Embed Size (px)
DESCRIPTION
Citation preview

Bariatric/ metabolic surgery-Bariatric/ metabolic surgery-What should patients know?What should patients know?
Torsten Olbers MD, PhDTorsten Olbers MD, PhD

Why lose weight?Why lose weight?
Improve health- Improve health- live healthier and longerlive healthier and longer
Quality of lifeQuality of life- - ability to live a normal lifeability to live a normal life

What do we want to achieve?
Lower body weightLower body weight Not per seNot per se
Improved QoLImproved QoL YesYes
Reduced morbidityReduced morbidity Yes!Yes!
Cost effective treatmentCost effective treatment Yes!Yes!
Prevent premature deathPrevent premature death YES! YES!

Not medicine Not medicine OROR surgery, surgery,
rather rather
medicine medicine ANDAND surgery surgery

An important question..An important question..
Do we suggest surgery,Do we suggest surgery,
or is it the patient driving..?or is it the patient driving..?

Who can be a surgical candidate?Who can be a surgical candidate?
BMI >35 kg/m² (BMI >30)BMI >35 kg/m² (BMI >30) > 18 y> 18 y Previous failure on conventional attemptsPrevious failure on conventional attempts No unstable psychiatric diseaseNo unstable psychiatric disease No current addiction (alcohol, pills, drugsNo current addiction (alcohol, pills, drugs))

Type of operationsType of operations
Gastric bandGastric band
Gastric Bypass Gastric Bypass
Sleeve gastrectomySleeve gastrectomy

Laparoscopic gastric bypassOlbers, Lönroth et al, Obesity Surgery 2003


How does it work?How does it work? Less hungerLess hunger Faster fullnessFaster fullness Changes in food preferenceChanges in food preference Altering energy expenditureAltering energy expenditure
Altering in signals regulating food intake and energy expenditure

Gastric bypass vs. Gastric bypass vs. SleeveSleeve
Gastric bypassGastric bypass ””Gold standard”Gold standard” Since 70iesSince 70ies Long term results- Long term results- 20y20y
All ”spare parts” All ”spare parts” left in situleft in situ
Cures reflux Cures reflux diseasedisease
Some more need for Some more need for supplementssupplements
SleeveSleeve Newcomer (5-10 y)Newcomer (5-10 y) No involvement of No involvement of small bowelsmall bowel
As ”major” surgeryAs ”major” surgery ””Spare parts” Spare parts” resectedresected
Reflux, vomitingReflux, vomiting

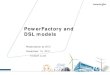
What to expect in weight loss?What to expect in weight loss?
Short term 33%, long term 25-30% weight lossShort term 33%, long term 25-30% weight loss
Loss of half to all of overweight over one yearLoss of half to all of overweight over one year
>90% have a good long term effect>90% have a good long term effect

Sjöström et al NEJM -07
SOS- Swedish Obese Subjects study

Sleep apnae Sleep apnae AsthmaAsthma
NASH, NAFLDNASH, NAFLDCardio-vascularCardio-vascular Type 2 diabetes Hyperlipidemia Hypertension
InfertilityInfertilityPCOSPCOS
Osthoarthritis, Osthoarthritis, pain, mobilitypain, mobility
GallstoneGallstone
CancerCancer
What about health?StrokeStroke
Psoriasis, RAPsoriasis, RA

Could you never eat ”normally” again?Could you never eat ”normally” again? Can be tough in the beginning (weeks-months)Can be tough in the beginning (weeks-months) Changes in sensations around foodChanges in sensations around food Not always liking same type of foodsNot always liking same type of foods You should be able to eat everything– You should be able to eat everything– in smaller amountsin smaller amounts

Diet before and after surgeryDiet before and after surgery
Low calorie diet some weeks before surgeryLow calorie diet some weeks before surgery Gradually increase in texture over first monthGradually increase in texture over first month

Portion sizePortion size
Varies!Varies!
After some months- small normal portionAfter some months- small normal portion

Eating after gastric bypassEating after gastric bypass Chew properlyChew properly Regular mealsRegular meals Keep the pace slowKeep the pace slow Planning!Planning! Don’t drink when eatingDon’t drink when eating Eat on a small plateEat on a small plate

