Embed Size (px)
DESCRIPTION
By Dr. Raham Bacha From Lecture Notes Of Professor. Dr. S. Amir Gilani.
Citation preview

لنا لما ع قالو ُسبحانك لا
يممتنا انك انت العليُم الحكما علا لا ا Surah Al Baqarah verse 32


By: Dr. Raham BachaMD, MSc Sonology Gold Medalist
(UOL)
PhD Ultrasound
The university of
Lahore

BY

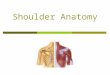
Gleno-humeral joint has the widest
range of movement compared with any
other joint in the body, this is
accomplished through sacrifice of the
bony stability which is seen in most
joints.

The gleno-humeral joint is a multi-
axial ball-and-socket joint. The
bony socket is the glenoid, which is
only about one third of the area of
the humeral head in contrast to the
acetabulum of if hip, which covers
most of the femoral head.


To compensate for the lack of bony
stability there is a closely applied
system of ligaments, tendons and
muscles around the gleno-humeral
joint, which act as dynamic
stabilisers. The most widely known
of these structures is the Rotator
Cuff.

HUMERUS: The hemispherical articular surface isbordered by the anatomical neck of thehumerus and is covered by hyalinecartilage. Greater tuberosity Lies lateral tothe anatomical neck. It has three facets.


1. The superior facet for insertion of the supraspinatus
tendon
2. The middle facet lies postero-inferior to "1". and is the
site of insertion for the infraspinatus tendon.
3. The posterior facet lies posterio-inferinr to "2." the
insertion of the teres minor tendon occurs on it.
Lesser tuberosity- lies anterior to the humeral head.
subscapularis tendon inserts on its apex.
Bicipital grove - Lies between the greater and lesser
tuberosities. Is normally occupied by the long head of
biceps tendm.


Acromion
Broad, flat plate of bone that is continuous with
the spine of the scapula. Lies superior to the
gleno-humeral joint. Articulates withthe clavicle
Projects from the superior aspect of the neck
of the scapula and lies anterior to the gieno-
hurneral joint
Coracoid Process

The Acromium and the Coracoid Process arejoined by the coracoTacromial ligament to
form a continuous protective arch over theshoulder joint. The rotator cuff and the longhead of biceps tendon may becomecompressed between the humeral head and
the coraco-acromial arch - Rotator Cuff
Impingement Syndrome.

Covered with hyaline cartilage. Connected tothe lateral aspect of the scapula by a broadneck. The glenoid labrum is a wedge-shapedfibrocartelagenous structure attached to themargin of the bony glenoid. This increasesthe stability of the gleno-humeral joint andcushions the humeral head.
Glenoid


Attached to the margin of the articular surface of theglenoid, external to the labrum and to the labrum
Humeral attachment: Anatomical neck of the
humerus,
except inferiorly where it attaches more inferiorly to themedial shaft of the humerus. The synovial membrane ofthe glenotumeral joint lines the capsule. The superiormiddle and inferior gleno-humeral ligaments
strengthen the capsule anteriorly. The coraco-
humeral ligament strengthens the capsule
superiorly.
Capsule

There are two breaches in the capsule of the shoulder joint
1. Above the superior gleno-hunieral ligament, for the tendon
of the long head of biceps.
2. Between the superior and middle glano-humeral
ligament's for the communication with the subscapular
bursa, which lies between the capsula and the subscapularis
tendon. This bursa may extend superiorly to lie beneath the
coracoid process to form subcoracoid bursa, however, this
bursa usually does not communicate with the subscapuiaris
bursa or the shoulder joint.
3. Occasionally there is a small defect In the back of the
capsule for a small infraspinatus bursa.



Arises from the subscapular fossa and inserts
on the anterior aspect of the lesser tuberosity
by a broad, thick tendon. Separated from the
coracoid process by the subcoracoid bursa
and the shoulder capsule by the
subscapularis bursa. Fibres from the
subscapularis tendon in combination with
capsular fibers, cross the bicipital grove,
forming the transverse humeral ligament.
Rotator cuffSubscapularis

Arises from the supraspinous fossa
of the scapula. Passes anteriorly and
laterally beneath the coraco-acromial
arch to insert on the superior facet of
the greater tuberosity of the humerus by
a broad, "beak shaped" tendon. The
long head of biceps tendon marks the
anterior margin of the tendon.
Supraspinatus

