Embed Size (px)
Citation preview
Manifestation of
coronary artery diseases
in Multi-Slice CT
Coronary angiography
Dr/AHMED ESAWY
Dr. Ahmed Esawy
MBBS M.Sc. MD
Dr/AHMED ESAWY
Manifestation of CAD
• CORONARY PLAQUE
• CORONARY ARTERY CALCIFICATION
• CORONARY ARTERY STENOSIS
• POSTOPERATIVE EVALUATION OF
CORONARY ARTERY
• ANOMALOUS CORONARY ARTERIES
• Non-atherosclerotic coronary abnormalities
1/ M. Kawasaki 2/ Myocardial bridging 3/ External compression 4/ Coronary dissection
Dr/AHMED ESAWY
CORONARY
PLAQUE
Dr/AHMED ESAWY
Atherosclerosis
• it was defined as slight to moderate wall change, without substantial narrowing of the vessel.
• Most acute coronary syndromes are initiated by sudden disruption of atherosclerotic plaques that are not causing significant stenosis.
• Those non stenotic plaques are associated with high lipid content.
• Calcium content, on the other hand, has been associated with plaque stability.
Dr/AHMED ESAWY
Atherosclerosis
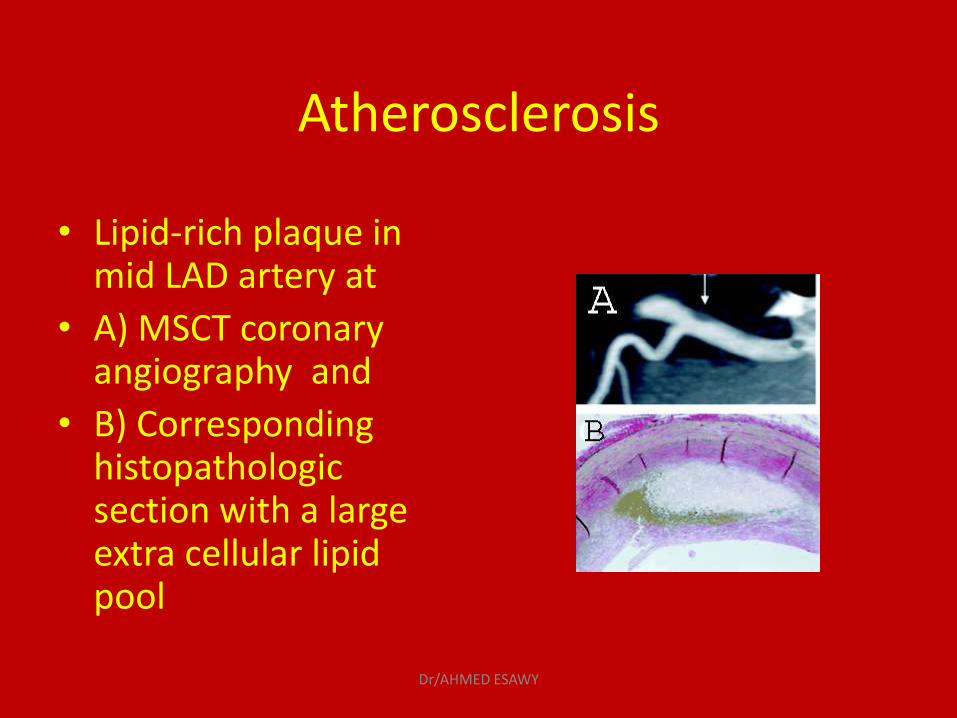
• Lipid-rich plaque in mid LAD artery at
• A) MSCT coronary angiography and
• B) Corresponding histopathologic section with a large extra cellular lipid pool
Dr/AHMED ESAWY
Vulnerable Plaque
Increased risk for erosion or rupture
Associated with acute coronary ischemic events
Dr/AHMED ESAWY
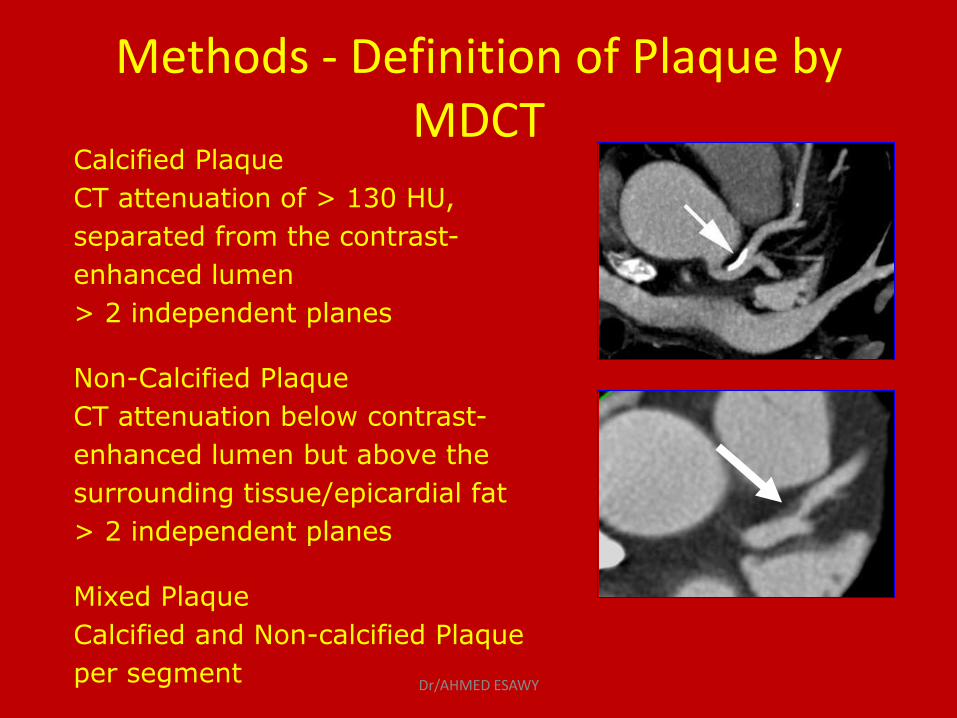
Calcified Plaque
CT attenuation of > 130 HU,
separated from the contrast-
enhanced lumen
> 2 independent planes
Non-Calcified Plaque
CT attenuation below contrast-
enhanced lumen but above the
surrounding tissue/epicardial fat
> 2 independent planes
Mixed Plaque
Calcified and Non-calcified Plaque
per segment
Methods - Definition of Plaque by MDCT
Dr/AHMED ESAWY
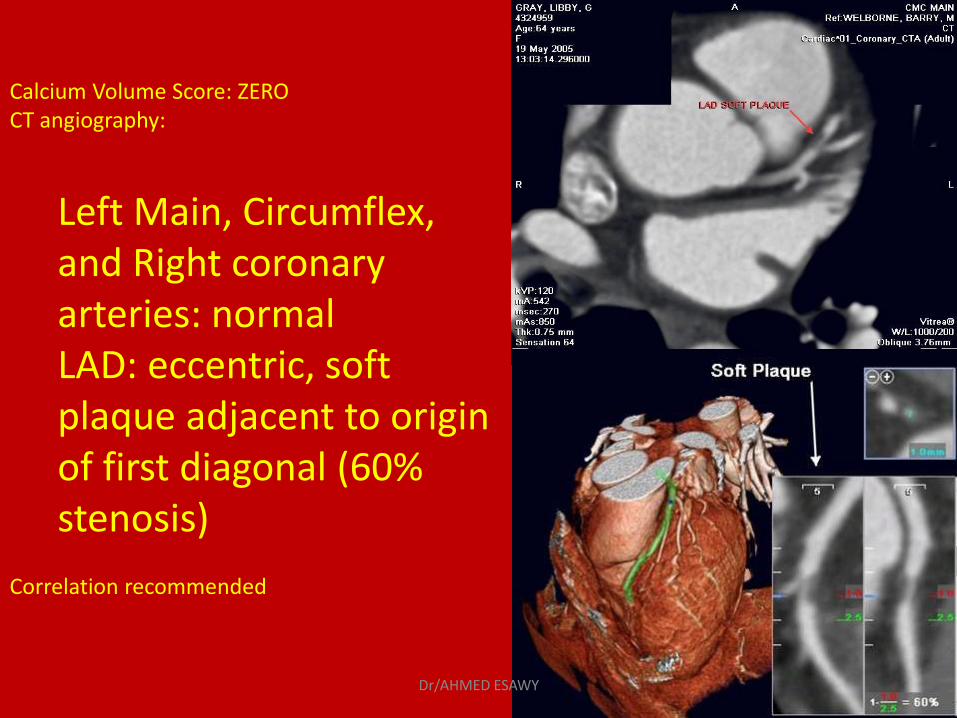
Calcium Volume Score: ZERO CT angiography:
Left Main, Circumflex, and Right coronary arteries: normal LAD: eccentric, soft plaque adjacent to origin of first diagonal (60% stenosis)
Correlation recommended
Dr/AHMED ESAWY
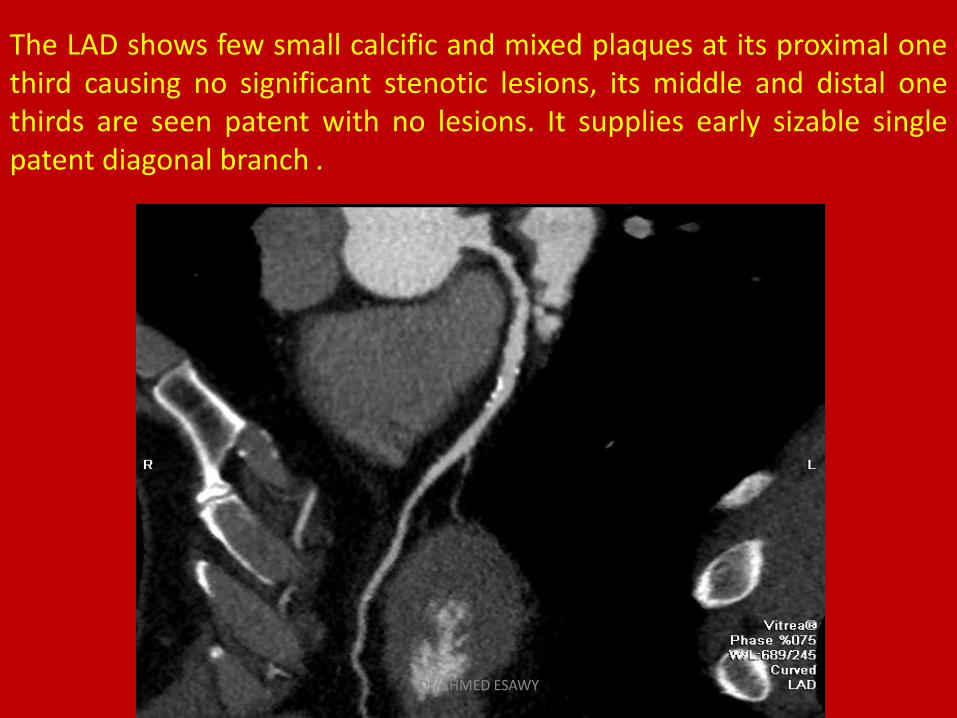
The LAD shows few small calcific and mixed plaques at its proximal one third causing no significant stenotic lesions, its middle and distal one thirds are seen patent with no lesions. It supplies early sizable single patent diagonal branch .
Dr/AHMED ESAWY
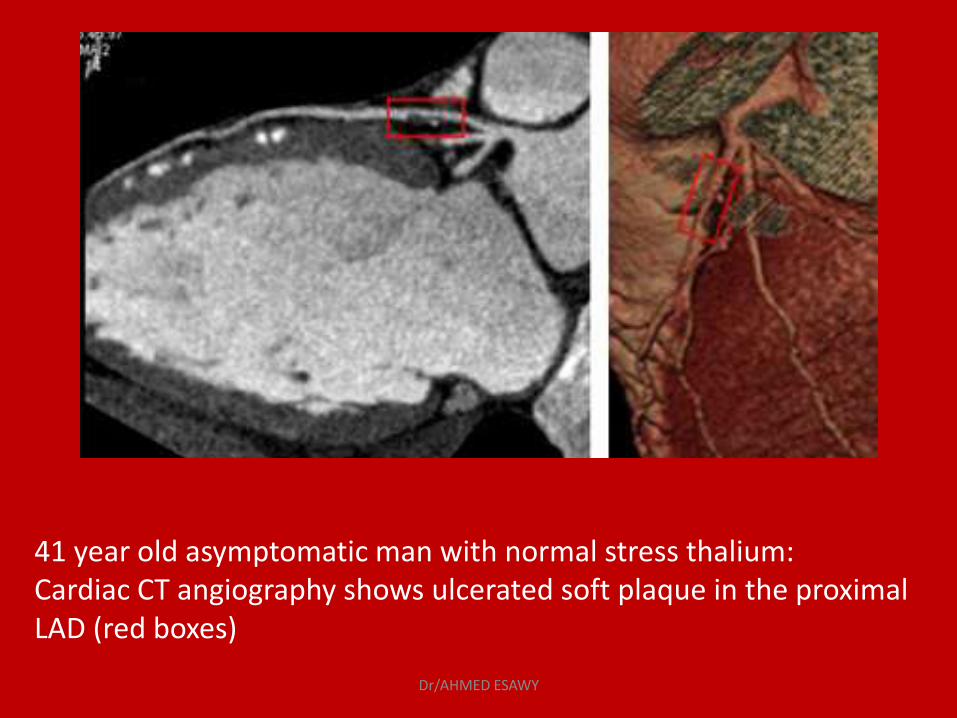
41 year old asymptomatic man with normal stress thalium: Cardiac CT angiography shows ulcerated soft plaque in the proximal LAD (red boxes)
Dr/AHMED ESAWY
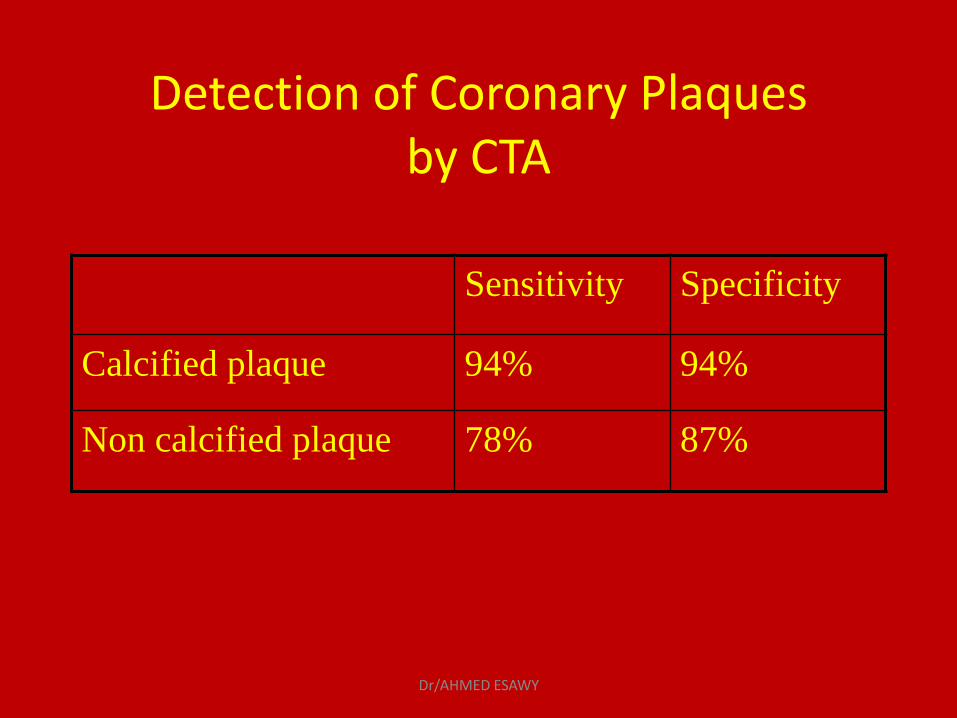
Detection of Coronary Plaques by CTA
Sensitivity Specificity
Calcified plaque 94% 94%
Non calcified plaque 78% 87%
Dr/AHMED ESAWY
Limitation of CT Plaque Imaging
Inadequate spatial resolution
Density measurement highly dependant on slice width and surrounding contrast enhancement
No activity or functional information
Dr/AHMED ESAWY
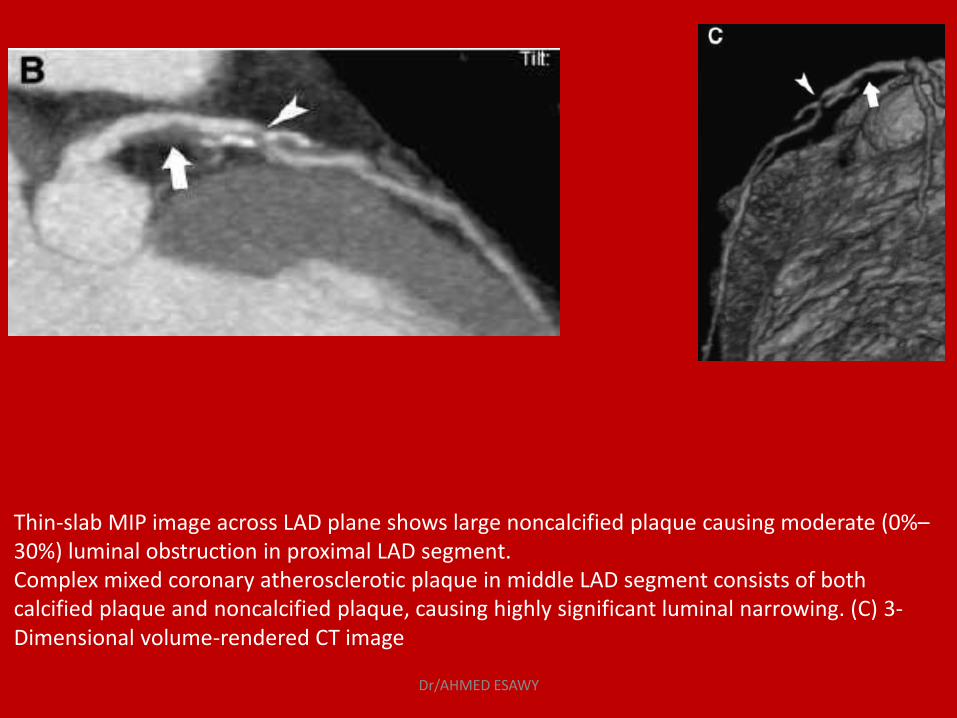
Thin-slab MIP image across LAD plane shows large noncalcified plaque causing moderate (0%–30%) luminal obstruction in proximal LAD segment. Complex mixed coronary atherosclerotic plaque in middle LAD segment consists of both calcified plaque and noncalcified plaque, causing highly significant luminal narrowing. (C) 3-Dimensional volume-rendered CT image
Dr/AHMED ESAWY
CORONARY ARTERY
CALCIFICATION
Dr/AHMED ESAWY
Coronary artery calcification- What do we know?
