Embed Size (px)
Citation preview
Social Cognition inPediatric-Onset MS
Leigh Charvet, Rebecca Cleary, Katherine Vazquez, Livana Koznesoff, Kate Bartolotta, Jeremy
Benhamroum & Lauren Krupp for the
U.S. Network of Pediatric MS Centers
Lourie Center for Pediatric MS, Stony Brook Medicine
Supported by the National MS Society (grant numbers PP2106, 10020073405); NIH (grant number R01NS071463); The Lourie Foundation, Inc.
Social cognition
• Cognitive processes that guide social interaction
• Theory of mind (ToM) is core construct – infer another’s mental state, making attributions to
their knowledge, beliefs, and emotions– affective and cognitive
Social cognitive deficits
• Characterize autism spectrum disorders, frontal lobe injury, schizophrenia
• More recent studies have found often subtle deficits in a wide range of neurodegenerative conditions
Social cognition in adults with MS
• Deficits found in:– Accurate attribution of the mental state of others– Accurate recognition of emotions, intentions
• Cognitively intact participants • Independent from – disease duration– level of neurologic impairment (EDSS)– fatigue and depressed mood
Pilot study objective
• To determine whether pediatric-onset MS is associated with impaired social cognition
• Pediatric-onset (less than 18 years):– Youngest MS subpopulation– Approximately one-third with cognitive
impairment
• Social cognition especially critical for this age group
Participants
• Pediatric-onset MS participants under the age of 21 years– No other primary neurologic, psychiatric or
medical condition– Steroid-free for 30 days or more and
neurologically stable
• Healthy controls participants– Recruited from community
Measures
• Symbol Digit Modalities Test (SDMT) • ToM– False Beliefs Task– Reading the Mind in the Eyes Test– Faux Pas Test
• Parent behavior inventory– Empathizing/Systematizing (EQ-SQ)
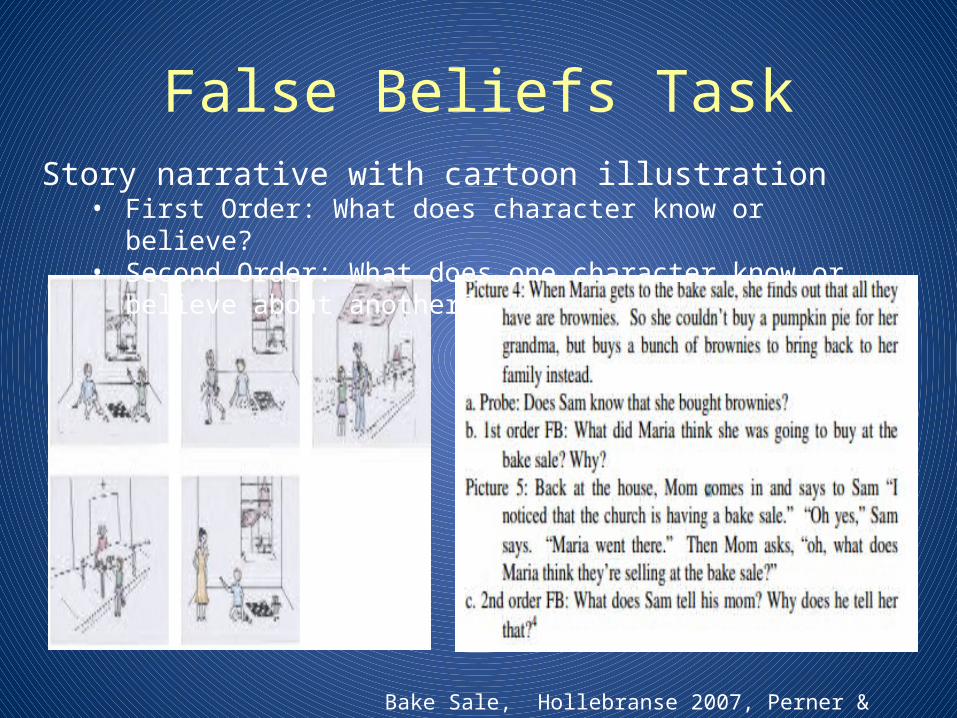
False Beliefs TaskStory narrative with cartoon illustration
• First Order: What does character know or believe?• Second Order: What does one character know or believe about another?