Arises from the infraspinous fossa of the
scapula. Its tendon blends (mix) with the
supraspinatus tendon and inserts on the
middle facet of the greater tuberosity of the
humerus.
Teres Minor
Arises from the upper two thirds of the
lateral border of the scapula and inserts on
the inferior facet of the greater tuberosity by
a thick flat tendon.
Infraspinatus

The short head arises from the coracoid process.
the long head arises from the supraglenoid tubercle
and the glenoid labrum by a long, round tendon.
The proximal tendon lies within the gleno-humeral
joint as it passes antero-laterally to the bicipital
groove where it passes beneath the transverse
humeral ligament and through the shoulder capsule.
The tendon takes with it, through the capsule. a sheath
of synovium for a variable distance into the bicipital
groove The tendon inserts on the radial tuberosity and
the bicipital aponeurosis.
Biceps Brachii

Arises from the lateral one third of the
clavicle, the lateral border of the
acromion, the spine of the scapula
and the fascia of the infraspinatus
muscle. it is a broad, flat muscle that
converges laterally to insert at the
deltoid tubercle on the lateral shaft of the
humerus.
Deltoid

BursaeThe subacromial-subdeltoid bursa
separates the deltoid from the underlying
rotator cuff, the long head of biceps tendon
and the greater tuberosity. It extends
medially under the acromion and does
not communicate with the gleno-humeral
joint. The subscapularis subcoracoid and
infraspinatus burs have been discussed
earlier.


The muscles of the rotator cuff and the tendon of the
long head or biceps play a crucial role in the stability
of the shoulder joint by acting as antagonists to
muscle groups acting in the Opposite direction. The
antagonistic action of the rotator cuff muscles
maintains the humeral head, centered in the glenoid
through the full range of shoulder movement.

In abduction, the deltoid muscle tends to draw
the humerus superiorly. The supraspinatus muscle
tendon contracts at the beginning of abduction,
thereby resisting the superior movement of
the humeral head. The supraspinatus muscle is
assisted in this function by the long head of
biceps tendon, which also resists the superior
movement of the humeral head.

When there is a loss of balance between the
supraspinatus muscle, the long head of biceps
tendon and the action of the abductors, the
rotator cuff and the adjacent soft tissues
become compressed between the humeral head
and the coracoacromial arch. This is the basis
of rotator cuff impingement in a majority of
cases where no bony cause is found.

1. Abduction
2. Adduction
3. Flexion/Extension
4. Internal rotation
5. External rotation
6. Circurnduction - Which is a
conibinatior) of the above movements
The planes of movement
of the shoulder joint are:

True abduction occurs through a vertical plane,anterior to the coronal plane, in line with the
axis of the scapula.• The deltoid is the main abductor of the arm.
• The supraspinatus is important in the early phases of
abduction and then helps to maintain the joint stability
by restraining this movement.
• The remainder of the rotator cuff muscles help to
maintain the humeral head within the glenoid.
Abduction

The reverse of abduction
Latissimus dorsi, teres major,
subscapularis and the pectoral muscles
combine to effect active adduction.
Adduction

• It Is in a plane at 90 degrees to the plane ofabduction. The biseps brachii, coraco-brachialis, pectoralis major and the anteriorfibres of the deltoid muscle are the main
flexors.• The posterior fibres of the deltoid and the
teres_ major are the main extensors of theshoulder with the latissimus dorsi and thesterno-costal fiberes of the pectoralis majorrestrainig from full flexion.
Flexion/Extension

Internal rotation is effected bysubscapularis, teres major, latissimus dorsi,
pectoralis major and the anterior fibres of the deltoid.
External rotation is effected by infraspinatus,the posterior fibres of the deltoid and the teres minor.
Rotation

This movement is a combination of all theabove movements, with the humerusdescribing a circle or a cone centred on theglenoid.
Movement of the scapula also facilitates thismovement.
Circumduction


The structures successfully
evaluated by ultrasound
include:
• The rotator cuff tendons
• The long head of biceps tendon
• Bursae around the shoulder
• Impingement of the above structures on the
coraco-acromial arch
• The bony structures of the shoulder
• The A-C joint
• The muscles around the shoulder

The advantages of ultrasound include The ability to examine the shoulder as it is
moved through its normal range of movement
Sensitivity and specificities have been reported in
the 90% range
Easy comparison with the opposite side
The ability to palpate and localise sites of pain
and tenderness with the ultrasound transducer
Wide availability
Relatively low cost

