Embed Size (px)
Citation preview

SEMEN ANALYSIS – REVISITED
Dr. Shah Dupesh MBBS, DCE, FASM, (PhD)
The guy who takes care of the MEN in the WOMENS CENTER ;-)
SEMEN ANALYSIS: A BIT OF HISTORY
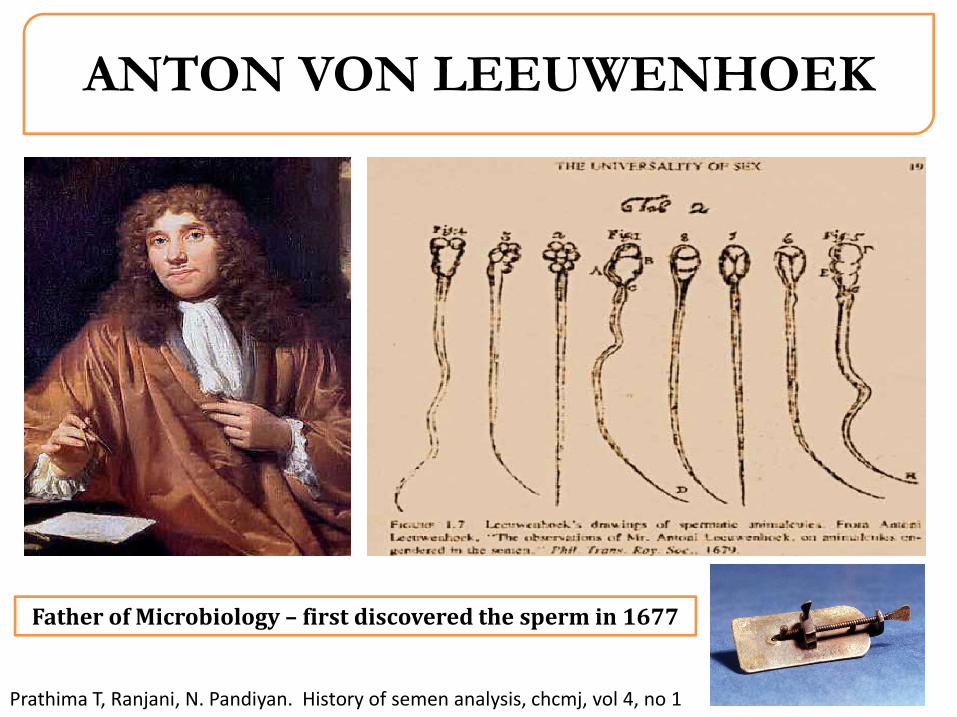
ANTON VON LEEUWENHOEK
Prathima T, Ranjani, N. Pandiyan. History of semen analysis, chcmj, vol 4, no 1
Father of Microbiology – first discovered the sperm in 1677
SEMEN ANALYSIS – BIG DEAL?
6-7 years ago concerns were raised about the standard of care of men with infertility
Changes in semen analysis among infertile men are usually non specific and frequently give very little information about the cause of infertility. non specific and frequently give very little information about the cause of infertility.
At a UG Level doctors also receive little training pertinent to this specialty. So how effectively are we managing the couple?
The prevalence of male factor infertility is 7% of all men*. This incidence is higher than Diabetes Mellitus
Jecquir and Cummins, 1997. Tournaye, 1997. *Nieschlag and Behre 2000

SEMEN ANALYSIS
Overview
Remains the gold standard test of choice when assessing test of choice when assessing infertility in a couple.
Ultimately decides the course of treatment for a couple
Gives an idea about a mans testicular germ cell output
Influenced by numerous factors.
SEMEN ANALYSIS – LIMITATION?
Several!!
Collection artifact
Analysis artifact
Interpretation artifact
What is Normal? remains controversial
Male fertility cannot be determined based on single report or solely on these results.
Depends on Man-laboratory-Physician unit.
ARTEFACTS IN SEMEN ANALYSIS
Collection Artefacts
Interpretation Artefacts
Analysis Artefacts
COLLECTION ARTEFACTS?
Again Several!!
Difficulty in semen Difficulty in semen collection.
Agony of Split ejaculate.
Incomplete sample.
Improper container.
Inconvenient space.
COMMERCIAL DIAGNOSTIC LABORATORIES DO NOT CARE!

Collection Artifacts? The hard truth
Environment if not conducive for arousal
Can affect a man’s erectile function
Can affect mans ability to give a complete
sample
Treatment strategies drastically change
ANALYSIS ARTEFACTS?
Over 95% of standalone commercial laboratories have still not upgraded to the latest WHO 2010 guideline values
This means men suffering from a genuine problem may be missedmissed
Our data of over 300 samples(unpublished), clearly shows that there is at least a 30% to 40% variance in sperm parameters of conc, motility and morphology between a good laboratory following WHO guidelines vs. those that don’t. Scary!!!!
INTERPRETATION ARTEFACTS?
