Embed Size (px)
Citation preview

ACS Critical Pathways 2007 Teleconferences
This activity is supported by an educational grant from the Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership.
This activity is co-provided by the Network for Continuing Medical Education and EduPro Resources LLC.
APRIL 11, 2007

STRIVETM
2
Faculty
Christopher P. Cannon, MDAssociate Professor of Medicine
Harvard Medical School
Senior Investigator, TIMI Study Group
Associate Physician, Cardiovascular Division
Brigham and Women’s Hospital
Boston, Massachusetts

STRIVETM
3
The Network for Continuing Medical Education and
EduPro Resources LLC require that CME/CNE faculty
disclose, during the planning of an activity, the existence
of any personal financial or other relationships they or
their spouses/partners have with the commercial
supporter of the activity or with the manufacturer of any
commercial product or service discussed in the activity.
Disclosure Statement

STRIVETM
4
Christopher P. Cannon, MD, has served as a consultant to Abbott Laboratories, Alnylam Pharmaceuticals, Arena Pharmaceuticals, AstraZeneca Pharmaceuticals LP, Biosite, Bristol-Myers Squibb Company, Eisai Inc., GlaxoSmithKline, Johnson & Johnson, Merck & Co., Inc., Pfizer Inc, sanofi-aventis, Schering-Plough Corporation, Tethys Bioscience, and Vertex Pharmaceuticals. He has received honoraria from Accumetrics, AstraZeneca Pharmaceuticals LP, BGB New York, Bristol-Myers Squibb Company, DIME, Genentech, Inc., Merck & Co. Inc., Pfizer Inc, sanofi-aventis, and Schering-Plough Corporation, and has received research support from Accumetrics, AstraZeneca Pharmaceuticals LP, Merck & Co., Inc., and Schering-Plough Corporation.
The team from Aurora St. Luke's Medical Center reports no such relationships.
Faculty Disclosure Statement

Highlights From the American College of Cardiology
2007 Annual Scientific Session
Christopher P. Cannon, MD

STRIVETM
6
Highlights From ACC 2007 COURAGE: Clinical Outcomes Utilizing Revascularization and
Aggressive Guideline-Driven Drug Evaluation MERLIN TIMI-36: Metabolic Efficiency with Ranolazine for
Less Ischemia in Non-ST Elevation Acute Coronary Syndromes
Danish Registry: More data on late stent thrombosis in DES-treated patients
An International Risk Prediction Model for Recurrent CV Events in REACH: Reduction of Atherothrombosis for Continued Health
ACUITY: Acute Catheterization and Urgent Intervention Triage StrategY (1 year results)

STRIVETM
7
COURAGEClinical Outcomes Utilizing Revascularization
and Aggressive Guideline-DrivenDrug Evaluation

STRIVETM
8
COURAGE: Background
Every year, more than 1 million PCI procedures are performed in the US
– The majority are undertaken electively in patients with stable CAD
Successful PCI of flow-limiting stenoses might be expected to reduce the rate of death, MI or hospitalization for ACS, however:
– Prior studies have shown only that PCI decreases the frequency of angina and improves short-term exercise performance
Boden WE, et al. N Engl J Med. 2007;356. Published online March 27, 2007.

STRIVETM
9
35,539 patients underwent assessment35,539 patients underwent assessment
1149 to PCI + OMT group
COURAGE: Study Design
32,468 excluded for not meeting inclusion criteria, logistics, or for >1 exclusions
Randomize
1138 to OMT alone group
Primary Outcome: Death or nonfatal MISecondary Outcomes: Death, MI, or stroke
Hospitalization for biomarker (-) ACSCost, resource utilization
Quality of life, including anginaCost-effectiveness
Primary Outcome: Death or nonfatal MISecondary Outcomes: Death, MI, or stroke
Hospitalization for biomarker (-) ACSCost, resource utilization
Quality of life, including anginaCost-effectiveness
Intensive, guideline-driven medical therapy and lifestyle intervention in both groups
N = 2287
Boden WE, et al. N Engl J Med. 2007;356. Published online March 27, 2007.
3071 met eligibility criteria2287 consented to participate
2.5 to 7 year (mean 4.6 year) follow-up