The disadvantages of ultrasound include
Highly user dependent
Clinicians find it difficult to interpret images
A number of conditions cannot be evaluated
most labral abnormalities
most bony lesions
capsulitis
A plain film examination should always be
performed in conjunction with the ultiasound. This
will assist in detection of bony lesions and fine
calcifications in the rotator cuff


Tears
Tendonitis
Impingement
Tendon Dislocation

TearsOccur mostly in degenerate or inflamed tendons and
therefor are uncommon in the young. A large amount of force
is required to tear a normal tendon. About 92% of rotator cuff
tears are of the chronic type, most commonly related to
impingement and tendonitis.
Only 8% of tears are acute and due to a single traumatic episode.
50% of patients with rotator cuff tears give no History of
injury. The tear of supraspinatus is common.

Diagnostic:
Absence of the supraspinatus tendon
A gap within the tendon filled with fluid or blood.
A hypoechoic cleft.
Focal thinning of the tendon with loss of the
normal convex contour of the subdeltoid fat plane

Inconclusive But Suggestive Signs:
An echogenic line in the tendon
An inhomogeneous area of echogenicity within the
tendon
Fluid in the subdeltoid burs?
Fluid in the biceps tendon sheath

Tears should be visible in two planes but may be
more obvious in one plane than the other.
Laminar tears. horizontally in the plane along the tendon.Tears are usually more obvious when the tendon is put understress. This is usually achieved by placing the arm in adductionand internal rotation that isachieved by placing the arm behindthe back. If this is not possible then the arm should be placed inextension

TENDONITIS
Mean inflammation of a tendon, it is a type of
tendinopathy. This usually occurs as a result of
a Repetitive micro-trauma due to over use
b Subacromial impingement

SONOGRAPHIC FEATURES OF TENDONITIS
Decrease in echogenicity
Fluid in the tendon sheath or adjacent bursa
Calcification - with acute calcific tendonitis the
calcium is usually liquid and may rupture into the joint
or subdeltoid bursa. With chronic tendonitis – solid
calcification may occur.
Tendonitis will often progress to tendon degeneration
and a tear

Tendonitis will often progress to tendon
degeneration and a tear.
Biceps teildonitis is relatively common and is
usually associated with fluid in the biceps
tendon sheath.
Fluid by itself is non-specific and may be due
to a shoulder joint effusion or rotator cuff
pathology. A small amount of fluid in the biceps
tendon sheath is norrnal.

It refers to compression of the rotator cuff and the
lot u head of biceps tendon between the humeral
head and the coraco-acromial arch.
90% of cases are due to shoulder instability
10% are due to mechanical causes such as
osteophytes on the acromion or A-C joint.
This is the most common cause of chronic
tendonitis and rupture.

Rotator cuff impingement may be divided into
three stages
Stage 1: swelling and hemorrhage
within the supraspinatus tendon
Stage 2: The tendon become thin and
fibrotic
Stage 3: The tendon tears

sonograpic Signs
Direct Signs:
Bunching of the supraspiriatus tendon
against the acromion on abduction
Fluid may be milked laterally in the
sub deltoid bursa with abduction
The humeral head may be forced
inferiorly at the top of abduction

Indirect Signs:
The rotator cuff does not pass freely beneath
the acromion (it is sometimes difficult to
separate guarding of a painful shoulder from
impingement in this situation)
Biceps or supraspinatus tendonitis with no
apparent cause.
Thickening of the subdeltoid bursa with no
apparent causa

The long head of the biceps tendon is heldin the bicipital groove by the transversehumeral ligament. Rupture of this ligamentallows dislocation of the biceps tendon. Itusually dislocates medially, either anterioror posterior to the subscapularis tendon.This is commonly associated withtendonitis and tears of the tendon due tomechanical abrasion of the tendon on thelesser tuberosity.

• An empty bicepital groove (Bewareof incorrect transducer angle)
• The tendon is visualized in adislocated position.
• The tendon may be seen todislocate with external rotation orwith flexion/extension.
• Underlying cortical irregularity
Sonographic Signs:

• Subaciornial-subdeltoid bursa
• Fluid in this bursa is highly suggestive of a
rotator cuff tear.
• It may also be seen in impingement or in
inflammatory arthritides such as rheumatoid
arthritis, which is often associated with
synovial thickening.
• Always check laterally down to the deltoid
tubercal as this bursa is quite extensive.

