Embed Size (px)
Citation preview


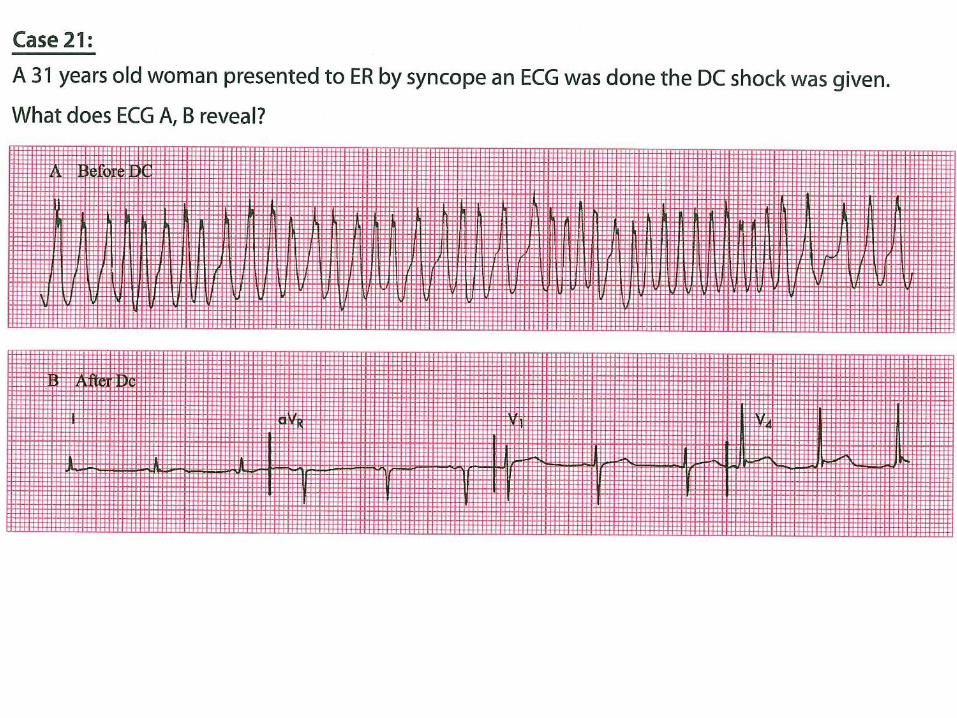
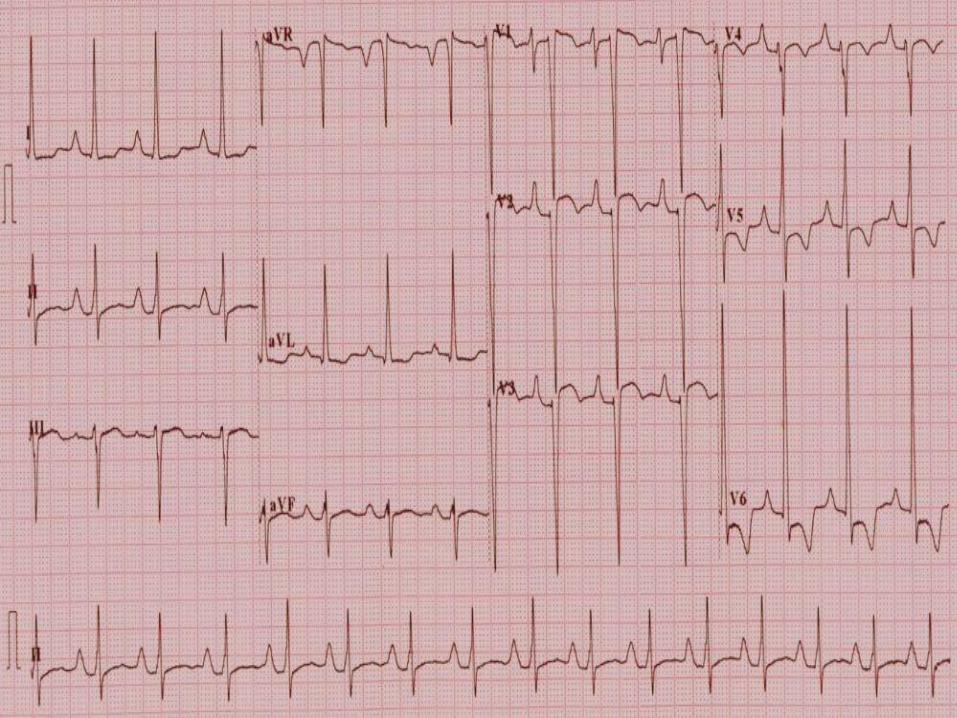
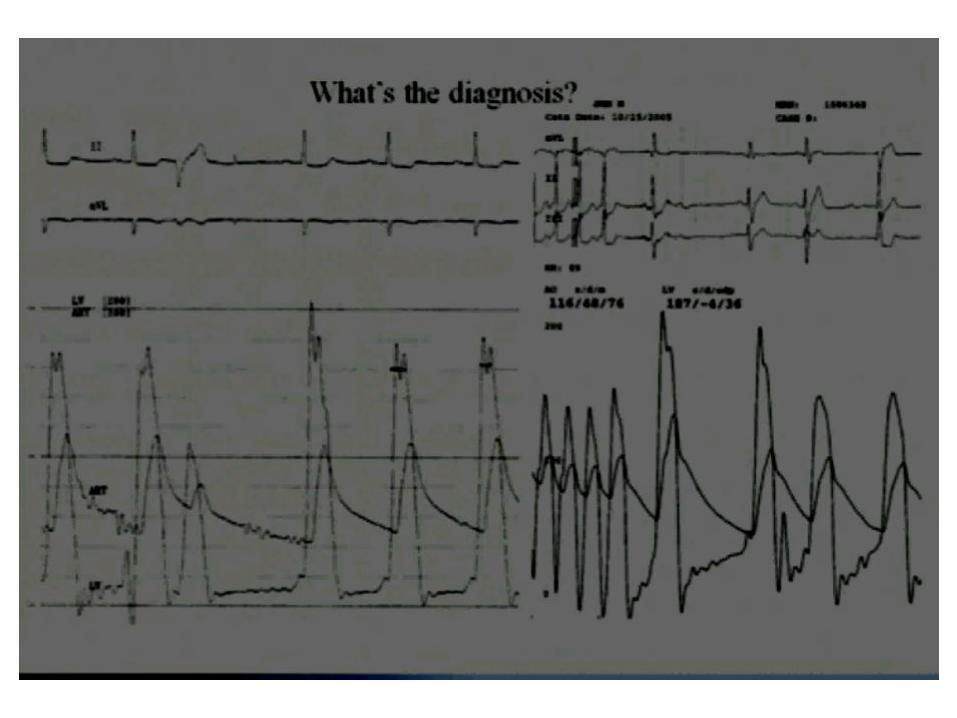

•1-Right bundle branch block with left axis means left anterior hemiblock = bifascicular block. T wave inversion in V1 to V3 could be due to right bundle branch block or previous anterior wall myocardial infarction •2-Brugada Syndrome Type 2 •3-The very rapid atrial fibrillation denote accessory pathway. The wide QRS is due to aberrant conduction (antegrade conduction in the accessory pathway). When sinus rhythm was restored, very short PR proves Wolff Parkinson White syndrome. •4-P pulmonale denotes large right atrium but instead of right ventricular hypertrophy there is left ventricular hypertrophy. This is ECG of tricuspid atresia. The raised ST in V1,2,3 is reciprocal change to the severe ST depression in V5,6. Sorry it is not easy ECG. •5-There is pressure gradient between LV and aorta that reached 71 mmHg. This is aortic valve stenosis and should not be difficult to diagnose. If there is subaortic membrane there will be two levels of pressure gradient during pull-back. Also in HOCM may show two levels. During the arrhythmia BP dropped but gradient increased after it (post extrasystolic potentiation). •6-Atrial flutter, note two P waves or A waves for every one QRS. The direction of conduction is anti-clock wise (counterclock wise) so it is Typical type of Atrial flutter.