STRIVETM
10
COURAGE: Inclusion and Exclusion Criteria
Men and women 1, 2, or 3 vessel disease
(>70% visual stenosis of proximal coronary segment)
Anatomy suitable for PCI CCS class I-III angina Objective evidence of
ischemia at baseline ACC/AHA class I or II
indication for PCI
Uncontrolled unstable angina
Complicated post-MI course Revascularization within 6
months Ejection fraction <30% Cardiogenic shock/severe
heart failure History of sustained or
symptomatic VT/VF Severe non-CV comorbidity
limiting survival
Boden WE, et al. N Engl J Med. 2007;356. Published online March 27, 2007.
Inclusion Criteria Exclusion Criteria
CCS = Canadian Cardiovascular Society

STRIVETM
11
COURAGE: Other Criteria Objective Evidence of Ischemia
– Spontaneous ST-T changes on ECG
– >1 mm ST deviation on treadmill test
– Ischemic imaging defect
Coronary Intervention
– Best practice
– May use all FDA or Health Canada approved devices
– Completeness of revascularization as clinically appropriate
Boden WE, et al. N Engl J Med. 2007;356. Published online March 27, 2007.

STRIVETM
12
COURAGE: Risk Factor GoalsVariable Goal
Smoking Cessation
Total Dietary Fat / Saturated Fat <30% calories / <7% calories
Dietary Cholesterol <200 mg/day
LDL-C (primary goal) 60-85 mg/dL
HDL-C (secondary goal) >40 mg/dL
Triglyceride (secondary goal) <150 mg/dL
Physical Activity 30-45 min. moderate intensity 5x/week
Body Weight by BMI Initial BMI Weight Loss Goal 25-27.5 BMI <25 >27.5 10% relative weight loss
Blood Pressure <130/85 mm Hg
Diabetes HbAlc <7.0%
Boden WE, et al. N Engl J Med. 2007;356. Published online March 27, 2007.

STRIVETM
13
COURAGE: Optimal Medical Therapy*
Category Agents
Antiplatelet Aspirin Clopidogrel in accordance
with established practice standards
Statin Simvastatin ± ezetimibe or extended-release niacin
ACE Inhibitor or ARB Lisinopril or losartan
Beta blocker Long-acting metoprolol
Calcium channel blocker Amlodipine
Nitrate Isosorbide 5-mononitrate
Boden WE, et al. N Engl J Med. 2007;356. Published online March 27, 2007.
*Applied to both arms by protocol and case-managed.

STRIVETM
14
COURAGE: Baseline Demographic Characteristics
Characteristic PCI + OMT (N = 1149) OMT (N = 1138) P value
Age (y)
Sex (n, %)
Male
Female
Race or ethnic (n, %)
White
Black
Hispanic
Other
61.5±10.1
979 (85)
169 (15)
988 (86)
57 (5)
68 (6)
35 (3)
61.8±9.7
968 (85)
169 (15)
975 (86)
57 (5)
58 (5)
47 (4)
.54
.95
.64
Boden WE, et al. N Engl J Med. 2007;356. Published online March 27, 2007.

STRIVETM
15
COURAGE: Baseline Characteristics – AnginaCharacteristic PCI + OMT (N = 1149) OMT (N = 1138) P value
Angina CCS class (no, %)
0
I
II
III
Missing data
Duration of angina (months)
Median
Interquartile range
Episodes/week with exertion or at rest within last month
Median
Interquartile range
135 (12)
340 (30)
409 (36)
261 (23)
3 (<1)
5
1-15
3
1-6
148 (13)
341 (30)
425 (37)
221 (19)
2 (<1)
5
1-15
3
1-6
.24
.53
.83
Boden WE, et al. N Engl J Med. 2007;356. Published online March 27, 2007.