Bake Sale, Hollebranse 2007, Perner & Wimmer, 1985
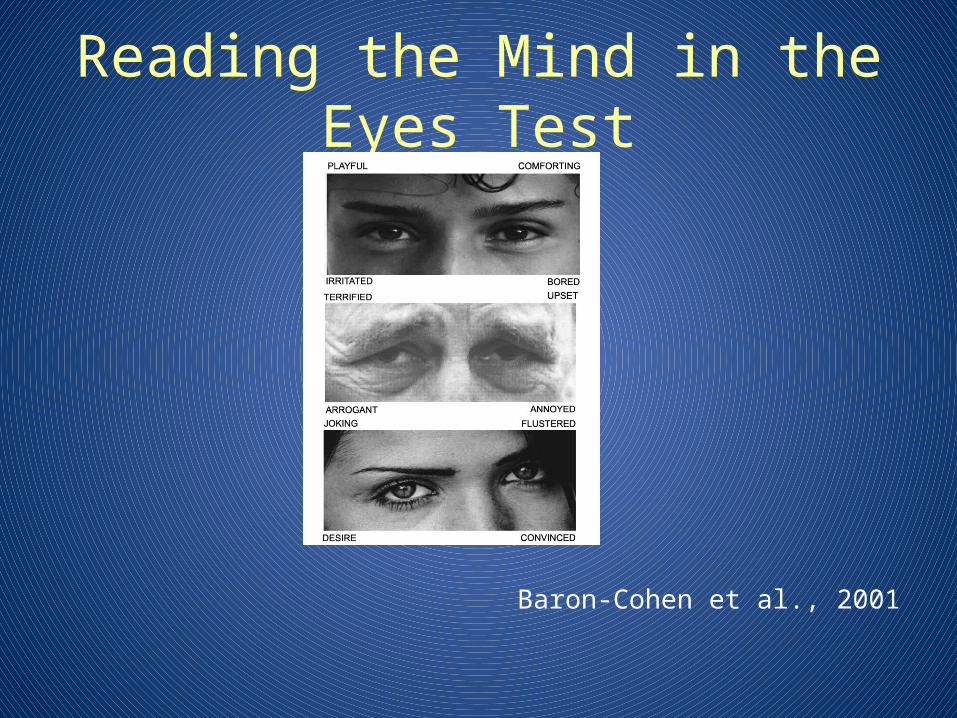
Reading the Mind in the Eyes Test
Baron-Cohen et al., 2001
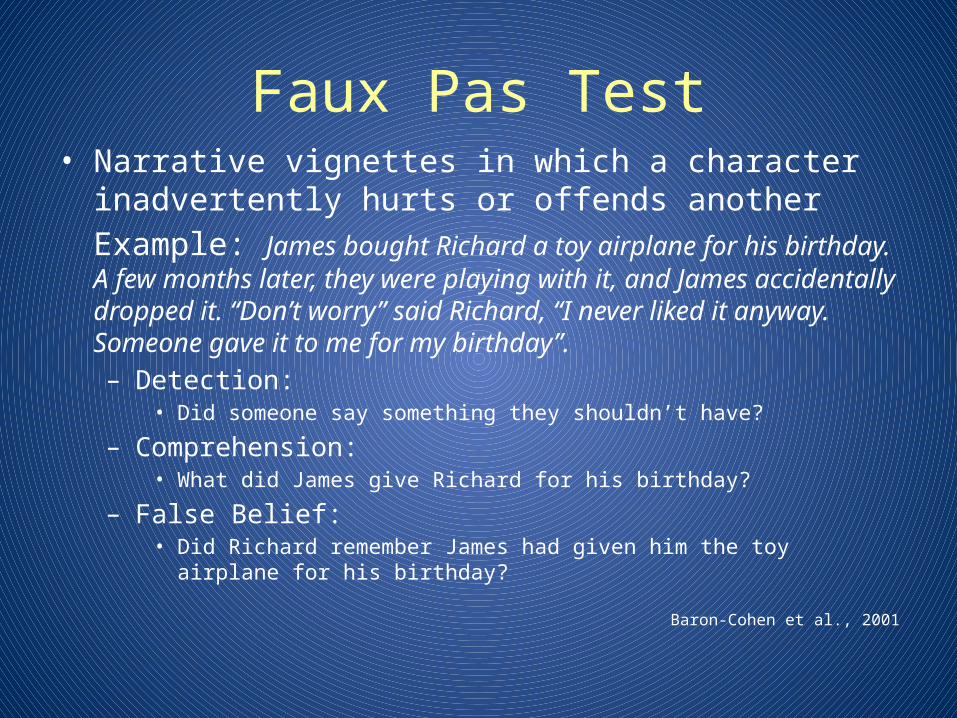
Faux Pas Test• Narrative vignettes in which a character inadvertently hurts or
offends another Example: James bought Richard a toy airplane for his birthday. A few months later, they were playing with it, and James accidentally dropped it. “Don’t worry” said Richard, “I never liked it anyway. Someone gave it to me for my birthday”. – Detection:
• Did someone say something they shouldn’t have?
– Comprehension: • What did James give Richard for his birthday?
– False Belief: • Did Richard remember James had given him the toy airplane for his birthday?
Baron-Cohen et al., 2001
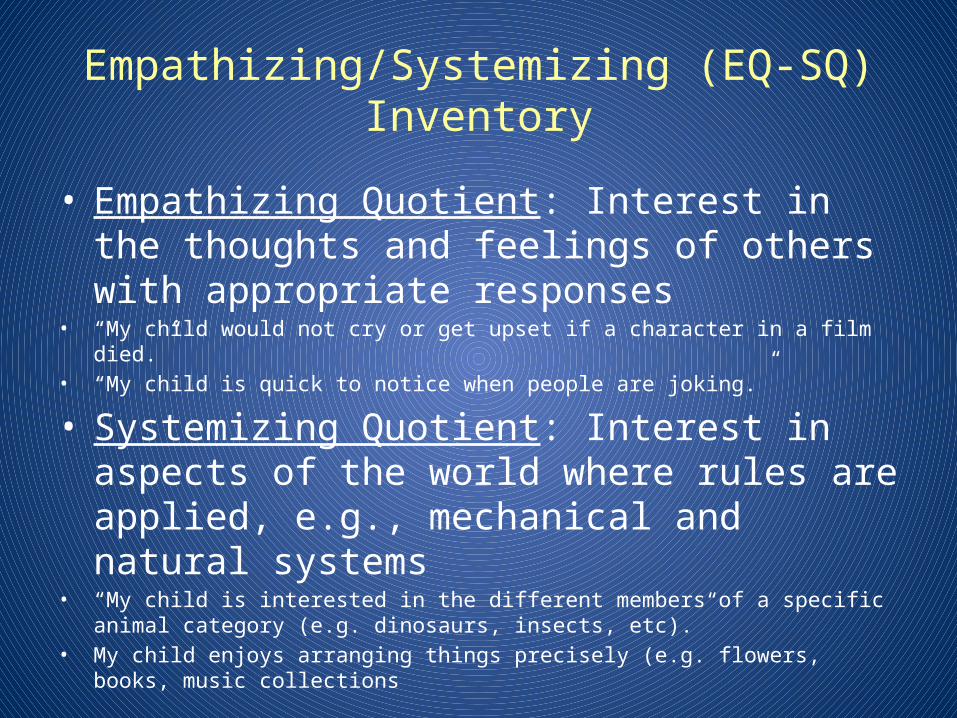
Empathizing/Systemizing (EQ-SQ) Inventory
• Empathizing Quotient: Interest in the thoughts and feelings of others with appropriate responses
• “My child would not cry or get upset if a character in a film died.”• “My child is quick to notice when people are joking.”
