Embed Size (px)
Citation preview

ACS Critical Pathways 2007 Teleconferences
This activity is supported by an educational grant from the Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership.
February 14, 2007

2STRIVETM
Faculty
Gregg C. Fonarow, MDEliot Corday Professor of Medicine
and Cardiovascular ScienceDirector, Ahmanson-UCLA Cardiomyopathy Center
UCLA Division of CardiologyUCLA Medical Center
Los Angeles, California

3STRIVETM
Disclosure StatementThe Network for Continuing Medical Education requires
that CME faculty disclose, during the planning of an
activity, the existence of any personal financial or other
relationships they or their spouses/partners have with
the commercial supporter of the activity or with the
manufacturer of any commercial product or service
discussed in the activity.

4STRIVETM
Faculty Disclosure Statement
Gregg C. Fonarow, MD, has served as a consultant to and has received research support and honoraria from Bristol-Myers Squibb Company, GlaxoSmithKline, Merck & Co., Inc., Pfizer Inc, sanofi-aventis, Schering-Plough Corporation, and Scios, Inc.
Gary S. Ledley, MD, of Albert Einstein Medical Center and Thomas Jefferson University, reports no such relationships.

The NCDR-ACTION Registry:Combining the Power and Resources of
CRUSADE and NRMI
Gregg C. Fonarow, MD

6STRIVETM
Polling Question #1
1. Yes
2. No
Does your institution currently participate in an acute coronary syndromes registry?

7STRIVETM
NCDR-ACTION RegistryTM
In January 2007, the ACC (in conjunction with the Duke Clinical Research Institute) launched the National Cardiovascular Data Registry—Acute Coronary Treatment and Intervention Outcomes Network (NCDR-ACTIONTM)
Largest, most comprehensive national cardiovascular patient database ever developed
Overall purpose: measure clinically-relevant quality indicators in the treatment of ACS (STEMI and NSTEMI); promote national quality improvement
Combines data collection/quality reporting features of:
– NRMI (National Registry of Myocardial Infarction)
– CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress ADverse Outcomes with Early Implementation of the ACC/AHA Guidelines)
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

8STRIVETM
NCDR-ACTION RegistryTM Features Web-based data collection and download tool
Embedded data elements used for JCAHO/CMS reporting can be entered into the ACTION Registry™ and then downloaded for other uses
Quarterly comparative institutional outcomes reports to enable benchmarking with peers and the national experience
Participant training resources (user manuals, workshops, and annual user group meetings)
Tools to advance hospital quality improvement
No cost to participate – sponsored by Genentech, Schering-Plough, and BMS/Sanofi Partnership
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

9STRIVETM
NCDR-ACTION Data CollectionInclusion Criteria
Patients must present for acute ischemic symptoms (typically reflected by primary admission diagnosis of STEMI, NSTEMI)
Patients admitted for other reasons who develop ischemic symptoms and positive cardiac markers during hospitalization are not eligible
Patients who present with ischemic symptoms without positive markers on admission, may be included if they evolve ↑ cardiac markers in the first 24 hours of hospitalization
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

10STRIVETM
NCDR-ACTION Data CollectionPresentation Features to be Collected:
Arrival time at participating hospital Transfer in from an outside hospital? Patient transported by EMS? First 12-lead ECG obtained pre-hospital? ECG findings:
ST-depression (>0.5 mm) Transient ST-elevation (<1.0 mm) for <10 min New LBBB Persistent ST-elevation T-wave inversion
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

11STRIVETM
NCDR-ACTION Data CollectionPresentation Features to be Collected:
Location first evaluated? (refers to first evaluation at your hospital) Emergency department (ED) → Transferred from ED (if patient was first evaluated in
the ED, enter date/time patient was moved out of ED, either to another location within your hospital or to another acute care center)
ICU/CCU/Telemetry/Cardiac Floor Cath Lab Other/noncardiac
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

12STRIVETM
NCDR-ACTION Data CollectionSigns and Symptoms at Presentation:
Onset date and time of ischemic symptoms:______ Signs of Congestive Heart Failure (CHF)?
Mild CHF Severe CHF Cardiogenic Shock
Positive cardiac markers? (check if any present within first 24 hours of admission): Troponin I or T Creatine kinase-myocardial band (CK-MB) Positive bedside troponin assay
Heart rate on admission:_________ Systolic blood pressure on admission:_________
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

13STRIVETM
NCDR-ACTION Data CollectionDemographics:
Age___, Sex___, Wt___, Height___, Race_______
Hispanic origin? (check if patient reports a Cuban, Mexican, Puerto Rican, South or Central American, or any other Spanish culture or origin, regardless of race)
Insurance Status HMO/private? Medicare? Medicaid? Self/none? Military/VAMC?
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