STRIVETM
16
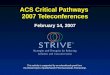
COURAGE: Survival Free of Death From Any Cause and MI
No. at Risk
OMT 1138 1017 959 834 638 408 192 30PCI+OMT 1149 1013 952 833 637 417 200 35
Years
0 1 2 3 4 5 6
0.0
0.5
0.6
0.7
0.8
0.9
1.0
PCI + OMT: 19%*
OMT: 18.5%* Hazard ratio: 1.0595% CI (0.87-1.27)P = .62
7
Boden WE, et al. N Engl J Med. 2007;356. Published online March 27, 2007.
Su
rviv
al F
ree
of
Dea
th F
rom
A
ny
Cau
se a
nd
MI
*Cumulative event rates at a median of 4.6 years.

STRIVETM
17
COURAGE: Cumulative Event Rates at a Median of 4.6 Years
<.0010.51–0.710.6032.621.1Revasc.(PCI or CABG)
.560.84–1.371.0711.812.4Hospitalization for ACS
.190.80–3.041.56 1.8 2.1Stroke
.330.89–1.431.1312.313.2Nonfatal MI
.380.65–1.160.87 8.3 7.6Death
.620.87–1.271.0519.520 Death, MI, stroke
.620.87–1.271.05 18.519Death, MI
Pvalue
95% CI Hazard ratio
OMT(%)
PCI + OMT (%)
Outcome
Boden WE, et al. N Engl J Med. 2007;356. Published online March 27, 2007.

STRIVETM
18
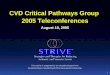
COURAGE: Overall Survival
No. at Risk
OMT 1138 1073 1029 917 717 468 302 38PCI+OMT 1149 1094 1051 929 733 488 312 44
Years0 1 2 3 4 5 6
0.0
0.5
0.6
0.7
0.8
0.9
1.0 PCI + OMT: 7.6%*
OMT: 8.3%*
7
Hazard ratio: 0.8795% CI (0.65-1.16)P = .38
Boden WE, et al. N Engl J Med. 2007;356. Published online March 27, 2007.
Ove
rall
Su
rviv
al
*Cumulative event rates at a median of 4.6 years.

STRIVETM
19
COURAGE: Freedom From Angina During Long-term Follow-up
Time Point (y) PCI + OMT OMT P value
Baseline 12% 13% NS
1 y 66% 58% <.001
3 y 72% 67% .02
5 y 74% 72% NS
Boden WE, et al. N Engl J Med. 2007;356. Published online March 27, 2007.

STRIVETM
20
COURAGE: Conclusions
As an initial management strategy in patients with stable coronary artery disease, PCI did not reduce the risk of death, MI, or other major cardiovascular events when added to optimal medical therapy
PCI resulted in better angina relief during most of the follow-up period, but medical therapy was also effective, with no between–group difference in angina-free status at 5 years
Boden WE, et al. N Engl J Med. 2007;356. Published online March 27, 2007.

STRIVETM
21
MERLIN TIMI-36Metabolic Efficiency with Ranolazine for Less
Ischemia in Non-ST ElevationAcute Coronary Syndromes

STRIVETM
22
MERLIN TIMI-36: Background
Despite advances in antithrombotic therapies and invasive technology, risk of recurrent ischemic complications in patients with NSTE-ACS remains substantial
Ranolazine is a novel agent that inhibits the late sodium current thereby reducing cellular sodium and calcium overload; has been shown to reduce ischemia in patients with chronic stable angina
MERLIN TIMI-36 was designed to evaluate the safety and efficacy of long-term treatment with ranolazine compared with placebo in NSTE-ACS
Morrow DA, et al. Am Heart J. 2006;151:1186.