Coronary artery calcification is a reliable sign of chronic atherosclerotic changes
Calcified coronary plaque = coronary atherosclerosis
Calcium is absent in normal vessel walls
Calcium seen in arterial wall from 20 years of age
Calcification increases with age and with extent of disease
Dr/AHMED ESAWY
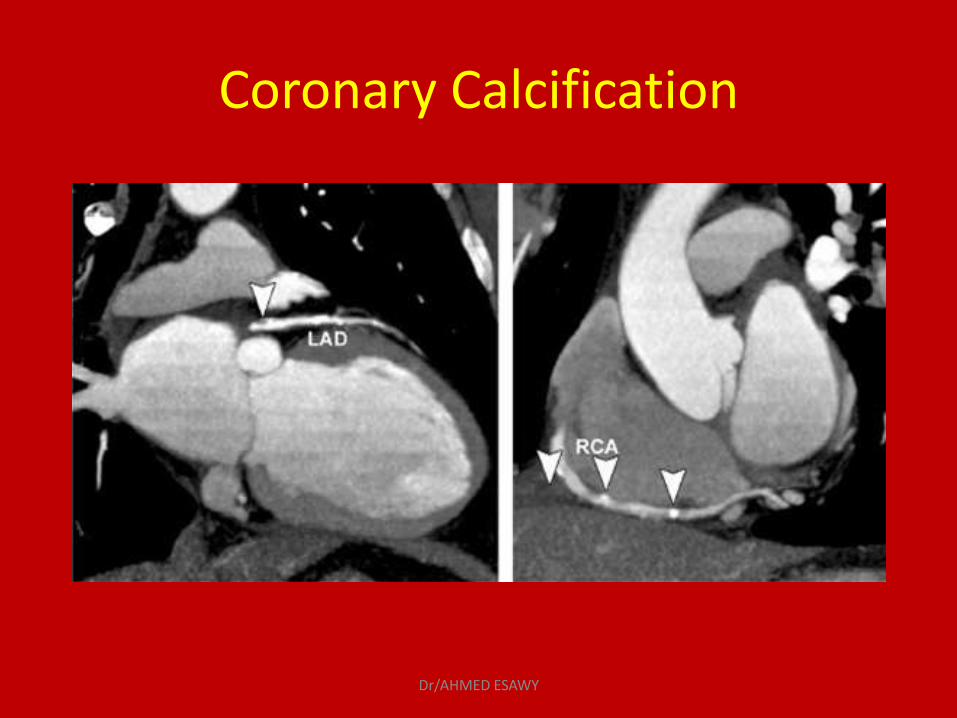
Coronary Calcification
Dr/AHMED ESAWY
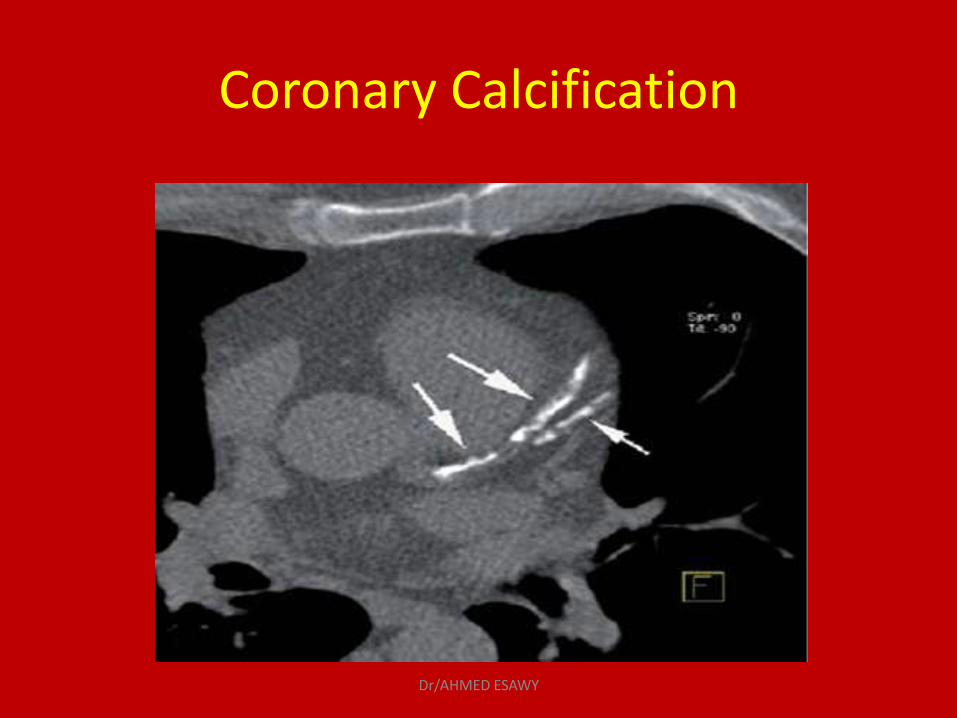
Coronary Calcification
Dr/AHMED ESAWY
Calcium or Agatston Score
Agatston score based on the maximum CT number and the area of calcium deposit in each lesion.
The score of each single lesion on each image is the product of its area multiplied by a cofactor reflecting calcium density in each lesion.
Agatston score is not a linear measurement and is complex to calculate.
Threshold set is > 130 Hu
Dr/AHMED ESAWY
Cardiac Calcium Scoring
Addition of CACS to a prediction model based on traditional risk factors significantly improved the classification of risk
Calcium Score Presence of CAD
0 No evidence of CAD
1-10 Minimal evidence of CAD
11-100 Mild evidence of CAD
101-400 Moderate evidence of CAD
Over 400 Extensive evidence of CAD
Dr/AHMED ESAWY
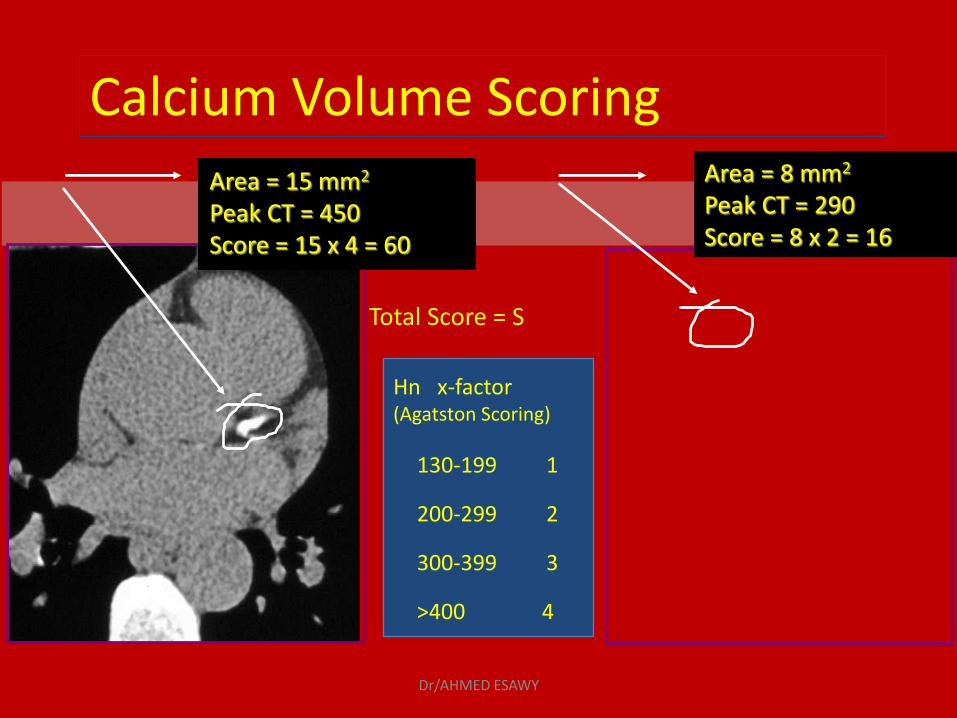
Hn x-factor (Agatston Scoring)
130-199 1
200-299 2
300-399 3
>400 4
Area = 15 mm2 Peak CT = 450 Score = 15 x 4 = 60
Area = 8 mm2 Peak CT = 290 Score = 8 x 2 = 16
Total Score = S
Calcium Volume Scoring
Dr/AHMED ESAWY
Who should be screened using CT for calcium scoring ? - Patient with risk factors for CAD (high cholesterol, DM, HTN,
Smoker, obese, FH of CAD) What are the limitations of Cardiac CT for Calcium Scoring? - weight limit, CAD can still be present without calcium even
if your calcium score is low, HR > 90, insurance coverage
- Calcium score correlates directly with risk of events and likelihood of obstructive CAD
Dr/AHMED ESAWY
Predictive Value of Coronary Calcium for cardiac events
Calcium scores have predictive value for future coronary events.
Calcium score > 100 : medium risk
Calcium score > 400 : high risk
Calcium score > 1000 : very high risk (events in
the short term (1-2 years)
Dr/AHMED ESAWY
Prognostic Value of Calcium Scoring
Calcium score > 100.
10 times high risk of a cardiac event than those with lower score
Cardiac events occurred earlier and more frequently in patients with scores > 1000.
Dr/AHMED ESAWY
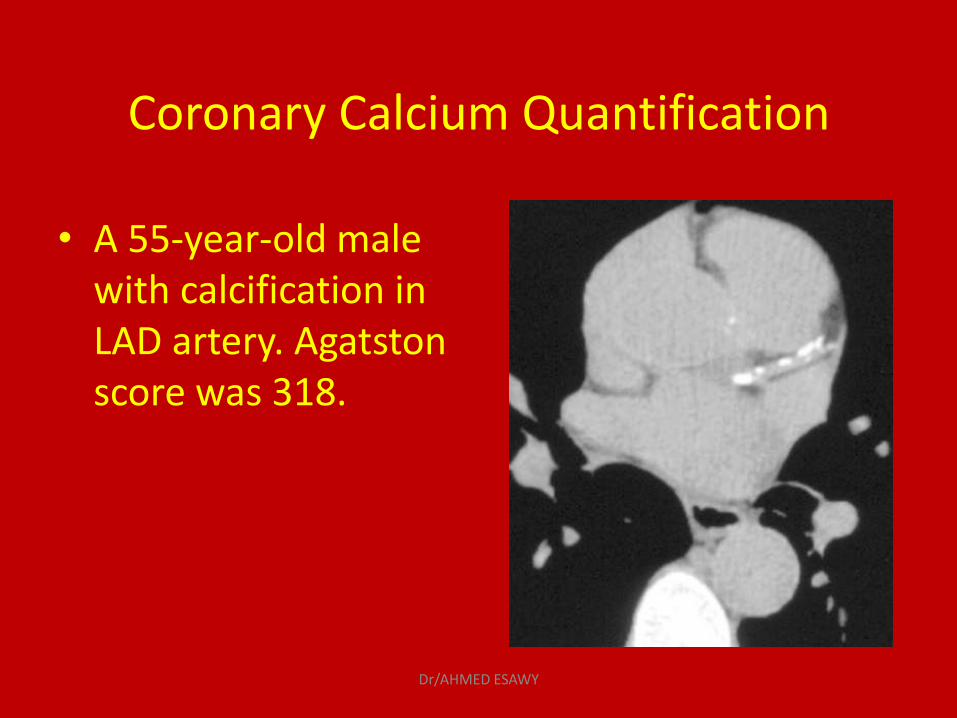
Coronary Calcium Quantification
• A 55-year-old male with calcification in LAD artery. Agatston score was 318.