It is not normal with vomiting or It is not normal with vomiting or abdominal pain after gastric bypass!abdominal pain after gastric bypass!
If early: If early: suspect complicationsuspect complication
If late: If late: suspect internal herniationsuspect internal herniation

SupplementationSupplementation
• • Less food intake initiallyLess food intake initially• • Impaired uptakeImpaired uptake
Vitamin BVitamin B1212
Calcium + Vitamin DCalcium + Vitamin D Multi vitamin- and Multi vitamin- and
mineral tabletmineral tablet Iron to fertile womenIron to fertile women

Healthy choices!Healthy choices!
VariationVariation Prioritize proteinPrioritize protein A lot of fruit and vegetablesA lot of fruit and vegetables Full corn breadFull corn bread Fast food less appealingFast food less appealing

DumpingDumping
Food enters directly to the intestineFood enters directly to the intestine Not harmful, just very unpleasant!Not harmful, just very unpleasant! Tiredness/weakness, nausea, palpitation, Tiredness/weakness, nausea, palpitation,
cold sweatingcold sweating Disappears within 15-30 minDisappears within 15-30 min
– Sweet and fat foodsSweet and fat foods– Too large amountToo large amount– Too fastToo fast

Normal courseNormal course
Early mobilisationEarly mobilisation Start drinking- often and littleStart drinking- often and little First 24 h can be toughFirst 24 h can be tough 1-2 days in hospital1-2 days in hospital 3 weeks sick leave3 weeks sick leave Physical activity allowed, almost no restrictionPhysical activity allowed, almost no restriction

What can go wrong?What can go wrong?• Complication 1/20Complication 1/20
1-2/100 serious (possibly reoperation)1-2/100 serious (possibly reoperation) HaemorrhageHaemorrhage LeakageLeakage Pulmonary embolismPulmonary embolism
• Complications usually early after surgeryComplications usually early after surgery• What is the risk of dying? 0,5/ 1000What is the risk of dying? 0,5/ 1000

Late complaintsLate complaints Feeling cold and tiredFeeling cold and tired Modest hair loss after some 3-6 monthsModest hair loss after some 3-6 months Risk for vitamin/mineral deficienciesRisk for vitamin/mineral deficiencies Excessive skinExcessive skin ””Hypoglycaemia”Hypoglycaemia” AlcoholAlcohol Abdominal painAbdominal pain


Treatment of reactive hypoglycaemiaTreatment of reactive hypoglycaemia
Patti ME. Diabetologia 2005; 48: 2236-2240 Goldfine AB. J Clin Endocrinol Metab 2007; 92: 4678-4685 Kellogg TA. Surg Obes Relat Dis 2008; 4: 492-499Tack J. Nat Rev Gastroenterol Hepatol. 2009;6: 583-90

Bariatric/ metabolic surgeryBariatric/ metabolic surgery
Do the patient need help with signals?Do the patient need help with signals? Reasonable expectationsReasonable expectations Be aware about risk of complicationsBe aware about risk of complications Weight loss does not resolve all problems..Weight loss does not resolve all problems..

Follow upFollow up
2 months2 months
6 months6 months
12 months12 months
24 months24 months
Thereafter yearly assessments and bloodsThereafter yearly assessments and bloods
Availability for extra visits!Availability for extra visits!

Metabolic surgery-Metabolic surgery-
a novel indication?.. a novel indication?..

Bariatric surgery reduces CV eventsBariatric surgery reduces CV events
Sjöström et al JAMA 2012

...but only fasting insulin predict benefit (not BMI)...but only fasting insulin predict benefit (not BMI)

Bariatric surgery reverses end Bariatric surgery reverses end organ damage organ damage Mingrone et al Diabetes Care 2011Mingrone et al Diabetes Care 2011


Effects of Gastric Bypass Surgery in Patients With Type 2 Diabetes and Only Mild Obesity
Ricardo V. Cohen, M.D., Jose C. Pinheiro, M.D., Carlos A. Schiavon, M.D., João E. Salles, M.D., Bernardo L. Wajchenberg, M.D., David E. Cummings,
M.D.
Diabetes Care Volume 35: 1420-1428
July, 2012