STRIVETM
23
Follow-up visits: Day 14, Month 4, Q4 Months
Placebo (n = 3,281) Matched IV/PORanolazine (n = 3,279) IV → PO
Standard Therapy for ACS
Morrow DA, et al. Am Heart J. 2006;151:1186.
UA/NSTEMI (N = 6560)1) Rest symptoms within 48 h 2) High-risk features
MERLIN TIMI-36: Study Design
Holter monitoring at enrollment x 7d
Final Visit
Additional end points: Exercise performance, new/worsening heart failure, quality of life, extent of myocardial injury, clinically significant arrhythmia.
DurationEvent-driven
Mean Follow-up: Median, 348 Days
Primary end point: Composite of CV death, MI, or recurrent ischemiaSecondary end point: Composites of CV death, MI, severe recurrent
ischemia; and positive Holter at 30 days

STRIVETM
24
MERLIN: Efficacy Results
End pointPlacebo
(n = 3281)
Ranolazine(n = 3279)
Hazard Ratio
P value
CV death/recurrent ischemia (primary end point)
23.5 21.8 0.92 .11
CV death/MI 10.5 10.4 0.99 .87
Recurrent ischemia 16.1 13.9 0.87 .030
Morrow D, et al. Presented at: American College of Cardiology 2007 Scientific Sessions; March 27, 2007; New Orleans, Louisiana.

STRIVETM
25
MERLIN: Safety Results
End pointPlacebo
(n = 3273)Ranolazine(n = 3268)
Hazard ratio
P value
Death, any cause(number of patients)
175 172 0.99 .91
Sudden cardiac death (number of patients)
65 56 0.87 .43
Symptomatic documented arrhythmia
(number of patients)
102 99 0.97 .84
Clinically significant arrhythmia on Holter(% of patients)
83.1% 73.1% 0.89 <.001
Morrow D, et al. Presented at: American College of Cardiology 2007 Scientific Sessions; March 27, 2007; New Orleans, Louisiana.

STRIVETM
26
MERLIN: Conclusions
In NSTE-ACS, no difference between ranolazine and placebo in death or MI, but improvements in recurrent ischemia with ranolazine
Reduced need for anginal therapy intensification with ranolazine
No adverse trend in death or arrhythmia with ranolazine; suggestion of possible antiarrhythmic effect with ranolazine
Study supports use of ranolazine in stable disease

STRIVETM
27
Danish Registry

STRIVETM
28
Danish Registry: Background
Use of drug-eluting stents (DES) recently associated with increased risk of stent thrombosis
Based on Academic Research Consortium (ARC) definition, Maeng, et al reported on the incident of stent thrombosis in patients treated with DES (sirolimus- and paclitaxel-eluting) and bare-metal stents (BMS) in Western Denmark
Maeng M, et al. Presented at: American College of Cardiology 2007 Scientific Sessions; March 24, 2007; New Orleans, Louisiana.

STRIVETM
29
Academic Research Consortium: Proposed Definitions for Stent Thrombosis
*Acute/Subacute can also be replaced by early stent thrombosis. Early stent thrombosis = 0-30 days.
Cutlip D. Presented at TCT; October 2006; Washington, DC.
Expanded Stent Thrombosis Definition
Timing
Acute Thrombosis*: 0 – 24 hrs. post
Subacute Thrombosis*: >24 hrs – 30 days post
Late Thrombosis: 30 days – 1 year post
Very Late Thrombosis: >1 year post
1. Definite/Confirmed2. Probable3. Possible