Dr/AHMED ESAWY
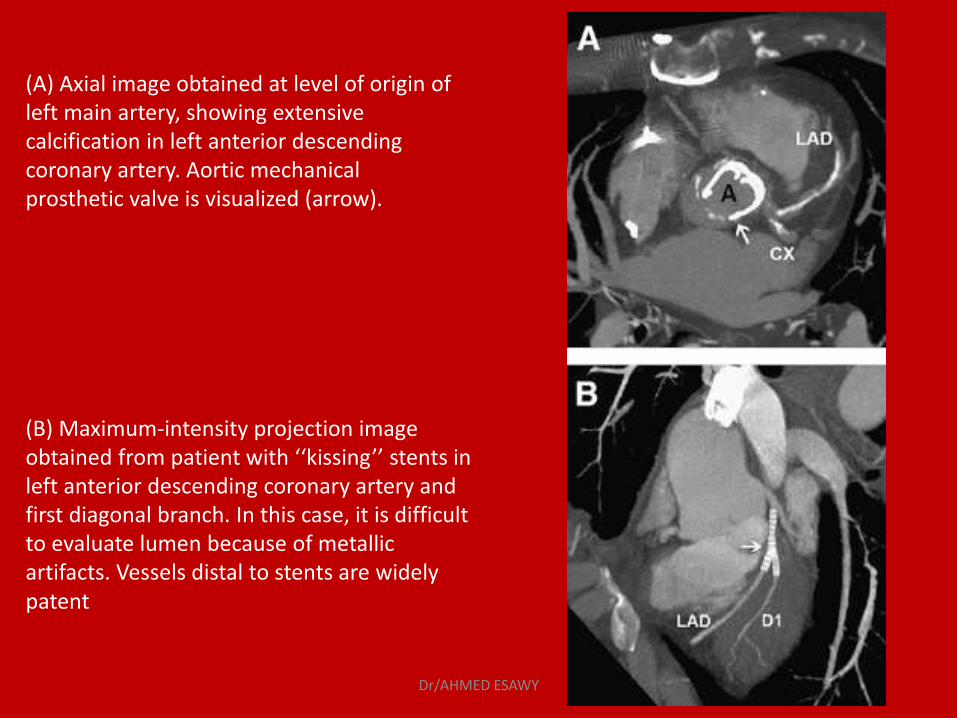
(A) Axial image obtained at level of origin of left main artery, showing extensive calcification in left anterior descending coronary artery. Aortic mechanical prosthetic valve is visualized (arrow). (B) Maximum-intensity projection image obtained from patient with ‘‘kissing’’ stents in left anterior descending coronary artery and first diagonal branch. In this case, it is difficult to evaluate lumen because of metallic artifacts. Vessels distal to stents are widely patent
Dr/AHMED ESAWY
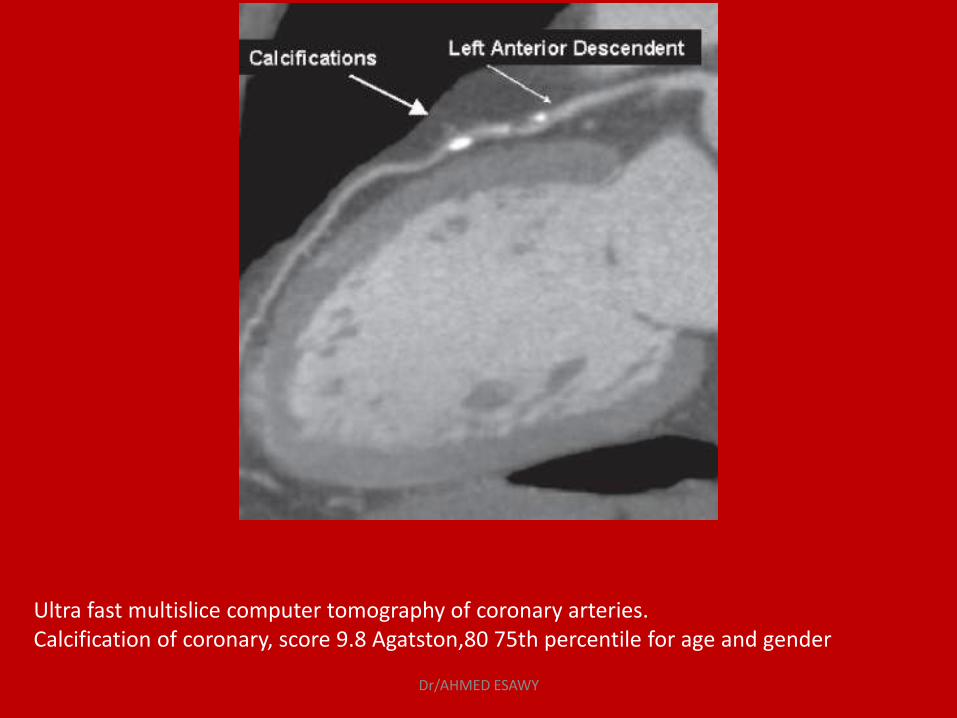
Ultra fast multislice computer tomography of coronary arteries. Calcification of coronary, score 9.8 Agatston,80 75th percentile for age and gender
Dr/AHMED ESAWY
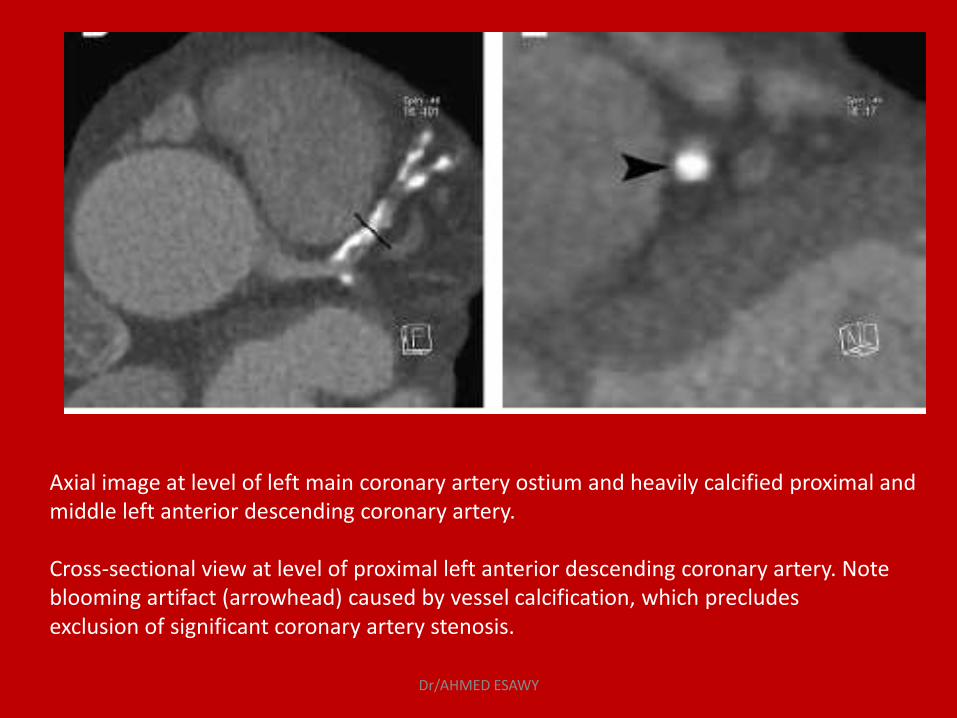
Axial image at level of left main coronary artery ostium and heavily calcified proximal and middle left anterior descending coronary artery. Cross-sectional view at level of proximal left anterior descending coronary artery. Note blooming artifact (arrowhead) caused by vessel calcification, which precludes exclusion of significant coronary artery stenosis.
Dr/AHMED ESAWY
CORONARY ARTERY
STENOSIS
Dr/AHMED ESAWY
Coronary Artery Stenosis
• Hemodynamically relevant stenosis was defined as substantial wall irregularity, with more than 50% vascular narrowing.
• The degree of stenosis was measured on transverse scans and MPRs by using an automated distance-measuring tool.
Dr/AHMED ESAWY

Dr/AHMED ESAWY
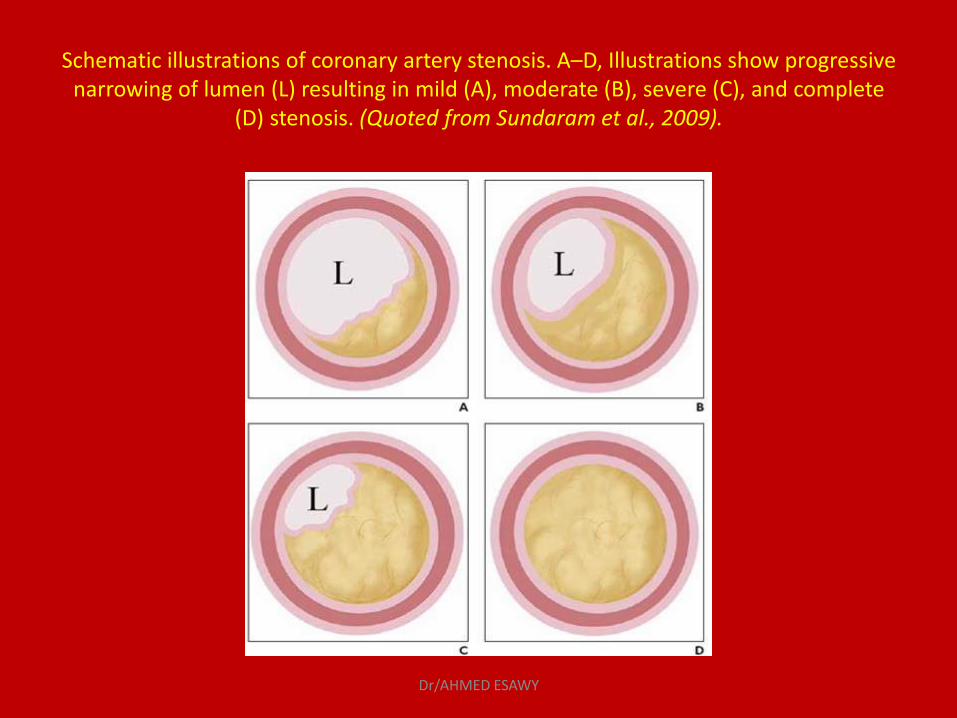
Schematic illustrations of coronary artery stenosis. A–D, Illustrations show progressive narrowing of lumen (L) resulting in mild (A), moderate (B), severe (C), and complete
(D) stenosis. (Quoted from Sundaram et al., 2009).
Dr/AHMED ESAWY
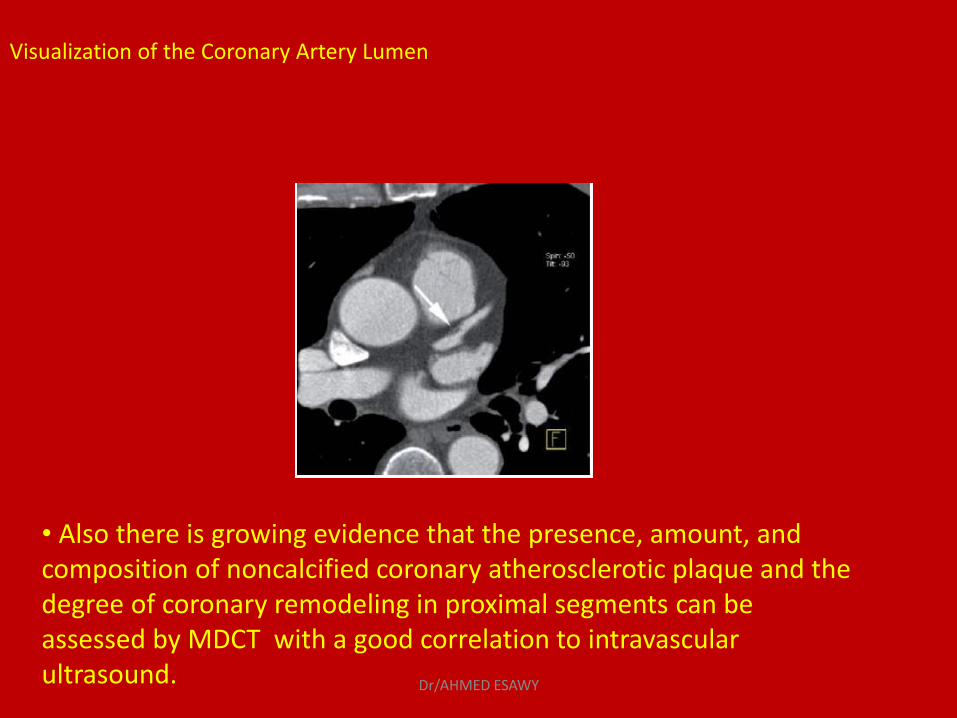
• Also there is growing evidence that the presence, amount, and composition of noncalcified coronary atherosclerotic plaque and the degree of coronary remodeling in proximal segments can be assessed by MDCT with a good correlation to intravascular ultrasound.
Visualization of the Coronary Artery Lumen
Dr/AHMED ESAWY
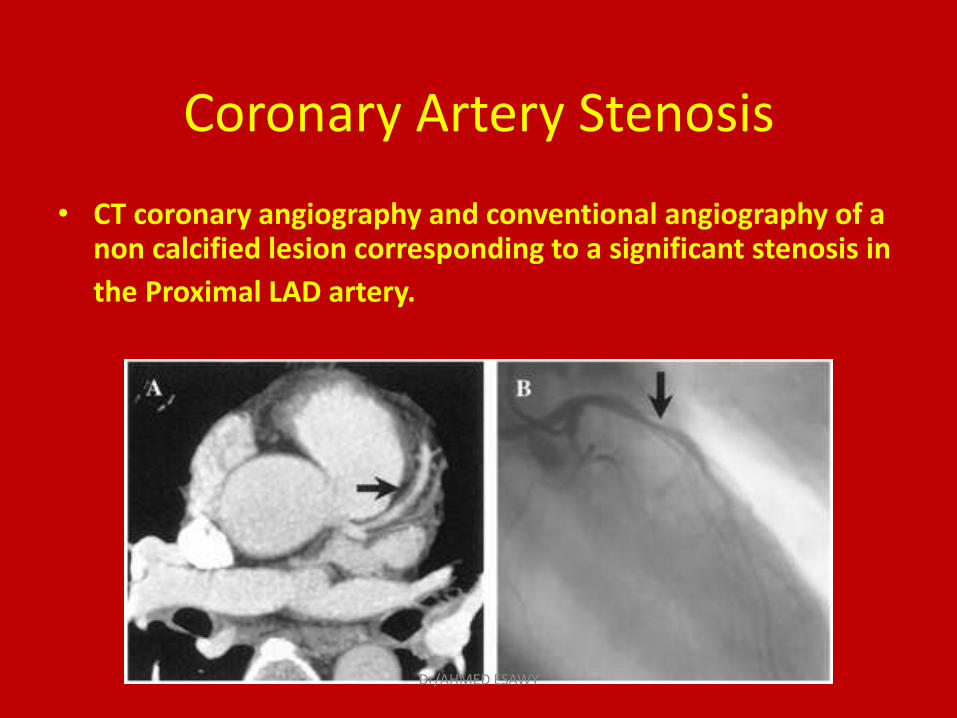
Coronary Artery Stenosis
• CT coronary angiography and conventional angiography of a non calcified lesion corresponding to a significant stenosis in
the Proximal LAD artery.
Dr/AHMED ESAWY
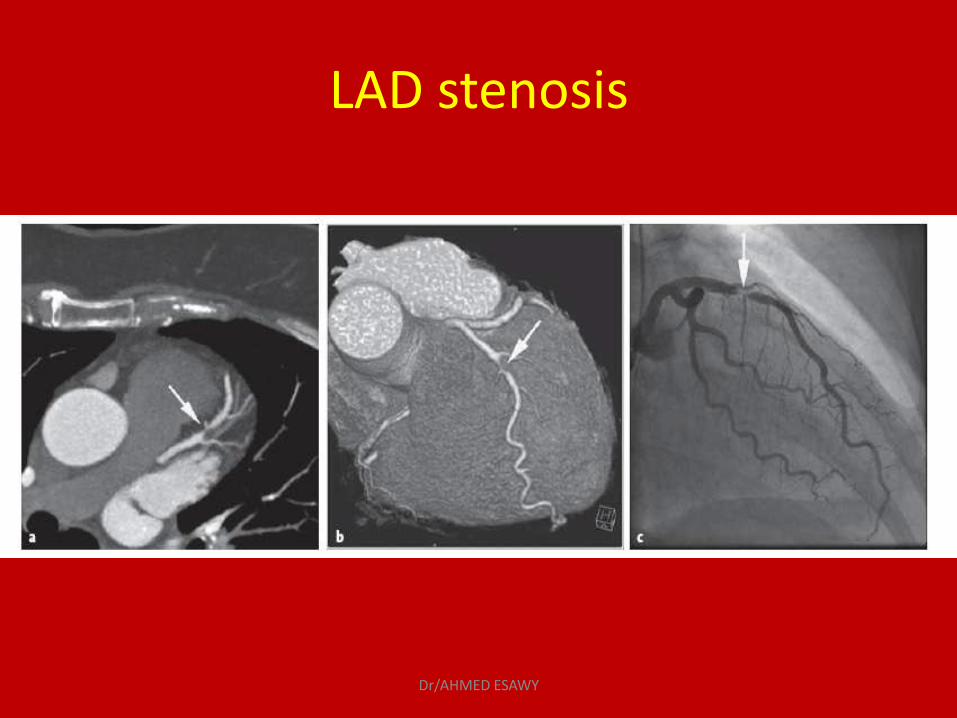
LAD stenosis
Dr/AHMED ESAWY
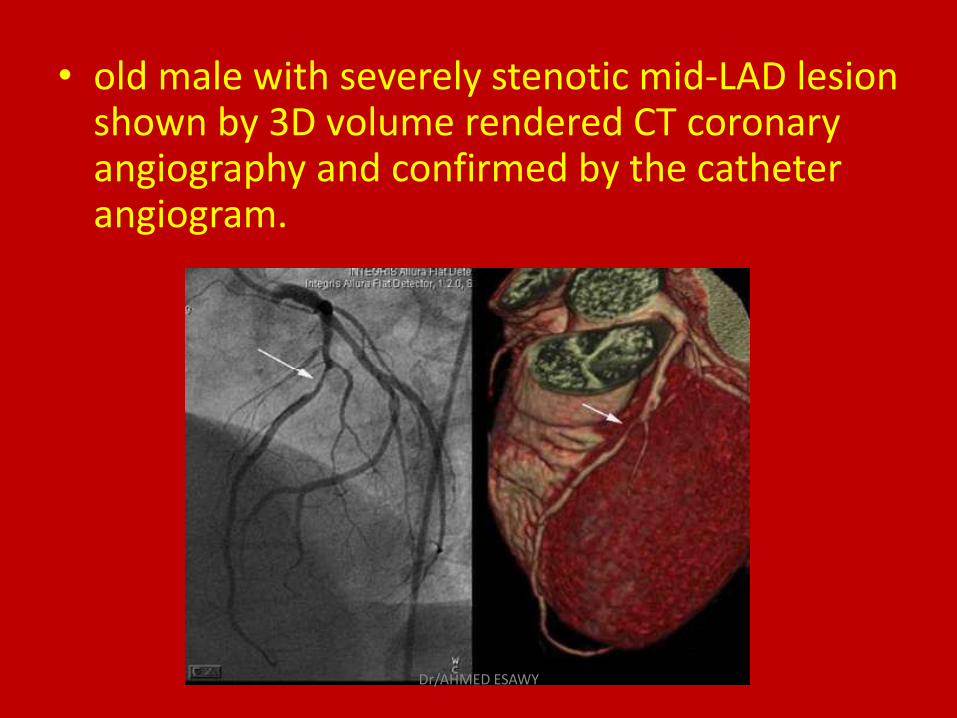
• old male with severely stenotic mid-LAD lesion shown by 3D volume rendered CT coronary angiography and confirmed by the catheter angiogram.