• Systemizing Quotient: Interest in aspects of the world where rules are applied, e.g., mechanical and natural systems
• “My child is interested in the different members of a specific animal category (e.g. dinosaurs, insects, etc).”
• My child enjoys arranging things precisely (e.g. flowers, books, music collections
• Baron-Cohen et al., 2005
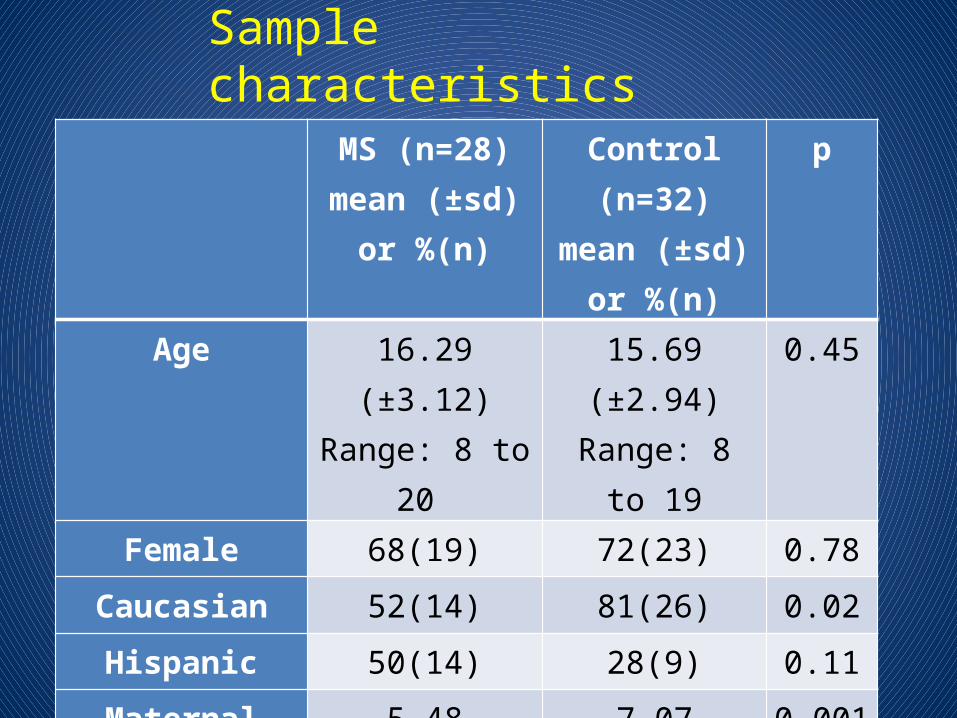
Sample characteristics MS (n=28)
mean (±sd) or %(n)
Control (n=32)mean (±sd) or
%(n)
p
Age 16.29 (±3.12)Range: 8 to 20
15.69 (±2.94)Range: 8 to 19
0.45
Female 68(19) 72(23) 0.78
Caucasian 52(14) 81(26) 0.02
Hispanic 50(14) 28(9) 0.11
Maternal Education
5.48 (±1.89) 7.07 (±1.24) 0.001
WASI FSIQ 103.29 (±12.67) 108.06 (±13.82) 0.21
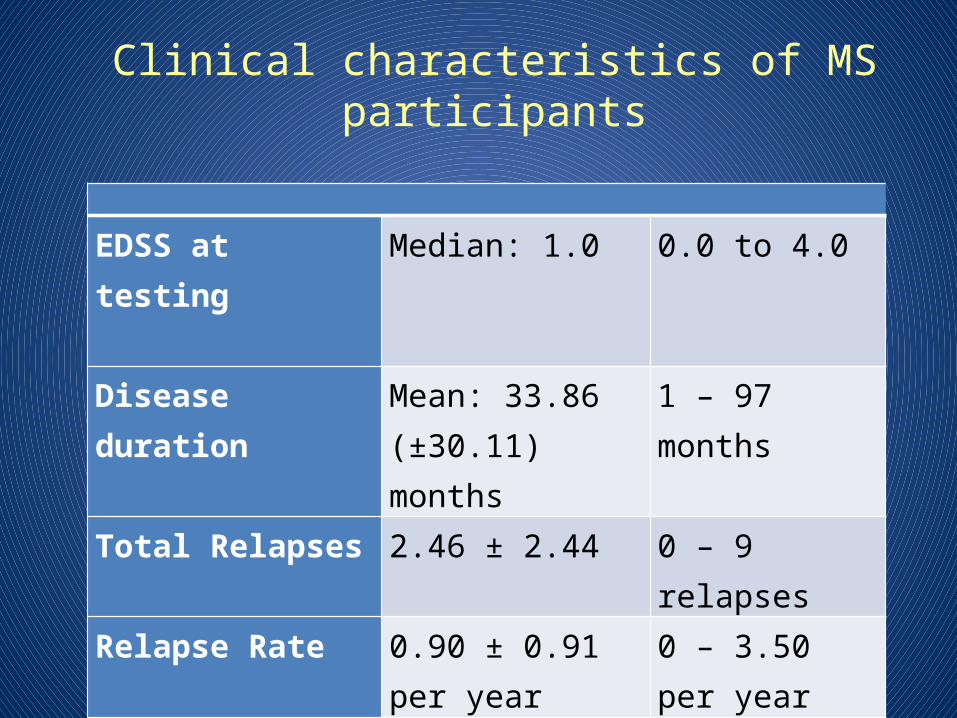
Clinical characteristics of MS participants
EDSS at testing Median: 1.0 0.0 to 4.0
Disease duration Mean: 33.86 (±30.11) months
1 – 97 months
Total Relapses 2.46 ± 2.44 0 – 9 relapsesRelapse Rate 0.90 ± 0.91 per
year0 – 3.50 per year
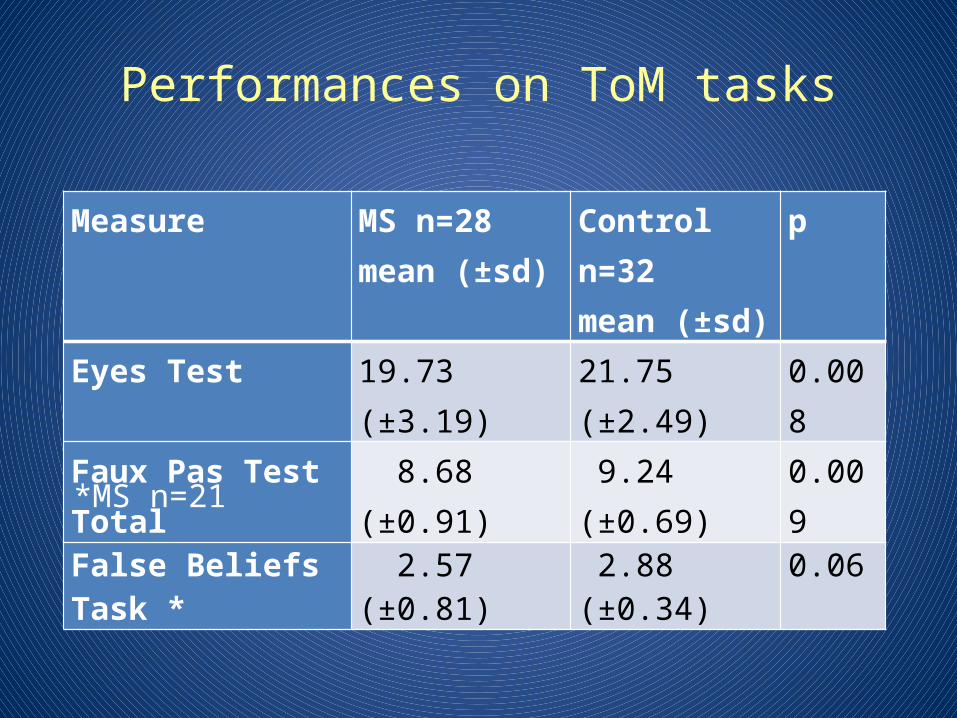
Performances on ToM tasks
Measure MS n=28mean (±sd)
Control n=32mean (±sd)
p
Eyes Test 19.73 (±3.19) 21.75 (±2.49) 0.008
Faux Pas Test Total 8.68 (±0.91) 9.24 (±0.69) 0.009
False Beliefs Task * 2.57 (±0.81) 2.88 (±0.34) 0.06
*MS n=21