14STRIVETM
NCDR-ACTION Data CollectionMedical History:
Hypertension? Diabetes mellitus? Peripheral arterial disease?
Claudication, either with exertion or at rest Amputation for arterial vascular insufficiency Vascular reconstruction, bypass surgery, or percutaneous intervention
to the extremities Documented aortic aneurysm Positive noninvasive (eg, ABI <0.8)
Current/recent smoker? Dyslipidemia? Prior MI, PCI, or CABG? Prior CHF? Prior stroke? Current dialysis?
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

15STRIVETM
NCDR-ACTION Data CollectionMedications (Check all that apply):
Home medications (check if the patient has been taking the medicine routinely at home prior to this hospitalization)
Medications in first 24 hours of treatment (enter date/time of initial dose and amount of dose) Aspirin _____________ Clopidogrel __________ Beta blocker ____________ ACE inhibitor ______________ Angiotensin Receptor Blocker (ARB) ________ Statin _____________ Other lipid-lowering agent (nonstatin) _______
Documented evidence of acute contraindication
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

16STRIVETM
NCDR-ACTION Data CollectionGP IIb-IIIa Inhibitor Type of Medication: Check if GP IIb-IIIa was administered during
the hospital stay. If yes, check the type of GP IIb-IIIa used: Eptifibatide (Integrilin); dose:_____________ Tirofiban (Aggrastat); dose: ______________ Abciximab (ReoPro); dose: ______________
Date and Time of Therapy Start (enter date/time of either the first bolus or beginning of infusion; if
patient was transferred to your hospital with therapy ongoing and initiation date/time unavailable, leave blank, but complete therapy stop time)
Stop (enter date/time infusion was permanently discontinued; do not record stop date/time if patient was transferred from your hospital with therapy ongoing)
Documented Evidence of Contraindication
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

17STRIVETM
NCDR-ACTION Data CollectionAnti-Thrombin Agent Type of Medication: Check if anti-thrombin was administered during
the hospital stay. If yes, check the type of anti-thrombin used: IV UFH (dose:__________) LMWH (dose: _____________) Bivalirudin (dose: ___________) Fondaparinux (dose: ____________)
Date and Time of Therapy IV UFH (enter date/time of 1st IV administration; do not record SC UFH) LMWH (Record date/time of 1st SC administration; Do not record IV
LMWH) Bivalirudin (Record date/time of 1st admin) Fondaparinux (Record date/time of 1st admin)
Documented Evidence of a Contraindication
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

18STRIVETM
NCDR-ACTION Data CollectionIn-Hospital Procedures Reperfusion Tx? (<12h from symptom onset?) If yes:
Thrombolytic therapy? (date/time of first bolus or beginning of infusion; indicate type of lytic first administered and the dose strength)
Primary PCI? (time patient arrived to cath lab where PCI performed; time first device activated): Time of first balloon inflation; if no balloon inflated, then time first stent
deployed, or Time of first treatment of lesion (eximer time, time rotablader used, time
angiojet, or other device) Stent placed? Indicate type and reason for PCI
If no reperfusion therapy administered, document evidence of contraindication
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

19STRIVETM
NCDR-ACTION Data CollectionIn-Hospital Procedures Noninvasive stress testing (refers to exercise or pharmacologic stress
testing with or without echo or radionuclide imaging) Date of procedure: _________
Diagnostic Cath: Enter date/time vascular access obtained or 1st time documented on cath report. Select all vessels with >50% stenosis, including native stenosis in vessels perfused by a graft. If stenosis located in a marginal branch, record location of stenosis as parent vessel: LM: Left main artery LAD: Left anterior descending artery LCX/CX: Left circumflex artery RCA: Right coronary artery Graft: Saphenous vein or artery, or internal mammary artery graft
If no cath, document evidence of contraindication
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

20STRIVETM
NCDR-ACTION Data CollectionIn-Hospital Procedures LVEF? If yes, enter result from cath or noninvasive imaging. If value reported as range
(eg, 40-45%), record lowest value (eg, 40%). If no numeric value given, record “normal, mild, or severe”
PCI (if not primary PCI for STEMI): Refers to balloon angioplasty, stenting, atherectomy, or laser intervention not used as a reperfusion strategy. Check “yes” if a guidewire was placed and device activated/inflated, even if final PCI result unsuccessful. If unable to place guidewire or activate a device, check “no.” If yes, indicate time of first balloon inflation. If no balloon inflated, indicate time first
stent deployed; or Time of first treatment of lesion (excimer time, time rotablader used, time angiojet,
or other thrombectomy device used) If stent was placed, check “yes” and indicate type of stent and primary reason PCI
was performed or attempted. CABG? If yes, enter date/time the patient entered O.R. or
first time documented on O.R. report
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