Dr/AHMED ESAWY
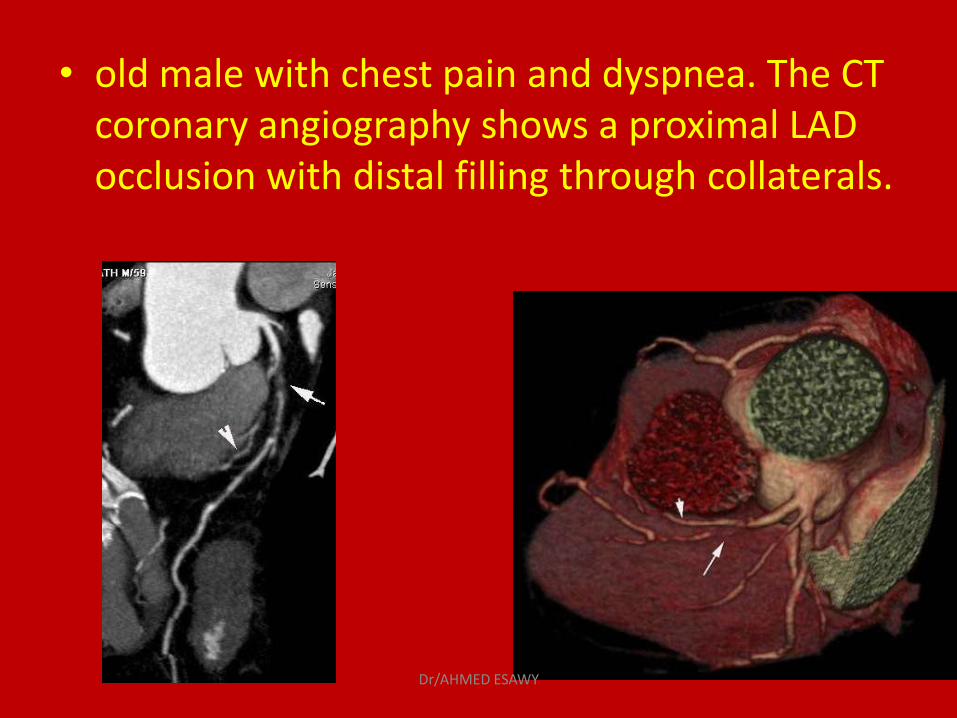
• old male with chest pain and dyspnea. The CT coronary angiography shows a proximal LAD occlusion with distal filling through collaterals.
Dr/AHMED ESAWY
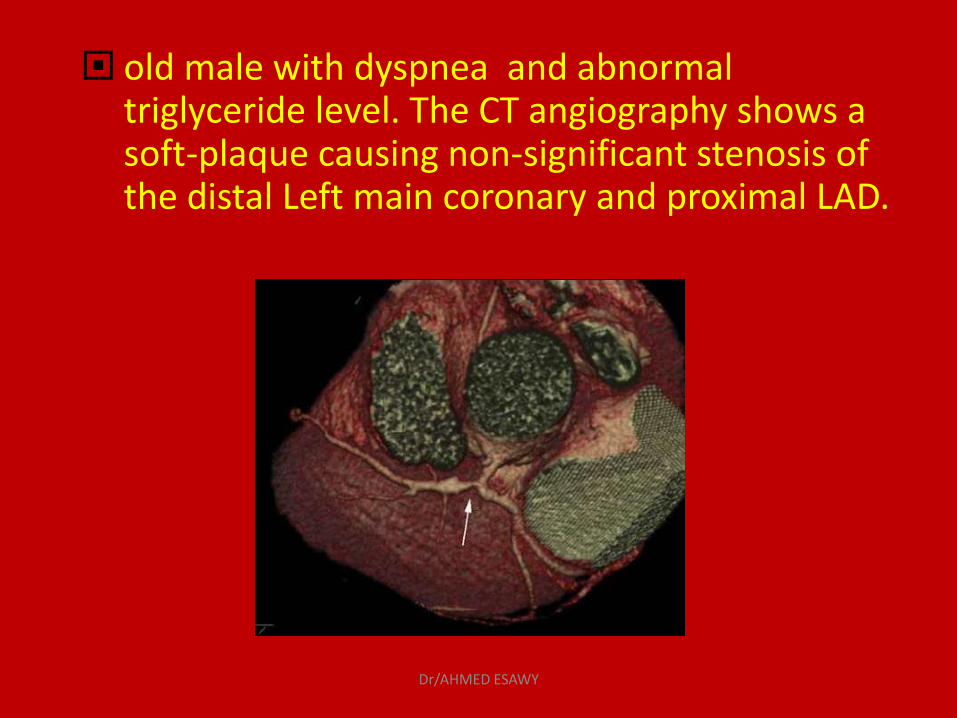
old male with dyspnea and abnormal triglyceride level. The CT angiography shows a soft-plaque causing non-significant stenosis of the distal Left main coronary and proximal LAD.
Dr/AHMED ESAWY

Oblique coronal image obtained from patient with anginal symptoms and indeterminate stress test results, showing severe stenosis of ostium of left main coronary artery (arrow).
Dr/AHMED ESAWY
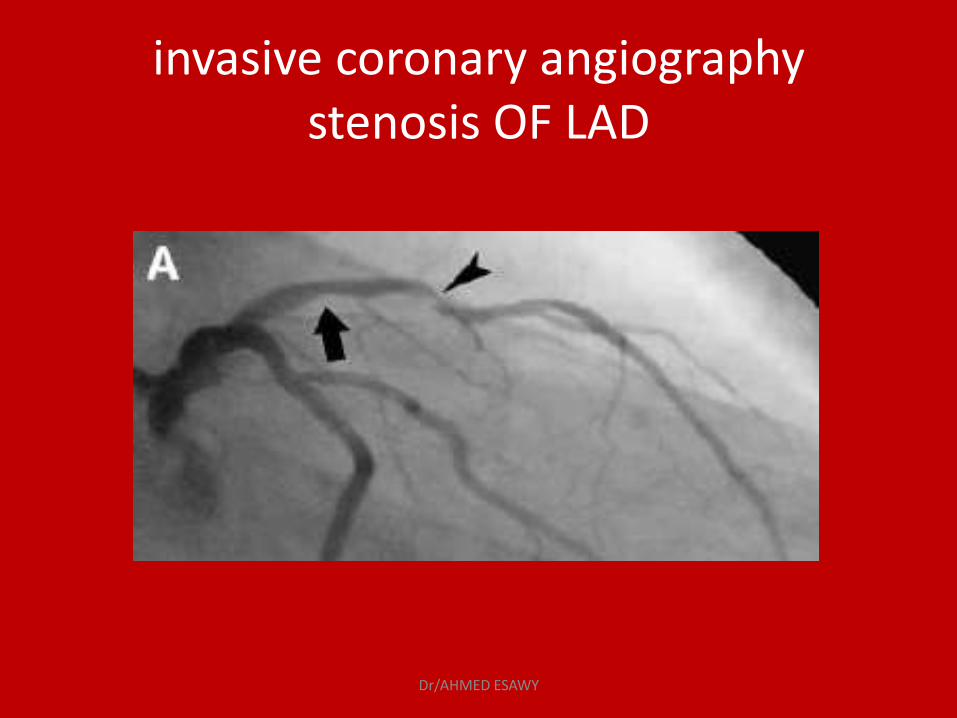
invasive coronary angiography stenosis OF LAD
Dr/AHMED ESAWY
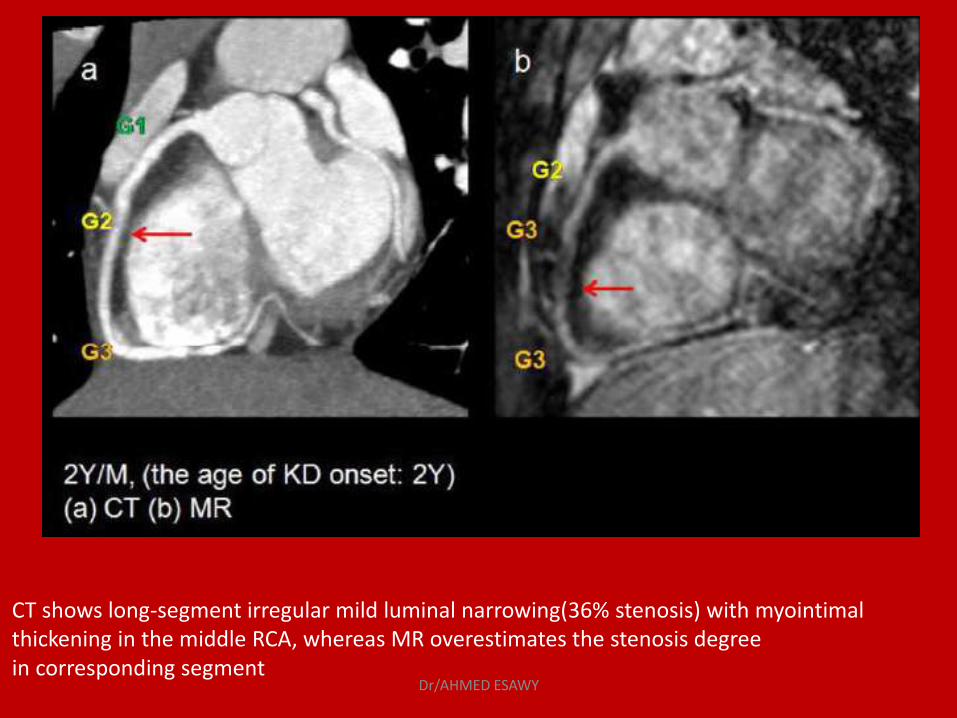
CT shows long-segment irregular mild luminal narrowing(36% stenosis) with myointimal thickening in the middle RCA, whereas MR overestimates the stenosis degree in corresponding segment
Dr/AHMED ESAWY
POSTOPERATIVE
EVALUATION OF
CORONARY ARTERY
BY PASS
Dr/AHMED ESAWY
Postoperative evaluation of Coronary Artery
• Coronary artery bypass graft surgery Patency or occlusion of grafts can be established
by the presence or absence of contrast enhancement, respectively.
However, artifacts from metallic surgical clips may obscure the adjacent portion of a coronary graft.
Dr/AHMED ESAWY
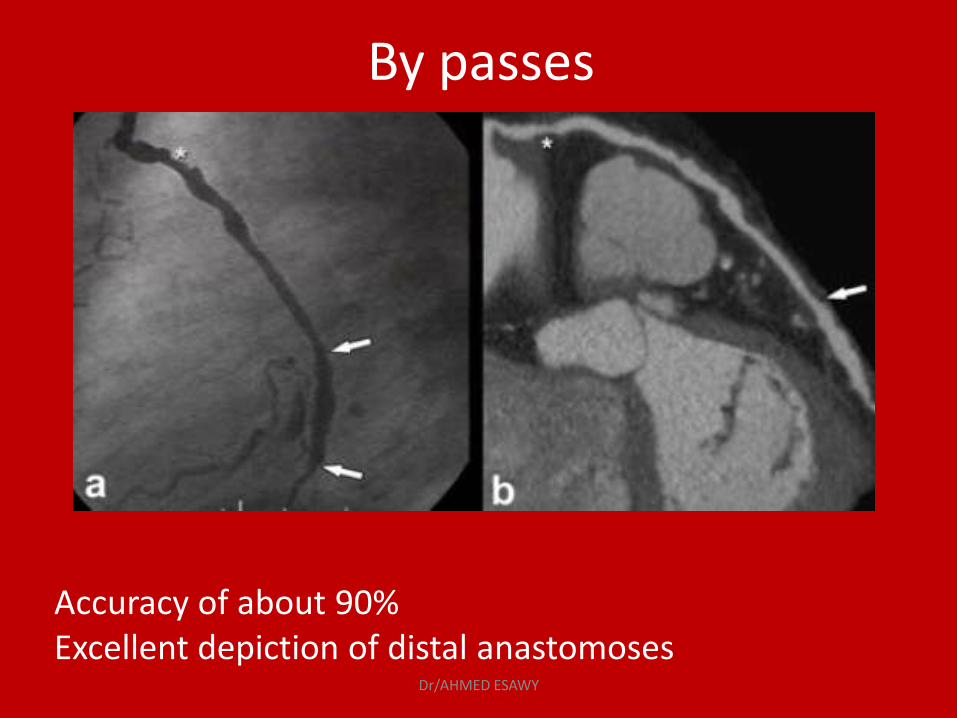
By passes
Accuracy of about 90% Excellent depiction of distal anastomoses
Dr/AHMED ESAWY
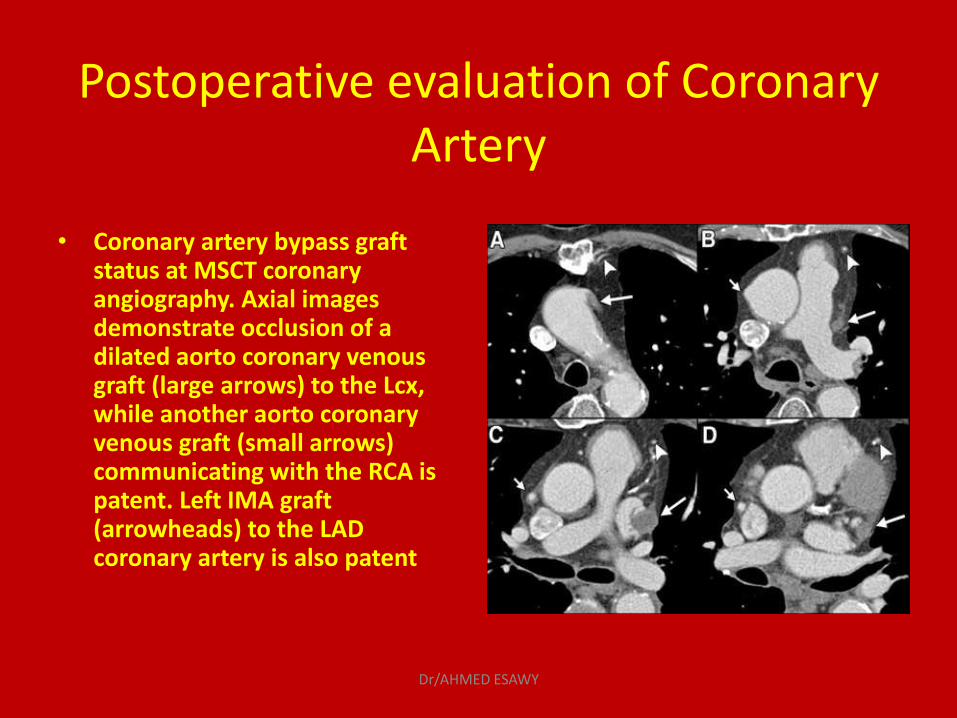
Postoperative evaluation of Coronary Artery
• Coronary artery bypass graft status at MSCT coronary angiography. Axial images demonstrate occlusion of a dilated aorto coronary venous graft (large arrows) to the Lcx, while another aorto coronary venous graft (small arrows) communicating with the RCA is patent. Left IMA graft (arrowheads) to the LAD coronary artery is also patent
Dr/AHMED ESAWY
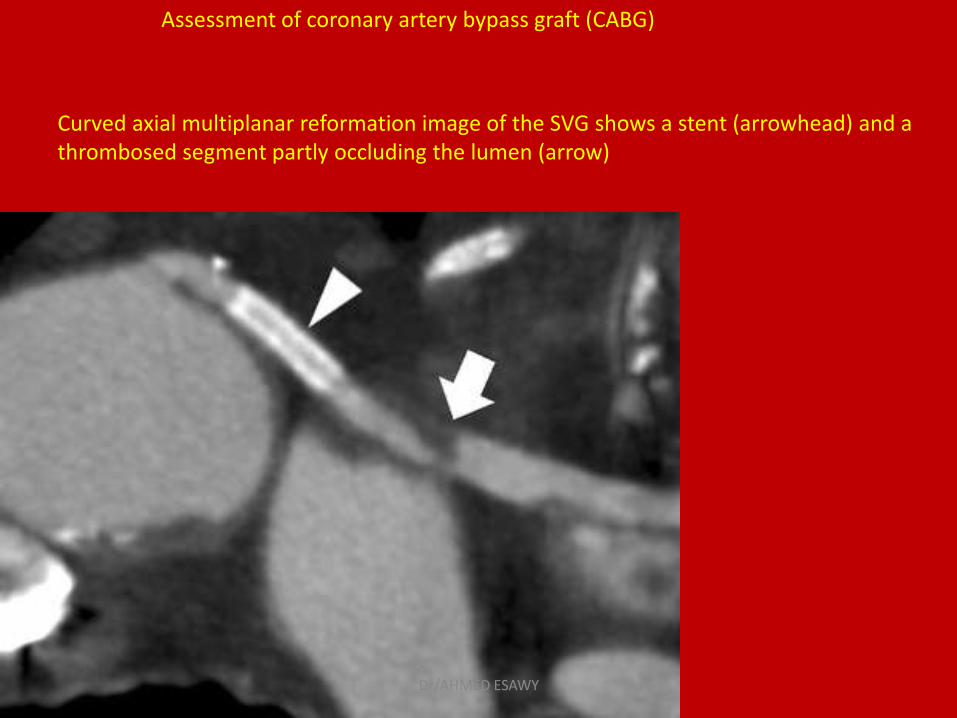
Assessment of coronary artery bypass graft (CABG)
Curved axial multiplanar reformation image of the SVG shows a stent (arrowhead) and a thrombosed segment partly occluding the lumen (arrow)
Dr/AHMED ESAWY
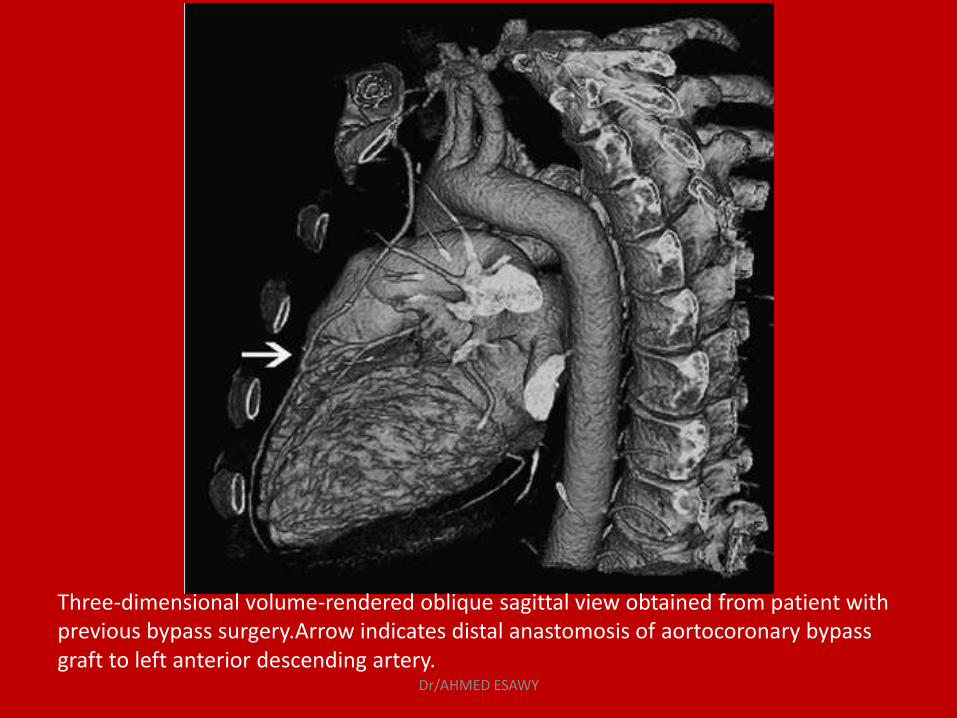
Three-dimensional volume-rendered oblique sagittal view obtained from patient with previous bypass surgery.Arrow indicates distal anastomosis of aortocoronary bypass graft to left anterior descending artery.