This may communicate with the shoulder
joint.In these cases fluid will be seen at this site with a joint effusion
Sub-coracoid bursa
This bursa may also communicate with the shoulder jointIsolated fluid may be seen in the subcoracoid bursa with subscapularisimpangment.
Infraspinatus bursa

Ultrasound is sensitive for detection
of fractures in the visible bony surfaces,
especially the greater tuberosity.
Undisplaced fractures of the greater
tuberosity are commonly missed on
plain films.
FRACTURES


The capsule of the A-C joint
normally has a convex superior
surface Abnormal findings include:
Widening of the joint
Fracture fragments
Degenerative change
Ganglion cysts
A-C JOINT


Comparison views of the right and
left AC joints in this patient reveal
separation of the AC joint on the
right side as demonstrated by the
increased distance between the
acromion and the clavicle (curved
arrow).
AC Joint Separation

Hematomas, tears and tumors in the
muscles and soft tissues surrounding the
shoulder joint are usually be visible.
Detection of these abnormalities is assisted
by the ability to examine the exact sate of
swelling or tenderness
PERI-ARTICULAR ABNORMALITIES


Many different techniques for evaluatingthe shoulder by ultrasound have beendescribed. The ideal seems to beexamination of each component of therotator cuff morphologically andfunctionally.

• A high frequency, linear array, small partstransducer with good near field is ESSENTIAL.
• Adjust output (power) to avoid over saturation— remember all structures are superficial.
• Select appropriate 2D grey scale map,persistence, frame rate and line density tooptimise the image.
• Hardcopy images are taken according todepartment protocol, with additional views ofrelevant pathology.
• Useful to record dynamic assessment onVCR.
EQUIPMENT:

TECHNIQUE:
BOTH SIDES ARE EXAMINED, THE
NORMAL FIRST this "sets up the
equipment, the patient, and yourself. A formal
routine is followed to ensure that
no abnormality is overlooked. Each phase
leads onto the next, making it easier
for the novice to maintain their anatomical
bearings.

The routine is, in order
BICEPS
Transverse, longitudinal and dynamic (internal
and external rotation). SUBSCAPULARIS
Longitudinal and dynamic (internal and external
rotation).
CORACO - ACROMIAL LIGAMENT
Longitudinal and dynamic (internal and external
rotation)
SUPRASPINATUS
Transverse, longitudinal and dynamic (passive
and active abduction)

INFRASPINATUS - Longitudinal and dynamic
(internal and external rotation). TERES MINOR -
Longitudinal and dynamic (internal and external
rotation).
ACROMIO - CLAVICULAR JOINT Longitudinal and
dynamic (abduction, adduction and forward flexion).
AREA OF PATIENT'S CONCERN ASK the patient
what movements are difficult or painful, and if they
have any "sore spots". Throughout the examination, if
an area of concern is encountered, reference is made
back to the normal side.

Bony landmarks are particularly
useful in locating the various
tendons. When structures of
uncertain origin are encountered the
rule "when in doubt, move it" is very
useful, provided the sonographer has
a sound knowledge of anatomy.

It is transverse view at the level of the long
head of the biceps tendon at its intra-
capsular level. Note the echogenic tendon
separating the supraspinatus (laterally) and
subscapularis (medially) tendons. This
region is called the rotator cuff interval and
it is important not to confuse this echogenic
focus, often flanked by two hypoechoic
areas, with a rotator cuff abnormality.
The Rotator Cuff Interval


The patient sits facing the monitor, preferably on
an adjustable chair, with their arm by their side,
hand resting on the outer thigh. In this position
the bicipital groove lies anteriorly —(if the hand
lies in the lap, the groove is quite medial, and
can be difficult to located. Placing the
transducer horizontally on the anterior upper
shoulder, the bicipital groove can be seen — this
is a VERY IMPORTANT bony landmark.
BICEPS:

TRANSVERSE — slide the transducer from superior to
inferior in the axial (horizontal) position, from the
acromion to the belly of the biceps muscle, keeping the
transducer perpendicular to the tendon. "Heel and toe"
movements with the transducer may be necessary to show
tendon texture and/or fluid in the groove. The biceps
tendon is usually oval and often lies eccentrically within
the groove. The transverse humeral ligament can be seen
superficial to the tendon as a thin echogenic line and is a
continuation of the fascia overlying the subscapularis
tendon.