STRIVETM
30
Academic Research Consortium: Proposed Definitions for Stent Thrombosis
The incidental angiographic documentation of stent occlusion in the absence of clinical syndromes is not considered a confirmed stent thrombosis (silent thrombosis).
Cutlip D. Presented at TCT; October 2006; Washington, DC.
1. Definite/Confirmed
Autopsy evidence or angiographic confirmed stent thrombosis (definite) is considered to have occurred if:1. TIMI flow is:
a) Grade 0 with occlusion originating in the stent or segment 5 mm proximal or distal to the stent region in the presence of thrombus
b) Grade 1, 2, 3 originating in the stent or in the segment 5 mm proximal or distal to the stent region in the presence of thrombus
AND at least one of the following criteria within 48 hrs:2. New onset of ischemic symptoms at rest (typical chest pain with duration
>20 minutes)3. New ischemic ECG changes suggestive of acute ischemia4. Typical rise and fall in cardiac biomarkers (>2x ULN of CK)

STRIVETM
31
Academic Research Consortium: Proposed Definitions for Stent Thrombosis
Cutlip D. Presented at TCT; October 2006; Washington, DC.
Probable stent thrombosis is considered to have occurred in the following cases:1. Any unexplained death within the first 30 days.2. Irrespective of the time after the index procedure, any MI in the absence
of any obvious cause which is related to documented acute ischemia in the territory of the implanted stent without angiographic confirmation of stent thrombosis.
Possible stent thrombosis is considered to have occurred with any unexplained death beyond 30 days.
3. Possible
2. Probable

STRIVETM
32
Danish Registry: Results
End pointBMS (%)
(n = 8847)DES (%) (n = 3268)
Adj. RR
P value
Target lesion revascularization
7.1 4.6 0.57 <.0001
Overall probable, possible, or definite stent thrombosis (ARC definition)
2.15 1.8 0.92 NS
Definite stent thrombosis, 12-15 months
0.009 0.09 10.9 .029
Overall death 6.2 4.4 0.90 .29
Overall MI 3.0 3.2 1.14 .31
MI, 12-15 months Data notPresented
Data notPresented 4.0 <.0001
Maeng M, et al. Presented at: American College of Cardiology 2007 Scientific Sessions; March 24, 2007; New Orleans, Louisiana.

STRIVETM
33
Danish Registry: Conclusions
After 15 months, the investigators noted no overall differences in rates of stent thrombosis or death and MI between DES and BMS
After clopidogrel was discontinued at 12 months, rates of stent thrombosis and MI were significantly higher in DES-treated patients
These findings are consistent with other recent studies
Maeng M, et al. Presented at: American College of Cardiology 2007 Scientific Sessions; March 24, 2007; New Orleans, Louisiana.

STRIVETM
34
REACH Update: An International Risk Prediction
Model for Recurrent CV EventsReduction of Atherothrombosis for Continued Health (International Risk Reduction Model
for Recurrent CV Events)

STRIVETM
35
REACH CV EventsPrediction Model: Background
The capability of CV risk factors to predict recurrent CV events in a “real world” setting not well characterized
REACH is an international, prospective cohort of 68,236 patients with either established atherosclerotic arterial disease (CAD, PAD, CVD) or at least 3 risk factors for atherothrombosis
REACH provides a global, well-defined, outpatient population with known CV disease
Wilson PW. Presented at: American College of Cardiology 2007 Scientific Sessions; March 27, 2007; New Orleans, Louisiana.

STRIVETM
36
REACH CV EventsPrediction Model: Methods
A prediction model was developed based on 18,802 men and 9,430 women with known CV disease (CAD, CVD, and/or PAD) at entry from North America/Western Europe– Full baseline and 10-year data were available
At 1 year, 709 CV events (CV death, MI, stroke) in men and 417 in women were reported
A single sex-adjusted model was developed since results were similar in separate sex models
Wilson PW. Presented at: American College of Cardiology 2007 Scientific Sessions; March 27, 2007; New Orleans, Louisiana.