Dr/AHMED ESAWY
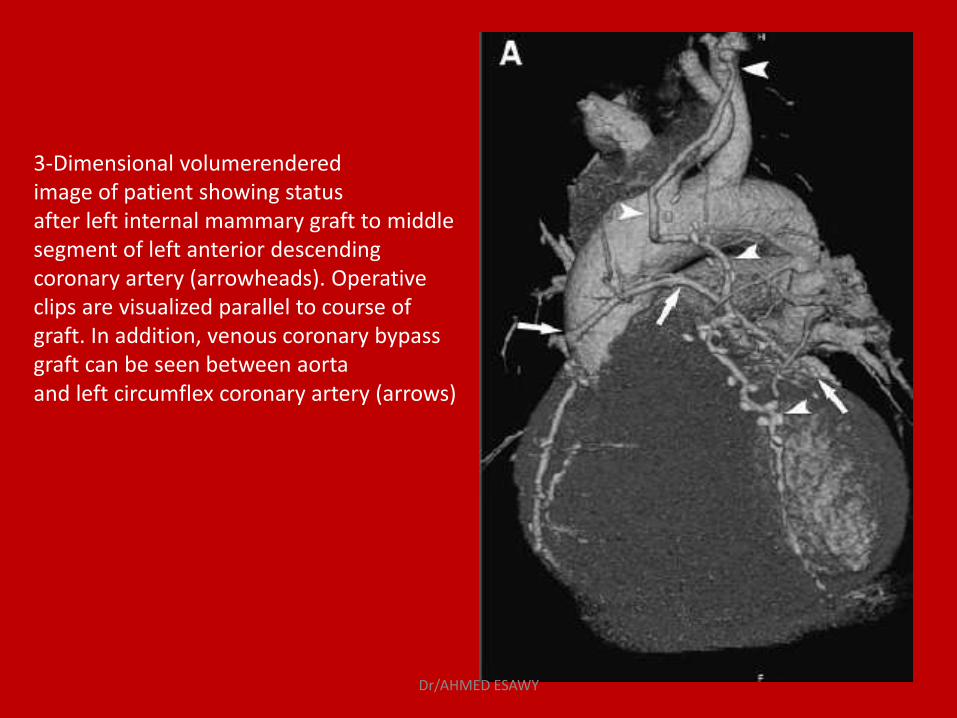
3-Dimensional volumerendered image of patient showing status after left internal mammary graft to middle segment of left anterior descending coronary artery (arrowheads). Operative clips are visualized parallel to course of graft. In addition, venous coronary bypass graft can be seen between aorta and left circumflex coronary artery (arrows)
Dr/AHMED ESAWY
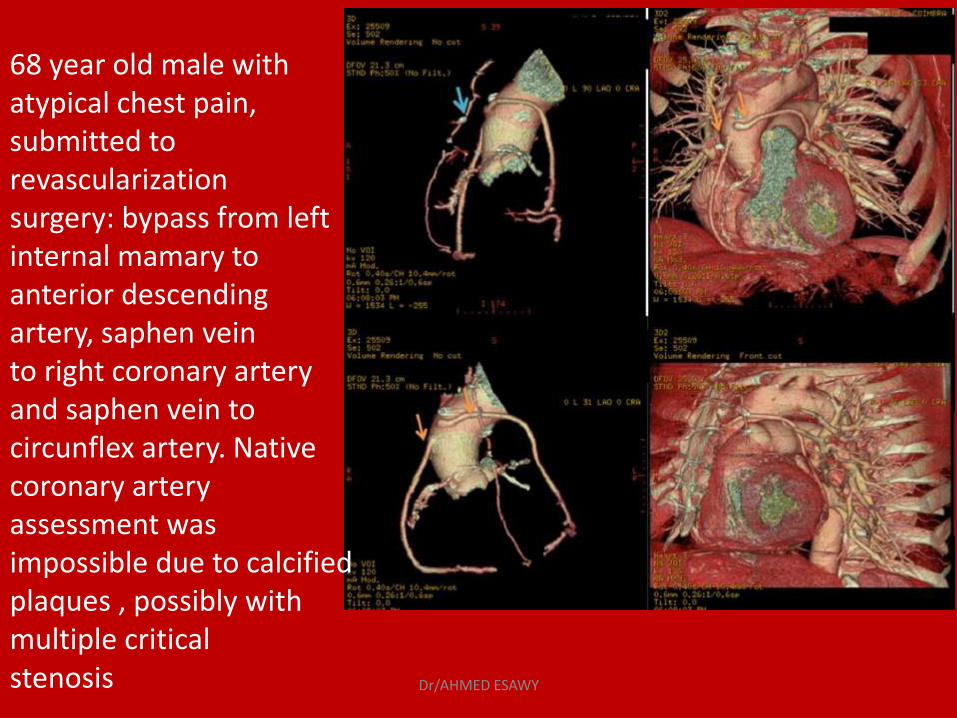
68 year old male with atypical chest pain, submitted to revascularization surgery: bypass from left internal mamary to anterior descending artery, saphen vein to right coronary artery and saphen vein to circunflex artery. Native coronary artery assessment was impossible due to calcified plaques , possibly with multiple critical stenosis Dr/AHMED ESAWY
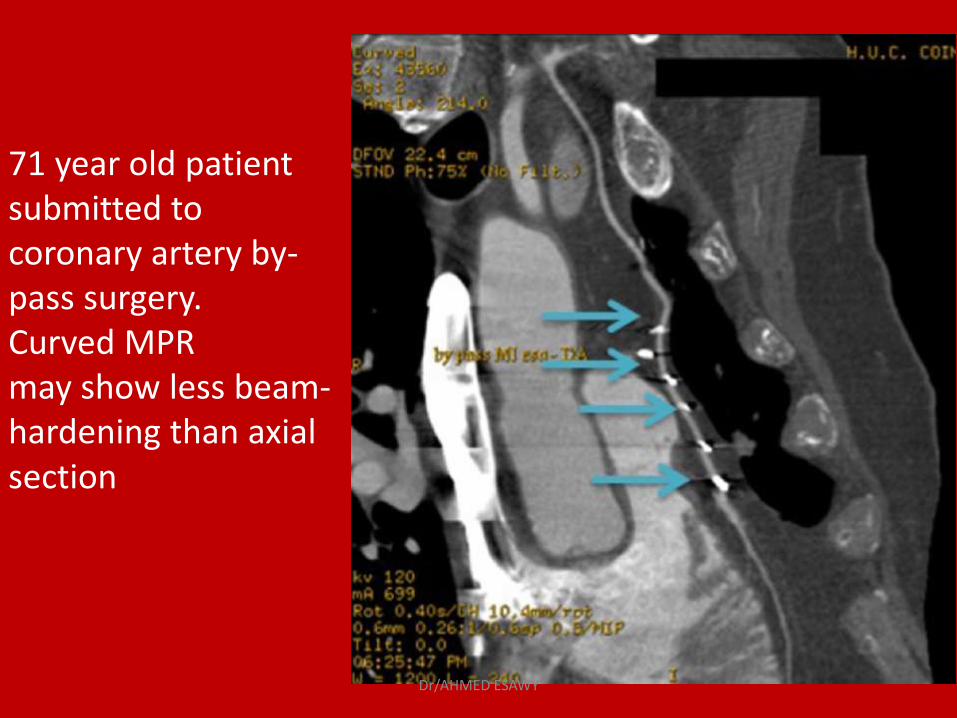
71 year old patient submitted to coronary artery by-pass surgery. Curved MPR may show less beam-hardening than axial section
Dr/AHMED ESAWY
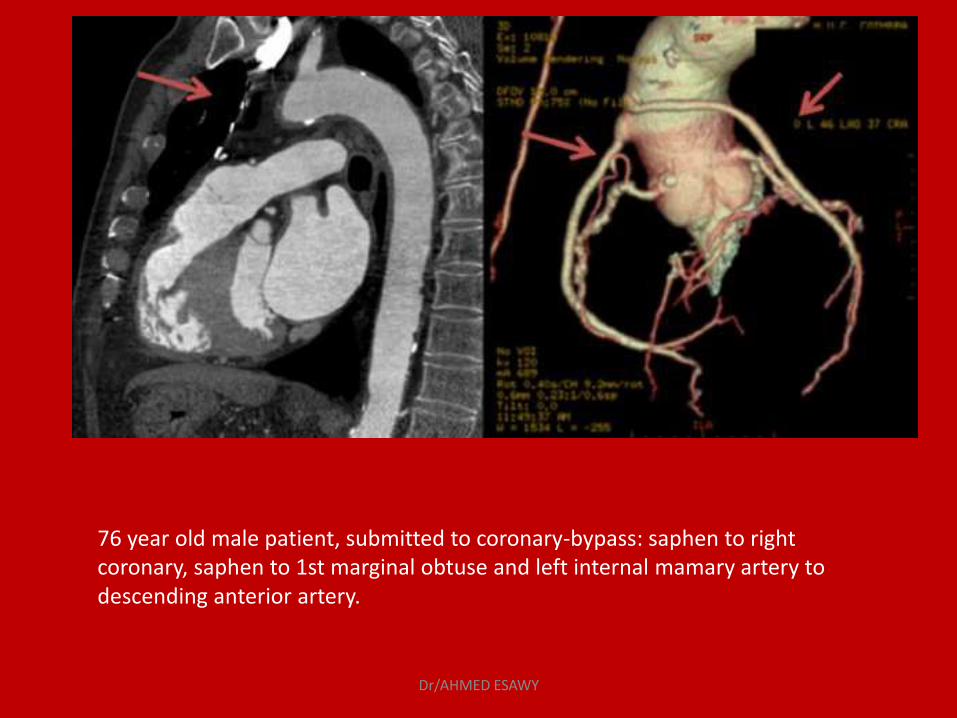
76 year old male patient, submitted to coronary-bypass: saphen to right coronary, saphen to 1st marginal obtuse and left internal mamary artery to descending anterior artery.
Dr/AHMED ESAWY
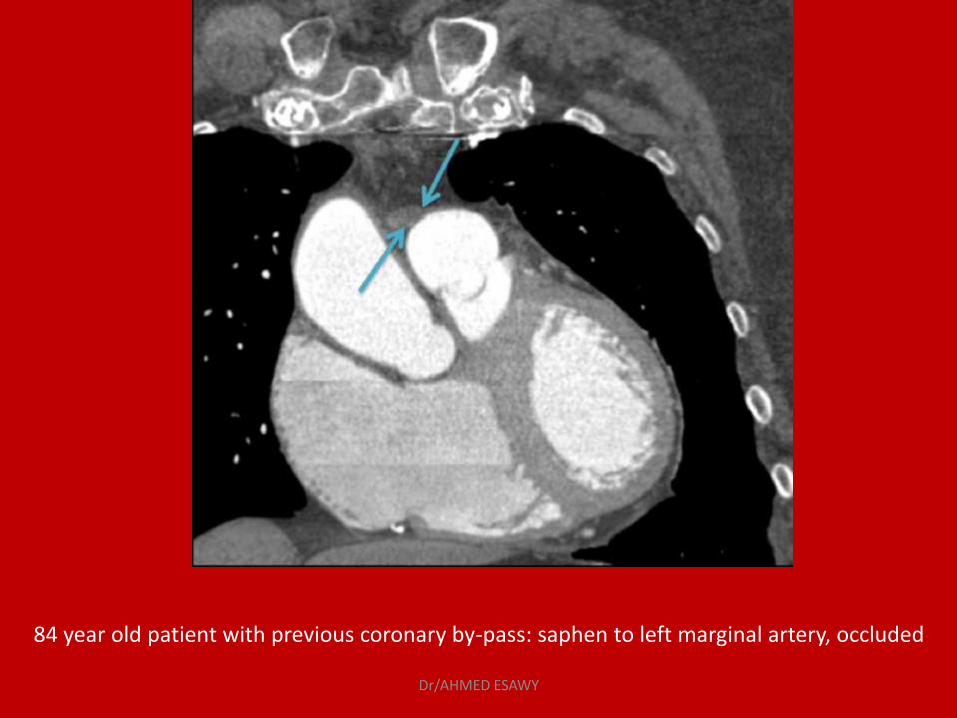
84 year old patient with previous coronary by-pass: saphen to left marginal artery, occluded
Dr/AHMED ESAWY
Looking at the MDCT:Surgery
• Overview anastomisis (start by the 3D) • Evalute grafts in axial and orhogonal MPR planes • Evaluate anastomosis and run-off • Evaluate aorta and left-ventricle size
• It is essential that the whole graft is included in the acquisition. • The most common cause of saphenous graft failure is thrombosis in
the first year and after that atherosclerotic changes ensue. • Arterial grafts usually have longer life span. • MDCT, unlike angiography, allows assessment of occluded grafts
Dr/AHMED ESAWY
POSTOPERATIVE
EVALUATION OF
CORONARY ARTERY
STENT
Dr/AHMED ESAWY
Postoperative evaluation of Coronary Artery
Coronary artery stent
Evaluation of stent patency is by demonstration of contrast enhancement at the leading and trailing ends of a stent.