Biceps Tendon - Transverse View

Longitudinal - Rotating the transducer
through 90 degrees, the tendon is an
echogenic fibrillar structure lying
anterior to the strongly echogenic
humeral shaft. Again, "hee/ and toe"
movements will compensate for
anisotropy. Examine tendon from
acromion to muscle belly.

Biceps Tendon Long axisDemonstrate the biceps tendon in a sagittal view (white arrow) Note the
Classic fibrillar echo pattern evident within the tendon
also note the transverse humeral ligament in this plane (small white arrow)
Dynamic — The oiclpitai grocyi-e is scanned transversely as the arm is
Inter- sally
ana externally rotated. any subluxation of the tendon should be visible on
the
screen — t is usually obvious to the patient as a palpable and often audible
cli ,k Scanninc the tendon longitudinally with it under tension (patient to
pull
up the - forearm agaulst your pushing) also show movement of the
tendon
fibres

Lonoitudinai — From tne transverse vie■A" of the e biceps. the insertion of tne
subsoapulans tendon can be seen on the medial aspect of the lesser
tuberosity The insertion is the apex of a somewhat triangular tendon. so care
should be taken to observe the whole insertion — it can be 3 to 6 ems wide.
With the arm in external rotation. the whole length of the tendon can be seen
under the subdeltoid bursa
SUBSCAPULARIS

- Short Axis
Figure illustrates a normal subscapularis
tendon (arrows) in a short axis, or transverse
plane. Note the deltoid muscle labeled 0)
superficially, as well as the humeral head
(labeled H) and lesser tuberosity (labeled
LT). Remember, the transducer must be
oriented almost longitudinally in order to
visualize this tendon in a transverse plane
Subscapittaris Tendon

Subscapularis Tendon - Long Axis

Dynamic — Internal and external
rotation of the arm will demonstrate the
passage of the tendon and very broad
muscle belly under the coracoid process.
Bursal fluid may become more evident,
and impingement of the bursa or muscle
on the coracoid can be seen.

At the end of the examination of the subscapularis, the
transducer should be horizontal with the coracoid process and
subscapularis tendon visible. Fix the medial end of the
transducer and rotate the lateral end superiorly, so that a line
drawn through the transducer would pass through the nipple on
the other side of the body. The coraco-acromnial ligament is
visible as a pair of echogenic thin lines with an intervening thin
sonolucent line, running between the coracoid and the
acromion. At the coracoid the ligament appears to pass
superficially but at the acromion the ligament passes deep to
the bone, and is often not well seen. If the patient has had
previous surgery of the shoulder the lateral part of the
ligament may well have been removed.
CORACO - ACROMIAL LIGAMEN

Dynamic - On internal and external iotation tI
ie iotator cuff is seen gliding beneath the
ligament and the deltoid muscle moves
slightly from side to side superficial to it - the
ligament should be assessed for flexibility,
fluid in the subdeltoid bursa quite often being
seen beneath it.

Transverse - the supraspinatus tendon inserts onto the greater
tuberosity and forms the superior and lateral portions of the
cuff: normally it is covered by the bony acromion, so has to
be put Linder tension to observe it in its entirety, this
involves moving the arm into various positions. The easiest
position is to flex the elbow, place the palm of the hand onto
the hip, and tuck the elbow into the side or extend the arm
down by the side and turn the thumb inward: or place the
arm behind the back, making sure there is no "gap" between
the elbow and the torso this can be quite difficult for elderly
patients. A combination of .these three manoeuvres can be
attempted.
SUPRASPINATUS

The transducer is placed on the acromion in the
coronal plane, and slid laterally the acoustic shadow
of the acromion is replaced by a pair of parallel
curved echogenic lines The anterior line is the
subdeltoid bursa and the posterior, the humeral head.
Articular cartilage is seen as a thin hypoechoic line
anterior to the humeral head. Move the transducer in
this plane anteriorly until the biceps tendon is seen as
an oval echogenic structure - THIS IS A VERY
IMPORTANT LANDMARK - as the supraspinatus
tendon immediately

posterior to it is known as the critical zone of the tendon,
ie., it is more prone to degenerative change because of
poor vascularity. Moving the transducer posteriorly will
delineate the junction of the supraspinatus and
infraspinatus, seen as an oblique echogenic line, near the
posterior edge of the acromion. Scan the tendon down onto
its insertion onto the humeral head, noting any pitting or
bony changes on the humeral head. possibly indicative of
tears. Continue scanning in the same plane onto the
humeral head, to rule out fluid in the subdeltoid bursa
beyond the tendon insertion -• care should be taken to scan
very lightly, as fluid can be very easily dispersed.