STRIVETM
37
REACH: Multivariable-adjusted HR and P Value for Variables Considered
Variable (unit) HR per unit P value
Gender (male) 1.02 .7087
Age (year) 1.03 <.0001
Smoking (current vs other) 1.42 <.0001
Diabetes (yes/no) 1.60 <.0001
1, 2 or 3 vasc. beds (CAD, CVD, PAD) 1.00, 1.20, 1.44 .0013
CV event in past year (yes/no) 1.47 <.0001
Cardiac failure (yes/no) 1.78 <.0001
Statins (yes/no) .72 <.0001
Acetyl salicylic acid (yes/no) .87 .0352
Hypertension therapy (yes/no) 1.18 .2187
Morrow D, et al. Presented at: American College of Cardiology 2007 Scientific Sessions; March 27, 2007; New Orleans, Louisiana.
Number at risk: 27,632; Number of events: 1,126.

STRIVETM
38
REACH CV Events Prediction Model: Results/Conclusions
Statin therapy, number of vascular beds affected, diabetes, smoking, cardiac failure and history of CV event(s) <1 year were significantly associated with next CV event
This prediction model is the first to estimate risk for recurrent CV events in outpatients
Risk factors, burden of disease, and treatment are all related to increased risk for a subsequent CV event
Wilson PW. Presented at: American College of Cardiology 2007 Scientific Sessions; March 27, 2007; New Orleans, Louisiana.

STRIVETM
39
ACUITY: One Year ResultsAcute Catheterization and Urgent Intervention
Triage StrategY

STRIVETM
40
ACUITY: Patient Follow-up at 1 Year*
Heparin + GP IIb/IIIa4,603
Bivalirudin + GP IIb/IIIa4,604
Bivalirudin alone4,612
All patientsN = 13,819
25 Withdrawn62 Lost to Follow-up
Heparin + IIb/IIIa4,516 (98.1%)
1-year FU
Bivalirudin + IIb/IIIa4,502 (97.8%)
1-year FU
Bivalirudin alone4,521 (98.0%)
1-year FU
33 Withdrawn69 Lost to Follow-up
25 Withdrawn66 Lost to Follow-up
R
*End points adjudicated: Composite ischemia(death, MI, unplanned revasc) and stent thrombosis
Stone GW. Presented at: American College of Cardiology 2007 Scientific Sessions; March 26, 2007; New Orleans, Louisiana.

STRIVETM
41
0 30 60 90 120 150 180 210 240 270 300 330 360 3900
5
15
25
Isch
emic
Co
mp
osi
te (
%)
Days From Randomization
10
20UFH/Enoxaparin + IIb/IIIa
Bivalirudin + IIb/IIIaBivalirudin alone
EstimateP
(log rank)
30-day
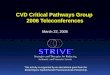
7.4%.367.8%.347.9%
—
EstimateP
(log rank)
16.3%.3816.5%.3116.4%
1-year
—
P = .55
Bivalirudin alone vs Hep + GPIHR [95% CI] = 1.05 (0.95-1.17)
Bivalirudin + GPI vs Hep + GPIHR [95% CI] = 1.05 (0.94-1.16)
ACUITY: Ischemic Composite End Point(Death, MI, unplanned revascularization for ischemia)
UFH/Enoxaparin + GPI vs Bivalirudin + GPI vs Bivalirudin AloneUFH/Enoxaparin + GPI vs Bivalirudin + GPI vs Bivalirudin Alone
Stone GW. Presented at: American College of Cardiology 2007 Scientific Sessions; March 26, 2007; New Orleans, Louisiana.

STRIVETM
42
0 30 60 90 120 150 180 210 240 270 300 330 360 3900
3
4
5
Ste
nt
Th
rom
bo
sis
(%
)
Days From Randomization
2
1
ACUITY: Stent Thrombosis (Protocol Defn.)
Drug-eluting Stents (DES) vs Bare-Metal Stents (BMS)Drug-eluting Stents (DES) vs Bare-Metal Stents (BMS)
EstimateP
(log rank)
≥1 DES (N = 4630).38
2.2%
1-year
All BMS (N = 2528) 2.3%
All (N = 7158) 2.2%
Stone GW. Presented at: American College of Cardiology 2007 Scientific Sessions; March 26, 2007; New Orleans, Louisiana.