Dr/AHMED ESAWY
Evaluation of the patency of coronary vessels after intervention
MDCT is limited in its ability to visualize lumen within intracoronary stents because of metal artifacts making the detection of intrastent stenosis difficult.
The accuracy of stent evaluation may depend upon stent diameter
< 3mm inaccessible.
Dr/AHMED ESAWY

Successful (LAD; 3.5 mm) Dr/AHMED ESAWY

Limited (LAD; 4.0 mm) Dr/AHMED ESAWY
Stents
Accuracy of about 70-80% Only BIG stents (≥ 3.5 mm) Only 50% of the small guy2
Dr/AHMED ESAWY
Dr/AHMED ESAWY
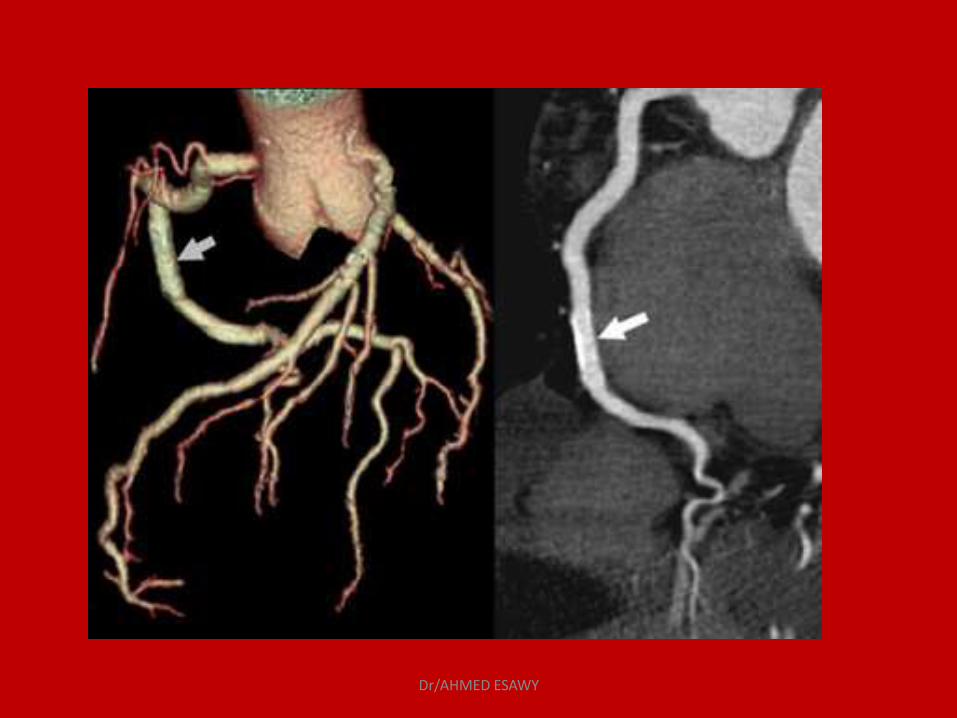
Postoperative evaluation of Coronary Artery
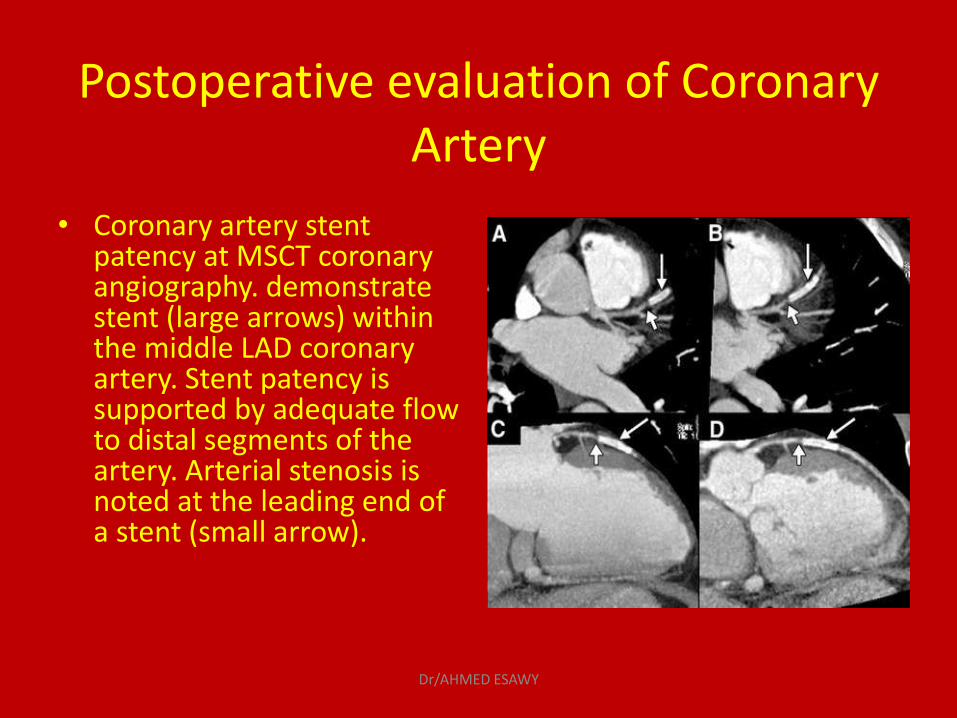
• Coronary artery stent patency at MSCT coronary angiography. demonstrate stent (large arrows) within the middle LAD coronary artery. Stent patency is supported by adequate flow to distal segments of the artery. Arterial stenosis is noted at the leading end of a stent (small arrow).
Dr/AHMED ESAWY
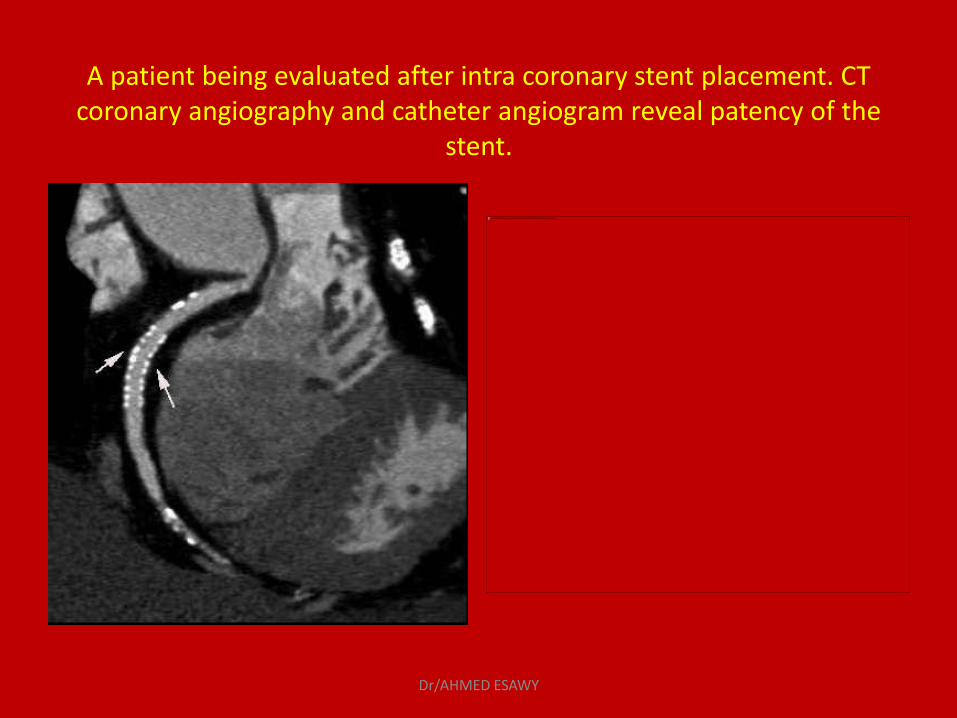
A patient being evaluated after intra coronary stent placement. CT coronary angiography and catheter angiogram reveal patency of the
stent.
Dr/AHMED ESAWY
Imaging of coronary stents
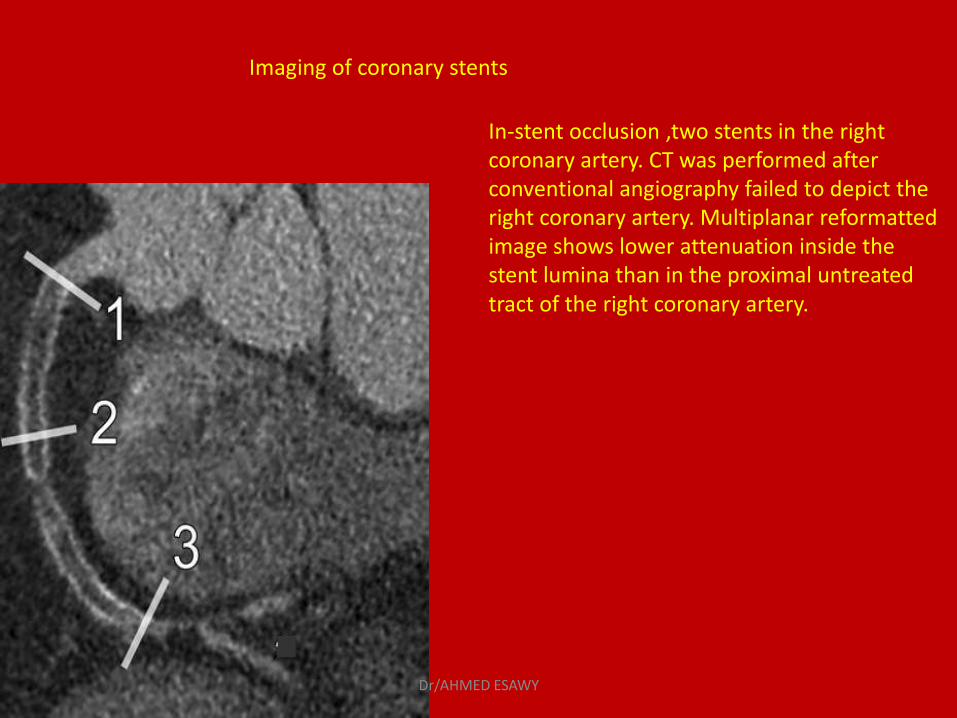
In-stent occlusion ,two stents in the right coronary artery. CT was performed after conventional angiography failed to depict the right coronary artery. Multiplanar reformatted image shows lower attenuation inside the stent lumina than in the proximal untreated tract of the right coronary artery.
Dr/AHMED ESAWY
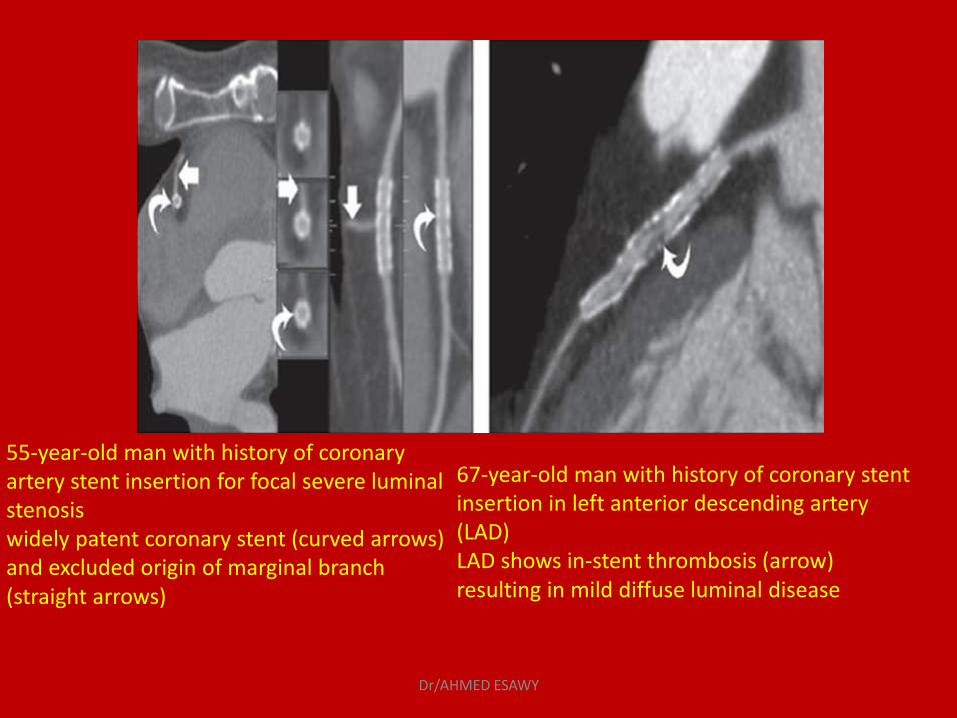
55-year-old man with history of coronary artery stent insertion for focal severe luminal stenosis widely patent coronary stent (curved arrows) and excluded origin of marginal branch (straight arrows)
67-year-old man with history of coronary stent insertion in left anterior descending artery (LAD) LAD shows in-stent thrombosis (arrow) resulting in mild diffuse luminal disease
Dr/AHMED ESAWY
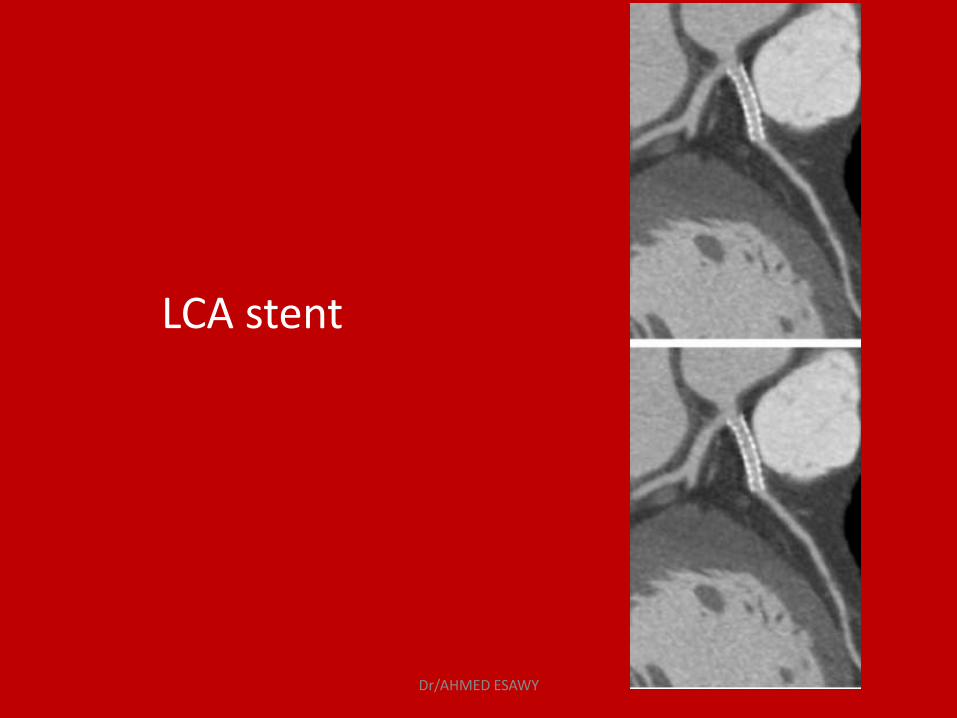
LCA stent
Dr/AHMED ESAWY
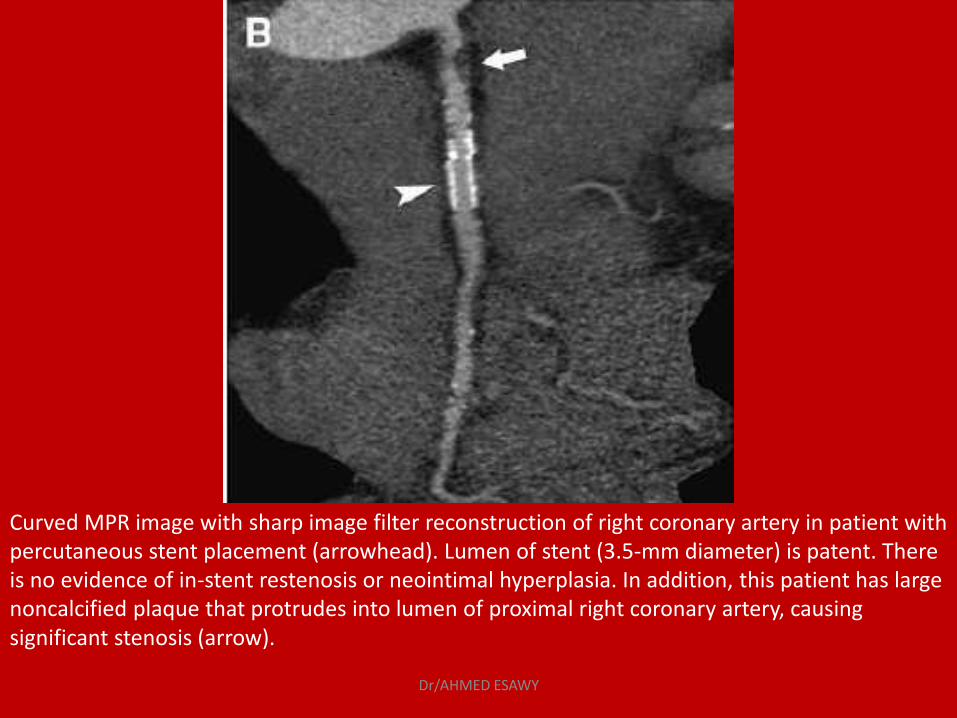
Curved MPR image with sharp image filter reconstruction of right coronary artery in patient with percutaneous stent placement (arrowhead). Lumen of stent (3.5-mm diameter) is patent. There is no evidence of in-stent restenosis or neointimal hyperplasia. In addition, this patient has large noncalcified plaque that protrudes into lumen of proximal right coronary artery, causing significant stenosis (arrow).