Lorigi_tudinal - Rotate the transducer through 90 degrees, and use
the acromion as a landmark.
The anterior part of the supraspinatus lies anterior to the acromion.
The tendon has a sickle shape Often the coraco-acromial ligament is
seen in cross-section immediately superficial to the tendon The
ligament is iistrally an echogenic dot. often with a sonolucent
centre. Sliding the transducer slightly anterior to the supraspinatus
the tendon of long head of biceps is again encountered.
The mid portion of the tendon has an "eagles beak" appearance. 1 he
acoustic shadow of the acromion resembles the head of the eagle,
the smooth convex upper border of the tendon is the top of the beak,
and the top of the humeral head is the bottom of the beak The hook
of the beak is the greater tuberosity.

Sliding the transducer slightly niore
posteriorly, the hook of the greater
tuberosity is lost and the beak has a
flatter appearance, resembling more a
"crow's beak".

Supraspinatus Tendon - Long Axis

Supraspinatus Tendon - Short Axis

Dynamic --- With the transducer parallel to the
longitudinal plane of the supraspinatus tendon,
abduct the patient's arm whilst watching the
tendon movement on the screen. The tendon
and subdeltoid bursa should slide completely
under the acromion or coraco-acrornial
ligament. The movement should be performed
by the patient (active) and by the sonographer
(passive) with the arm in different degrees of
internal and external rotation.

The dynamic procedure should be performed so that the
anterior and mid (and occasionally posterior) portions of
the tendon are examined as pathology can occur in any
region with any movement, depending on the clinical
situation eg in some occupations, where many movements
are performed with the arms over thehead, the posterior
tendon suffers more than the anterior, and vice versa. It
should be noted that when thc, arm is in marked internal
rotation, there is a natural limit to the amount of abduction
that can occur (approximately 90 degrees)

Longitudinal — With the patient's arm in
internal rotation, place the transducer on the
spine of the scapula, aligned to its
longitudinal axis. Slide inferiorly and
laterally to demonstrate the infraspinatus
tendon insertion onto the greater tuberosity.
Then move back medially to the
musculotendinous junction.
INFRASPINATUS

Infraspinatus Tendon - Short Axis

Infraspinatus Tendon Tendon - Long Axis

Dynamic — Moving the arm
through external and internal
rotation demonstrates
the tendon moving over the
humeral head. Deeper to the
tendon the posterior

glenoid labrum can be seen as a thin echogenic
triangular structure "leaning“ on the humeral head.
Effusions in the gleno-humeral joint are easily
identified in this position as sonolucent collections
adjacent to the glenoid labrum. These collections
change shape with the movement of the humerus.

Longitudinal - From the infraspinatus position, slide the
transducer inferiorly, approximately 1 cm. The thicker
Teres tendon resembles a ship's prow. becoming more
elongated as the arm is internally rotated. The tendon
itself is more oblique than infraspinatus — to view
longitudinally, rotate the medial end /, of the transducer
slightly inferiorly.
TERES MINOR

Dynamic -- Again, on internal and
external rotation, the tendon
assessed, as can be any fluid
collections in the posterior joint
space.

his is usually easily palpable. If not, in the
longitudinal supraspinatus position, slide the
transducer slightly antero--medially across the
acromion and the joint should become obvious as a
sonolucent inverted triangle between the acoustic
shadows of the acromion and the clavicle ("The fat
seagull sign"). Scan from anterior to posterior.
ACROMIO-CLAVICULAR JOINT

Dynamic — Frorn tlie resting position
(arm extended down by the patient's side),
abduct and adduct the arm, observing any
change in the shape of the joint capsule.
Also observe any movements of the bones
themselves -- especially in the forward
flexion position.

• This is the BASIC examination: other areas of concern
include-
• the suprascapular notch and spino-glenoid notch
(affecting the
• suprascapular nerve),
• the short head of biceps,
• muscle texture in disuse syndromes (especially infra- and
supraspinatus)
• rhomboids,
• deltoid origin and insertion
• pectoralis muscles
• triceps