21STRIVETM
NCDR-ACTION Data CollectionIn-Hospital Clinical Events
For each clinical event, check “no” or “yes.” If yes, enter date of first occurrence, and answer all subquestions.
Death (Enter date/time of death; check “died” in discharge section.) Postadmission infarction (clinical signs/symptoms of new infarction or repeat infarction
distinct from presenting event and meeting at least one of the definitions below): In patients presenting without an MI:
CK-MB or troponin values above the ULN New, significant Q waves in at least 2 contiguous ECG leads
In patients presenting with an MI: Prior to revascularization
New, significant Q waves in >2 contiguous ECG leads An increase in CK-MB or troponin above the ULN (if most cardiac markers prior to
the event were normal) An increase in CK-MB or troponin by >50% above the recent value (if most recent
cardiac markers prior to the event were above the ULN)
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

22STRIVETM
NCDR-ACTION Data CollectionIn-Hospital Clinical Events
In patients presenting with an MI (continued): Within 24 hours of PCI
↑ in CK-MB >50% over level preceding the procedure (if most recent cardiac markers prior to procedure were above the ULN)
↑ in CK-MB to a value at least 3x the ULN (if most recent cardiac markers prior to procedure were normal)
New, significant Q waves in >2 contiguous ECG leads Within 24 hours of CABG
Increase in CK-MB to a value at least 5x the ULN New, significant Q waves in >2 contiguous ECG leads
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

23STRIVETM
NCDR-ACTION Data CollectionIn-Hospital Clinical Events
Cardiogenic shock? Congestive heart failure? Stroke?
Hemorrhagic? Witnessed bleeding event?
Event resulted in hemodynamic instability? Any RBC/whole blood transfusion?
Related to CABG?
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

24STRIVETM
NCDR-ACTION Data CollectionLaboratory Results Cardiac Markers
Total CPK value CK-MB: If CPK was ever abnormal, record CK-MB results:
Initial Sample (check “not done” or fill in date, value, ULN) Peak Sample (check “not done” or fill in date, value, ULN)
Troponin: Initial Sample (check “not done” or fill in date, value, ULN) Peak Sample (check “not done” or fill in date, value, ULN)
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

25STRIVETM
NCDR-ACTION Data CollectionLaboratory Results Initial Creatinine Hematocrit Values
Initial Lowest Recorded Sample
Hemoglobin A1C INR on Admission Lipids (ie, total cholesterol, HDL, LDL, TG) performed either
during this admission or within 6 months prior to hospitalization)
BNP Value
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

26STRIVETM
NCDR-ACTION Data CollectionDischarge Recommendations for Discharge: Check “yes” if documentation exists in the
medical chart that refers to discussion about smoking cessation, dietary modification, cardiac rehab referral, exercise counseling, or provision to patient of educational materials regarding these interventions Cardiac rehab referral Primary inpatient service during hospitalization (check specialty of
attending physician who primarily cared for patient according to most frequent and consistent notations in medical record)
Patient: Discharged (check “to home, rehab center, or extended care facility”;
enter date) Died Transferred to another acute-care center
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

27STRIVETM
NCDR-ACTION RegistryTM
Enrollment and data collection has started
First NCDR-ACTION Registry report will include first quarter 2007 (January to March 2007) data and is tentatively scheduled to be distributed in August 2007 and quarterly from that time forward
Current CRUSADE and NRMI participants will receive FAQs unique to their participation
For more information, contact the NCDR-ACTION Registry by e-mail or phone:
– 1-800-257-4737
ACC-NCDR 2007. Available at: www.accncdr.com/WebNCDR/Action/default.aspx

28STRIVETM
NCDR-ACTION Registry Sample Report: Guidelines Adherence
Sample Report:GuidelinesAdherence

29STRIVETM
NCDR-ACTION Registry Sample Report: Discharge Therapies
Sample Report:Discharge Therapies

STRIVETM
30
CRUSADE Update Can Rapid Risk Stratification of Unstable Angina Patients Suppress ADverse Outcomes with Early
Implementation of the ACC/AHA Guidelines

STRIVETM
31
Hospital Presentation Characteristics in CRUSADE:
October 1, 2005 – September 30, 2006 (n=31,613) Qualifying criteriaST-segment depression 28%Transient ST-segment elevation 5%Positive cardiac markers 93%
Baseline cardiac markers DrawnPositive
CK-MB 81%75%TnT/TnI 99%92%
Presenting characteristics Tachycardia 22%Hypotension 3%Signs of CHF 23%
Available at: http://www.crusadeqi.com.© 2007 Duke Clinical Research Institute. Adapted with permission.