Dr/AHMED ESAWY
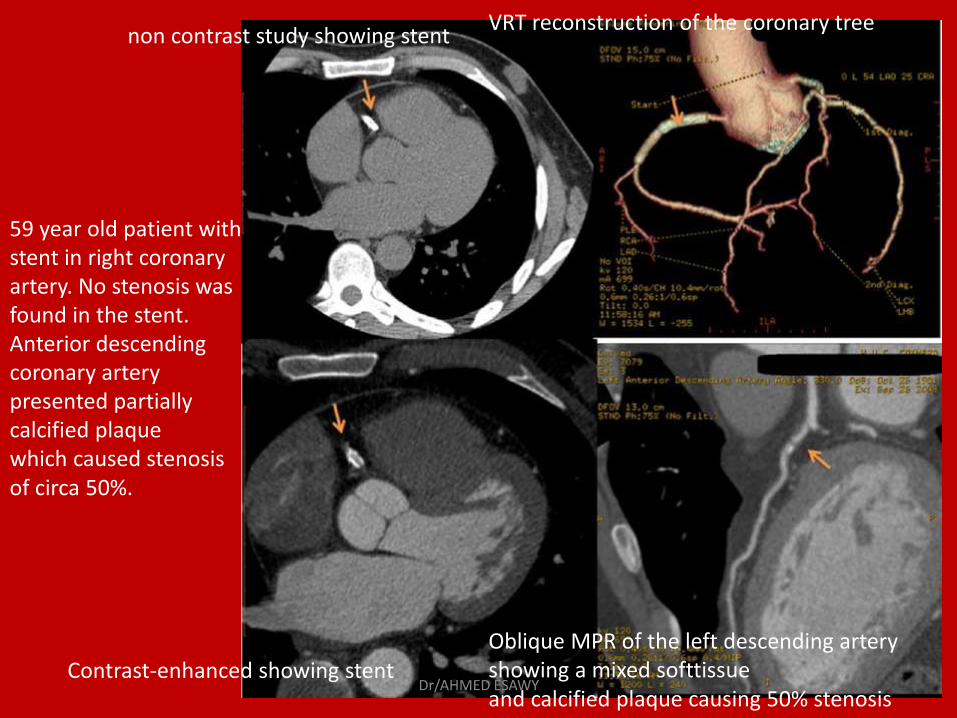
non contrast study showing stent VRT reconstruction of the coronary tree
Contrast-enhanced showing stent Oblique MPR of the left descending artery showing a mixed softtissue and calcified plaque causing 50% stenosis
59 year old patient with stent in right coronary artery. No stenosis was found in the stent. Anterior descending coronary artery presented partially calcified plaque which caused stenosis of circa 50%.
Dr/AHMED ESAWY
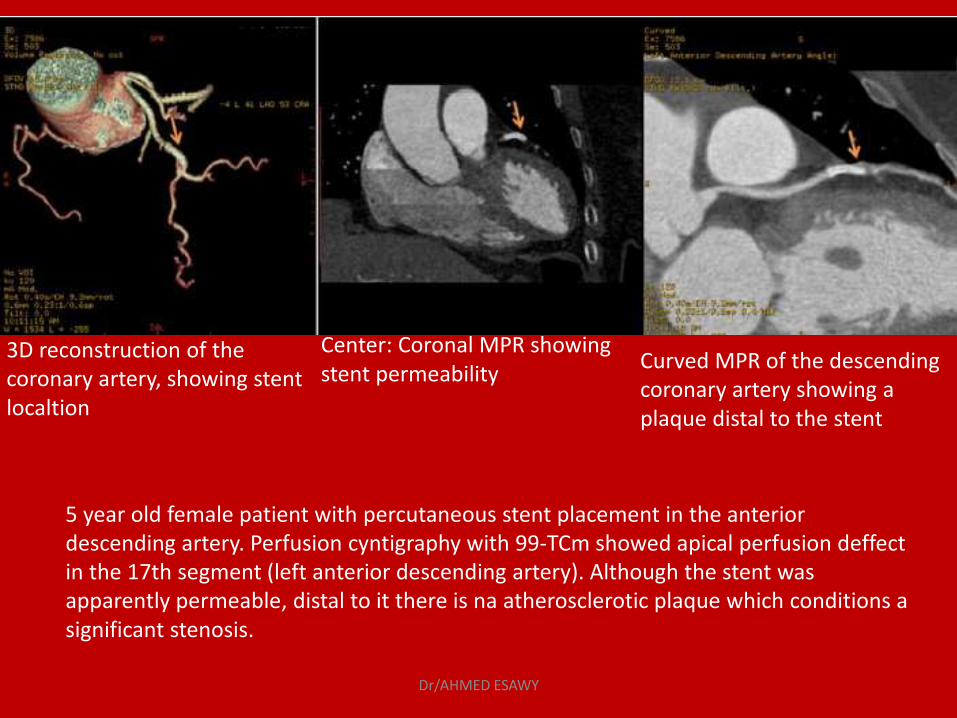
3D reconstruction of the coronary artery, showing stent localtion
Curved MPR of the descending coronary artery showing a plaque distal to the stent
Center: Coronal MPR showing stent permeability
5 year old female patient with percutaneous stent placement in the anterior descending artery. Perfusion cyntigraphy with 99-TCm showed apical perfusion deffect in the 17th segment (left anterior descending artery). Although the stent was apparently permeable, distal to it there is na atherosclerotic plaque which conditions a significant stenosis.
Dr/AHMED ESAWY
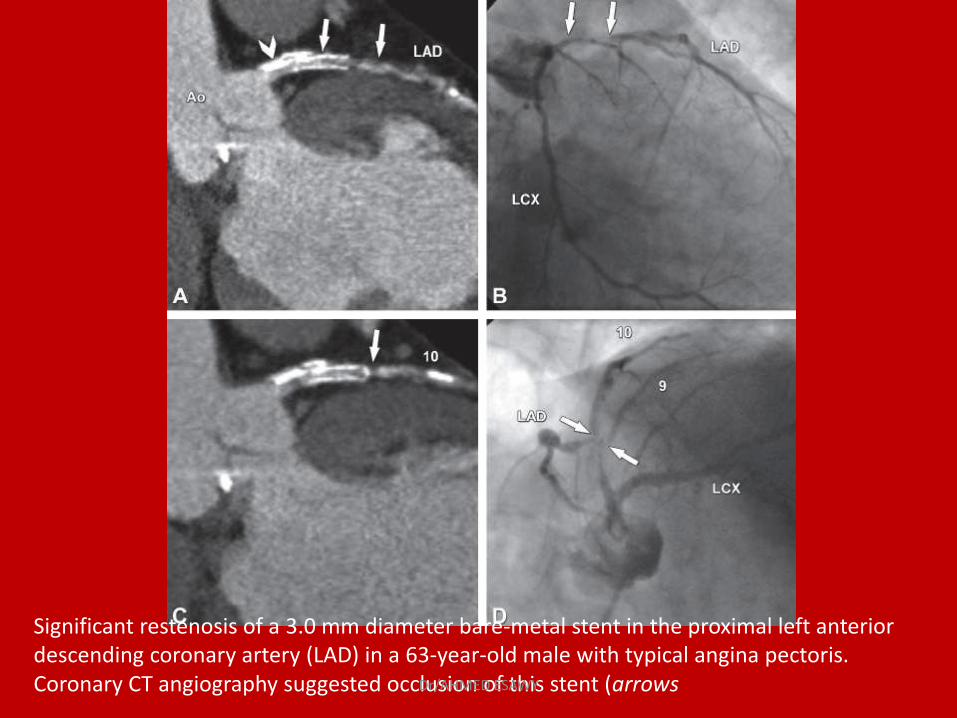
Significant restenosis of a 3.0 mm diameter bare-metal stent in the proximal left anterior descending coronary artery (LAD) in a 63-year-old male with typical angina pectoris. Coronary CT angiography suggested occlusion of this stent (arrows Dr/AHMED ESAWY
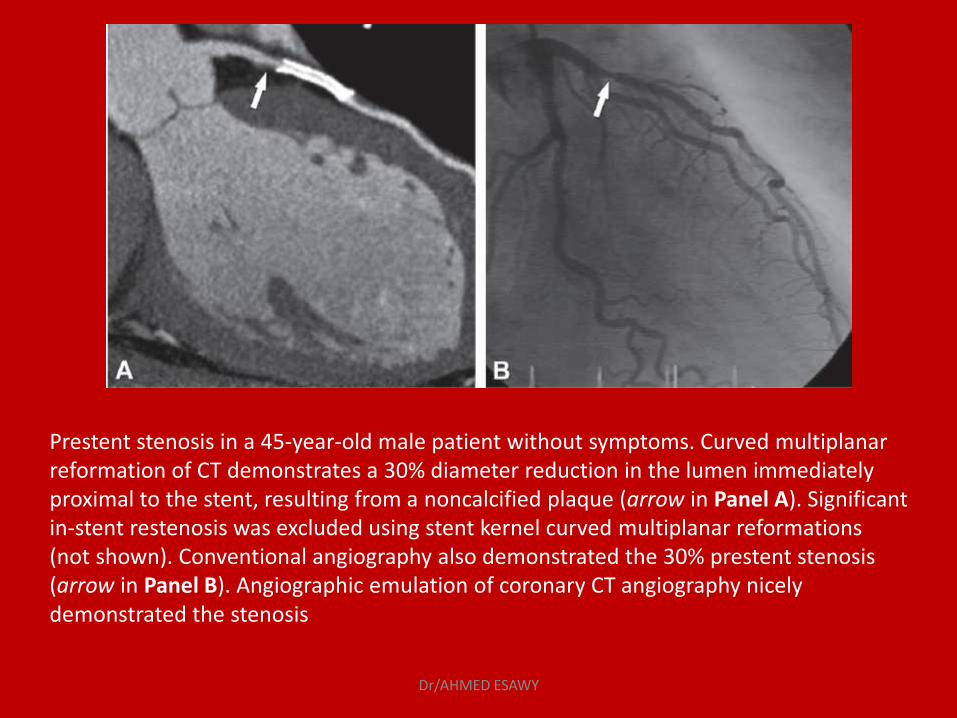
Prestent stenosis in a 45-year-old male patient without symptoms. Curved multiplanar reformation of CT demonstrates a 30% diameter reduction in the lumen immediately proximal to the stent, resulting from a noncalcified plaque (arrow in Panel A). Significant in-stent restenosis was excluded using stent kernel curved multiplanar reformations (not shown). Conventional angiography also demonstrated the 30% prestent stenosis (arrow in Panel B). Angiographic emulation of coronary CT angiography nicely demonstrated the stenosis
Dr/AHMED ESAWY
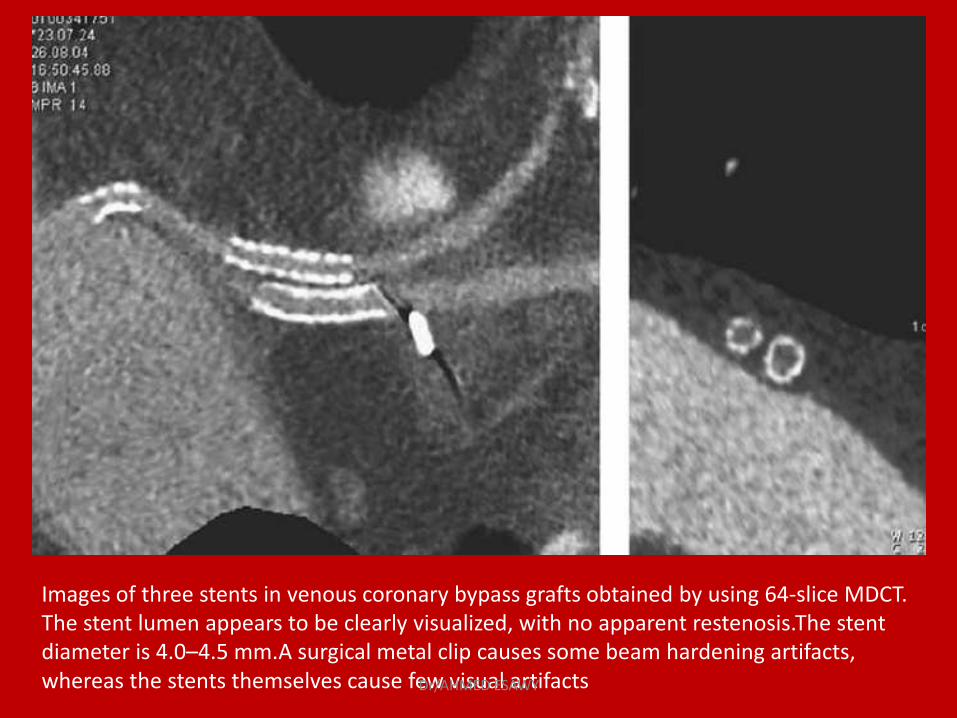
Images of three stents in venous coronary bypass grafts obtained by using 64-slice MDCT. The stent lumen appears to be clearly visualized, with no apparent restenosis.The stent diameter is 4.0–4.5 mm.A surgical metal clip causes some beam hardening artifacts, whereas the stents themselves cause few visual artifacts Dr/AHMED ESAWY
Coronary Stent Fracture
Dr/AHMED ESAWY
What to state on the examination? • Is the in-stent portion diagnostic quality? • Is there stenosis inside the stent
• Looking at the MDCT:Stents
1. Multiplanar reconstructions 2. Used curved MPR 3. If artifacts cannot be excluded then lumen is nondiagnostic.
• Presence of distal contrast does not exclude in-stent stenosis. • Major complications are stent-thrombosis and restenosis.