Roux-en-Y Gastric Bypass vs Intensive Medical Roux-en-Y Gastric Bypass vs Intensive Medical Management for the Control of Type 2 Diabetes, Management for the Control of Type 2 Diabetes, Hypertension, and Hyperlipidemia: The Diabetes Hypertension, and Hyperlipidemia: The Diabetes
Surgery Study Randomized Clinical TrialSurgery Study Randomized Clinical TrialIkramuddin et al, JAMA 2013Ikramuddin et al, JAMA 2013

EOSSEOSS

The IDF Position Statement on The IDF Position Statement on Bariatric Surgery in obese type 2 Bariatric Surgery in obese type 2
diabetes 2011diabetes 2011
Bariatric Surgical and Procedural Interventions in the Bariatric Surgical and Procedural Interventions in the Treatment of Obese Patients with Type 2 DiabetesTreatment of Obese Patients with Type 2 Diabetes

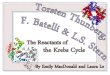
Management Algorithm for Metabolic Management Algorithm for Metabolic Control in Type 2 DiabetesControl in Type 2 Diabetes
Basal Premixed
Basal Bolus insulin
Sulphonylurea
Acarbose DPP-4 inhibitor/ GLP-1 analogues
Glitazone Insulin
Lifestyle Modification•diet modification•weight control•physical activity
Metformin
Bariatric Surgery
BMI > 30 eligible & BMI > 35 prioritized
*If HbA1c >7.5% despite optimized conventional therapy, especially if weight is increasing, or if other weight responsive comorbidities are not reaching target on conventional therapy.
Bariatric SurgeryBMI > 35 eligible BMI > 40 prioritised
Bariatric Surgical and Procedural Interventions in the Bariatric Surgical and Procedural Interventions in the Treatment of Obese Patients with Type 2 DiabetesTreatment of Obese Patients with Type 2 Diabetes

Metabolic surgeryMetabolic surgery- Reconstructions of the GI tract can resolve:Reconstructions of the GI tract can resolve:
- Type 2 diabetes mellitusType 2 diabetes mellitus- Sleep apnoeaSleep apnoea- HyperlipidemiaHyperlipidemia- HypertensionHypertension- NASH/NAFLDNASH/NAFLD- Renal impairmentRenal impairment- AsthmaAsthma- PsoriasisPsoriasis- EtcEtc
Which patients benefit most?Which patients benefit most?

ConclusionConclusion Currently strongest evidence for benefits in Currently strongest evidence for benefits in
patients having a BMI>35patients having a BMI>35
No problem justifying surgery for metabolically No problem justifying surgery for metabolically impaired patients having a BMI<35impaired patients having a BMI<35
Need of hard endpoint studies: RCTs for T2D- Need of hard endpoint studies: RCTs for T2D- best medical vs. best medical+ surgerybest medical vs. best medical+ surgery
Surgery should be regarded as add on therapySurgery should be regarded as add on therapy

Future
• Metabolic surgery
• Diabetic surgery
• Tailored surgery/medication- phenotypes
• Studies of the mechanism of action

An important question..An important question..
Do we suggest surgery, or do Do we suggest surgery, or do patients need to claim right to patients need to claim right to
treatment?....treatment?....

AcknowledgementsAcknowledgements
UCD- DublinUCD- Dublin– Carel le RouxCarel le Roux
Imperial College LondonImperial College London– Alex MirasAlex Miras– Dimitris PournarasDimitris Pournaras– Sam SchoultzSam Schoultz
Sahlgrenska AcademySahlgrenska Academy– Hans LönrothHans Lönroth– Lars SjöströmLars Sjöström– Lars FändriksLars Fändriks– Marlin WerlingMarlin Werling– Anna LaureniusAnna Laurenius
University Hospital OsloUniversity Hospital Oslo– Torgeir SövikTorgeir Sövik– Eerlend AasheimEerlend Aasheim– Tom MalaTom Mala
University of ZurichUniversity of Zurich– Thomas LutzThomas Lutz– Marco BueterMarco Bueter

””Metabolic surgeryMetabolic surgery””
Duodeno-jejunal bypass
Ileal transposition Endoluminal sleeve