterioration, death and
dependency after ICH
MEDICAL TREATMENT FOR ICH(Blood Pressure and Outcome in ICH)
• Safety of Early Intensive BP-Lowering Treatment– ATACH trial (Antihypertensive Treatment of Acute Cerebral
Hemorrhage)
• IV nicardipine-based BP lowering within 3 hrs of ICH
– INTERACT-1 trial (Intensive BP Reduction in Acute Cerebral Hemorrhage) – pilot phase
• BP lowering within 6 hrs of ICH
– Both found rapid reduction of SBP < 140 to be safe
– INTERACT-2 – main phase
• No increase in death or serious adverse events from early intensive BP lowering in eligible patients

MEDICAL TREATMENT FOR ICH(Blood Pressure and Outcome in ICH)
• Efficacy of Early Intensive BP-lowering Treatment– INTERACT-2
• Intensive BP lowering, n=2839 pts with SBP 150- 220 mmHg within 6 hours of ICH
• Two arms :
– A: intensive therapy ( BP lowered to target SBP<140 within 1 hr of randomization , for 7 days)
– B: standard therapy ( SBP< 180 mmHg)
• Primary outcome : death / major disability (MRS > 3) : OR 0.87 (p= 0.06)
• Secondary end points
– Functional recovery : OR 0.87 (p = 0.04)
– Physical & mental-health QoL: OR 0.87 (p = 0.002)
MEDICAL TREATMENT FOR ICH(Blood Pressure and Outcome in ICH)
• Efficacy of Early Intensive BP-lowering Treatment– INTERACT-2
• no clear relationship between outcome and the time from onset of ICH to commencing treatment
• no significant effect of intensive BP-lowering treatment on hematoma growth.

MEDICAL TREATMENT FOR ICH(Blood Pressure and Outcome in ICH)
• Recommendations, for ICH patients presenting with:
– SBP between 150 and 220 mmHg and without contraindication to acute BP treatment, acute lowering of SBP to 140 mm Hg is safe (Class I; Level of Evidence A) and can be effective for improving functional outcome (Class IIa; Level of Evidence B). (Revised from the previous guideline)
– SBP >220 mm Hg: to consider aggressive reduction of BP with a continuous intravenous infusion and frequent BP monitoring (Class IIb; Level of Evidence C). (New recommendation)
Inpatient mx (Seizures and AED)• Frequency of early seizures after ICH ~ 16%
– Due to cortical involvement
• Epilepsy occurs in ~ 10%– Risks include stroke severity, cortical location of hematoma, and
delayed initial seizures.
• Clinical seizures should be treated with AEDs (Class I; Level of Evidence A).
• Pts with a change in mental status who are found to have electrographic seizures on EEG should be treated with AEDs (Class I; Level of Evidence C).
• Prophylactic AED is not recommended (Class III; Level of Evidence B).

Inpatient mx and prevention of secondary brain injury (Mx of medical complications)
• Frequency of medical complications after ICH is high
• Most common complications:– Pneumonia (5.6%)– Aspiration (2.6%)– Respiration failure/distress (2%)– PE (1.3%)– Sepsis (1.7%)
• ~ 50% of death after stroke are related to medical complications, usually after 7 days of hospitalization.
4.Stroke rehabilitation
Stroke rehabilitation
1) Drug Therapy Options Evolving to Enhance Motor Recovery : – -ve study– Fluoxetine for Motor Recovery in Acute Ischemic
Stroke (FLAME) study*: • n = 118• given within the first 10 days • pt with moderate-to-severe motor deficit, the early
prescription of fluoxetine + physiotherapy enhances motor recovery after 3 months.
Chollet F, Tardy J, Albucher JF, Thalamas C, Berard E, Lamy C, et al. Fluoxetine for motor recovery after acute ischaemic stroke(FLAME): a randomised placebo-controlled trial. Lancet Neurol. 2011;10:123–130.
Stroke rehabilitation
2) Early Mobilization
• The A Very Early Rehabilitation Trial (AVERT) study*,**, mobilization within the first 24 hours of stroke and at regular intervals – is safe, feasible, and fast-track return to walking unassisted, – increasing the likelihood of milder stroke discharged home, – good functional outcomes at 3 and 12 months. – prevent poststroke complications i.e contractures and DVT.
*van Wijk R, Cumming T, Churilov L, Donnan G, Bernhardt J. An early mobilization protocol successfully delivers more and earlier therapy to acute stroke patients: further results from phase II of AVERT. Neurorehabil Neural Repair. 2012;26:20–26.**Cumming TB, Thrift AG, Collier JM, Churilov L, Dewey HM, Donnan GA, et al. Very early mobilization after stroke fast-tracks return to walking: further results from the phase II AVERT randomized controlled trial. Stroke. 2011;42:153–158.

Stroke rehabilitation
3) Ambulation With Body Weight Support Treadmill Training (RCT, n=408)
– training on a treadmill with body weight support • 2 months after the stroke (early locomotor training);
• 6 months after the stroke (late locomotor training)
• exercise program at home (2 months)
– After 1 year, 52.0% had increased walking ability. – No significant differences in between groups– All groups had similar improvements in walking speed, motor
recovery, balance, functional status, and QoF.– early training of locomotion carried a higher risk for falls.
Stroke rehabilitation
4) Robotic
• Cochrane* systematic review 19 trials (n=666 participants).
• Electromechanical and robot-assisted arm training:– did improve activities of daily living and arm function – but not arm muscle strength – did not increase the risk of patients to dropout and adverse
events were rare.
*Mehrholz J, Hädrich A, Platz T, Kugler J, Pohl M. Electromechanical and robot-assisted arm training for improving generic activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst Rev. 2012;6:CD006876.
Stroke rehabilitation
5) Virtual Reality (Virtual reality and video game applications)
• 12 studies, 195 participants• 11 out of 12 studies identified showed a significant benefit toward
VR for the selected outcomes.
Stroke rehabilitation
6) Transcranial Magnetic Stimulation
• Meta-analysis*, the effects of repetitive transcranial magnetic stimulation (rTMS) on upper limb motor function in patients with stroke.
• Evaluating 18 randomized controlled trials published between 1990 and 2011
• Conclution: – rTMS has a positive effect on motor recovery in patients with stroke,
especially for those with subcortical stroke– low-frequency rTMS over the unaffected hemisphere may be more
beneficial than high-frequency rTMS over the affected hemisphere
Hsu WY, Cheng CH, Liao KK, Lee IH, Lin YY. Effects of repetitive transcranial magnetic stimulation on motor functions in patients with stroke: a meta-analysis. Stroke. 2012;43:1849–1857.

5.Novel therapy

Novel therapy
Stem cell therapy
• Repair of the infarcted area of brain through enhancing neuroprotective and repair mechanisms
• Cell therapy promotes re-vascularization, and reduces cerebral inflammation
• Phase II clinical trials of intravenous transplantation of autologous bone-marrow stem cells have reported safety and tolerability in stroke patients
• Pending the results of future larger trials
• PISCES study currently underway in Glasgow*The PISCES Study. The PISCES Clinical Trial in Disabled Stroke Patients. http://www.reneuron.com/the-piscesclinical-trial-in-disabled-stroke-patients (2 June 2012, date last accessed).

Thank you





