Dr/AHMED ESAWY
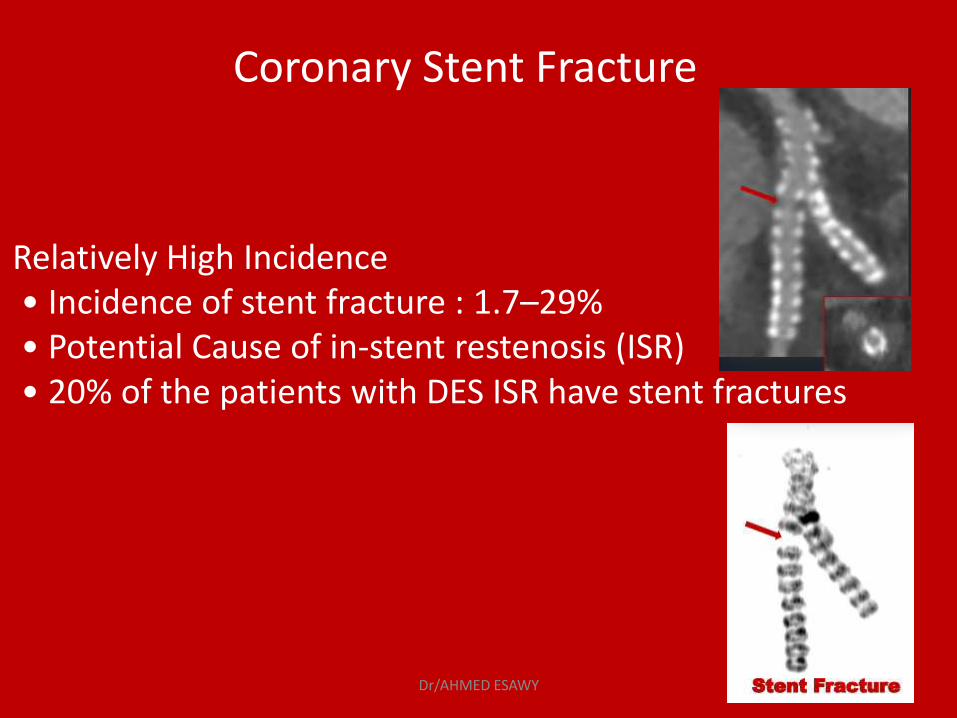
Coronary Stent Fracture
Relatively High Incidence • Incidence of stent fracture : 1.7–29% • Potential Cause of in-stent restenosis (ISR) • 20% of the patients with DES ISR have stent fractures
Dr/AHMED ESAWY
Longitudinal Compression
Definition • Distortion or shortening of a stent in the longitudinal axis following successful stent • New generation drug-eluting stents (DES) • Lower longitudinal strength due to thin strut
Dr/AHMED ESAWY
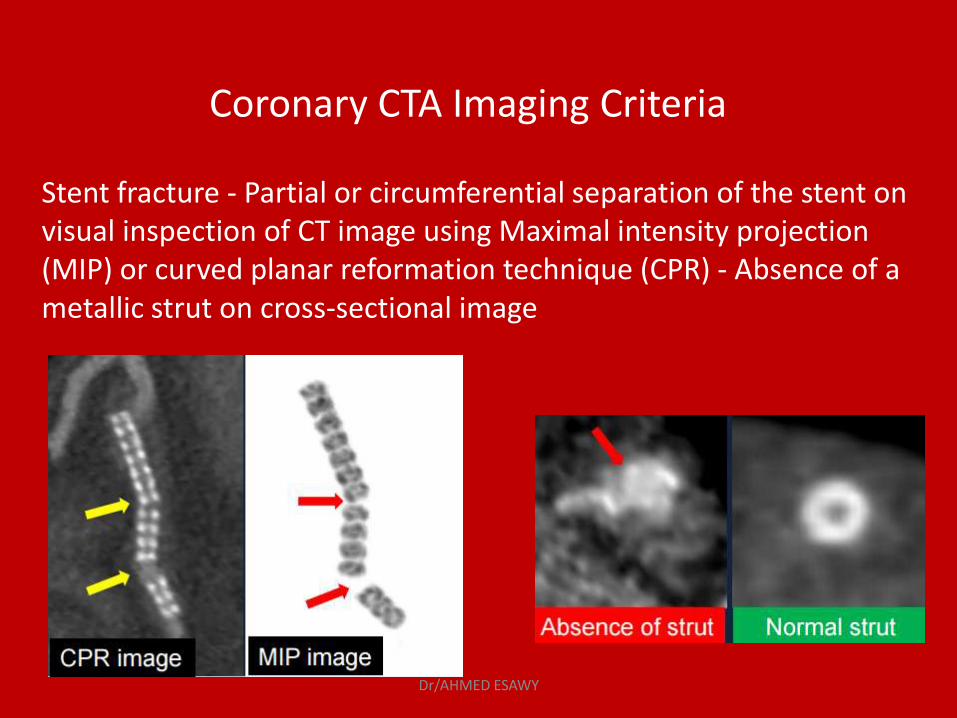
Coronary CTA Imaging Criteria
Stent fracture - Partial or circumferential separation of the stent on visual inspection of CT image using Maximal intensity projection (MIP) or curved planar reformation technique (CPR) - Absence of a metallic strut on cross-sectional image
Dr/AHMED ESAWY
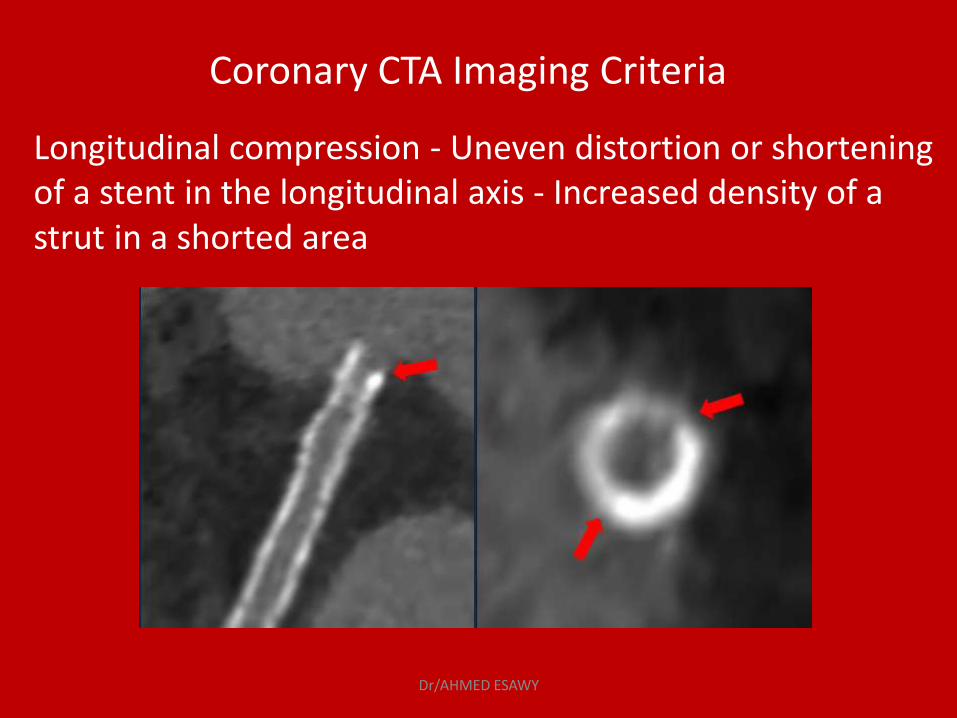
Coronary CTA Imaging Criteria
Longitudinal compression - Uneven distortion or shortening of a stent in the longitudinal axis - Increased density of a strut in a shorted area
Dr/AHMED ESAWY
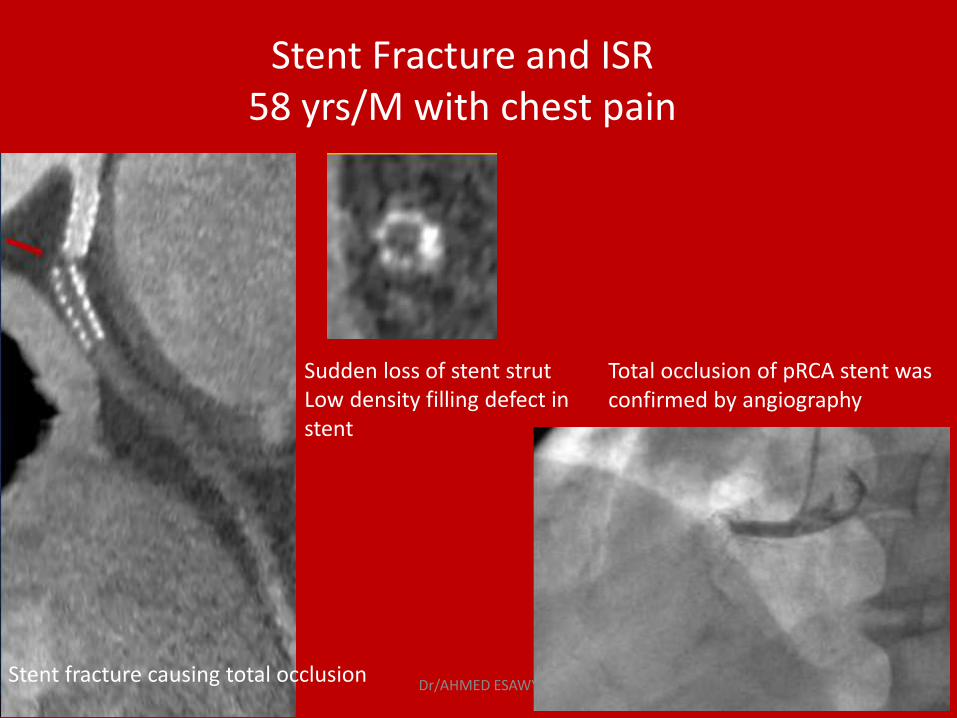
Stent Fracture and ISR 58 yrs/M with chest pain
Stent fracture causing total occlusion
Sudden loss of stent strut Low density filling defect in stent
Total occlusion of pRCA stent was confirmed by angiography
Dr/AHMED ESAWY
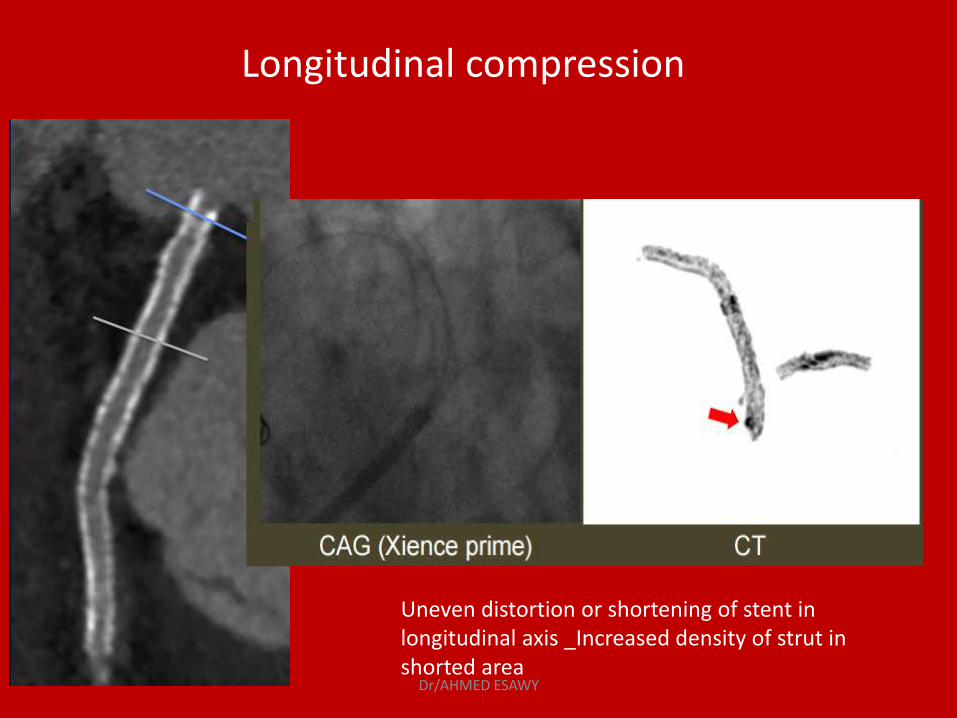
Longitudinal compression
Uneven distortion or shortening of stent in longitudinal axis _Increased density of strut in shorted area
Dr/AHMED ESAWY
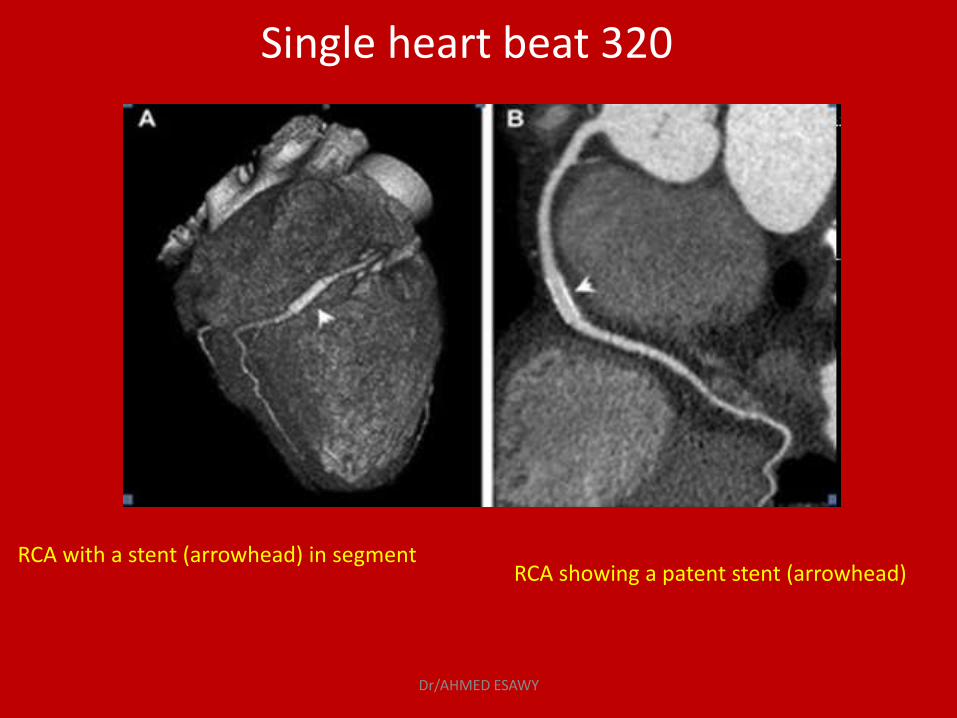
Single heart beat 320
RCA with a stent (arrowhead) in segment RCA showing a patent stent (arrowhead)
Dr/AHMED ESAWY
Single heart beat 320
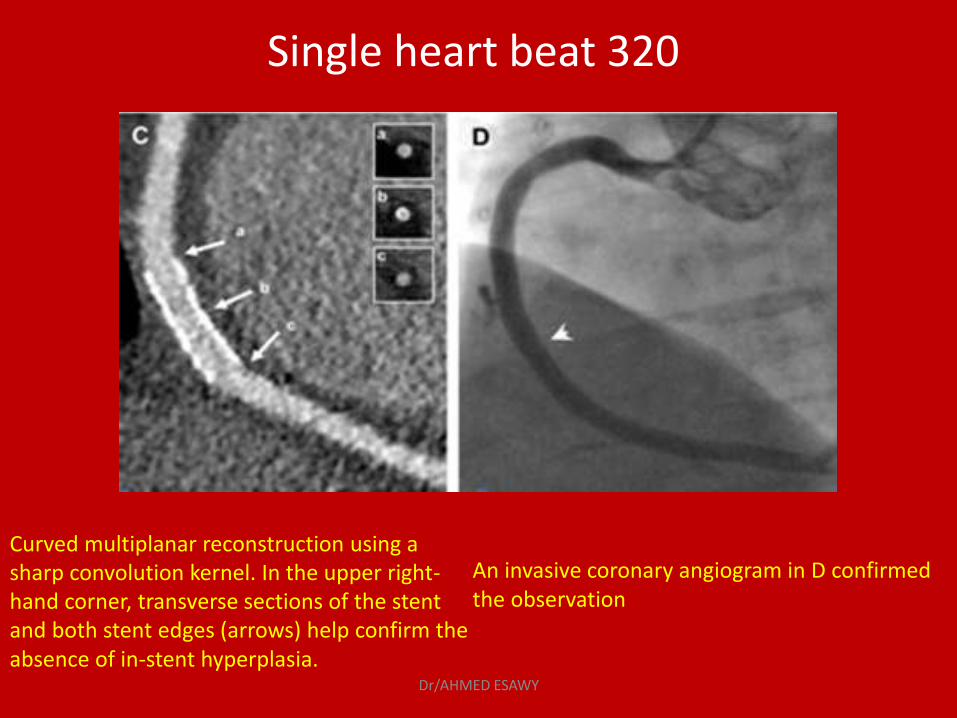
Curved multiplanar reconstruction using a sharp convolution kernel. In the upper right-hand corner, transverse sections of the stent and both stent edges (arrows) help confirm the absence of in-stent hyperplasia.
An invasive coronary angiogram in D confirmed the observation
Dr/AHMED ESAWY



