Item sub-analyses• Faux Pas Test: –MS participants’ performed lower on the false
beliefs component• Identification of faux pas p=0.19• Story comprehension p=0.25• False beliefs p=0.008
• False Beliefs task:–MS group made more errors for both first and
second order items– Approached significance for more errors on
second order item (p=0.08)

ToM and relation to demographic factors
• MS group more racially diverse with lower maternal educational attainment
• Controlling for these and other factors (age, estimated IQ, gender, or ethnicity) did not alter pattern of results
ToM and relation to MS clinical features
• Total ToM performance – Total number of relapses (r=-0.39, ns)– Disease duration (r=-0.27, ns)– EDSS (r=-0.17, ns)– Relapse rate (r=0.13, ns)
Relation to information processing speed (SDMT)
• SDMT z-scoresMS= - 0.26 (±1.74) vs. HCs= 0.44 (±1.19), p=0.08
• SDMT impairment– 10 (38%) in MS vs. 2 (6%) in HC group
• SDMT with ToM total score, r=0.35, p=0.01• Controlling for SDMT, MS participants’ ToM
performance remained lower than controls (p=0.05)
EQ-SQ Inventory
• MS n=18 vs. HC n=16• Mean EQ: 40.28 ±5.94 vs. 40.69 ±8.51 (ns)• Mean SQ= 23.94 ± 8.29 vs. 23.69 ± 5.77 (ns)• Not related to ToM performance (in either
group)
Summary
• Relative to healthy controls, pediatric-onset MS participants performed worse on study ToM measures– Poorer facial recognition of affective state– Poorer ability to identify beliefs and knowledge of others
• Not explained by demographic factors• Not clearly linked with disease activity • Lower SDMT performance was predictive of ToM, but did not
fully account for the MS group’s deficit• The EQ-SQ inventory did not distinguish the two groups
Limitations
• Cross-sectional pilot study• Only preliminary measures of ToM• Additional measures of cognitive functioning
needed– Executive functioning
• Real-world measures of actual social functioning
Conclusions• ToM deficits may occur in pediatric-onset MS• Consistent with findings in adult MS samples • Deficits are subtle and clinical significance is
unclear• May underlie functional difficulties that would
otherwise go undetected• Youngest may be most vulnerable to long-term
consequences of even subtle deficits








![· Web viewMemory & Cognition, 12, 31-45. [Sereno, 1991] Sereno, J. A. (1991). Graphemic, associative, and syntactic priming effects at a brief stimulus onset asynchrony in lexical](https://img.pdfslide.us/doc/110x75/5b49ab857f8b9a5c278b8c69/-web-viewmemory-cognition-12-31-45-sereno-1991-sereno-j-a-1991.jpg)