STRIVETM
43
Mo
rtal
ity
(%)
Days From Randomization
0 30 60 90 120 150 180 210 240 270 300 330 360 3900
5
15
30
10
25
20
1-yearEstimate
Major Bleed only (without MI) (N = 551) 12.5%28.9%Both MI and Major Bleed (N = 94)
3.4%No MI or Major Bleed (N = 2,557)MI only (without Major Bleed) (N = 611) 8.6%
ACUITY: Impact of MI and Major Bleeding(non-CABG) in the First 30 Days on Risk of
Death Over 1 Year
28.9%
12.5%
8.6%
3.4%
Stone GW. Presented at: American College of Cardiology 2007 Scientific Sessions; March 26, 2007; New Orleans, Louisiana.

STRIVETM
44
ACUITY: Conclusions• In patients with moderate and high risk ACS
undergoing an early invasive strategy with the use of GP IIb/IIIa inhibitors
• Bivalirudin is an acceptable substitute for either unfractionated heparin or enoxaparin
• Compared to either UFH/enoxaparin with GP IIb/IIIa inhibitors or bivalirudin with GP IIb/IIIa inhibitors
• A bivalirudin alone strategy results in marked reduction of bleeding at 30 days, and similar rates of mortality and composite ischemia at 1 year
• The results of this study further establish the important relationship between iatrogenic bleeding complications and subsequent mortality in patients with ACS
Stone GW. Presented at: American College of Cardiology 2007 Scientific Sessions;March 26, 2007; New Orleans, Louisiana.

STRIVETM
45
Featured InstitutionAurora St. Luke’s Medical Center
Milwaukee, Wisconsin

STRIVETM
46
Polling Question #2
1) We are currently on the same item
2) We have since moved to the next checkbox on the checklist
3) We have progressed by more than one item on the checklist
4) ACS pathways are up-to-date and regularly followed
If you participated in a previous teleconference, how much progress have you made since then?
(Please refer to the checklists on the next 3 slides.)

STRIVETM
47
Progress Checklist:Immediate Goals
Assemble team and set up meeting of working group
Develop draft pathways
Circulate pathways to all cardiology, ED, and CV nursing staff for comments
Circulate discharge plan and other tools to all cardiology, ED, and CV nursing staff for comments

STRIVETM
48
Progress Checklist:Short-term Goals/Activities
Finalize critical pathways
Launch critical pathways
Circulate memo
Grand rounds/conference: Cardiology/IM
Grand rounds/conference: Emergency Dept.
Grand rounds/conference: Nursing

STRIVETM
49
Progress Checklist:Long-term Goals/Activities
Monitor data: which registry?
NRMI AHA Get With The Guidelines ACC National Cardiovascular Data Registry CRUSADE GRACE REACH Other

STRIVETM
50
Question-and-Answer Session

STRIVETM
51
Concluding RemarksChristopher P. Cannon, MD
Next ProgramChristopher P. Cannon, MD
Wednesday, May 16, 200712:00 Noon Eastern Time
(9:00 AM Pacific Time)
The AHA/ACC/SCAI/ACS/ADA Science Advisory on Prevention of Premature Discontinuation of Dual Antiplatelet
Therapy in Patients With Coronary Artery Stents
















![AmFam Teleconf 4 -- Marketing Tools Business Accelerator[1]](https://img.pdfslide.us/doc/110x75/5553337bb4c90555308b4b4a/amfam-teleconf-4-marketing-tools-business-accelerator1.jpg)






![AVMARK NL Apr11[1].PDF Final Copy](https://img.pdfslide.us/doc/110x75/54f8df564a79599a0e8b48ee/avmark-nl-apr111pdf-final-copy.jpg)