STRIVETM
32
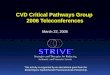
CRUSADE: Trends in Acute Therapy Adherence
Available at: http://www.crusadeqi.com.© 2007 Duke Clinical Research Institute. Adapted with permission.
98%92%
89%
48%
98%91% 87%
50%
0%
25%
50%
75%
100%
Antiplatelet β-Blocker Heparin GP IIb/IIIaInhibitor
Quarter 4-05 Quarter 1-06 Quarter 2-06 Quarter 3-06
Quarter 4, 2005, through Quarter 3, 2006.

STRIVETM
33
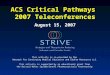
CRUSADE Data: October 1, 2005-September 30, 2006 (n=31,613)
CRUSADE: Invasive Cardiac Procedures October 1, 2005 – September 30, 2006 (n=31,613)
(Among Patients Without Contraindications to Cath)
Available at: http://www.crusadeqi.com.© 2007 Duke Clinical Research Institute. Adapted with permission.
84%
67%
53%
39%
12%
0%
20%
40%
60%
80%
100%
Cath Cath<48 hr
PCI PCI <48 hr CABG

STRIVETM
34
CRUSADE: Trends in Discharge Therapy Adherence
Quarter 4, 2005, through Quarter 3, 2006
Available at: http://www.crusadeqi.com.© 2007 Duke Clinical Research Institute. Adapted with permission.
93%
77%
93%
68%
90%
76%
93%
65%
90%96%
0%
25%
50%
75%
100%
Aspirin Clopidogrel β-Blocker ACE Inhibitor Lipid- Lowering
Agent
Quarter 4-05 Quarter 1-06 Quarter 2-06 Quarter 3-06

STRIVETM
35
CRUSADE: Trends in Discharge Recommendations Adherence
89%
80%
60%
85%
64%
88%
0%
25%
50%
75%
100%
Smoking CessationCounseling
Dietary Modification Cardiac RehabilitationReferral
Quarter 4-05 Quarter 1-06 Quarter 2-06 Quarter 3-06
Quarter 4, 2005, through Quarter 3, 2006. Available at: http://www.crusadeqi.com.© 2007 Duke Clinical Research Institute. Adapted with permission.

STRIVETM
36
CRUSADE: Overall Guideline Adherence Trends Over Time
Available at www.crusadeqi.com © 2007 Duke Clinical Research Institute. Adapted with permission.
Quarter 1 2002
Quarter 12003
Quarter 22004
Quarter 32005
Quarter 32006
68.1%73.0%
78.3%80.1% 83.3%
0%
25%
50%
75%
100%

STRIVETM
37
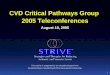
Performance Matters! Association Between Hospital Guideline
Adherence and In-Hospital Mortality in CRUSADE
Adapted with permission from Peterson ED, et al. JAMA. 2006;295:1912-1920.
NSTE ACS = non–ST-segment elevation ACS; NSTEMI = non–ST-segment elevation MI.
8
7
6
5
4
3
2
1
01 2 3 4
In-H
osp
ital
Mo
rtal
ity
, %
Hospital Composite GuidelineAdherence Quartiles
NSTE ACS 8
7
6
5
4
3
2
1
01 2 3 4
In-H
osp
ital
Mo
rtal
ity
, %
Hospital Composite GuidelineAdherence Quartiles
NSTEMI
CRUSADE = Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the ACC/AHA Guidelines.

38STRIVETM
Featured Institution
Albert Einstein Medical CenterPhiladelphia, Pennsylvania

STRIVETM
39
Polling Question #2
1. We are currently on the same item
2. We have since moved to the next checkbox on the checklist
3. We have progressed by more than one item on the checklist
4. ACS pathways are up-to-date and regularly followed
If you participated in a previous teleconference, how much progress have you made since then?
(Please refer to the checklists on the next 3 slides.)

STRIVETM
40
Progress Checklist:Immediate Goals
Assemble team and set up meeting of working group
Develop draft pathways
Circulate pathways to all cardiology, ED, and CV nursing staff for comments
Circulate discharge plan and other tools to all cardiology, ED, and CV nursing staff for comments

STRIVETM
41
Progress Checklist:Short-term Goals/Activities
Finalize critical pathways
Launch critical pathways
Circulate memo
Grand rounds/conference: Cardiology/IM
Grand rounds/conference: Emergency Dept.
Grand rounds/conference: Nursing

STRIVETM
42
Progress Checklist:Long-term Goals/Activities
Monitor data: Which registry?
NRMI
AHA Get With the Guidelines
ACC National Cardiovascular Data Registry
CRUSADE
GRACE
REACH
Other

STRIVETM
43
Question-and-Answer Session

STRIVETM
44
Concluding RemarksGregg C. Fonarow, MD
Next ProgramGregg C. Fonarow, MD
Wednesday, March 14, 20073:00 PM Eastern Time
(12:00 Noon Pacific Time)AHA Get With The Guidelines:
New Guidelines, New Challenges