Interpreting a requires ahigh degree of clinicalskill and past experience
15mill/ml sample with 2ml volume =
30million/ejaculate
6mill/ml sample with 5ml volume =
30million/ejaculate
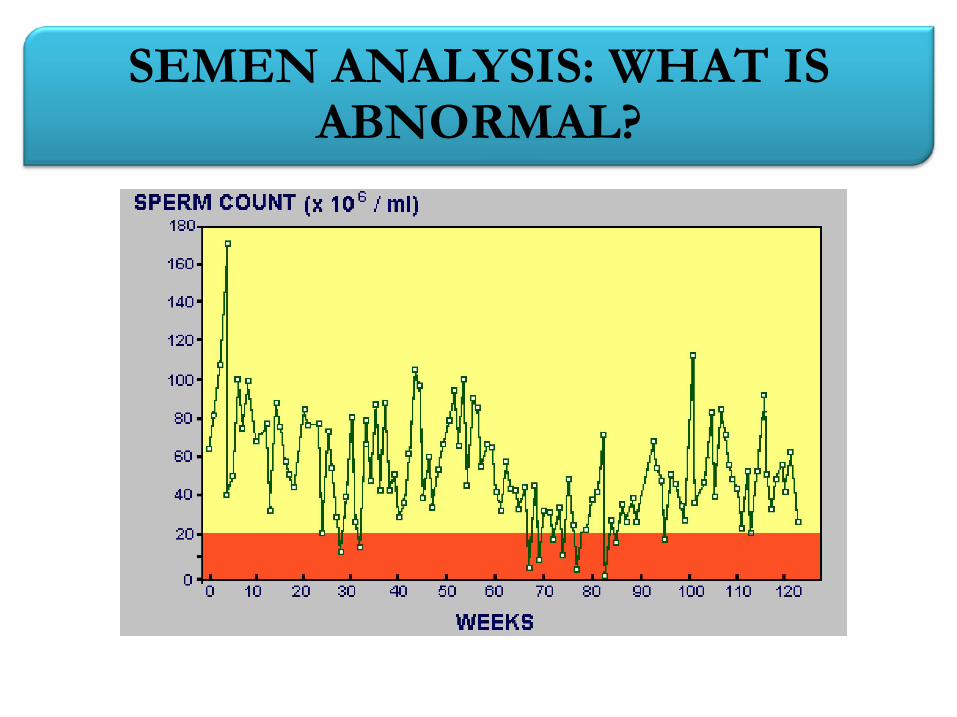
SEMEN ANALYSIS: WHAT IS ABNORMAL?
Although the clinical value of the analysis of human semen has previously been
questioned, it has lately regained its position as the cornerstone of the male
infertility work-up
(Chong et al, 1983, McDonough P, 1997)
SEMEN ANALYSIS: WHAT IS NORMAL?
Semen is the most heterogeneous of biological fluids wherein parameters
concerning the motility, concentration and morphology varies between regions,
countries, individuals and between two samples in the same individual
(Cooper et al, 2009)
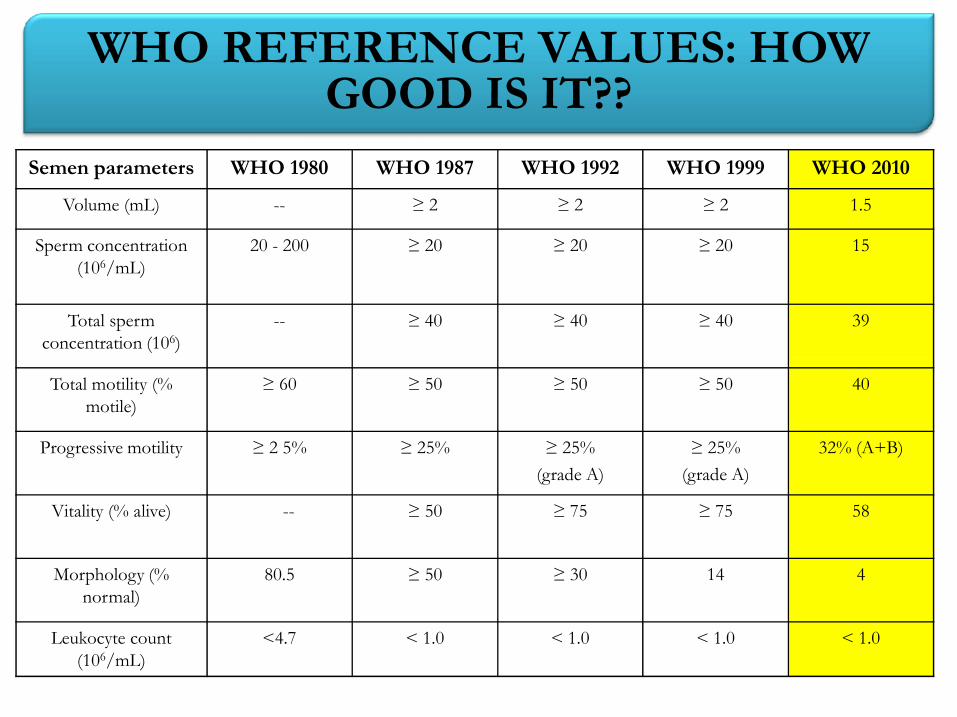
Semen parameters WHO 1980 WHO 1987 WHO 1992 WHO 1999 WHO 2010
Volume (mL) -- ≥ 2 ≥ 2 ≥ 2 1.5
Sperm concentration (106/mL)
20 - 200 ≥ 20 ≥ 20 ≥ 20 15
Total sperm concentration (106)
-- ≥ 40 ≥ 40 ≥ 40 39
WHO REFERENCE VALUES: HOW GOOD IS IT??
Total motility (% motile)
≥ 60 ≥ 50 ≥ 50 ≥ 50 40
Progressive motility ≥ 2 5% ≥ 25% ≥ 25%
(grade A)
≥ 25%
(grade A)
32% (A+B)
Vitality (% alive) -- ≥ 50 ≥ 75 ≥ 75 58
Morphology (% normal)
80.5 ≥ 50 ≥ 30 14 4
Leukocyte count (106/mL)
<4.7 < 1.0 < 1.0 < 1.0 < 1.0
WHO REFERENCE VALUES: HOW GOOD IS IT??
A significant overlap of parameters of sperm concentration, motility andmorphology has been reported between fertile and infertile male populations
(Gao et al, 2008)
There is a little consensus as to which of the parameters within a conventional
“Semen analysis remains a numbers game”
There is a little consensus as to which of the parameters within a conventionalsemen analysis is the BEST POOR PREDICTOR of pregnancy
(Jecquir, 2005 & 2006)
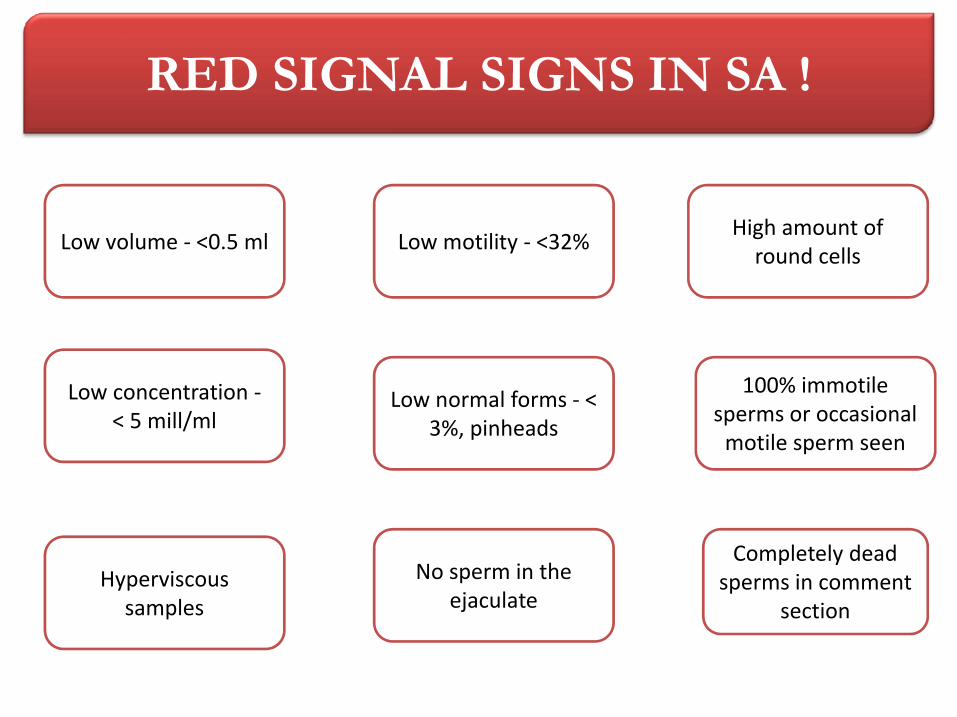
RED SIGNAL SIGNS IN SA !
Low volume - <0.5 ml Low motility - <32% High amount of
round cells
Low concentration -< 5 mill/ml
No sperm in the ejaculate
Low normal forms - < 3%, pinheads
100% immotile sperms or occasional
motile sperm seen
Hyperviscoussamples
Completely dead sperms in comment
section
Despite limitations, remains the
most important test.
No count below which pregnancy
is not possible- except
SEMEN ANALYSIS: THE CORNERSTONE TEST IN FERTILITY EVALUATION
500 million guys to one girl…hmm I
have better chances at winning a lottery
Azoospermia.
No count above which pregnancy
is certainly possible.
Men with Azoospermia, Total
asthenozoospermia or Total
Necrozoospermia are infertile
INTO THE FUTURE…..
SCSA
What are Normal or Reference values?
Which of the three is important?
Would semen analysis become binary reporting soon?
DNA fragmentation test of spermatozoa prior to IUI may be able to predict IUI success, we have seen good results as far ICSI is concerned
GENTLEMEN AND LADIES. THANK YOU!!!!





























